RESEARCH LETTER
A Little Finger with Long-standing Blue Discolouration and Nail Dystrophy
Sui-jiang WANG1![]() , Yu-Dan JIN2*, Xiao-Fang LI3 and Hai-Hua HUANG4
, Yu-Dan JIN2*, Xiao-Fang LI3 and Hai-Hua HUANG4
1Department of Plastic and Reconstructive Surgery, Guangdong Second Provincial General Hospital, Guangzhou, Guangdong, 510317, China, 2Department of Plastic and Reconstructive Surgery, Second People’s Hospital of Zhongshan, Zhongshan, Guangdong, 528447, China, 3Department of Pathology, Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, 524001, China, and 4Department of Plastic Surgery, The Second Affiliated Hospital, School of Medicine, The Chinese University of Hong Kong, Shenzhen & Longgang District People’s Hospital of Shenzhen, Shenzhen, Guangdong, 518172, China. *Email: jinyudan04@163.com
Citation: Acta Derm Venereol 2026; 106: adv-2026-0570. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0570.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Apr 2, 2026. Accepted after revision: Apr 16, 2026.
Published: May 4, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Blue nevi (BN), characterized by intradermal melanocytic proliferations with stromal sclerosis (1), may occur in skin or extracutaneous sites; those that occur in the nail unit are termed subungual BN. There have been 32 cases of subungual BN reported in English literature, none being associated with the little finger. They have a predilection for female and for hand, with the thumb and hallux being the most common and second common sites of involvement, respectively. Acquired lesions predominate and are diagnosed at a mean age of 40.7 years (range, 4–76 years) (2).
CASE REPORT
A 51-year-old woman presented with an asymptomatic pigmentation and nail splitting on her left little finger. The pigmentation began as a blue-grey spot at the midline of the proximal nailfold 22 years prior to presentation. A few months later, the patient noticed the central distal portion of the nail plate become pale, fragile and eventually splitting. Over time, the pigmentation enlarged slowly into the lunula, while the nail changes seemed no pronounced change. Physical examination revealed an enlarged lunula, ill-defined blue pigmentation of the proximal nailfold and lunula, and triangular onychoschizia with central fissuring on the left little finger (Fig. 1). Lymphadenopathy was not found. Both medical and family histories were noncontributory. The lesion, measured 5×3 mm, was removed with the matrix en bloc to the level of periosteum after reflection of the proximal nailfold, with no recurrence detected at 5-year follow-up.

Fig. 1. A left fifth finger with a macrolunula, ill-bordered blue pigmentation in the proximal nailfold and lunula areas, and triangular onychoschizia with central fissuring.
Histopathologically, the lesion was composed of pigmented spindle and dendritic cells interspersed with melanophages distributed among the thickened dermal collagen fibre bundles, with thinning of the matrix. Immunohistochemically, the cells stained positively with HMB-45, S-100, and MART-1. There was no junctional component nor atypical features (Fig. 2). This in combination with the clinical findings allowed a diagnosis of common blue nevus (2).
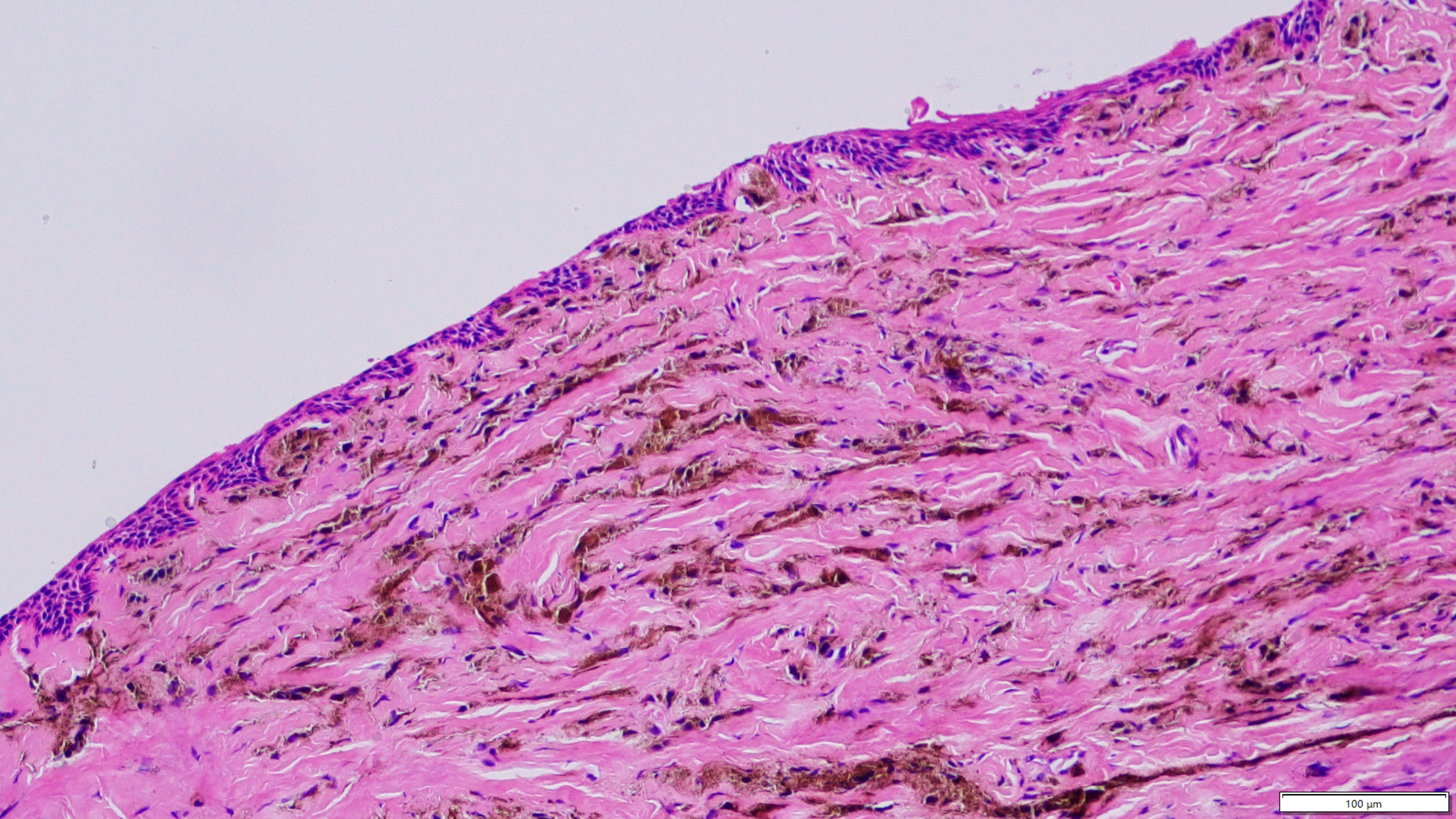
Fig. 2. Scanning magnification view of a common blue nevus with an intervening grenze zone and thinned matrix (haematoxylin-eosin, original magnification ×20; scale bar: 100 μm). The lesion is composed of spindled and dendritic nevus cells, melanophages, and thickened dermal collagen fibre bundles. The nevus cells contain variable amounts of melanin pigment in the cytoplasm and the processes. Neither cytological nor nuclear atypia nor mitotic activity is observed.
DISCUSSION
Subungual BN are clinically divided into periungual BN and subungual BN proper. Both of them are typically flat or slightly elevated, blue to blue-grey, asymptomatic, and<3 cm in diameter, with the latter probably with to boot presentations peculiar to the nail apparatus (2). On imaging, subungual BN present with structureless homogenous pigmentation dermoscopically (3) and homogenous hypoechogenic band ultrasonographically (4, 5).
Subungual BN proper account for more than 90 % of the reported cases (2). They are located under the matrix and/or nail bed and look ill-defined through the proximal nail fold and/or nail plate. Accompanying presentations include lunular dysmorphology, e.g., macrolunula and asymmetric lunula, nail dystrophy and nail dyschromia. Longitudinal melanonychia may show a malignant pattern and be the mere presenting sign (6), confusing BN with melanoma both clinically and dermoscopically. Macrolunula and onychodystrophy can occur separately or concomitantly, in benignancy or in melanoma, and regardless of BN subtypes. Nevertheless, their presence is strongly in favour of submatrical BN in the presence of a blue-black pigmentation at the proximal nailfold and/or lunula area (7). Macrolunula is etiologically underexpounded, and we believe it is liable to the thinning of the matrix. BN-related onychodystrophy is progressive, presented differently, from dermatoscopically mild dystrophy to clinically overt partial-thickness erosion, in different cases (2). In our case, it remained dystrophic without ulceration after a prolonged duration exceeding 20 years, in contrast to melanoma (1). Differential diagnoses of subungual BN include glomus tumour, myxoid cyst, pyogenic granulation, neurofibroma, tenosynovial giant cell tumour, aneurysmal bone cyst, onychopapilloma, onychomatricoma, onychocytic matricoma, pigmented epithelioid melanocytoma, squamous cell carcinoma, basal cell carcinoma, Kaposi sarcoma and melanoma (melanonychia and nonmelanonychia-type, primary, metastatic, and regressed); all but pigmented epithelioid melanocytoma can be clinically distinguishable.
Subungual BN require to be distinguished between common BN and melanocytomas, including cellular, combined, and atypical cellular BN, due to their distinct biological behaviour. Recent onset of a blue nodule or change of a preexisting blue lesion argues against common BN, yet current data fail to confirm a more rapid growth of cellular BN compared with common BN in the subungual setting despite those that do otherwise in cutaneous BN (1, 2). Long-standing lesions (>10 years) of ∽ 10 mm in diameter have been reported across the histopathologic subtypes of subungual BN (2). Histopathology is critical to the distinction. Common BN are distinguished by a predominance of loosely distributed pigmented dendritic melanocytes without atypic features nor a second nevus component (1, 2).
An excisional biopsy is mandatory, with techniques, including complete excision with free margins, matricoectomy, or involved nail apparatus, tailored to lesion characteristics, such as its site, size and orientation and level of suspicion (8). In those submatrical cases, nail deformity will be inevitable postoperatively.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge Mr. Hailun Wang for his help in preparation of specimens.
REFERENCES
- Elder DE, Barnhill RL, Cook MG, de la Fouchardiere A, Gerami P. Melanocytic tumors. In: Elder DE, Massi D, Scolyer RA, Willemze R, editors. WHO classification of skin tumors. 4th ed. Vol Lyon, France 2018: p. 65–152.
- Dehavay F, Goettmann S, Zaraa I, Moulonguet I, André J, Caucanas M, et al. Nail unit blue nevi: a 11-case series and review of the literature. Skin Appendage Disord 2020; 6: 287–295. https://doi.org/10.1159/000509204
- Martin B, de la Fouchardiere A, Markiewicz D, Bartolo E, Bhargava K, Lewis F, et al. Subungual melanoma with blue naevus-like morphological features: a clinicopathological retrospective analysis of nine cases. Pathology 2022; 54: 541–547. https://doi.org/10.1016/j.pathol.2021.12.293
- Causeret AS, Skowron F, Viallard AM, Balme B, Thomas L. Subungual blue nevus. J Am Acad Dermatol 2003; 49: 310–312. https://doi.org/10.1067/s0190-9622(03)00410-9
- Dogan S, Atakan N, Khurami H, Gökoz O, Bitik O. Subungual blue naevus presenting with elkonyxis. Hong Kong J Dermatol Venereol 2016; 24: 87–91.
- Göktay F, Güneş P, Yaşar Ş, Güder H, Aytekin S. New observations of intraoperative dermoscopic features of the nail matrix and bed in longitudinal melanonychia. Int J Dermatol 2015; 54: 1157–1162. https://doi.org/10.1111/ijd.12747
- Apalla Z, Lallas A, Longo C, Bobos M, Starace M, Lazaridou E, et al. The dermoscopic pattern of blue nevi involving the nail apparatus. Eur J Dermatol 2020; 30: 192–194. https://doi.org/10.1684/ejd.2020.3726
- Jellinek N. Nail matrix biopsy of longitudinal melanonychia: diagnostic algorithm including the matrix shave biopsy. J Am Acad Dermatol 2007; 56: 803–810. https://doi.org/10.1016/j.jaad.2006.12.001