SHORT COMMUNICATION
Atypical Prurigo Pigmentosa Following Ketogenic Diet: Successful Treatment with Doxycycline and Tofacitinib
Xiaoxiao ZHANG1 and Zhangyu BU1*
1The Fourth School of Clinical Medicine, Zhejiang Chinese Medical University. Hangzhou First People’s Hospital, Hangzhou City, Zhejiang Province, China. *Email: buzyhz@163.com
Citation: Acta Derm Venereol 2026; 106: adv-2026-0465. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0465.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 4, 2026. Accepted after revision: Mar 19, 2026.
Published: Apr 14, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
This work was supported by Hangzhou Health Commission Project (grant no.ZD20240004).
Prurigo pigmentosa (PP) is a rare inflammatory dermatosis first described by Nagashima in 1978, characterized by pruritic erythematous papules that typically resolve with reticular hyperpigmentation. While its pathogenesis remains incompletely understood, a strong association with ketogenic diet has been established (1, 2). We report a biopsy-confirmed case of PP in a female patient who developed rapid weight loss following a ketogenic diet, yet lacked the characteristic reticular hyperpigmentation. Histopathology revealed a predominantly lymphocytic infiltration. A combination therapy of doxycycline and tofacitinib resulted in rapid disease remission.
CASE REPORT
A female patient in her thirties presented with a 2-year history of intermittent pruritic eruptions on the abdomen. The episodes coincided with attempts at a ketogenic diet for weight reduction and were initially self-limiting. She had no underlying diseases and was not taking any medication. During this period, she was diagnosed with eczema at other hospitals and treated with topical corticosteroids and oral antihistamines without significant improvement.
Two months prior to admission, she strictly adhered to a ketogenic diet, achieving a rapid weight loss of 40 kg. Concurrently, the cutaneous lesions acutely exacerbated, spreading to the chest and back and becoming severely pruritic.
Physical examination revealed symmetrically distributed erythematous papules on the chest, back and abdomen (Fig. 1a, b). Notably, no reticular hyperpigmentation was observed. Differential diagnoses included erythema multiforme, dermatitis herpetiformis, and confluent and reticulated papillomatosis (3). However, the absence of target lesions, negative direct immunofluorescence and lack of response to prior anti-allergy treatments made these less likely.

Fig. 1. Clinical findings of prurigo pigmentosa.
A skin biopsy from the abdomen showed hyperkeratosis, focal parakeratosis, basal cell vacuolization and a superficial perivascular infiltrate predominantly composed of lymphocytes with scattered neutrophils. Focal pigment incontinence was present. Direct immunofluorescence was negative (Fig. 2).
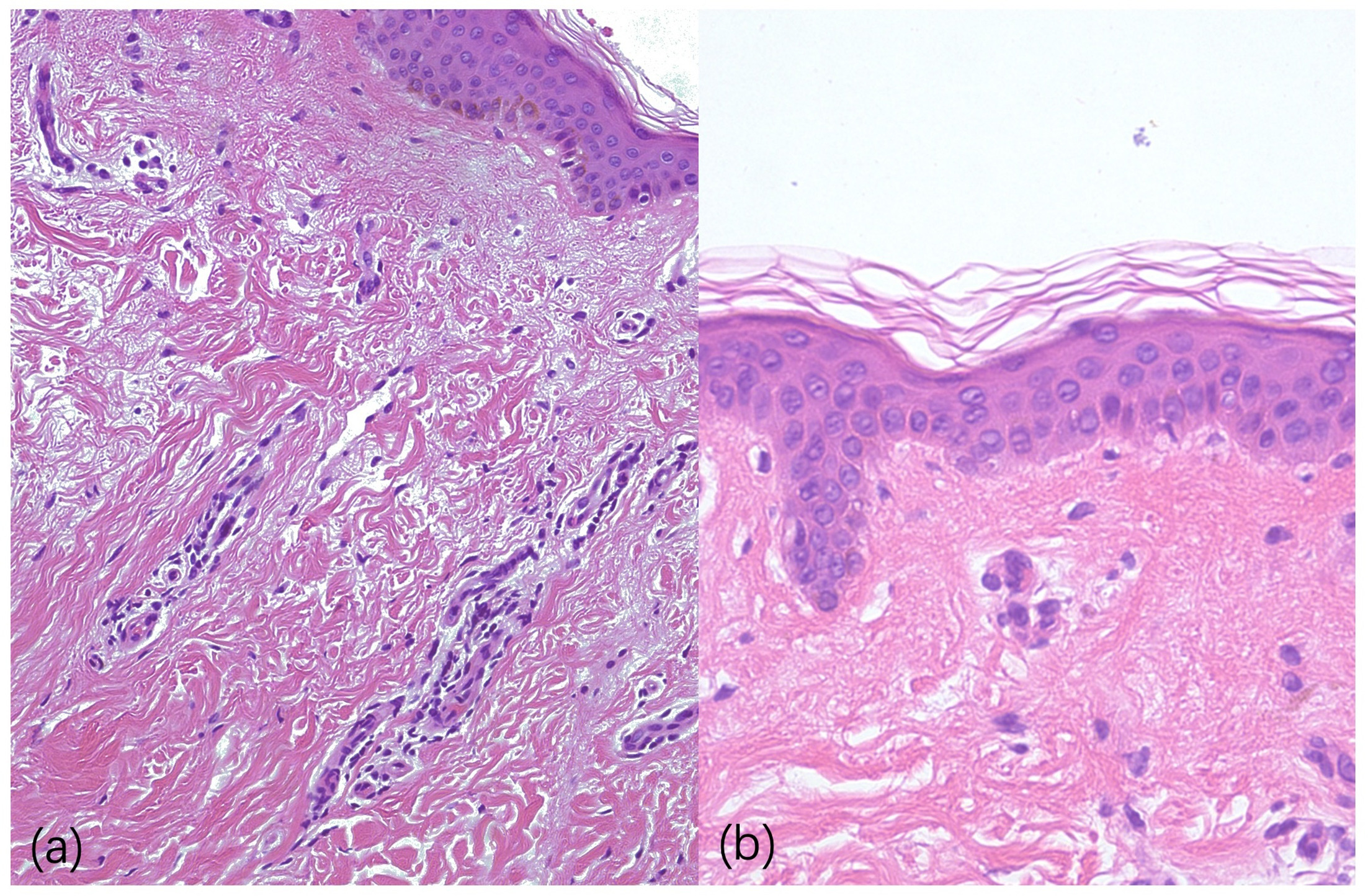
Fig. 2. Histopathology of prurigo pigmentosa (H&E, 200x). H&E: haematoxylin and eosin.
Based on the discrepancy between the atypical clinical presentation and histopathological findings suggestive of PP, a diagnosis of PP was established. Given the predominantly lymphocytic infiltrate, a T-cell-mediated pathogenesis with secondary neutrophil recruitment was postulated. Treatment was initiated with doxycycline 100 mg twice daily and tofacitinib 5 mg twice daily. After 4 weeks, pruritus completely resolved and the inflammatory lesions evolved into asymptomatic hyperpigmented macules (Fig. 1c, d). No new lesions emerged following gradual reintroduction of carbohydrates into the diet.
DISCUSSION
We report a case of PP with an atypical clinical presentation, lacking the characteristic reticular hyperpigmentation. The diagnosis was established through clinicopathological correlation, considering the typical lesional distribution, temporal association with ketogenic diet and supportive histopathological features. This case underscores that PP should be considered even in the absence of reticular hyperpigmentation, provided that the distribution and histopathology are consistent.
Recent evidence suggests that PP may represent a T cell-driven inflammatory dermatosis with secondary neutrophil recruitment. Liu et al. demonstrated upregulation of IL-6 and IL-8 in PP lesions, implicating the JAK-STAT signalling pathway in its pathogenesis (4). The JAK-STAT pathway plays a central role in mediating the effects of multiple pro-inflammatory cytokines. IL-6 signals through JAK1/JAK2, leading to STAT3 phosphorylation and subsequent Th17 differentiation. Th17 cells produce IL-17, a key inducer of neutrophil chemotaxis via IL-8 production from keratinocytes and fibroblasts. Tofacitinib, a JAK1/JAK3 inhibitor, disrupts this cascade at multiple levels: it directly suppresses T-cell activation, reduces Th17 differentiation and decreases IL-8 production, thereby attenuating neutrophil recruitment (5). Doxycycline complements this by directly inhibiting neutrophil chemotaxis, adhesion and matrix metalloproteinase release, addressing the effector phase of the inflammatory response (6).
In our patient, the predominantly lymphocytic infiltrate suggested that T cell-driven inflammation constituted the primary pathogenic mechanism. The rapid resolution of skin lesions following combination therapy suggests that doxycycline combined with tofacitinib may represent an effective therapeutic strategy for atypical or refractory PP with a prominent T-cell inflammatory phenotype.
While combination therapy offers theoretical synergistic benefits, potential risks include increased immunosuppression and drug interactions. Tofacitinib has been associated with potential adverse effects (7), including an increased risk of infections, while doxycycline may cause gastrointestinal discomfort and photosensitivity (8). In our patient, no adverse events were observed during the treatment period, suggesting that short-term combination therapy may be well tolerated. However, larger studies are needed to establish safety.
The predominantly lymphocytic infiltrate in our patient, as opposed to the neutrophilic predominance classically described, suggests that PP may encompass a spectrum of inflammatory phenotypes. This heterogeneity may explain the variable response to tetracycline monotherapy and supports a histopathology-guided approach to treatment selection. Cases with prominent lymphocytic infiltration may benefit from early addition of T-cell targeted therapies.
This case highlights two practical takeaways for clinicians: (1) PP should be suspected in patients with pruritic truncal eruptions and a history of ketogenic diet, even in the absence of reticular hyperpigmentation; and (2) skin biopsy with careful characterization of the inflammatory infiltrate can guide treatment selection, with lymphocyte-predominant cases potentially benefiting from JAK inhibitor combination therapy.
REFERENCES
- Demircioğlu D, Durmaz EÖ, Demirkesen C, Şahin S. Prurigo pigmentosa: review of the literature, impact of ketogenic diets and proposal of a hypothesis. Indian J Dermatol 2025; 70: 146–151. https://doi.org/10.4103/ijd.ijd_464_22
- Xiao A, Kopelman H, Shitabata P, Nami N. Ketogenic diet-induced prurigo pigmentosa (the “keto rash”): a case report and literature review. J Clin Aesthetic Dermatol 2021; 14: S29–S32.
- Capucilli P, Wan J, Corry J, Chuang JH, Linn RL, Perman MJ. Prurigo pigmentosa: an itchy, urticarial eruption confused for food allergy. J Allergy Clin Immunol Pract 2018; 6: 1381–1382. https://doi.org/10.1016/j.jaip.2018.02.033
- Liu Y, Li J, Zhou G, Wang J, Chen X, Chen S, et al. Prurigo pigmentosa: a retrospective study of 11 patients. Indian J Dermatol Venereol Leprol 2024; 90: 661–665. https://doi.org/10.25259/IJDVL_751_2023
- Schwartz DM, Kanno Y, Villarino A, Ward M, Gadina M, O’Shea JJ. JAK inhibition as a therapeutic strategy for immune and inflammatory diseases. Nat Rev Drug Discov 2017; 16: 843–862. https://doi.org/10.1038/nrd.2017.201
- Navarro-Triviño FJ, Pérez-López I, Ruiz-Villaverde R. Doxycycline, an antibiotic or an anti-inflammatory agent? The most common uses in dermatology. Actas Dermosifiliogr 2020; 111: 561–566. https://doi.org/10.1016/j.ad.2019.12.006
- Rajput Khokhar A, Ghoreschi K, Huynh J. Adverse effects of Janus kinase inhibitors with relevance for daily practice in dermatology. J Dtsch Dermatol Ges 2025; 23: 1127–1140. https://doi.org/10.1111/ddg.15796
- Waitayangkoon P, Moon SJ, Tirupur Ponnusamy JJ, Zeng L, Driban J, McAlindon T. Long-term safety profiles of macrolides and tetracyclines: a systematic review and meta-analysis. J Clin Pharmacol 2024; 64: 164–177. https://doi.org/10.1002/jcph.2358