RESEARCH LETTER
Acral Intravascular Papillary Endothelial Hyperplasia Mimicking Melanoma on Dermoscopy
Yang LI1†![]() , Eryi LIN1†, Fangfang WU1 and Guannan ZHU1*
, Eryi LIN1†, Fangfang WU1 and Guannan ZHU1*
1Dermatology Hospital, Southern Medical University, Guangzhou, China. *Email: zhuguannan@smu.edu.cn
†These authors contributed equally to this work and share first authorship.
Citation: Acta Derm Venereol 2026; 106: adv-2026-0440. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0440.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 24, 2026. Accepted after revision: Mar 10, 2026.
Published: Mar 30, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
To the Editor,
Acral pigmented lesions frequently pose diagnostic difficulties in daily dermatologic practice, particularly when dermoscopic structures traditionally associated with melanoma are encountered. Blue–white structureless zones are commonly regarded as alarming features; however, they may occasionally reflect nonmelanocytic processes related to haemorrhage or vascular pathology rather than true melanocytic proliferation.
We report the case of a 62-year-old patient who presented with a slowly enlarging blue–black nodule on the plantar aspect of the toe, noticed for several months. The lesion measured approximately 10 mm in diameter and appeared slightly exophytic with poorly defined borders (Fig. 1A). Given the acral location and dark colouration, acral melanoma was initially suspected, although the lesion was clinically symmetrical and lacked ulceration. Dermoscopic examination revealed a centrally located dark exophytic structure surrounded by blue–white structureless zones, a pattern that may raise suspicion for melanoma. In addition, a peripheral homogeneous dark red area encircled by a faint yellowish halo was observed, suggesting a haemorrhagic or vascular component and raising consideration of targetoid haemosiderotic haemangioma (Fig. 1B). Reflectance confocal microscopy demonstrated marked hyperkeratosis and multiple lacunar spaces within the superficial dermis filled with highly reflective material but did not reveal atypical melanocytic proliferation, pagetoid spread or junctional architectural disarray (Fig. 2A–B). Complete excision was performed.
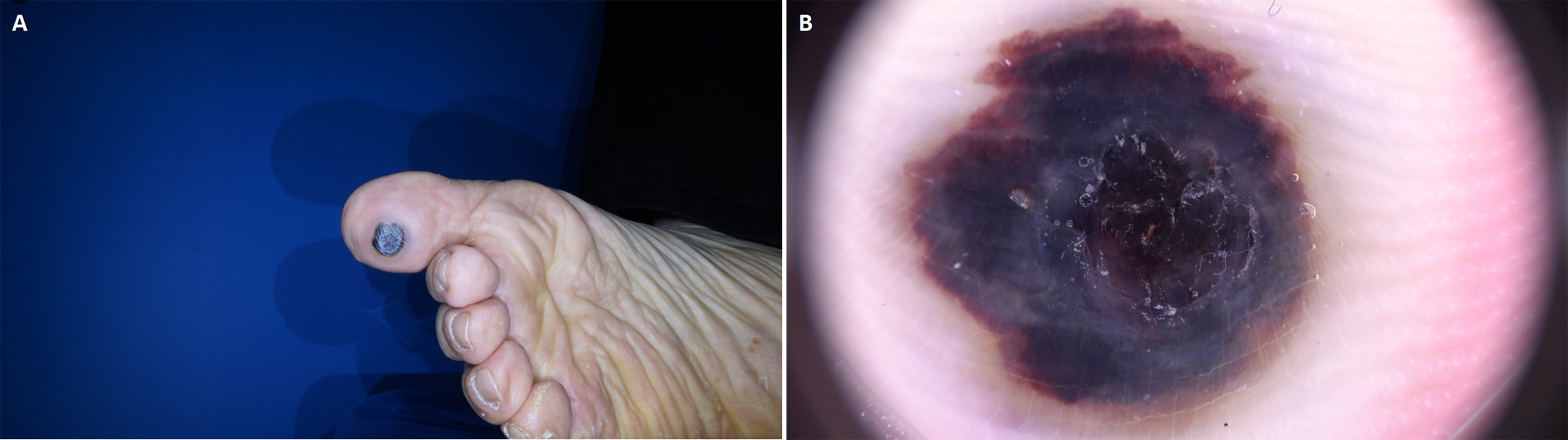
Fig. 1. Clinical and dermoscopic features of acral intravascular papillary endothelial hyperplasia. (A) Clinical photograph showing a blue–black, slightly exophytic nodule on the plantar aspect of the toe with relatively regular contours. (B) Dermoscopy demonstrating a centrally located dark exophytic structure surrounded by blue–white structureless zones. A peripheral homogeneous dark red area with a faint yellowish halo is also present.
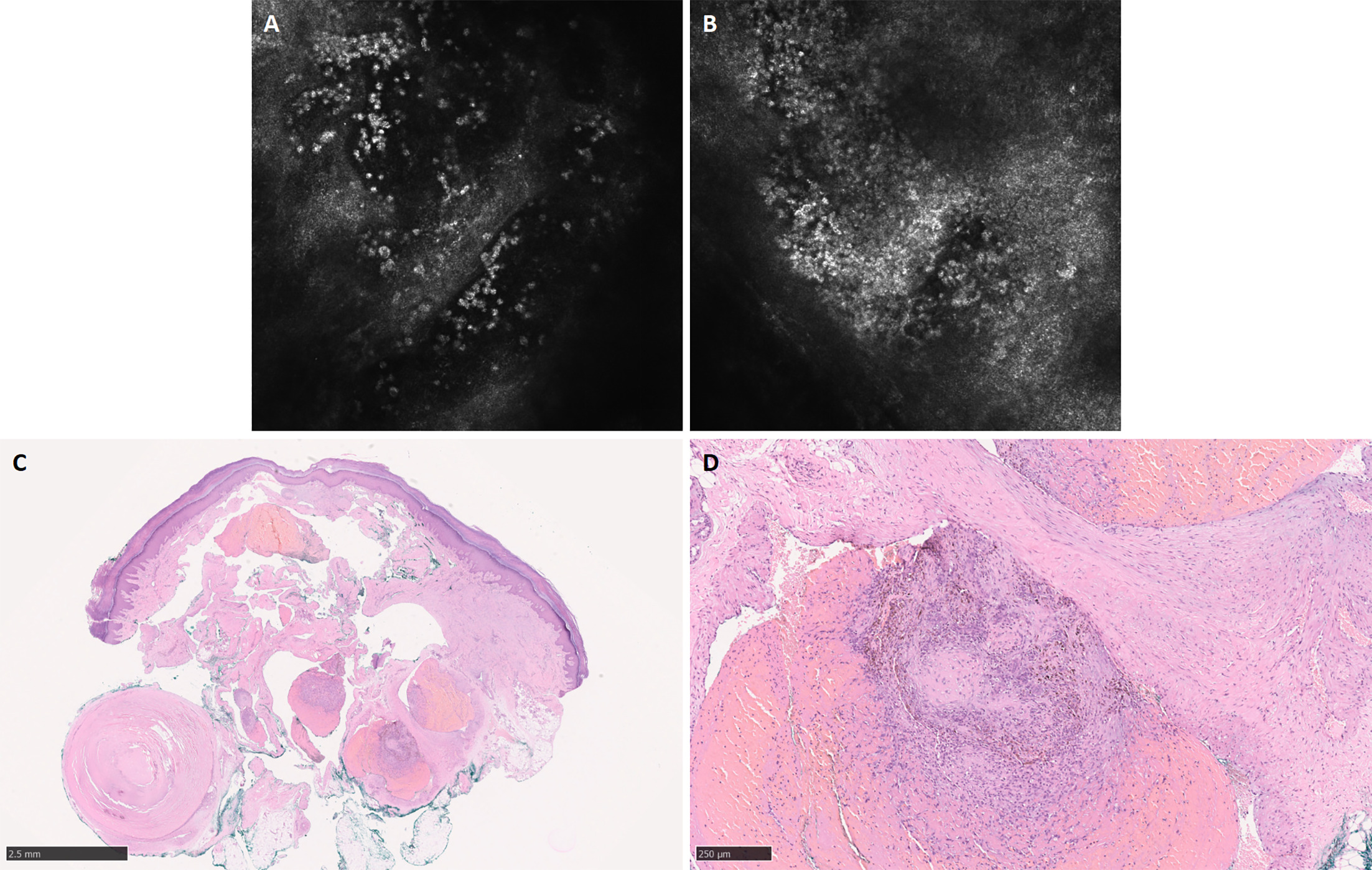
Fig. 2. Reflectance confocal microscopy and histopathologic findings. (A) Reflectance confocal microscopy showing marked hyperkeratosis and multiple lacunar spaces within the superficial dermis filled with highly reflective material. (B) Reflectance confocal microscopy showing absence of atypical melanocytic proliferation, pagetoid spread or junctional architectural disarray. (C) Histopathology demonstrating irregularly dilated dermal vessels containing intravascular papillary proliferations of capillary-sized endothelial structures associated with organizing thrombus (haematoxylin–eosin, original magnification ×40). (D) Higher magnification showing fibrin deposition and focal haemosiderin accumulation within the vascular lumen without cytological atypia (haematoxylin–eosin, original magnification ×200).
Histopathological examination showed irregularly dilated dermal vessels containing papillary proliferations of capillary-sized endothelial structures associated with organizing thrombus. Prominent fibrin deposition and focal haemosiderin accumulation were present, without cytologic atypia or increased mitotic activity. These findings were consistent with intravascular papillary endothelial hyperplasia (IPEH) (Fig. 2C–D).
IPEH, also known as Masson tumour, is a benign reactive vascular lesion characterized by papillary endothelial proliferation associated with thrombus organization (1). Although acral involvement has been described, most reported cases present as subcutaneous nodules, and dermoscopic features of acral IPEH have not been systematically reported (2). In the present case, dermoscopy revealed a pattern that closely mimicked melanoma. The blue–white structureless zone is a classic but nonspecific dermoscopic structure most commonly associated with melanoma (3). Histopathologically, the blue colour is due to the Tyndall effect, typically melanin or melanin-laden macrophages, whereas the white component reflects epidermal hyperkeratosis or epidermal thickening (4). Importantly, similar blue–white structureless zones may also be observed in nonmelanocytic lesions associated with haemorrhage and iron deposition.
The peripheral targetoid configuration and yellowish halo observed in this case resembled the dermoscopic pattern of targetoid haemosiderotic haemangioma, a benign vascular lesion characterized by repeated haemorrhage and haemosiderin deposition (5). This observation suggested a vascular process driven by thrombosis and blood degradation rather than a primary melanocytic proliferation. Clinicopathological correlation confirmed that the melanoma-like dermoscopic appearance was attributable to hyperkeratosis, intravascular thrombosis and prominent haemosiderin deposition within IPEH. Similar mechanisms have been described in other benign entities, such as haemosiderotic dermatofibroma, which may also simulate melanoma dermoscopically (6). Notably, although haemosiderin deposition is not uncommon in the histopathologic spectrum of IPEH, most reported lesions are located in the subcutaneous tissue. As a result, their dermoscopic correlates may not be readily appreciable, which could explain the paucity of dermoscopic descriptions of IPEH in the existing literature (7).
When dermoscopy reveals melanoma-like features in acral lesions but lacks definitive melanocyte-specific criteria, additional noninvasive imaging may be helpful. In this case, reflectance confocal microscopy supported a nonmelanocytic process by excluding key confocal features of melanoma, thereby reducing preoperative diagnostic uncertainty (8). Nevertheless, given the acral location and the clinical concern for melanoma, complete excision was considered necessary to establish a definitive diagnosis. This case highlights an important dermoscopic pitfall in acral vascular lesions and underscores the complementary role of dermoscopy, reflectance confocal microscopy and histopathologic examination in the evaluation of challenging acral pigmented lesions. Awareness of this presentation is clinically relevant, as IPEH is benign and curable by simple excision.
REFERENCES
- Leilei C, Yi Y, Shuyang Z. Intravascular papillary endothelial hyperplasia (Masson tumor) of the right wrist: a case report and literature review. JPRAS Open 2024; 41: 240–243. https://doi.org/10.1016/j.jpra.2024.03.014
- Alsaif M, Alosaimi K, Alhassan T, Alyamani A, Alfawzan M. Intravascular papillary endothelial hyperplasia (Masson’s tumor) of the finger: a case report and review of the literature. Case Reports Plast Surg Hand Surg 2025; 12: 2513066. https://doi.org/10.1080/23320885.2025.2513066
- Williams NM, Rojas KD, Reynolds JM, Kwon D, Shum-Tien J, Jaimes N. Assessment of diagnostic accuracy of dermoscopic structures and patterns used in melanoma detection: a systematic review and meta-analysis. JAMA Dermatol 2021; 157: 1078–1088. https://doi.org/10.1001/jamadermatol.2021.2845
- Massi D, De Giorgi V, Carli P, Santucci M. Diagnostic significance of the blue hue in dermoscopy of melanocytic lesions: a dermoscopic-pathologic study. Am J Dermatopathol 2001; 23: 463–469. https://doi.org/10.1097/00000372-200110000-00013
- Biondo G, Pistone G, Bongiorno MR. A pigmented papule acting like a playful ghost: dermoscopy of three targetoid hemosiderotic hemangiomas. G Ital Dermatol Venereol 2018; 153: 685–691. https://doi.org/10.23736/S0392-0488.17.05509-2
- Vargas-Chandomid E, Álvarez-Rivero V, Olguín-García M, Jurado-Santa F, Morales-Sánchez M. Dermoscopic findings of hemosiderotic dermatofibroma: a comprehensive review. Int J Dermatol Venereology Leprosy Sci 2022; 5: 16–19. https://doi.org/10.33545/26649411.2022.v5.i1a.108
- Johnson ES, Maxey JM, Brody R, Zhang P, Dioufa N. A rare case of intravascular papillary endothelial hyperplasia of the hypopharynx: a case report and literature review. Cureus 2025; 17: e88935. https://doi.org/10.7759/cureus.88935
- Scharf C, Argenziano G, Brancaccio G, Licata G, Ronchi A, Moscarella E. Melanocytic or not? Dermoscopy and reflectance confocal microscopy for lesions difficult to diagnose: a cross-sectional diagnostic accuracy study. Dermatol Pract Concept 2021; 11: e2021127. https://doi.org/10.5826/dpc.1104a127