ORIGINAL REPORT
Absolute Eczema Area and Severity Index Responses with Lebrikizumab in Patients with Moderate-to-severe Atopic Dermatitis: A Secondary Analysis of Two Phase 3 Trials
Diamant THAÇI1*![]() , Luis PUIG2
, Luis PUIG2![]() , Sei-ichiro MOTEGI3
, Sei-ichiro MOTEGI3![]() , Kim PAPP4,5
, Kim PAPP4,5![]() , Linda STEIN GOLD6
, Linda STEIN GOLD6![]() , Leon KIRCIK7,8,9
, Leon KIRCIK7,8,9![]() , Howard SOFEN10
, Howard SOFEN10![]() , Pablo FERNÁNDEZ-PEÑAS11
, Pablo FERNÁNDEZ-PEÑAS11![]() , Pedro HERRANZ12
, Pedro HERRANZ12![]() , Christian VESTERGAARD13
, Christian VESTERGAARD13![]() , Yu-Huei HUANG14
, Yu-Huei HUANG14![]() , Martin DOSSENBACH15
, Martin DOSSENBACH15![]() , Hany ELMARAGHY15
, Hany ELMARAGHY15![]() , Gaia GALLO15
, Gaia GALLO15![]() , Maria Jose RUEDA15, Marta CASILLAS15
, Maria Jose RUEDA15, Marta CASILLAS15![]() , Chao YANG15, Helena AGELL16, Meritxell FALQUÉS16
, Chao YANG15, Helena AGELL16, Meritxell FALQUÉS16![]() and Audrey NOSBAUM17
and Audrey NOSBAUM17![]()
1Institute and Comprehensive Center for Inflammatory Medicine, University of Lübeck, Lübeck, Germany, 2Department of Dermatology, Hospital de la Santa Creu i Sant Pau, Universitat Autònoma de Barcelona, Barcelona, Spain, 3Department of Dermatology, Gunma University Graduate School of Medicine, Maebashi, Japan, 4Alliance Clinical Research and Probity Medical Research, Waterloo, ON, Canada, 5Division of Dermatology, Temerty Faculty of Medicine, University of Toronto, Toronto, ON, Canada, 6Henry Ford Health System, Detroit, MI, United States, 7Clinical Professor of Dermatology, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 8Adjunct Clinical Professor of Dermatology, Indiana University School of Medicine, Indianapolis, IN, United States, 9Medical Director, Physicians Skin Care, PLLC; DermResearch, PLLC; Skin Sciences, PLLC, Louisville, KY, United States, 10University of California Los Angeles, Los Angeles, CA, United States, 11Department of Dermatology, Westmead Hospital, Sydney Medical School, The University of Sydney, Sydney, NSW, Australia, 12Department of Dermatology, Hospital Universitario La Paz, Madrid, Spain, 13Department of Dermatology and Venereology, Aarhus University Hospital, Aarhus, Denmark, 14Department of Dermatology, Chang Gung Memorial Hospital, Linkou Branch and School of Medicine, Chang Gung University, Taoyuan 333, Taiwan, 15Eli Lilly and Company, Indianapolis, IN, United States, 16Almirall, S.A., Barcelona, Spain, and 17Hospices Civils de Lyon, South of Lyon Hospital, Allergology and Clinical Immunology Department, Pierre-Bénite, France
Corr: Diamant Thaçi, Institut für Entzündungsmedizin, Universitätsklinikum Schleswig-Holstein Campus Lübeck, Ratzeburger Allee, 160 23538 Lübeck, Germany. *Email: diamant.thaci@uksh.de
Key words: lebrikizumab; atopic dermatitis; moderate-to-severe; Eczema Area and Severity Index; clinical trial.
Citation: Acta Derm Venereol 2026; 106: adv-2025-0160. DOI: https://doi.org/10.2340/actadv.v106.adv-2025-0160.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Nov 4, 2025. Accepted after revision: Apr 8, 2026.
Published: May 21, 2026.
Competing interests and funding: This study was funded by Eli Lilly and Company and Almirall, S.A. Almirall, S.A. has licensed the rights to develop and commercialize lebrikizumab for the treatment of dermatology indications including atopic dermatitis in Europe. Eli Lilly and Company has exclusive rights for development and commercialization of lebrikizumab in the United States and the rest of the world outside of Europe.
All group-level data analysed during this study are included in this published article or as supplementary information files. Individual-level data are not publicly available, as consent was not sought from study participants.
This study was based on previously conducted studies and did not collect any new primary data.
DT has received grant/research support from and served on a scientific advisory board and a speakers bureau for AbbVie, Almirall, Amgen, Boehringer Ingelheim, Celltrion, Fresenius, Eli Lilly and Company, Galderma, Johnson & Johnson, LEO Pharma, NewBridge, Novartis, Pfizer, Regeneron, Sanofi, Takeda, Target-RWE, UCB, and Vichy. LP has received consultancy/speaker’s honorariahonouraria from and/or participated in clinical trials sponsored by AbbVie, Almirall, Amgen, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Fresenius-Kabi, Johnson & Johnson Innovative Medicine, LEO Pharma, Eli Lilly and Company, Novartis, Pfizer, STADA, Sun Pharma, and UCB. S-iM has received consultancy/speaker’s honorariahonouraria from and/or participated in clinical trials sponsored by AbbVie, LEO Pharma, Otsuka Pharma, Eli Lilly and Company, Pfizer, Maruho Pharma and Torii Pharma. KP has served on a speakers bureau for AbbVie, Amgen, Astellas, Celgene, Eli Lilly and Company, Galderma, Janssen, Kyowa Kirin, LEO Pharma, Merck Sharp & Dohme, Novartis, Pfizer, and Valeant; has received grant/research support from AbbVie, Akros, Allergan, Amgen, Anacor, Arcutis, AstraZeneca, Baxalta, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Coherus, Dermira, Dow Pharma, Eli Lilly and Company, Galderma, Genentech, GlaxoSmithKline, Janssen, Kyowa Kirin, LEO Pharma, MedImmune, Meiji Seika Pharma, Merck Serono, Novartis, Pfizer, Regeneron, Roche, Sanofi Genzyme, Takeda, UCB, and Valeant; has served as a consultant for AbbVie, Akros, Amgen, Arcutis, Astellas, AstraZeneca, Baxalta, Baxter, Boehringer Ingelheim, Bristol Myers Squibb, CanFite, Celgene, Coherus, Dermira, Dow Pharma, Eli Lilly and Company, Forward Pharma, Galderma, Genentech, Janssen, Kyowa Kirin, LEO Pharma, Meiji Seika Pharma, Merck Serono, Merck Sharp & Dohme, Mitsubishi Pharma, Novartis, Pfizer, Regeneron, Roche, Sanofi Genzyme, Takeda, UCB, and Valeant; has received honoraria from AbbVie, Akros, Amgen, Baxter, Boehringer Ingelheim, Celgene, Coherus, Eli Lilly and Company, Forward Pharma, Galderma, GlaxoSmithKline, Janssen, Kyowa Kirin, Merck Serono, Merck Sharp & Dohme, Novartis, Pfizer, Takeda, UCB, and Valeant; and has served as scientific officer or on a steering committee/advisory board for AbbVie, Akros, Amgen, Anacor, Astellas, Baxter, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Dow Pharma, Eli Lilly and Company, Galderma, Janssen, Kyowa Kirin, Merck Serono, Merck Sharp & Dohme, Novartis, Pfizer, Regeneron, Sanofi Genzyme, and Valeant. LSG Gold is an investigator and/or consultant and/or speaker for: AbbVie, Amgen, Arcutis, Bristol Myers Squibb, Dermavant, Eli Lilly and Company, Galderma, Incyte Corporation, Janssen, Novartis, Ortho Dermatologics, Pfizer, Regeneron, Sanofi, and UCB Pharma. LK has received grants from Abbvie, Acambis, Amgen, Inc., Anacor Pharmaceuticals, Anaptys, Arcutis, Arena, Astellas Pharma US, Inc., Asubio, Biomimetrix, Biosion, Dermavant, Dermira, Dow Pharmaceutical Sciences, Inc., Eli Lilly and Company, Ferndale Laboratories, Inc., Galderma, Genentech, Inc., GlaxoSmithKline, PLC, Glenmark, Health Point, LTD, Incyte, LEO Pharma, L’Oreal, Nano Bio, Nektar, Novartis AG, Nucryst Pharmaceuticals Corp, Onset, OrthoDermatologics, OrthoNeutrogena, Promius, PharmaDerm, Pfizer, Quinnova, Rapt, Regeneron, Sanofi, SkinMedica, Inc., Stiefel Laboratories, Inc., Sun Pharma, and Valeant Pharmaceuticals Intl. He has received honoraria from Abbvie, Amgen, Inc., Anacor Pharmaceuticals, Arcutis, Arena, Assos Pharma, Astellas Pharma US, Inc., Biosion, Dermavant, Dermira, Eli Lilly and Company, Ferndale Laboratories, Inc., Galderma, Genentech, Inc., Glenmark, Incyte, Innocutis, Innovail, Kyowa Kirin, LEO Pharma, L’Oreal, Nano Bio, Nektar, Novartis AG, Onset, OrthoDermatologics, OrthoNeutrogena, Promius, PuraCap, Quinnova, Rapt, Regeneron, Sanofi, SkinMedica, Inc., Stiefel Laboratories, Inc., Sun Pharma, Taro, Triax, and Valeant Pharmaceuticals Intl. HS has received consultancy/speaker’s honorariahonouraria from and/or participated in clinical trials sponsored by AbbVie, Almirall, Amgen, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, LEO Pharma, Eli Lilly and Company, Novartis, Sun-Pharma, and UCB. PF-P has served on advisory boards for AbbVie, Celgene, Eli Lilly and Company, Roche, MSD, Janssen, Novartis, and MEDA; received grants/research support from AbbVie, Amgen, Eli Lilly and Company, Janssen, Novartis, Pfizer, Regeneron, and Roche; and received honoraria or consultation fees from AbbVie, Amgen, Eli Lilly and Company, Galderma, Janssen, La Roche-Posay, Merck Serono, MSD, Novartis, Roche, and Schering Plough. PH Herranz has served as consultant, investigator and /or speaker for: AbbVie, Almirall, Amgen, Bristol Myers Squibb, Galderma, LEO Pharma, Johnson & Johnson, Eli Lilly and Company, Novartis, Pfizer, Regeneron, Sanofi, and UCB. CV is an advisor, consultant or investigator for AbbVie, Sanofi Genzyme, Novartis, LEO Pharma, MSD, and Pfizer. He has received research grants from Pfizer, LEO Pharma and Novartis. He has received speaker honorariahonouraria and/or been a consultant for Sanofi Genzyme, LEO Pharma, MEDA, Pfizer, LEO Pharma, Galderma, Novartis, and AbbVie. Y-HH has conducted clinical trials while serving as a principal investigator for Galderma, Eli Lilly and Company, Novartis, and Janssen Pharmaceuticals. He has received honoraria for serving as an advisory board member for Pfizer, AbbVie, and Celgene and has received speaking fees from AbbVie, Eli Lilly and Company, and Novartis. MD, HE, GG, MJR, MC, and CY are employees and minor shareholders of Eli Lilly and Company. MF and Helena Agell are employees of Almirall, S.A. AN is Principal Investigator, advisory board member, speaker, and consultant for AbbVie, Eli Lilly and Company, Galderma, LEO Pharma, Novartis, Pfizer, Regeneron Pharmaceuticals, Inc., and Sanofi Genzyme.
The ADvocate trials (NCT04146363, NCT04178967) investigated adults/adolescents with moderate-to-severe atopic dermatitis (AD) receiving lebrikizumab (LEB) monotherapy, using percent improvement in the Eczema Area and Severity Index (EASI). In clinical trials, percent EASI improvement is used to compare study arms and measure treatment effect size/impact. In clinical practice, however, absolute EASI scores are used (especially in Europe), as they measure an individual’s disease state regardless of baseline severity. This post-hoc analysis assessed absolute EASI response – EASI≤7, ≤5, ≤3 and ≤1 – from the ADvocate trials to understand LEB efficacy in adults/adolescents with moderate-to-severe AD. Week-16 data from patients receiving LEB 250 mg Q2W (n=564) were compared with placebo (n=287). Across baseline moderate/severe/very severe EASI and baseline Investigator’s Global Assessment (IGA) 3/4, significantly higher percentages of patients receiving LEB than those receiving placebo achieved each absolute EASI response. Week-16 LEB EASI 75 responders (n=284) and per-protocol LEB non-responders (n=215) were assessed through week 52. Absolute EASI scores were generally low and stable among responders and reduced among non-responders. Overall, LEB was associated with high rates of durable absolute EASI response, even in cases of high baseline severity or suboptimal week-16 outcomes. Results reflect clinically meaningful improvements that could help guide clinical practice.
SIGNIFICANCE
Atopic dermatitis, or eczema, is a skin condition characterized by patches of red, itchy skin and sometimes oozing skin lesions. Treatments are usually assessed using percent improvement in the Eczema Area and Severity Index, or EASI. However, absolute EASI scores – disease severity at one time, rather than improvement over time – are also important. We found that patients with moderate-to-severe atopic dermatitis receiving lebrikizumab had significantly lower absolute EASI after 16 weeks. Meaningful improvements were often sustained through 1 year. Our findings may help patients and their doctors understand the benefits of lebrikizumab and choose the best treatment for the patient.
Atopic dermatitis (AD) is a common chronic eczematous inflammatory skin disease (1, 2, 3). Treatment response for AD is commonly assessed via percent improvement in the Eczema Area and Severity Index (EASI). Thresholds for improvement in EASI from baseline include ≥50%, ≥75%, ≥90% and 100% (4, 5, 6). The ADvocate1 (NCT04146363) and ADvocate2 (NCT04178967) phase 3 clinical trials reported EASI 75 and EASI 90 (≥75% and ≥90% EASI reduction from baseline) in adults and adolescents with moderate-to-severe AD receiving lebrikizumab (LEB) (7, 8). LEB monotherapy led to significant percent improvements in EASI at week 16, which were generally sustained through week 52 (9, 10, 11). Moreover, patients with suboptimal results (i.e. week-16 per-protocol LEB non-responders) showed an increased response with continued LEB therapy, with over three quarters achieving EASI 75 after 1 year (12).
Data on percent improvement in EASI, however, may not fully capture therapeutic responses in patients with moderate-to-severe AD. Absolute EASI scores can supplement data on percent improvement in EASI by reflecting current disease status regardless of baseline severity. Scores range from 0.0 to 72.0, where 0–1.0 indicates clear or almost clear skin, 1.1–7.0 indicates mild symptoms, 7.1–21.0 indicates moderate disease, 21.1–50.0 indicates severe disease, and >50.0 indicates very severe disease (13, 14). Intermediate cut-offs such as EASI≤3 may serve as useful indicators of optimal therapeutic responses (15). The minimal clinically important difference is 6.6 (16).
For characterizing a patient’s disease in clinical practice, absolute EASI scores are often more meaningful than percent EASI improvement, as they reveal important information that data on percent improvement alone may obscure. For example, in cases with baseline EASI>50 (very severe disease) or an Investigator’s Global Assessment (IGA) score of 4 (severe disease), patients showing 75% or even 90% improvement after treatment with novel therapeutics may still have major signs of disease such as residual skin lesions. Absolute EASI scores are used in real-world clinical practice (especially in Europe) and have been added to clinical recommendations and treat-to-target guidelines for clinician-reported outcome measures of moderate-to-severe AD in adults (15, 17). The use of absolute scores alongside percent improvement has similarly been adopted for the Psoriasis Area and Severity Index (18).
Despite their clinical utility, few studies have assessed absolute EASI scores in patients with moderate-to-severe AD (19, 20), and none have explored the possible association between LEB therapy and absolute EASI scores at key time points. This exploratory, post-hoc data analysis assessed how patients from the ADvocate trials achieved absolute EASI response rates (EASI≤7, ≤5, ≤3 and ≤1) to better understand the efficacy of LEB therapy in adults and adolescents with moderate-to-severe AD.
MATERIALS AND METHODS
Study design
Data were included from ADvocate1 and ADvocate2, two identically designed, 52 week, phase 3 trials investigating adults and adolescents with moderate-to-severe AD (9, 10). The study population was pooled from the ADvocate1 intent-to-treat (ITT) population and ADvocate2 modified intent-to-treat (mITT) population, the latter excluding 18 participants from one site whose eligibility could not be confirmed. This pooled mITT population (ADvocate1 ITT pooled with ADvocate2 mITT) was analysed. Adults and adolescents were analysed together.
The ADvocate trials included an induction period (baseline–week 16) and a maintenance period (week 16–52). During induction, loading doses of LEB 500 mg or placebo were administered at baseline and week 2, followed by LEB 250 mg or placebo every two weeks (Q2W). Induction involved LEB monotherapy; no other systemic or topical treatments for AD were permitted. At week 16, LEB responders and non-responders were assessed. Week-16 responders were defined per protocol as patients who, with LEB therapy and without rescue medication, achieved either an EASI 75 response (≥75% improvement in EASI from baseline) or an IGA score of 0 or 1 with ≥2-point improvement.
For the maintenance period, LEB responders were re-randomized 2 : 2 : 1 into two active treatment arms and one withdrawal arm: LEB 250 mg Q2W, LEB 250 mg Q4W, or placebo (LEB withdrawal). Week-16 LEB non-responders were assigned to the open-label escape arm, where they received LEB 250 mg Q2W. Responders who did not maintain EASI 50 (≥50% EASI improvement from baseline) were moved to the escape arm. Once in the escape arm, patients who did not achieve EASI 50 after 8 consecutive weeks of treatment were discontinued. During maintenance, intermittent topical rescue medications for AD were permitted. At the end of the maintenance period, EASI scores for week-16 responders and non-responders were assessed. Patients were then followed up for safety assessment and invited to enrol in the ADjoin long-term extension study (21, 22).
Eligibility criteria
Participants were adults (aged ≥18 years) or adolescents (aged 12 to <18 years, weighing ≥40 kg) diagnosed with moderate-to-severe AD ≥1 year before screening (10). AD was defined per American Academy of Dermatology Consensus Criteria (23); moderate-to-severe AD was defined per-protocol as EASI≥16, IGA≥3, and ≥10% body surface area of AD involvement at baseline. Participants were candidates for systemic therapy who either had a history of inadequate response to topical therapies or were deemed medically inadvisable to use topical therapies. Participants were naïve to LEB as well as to dupilumab and tralokinumab, other monoclonal antibodies used to treat AD.
Week-16 analysis
Week-16 analysis involved the pooled mITT population during induction. Efficacy endpoints in this post-hoc analysis included achieving week-16 absolute EASI responses of ≤7, ≤5, ≤3 and ≤1. The EASI≤7 (signifying mild symptoms or better) and EASI≤1 (signifying clear/almost clear skin) thresholds are well-established endpoints (13, 14), while the EASI≤5 and EASI≤3 thresholds were selected for this study as intermediate indicators of treatment response. Moreover, the EASI≤3 threshold is considered an optimal target signifying minimal disease activity (15). Treatment efficacy (LEB vs placebo) was assessed for the overall mITT population. Subgroup analyses were also performed by baseline EASI—16.0–21.0 (moderate disease), 21.1–50.0 (severe disease), and >50.0 (very severe disease) – as well as by baseline IGA score – IGA 3 (moderate disease) and IGA 4 (severe disease). For the subgroup analyses, additional endpoints included percent improvement in EASI from baseline (EASI 50, EASI 75 and EASI 90).
This study reports p-values from a post-hoc analysis, which are nominal and unadjusted for multiple comparisons. The p-values comparing proportions of responders from the LEB and placebo groups were calculated using Cochran–Mantel–Haenszel (CMH) tests adjusted by study (ADvocate1 vs ADvocate2), geographic region (US vs EU vs rest of world), age (adolescents vs adults), and baseline disease severity (IGA 3 vs 4). Data after the use of rescue medication or discontinuation of treatment due to lack of efficacy were set to baseline value; remaining missing data were imputed using multiple imputation (Appendix S1). Statistical tests were two-sided and evaluated at a significance level of 0.05. To explore potential effect modification by subgroup, interactions between treatment and subgroup were evaluated using logistic regression models that included treatment, subgroup, treatment-by-subgroup interactions and study as factors. Considering the low statistical power to detect interaction, the significance level for interaction was set at 0.1.
Week-52 analysis
Week-52 analysis involved the maintenance period and examined two subsets of patients from the pooled mITT population who received LEB during induction: week-16 LEB EASI 75 responders and week-16 LEB per-protocol non-responders. For week-16 responders, data were assessed across the two LEB treatment arms and the withdrawal arm. For week-16 non-responders, data from the escape arm were assessed. Efficacy endpoints were proportions of patients achieving EASI≤7, ≤5, ≤3 or ≤1 by week 52. No p-values were calculated; instead, data were analysed using descriptive statistics.
Week-16 EASI 75 LEB responders who received systemic rescue medication, discontinued treatment due to lack of efficacy or transferred to the escape arm had values set to baseline after that time point through week 52. Those who received topical rescue medication or discontinued treatment for other reasons had values set to “missing” after that time point through week 52. Multiple imputation was used to handle missing data (Appendix S1). For week-16 LEB non-responders, data were presented as observed cases, with no imputation for missing data.
All analyses were performed using Statistical Analysis System (SAS) software (version 9.4; SAS Institute, Inc.).
RESULTS
Baseline characteristics
The analysis of the induction period involved the pooled mITT population, which comprised 851 patients who received either LEB 250 mg Q2W (n=564) or placebo (n=287). The analysis of the maintenance period involved week-16 LEB EASI 75 responders (n=284) and week-16 LEB non-responders (n=215) (Table I). At baseline, mean EASI ranged from 29.3 to 30.3, mean body surface area involvement ranged from 45.7% to 46.9%, and between 38.0% and 38.8% of patients had an IGA score of 4.
Table I. Patient sample characteristics
| 16 week induction period | 36 week maintenance period | |||||
|---|---|---|---|---|---|---|
| Pooled mITT population (n=851)a | Week-16 LEB EASI 75 responders (n=284) | Week-16 per-protocol non-responders (n=215) | ||||
| Characteristic | LEB 250 mg Q2W (n=564) | PBO (n=287) | LEB 250 mg Q4W (n=115) | LEB 250 mg Q2W (n=112) | LEB withdrawal (n=57) | LEB Q2W (n=215) |
| Age, mean (SD) | 36.4 (17.3) | 34.8 (16.8) | 35.8 (17.3) | 35.9 (17.0) | 33.8 (16.9) | 36.6 (17.3) |
| Female, n (%) | 277 (49.1) | 148 (51.6) | 67 (58.3) | 52 (46.4) | 34 (59.7) | 88 (40.9) |
| Race, n (%) | ||||||
| White | 364 (64.5) | 178 (62.0) | 84 (73.0) | 80 (71.4) | 32 (56.1) | 124 (57.7) |
| Asian | 117 (20.7) | 75 (26.1) | 17 (14.8) | 19 (17.0) | 13 (22.8) | 58 (27.0) |
| Black | 58 (10.3) | 26 (9.1) | 12 (10.4) | 9 (8.0) | 8 (14.0) | 23 (10.7) |
| Otherb | 25 (4.4) | 8 (2.8) | 2 (1.7) | 4 (3.6) | 4 (7.0) | 10 (4.7) |
| Years since AD diagnosis, mean (SD) | 21.4 (15.0) | 21.9 (14.9) | 22.3 (14.6) | 21.5 (14.2) | 19.7 (14.8) | 21.9 (15.3) |
| EASI, mean (SD) | 29.3 (11.6) | 30.3 (11.9) | 28.9 (12.6) | 29.6 (10.8) | 28.8 (11.0) | 29.9 (11.4) |
| IGA, n (%) | ||||||
| 3 (moderate) | 345 (61.2) | 178 (62.0) | 76 (66.1) | 70 (62.5) | 36 (63.2) | 119 (55.3) |
| 4 (severe) | 219 (38.8) | 109 (38.0) | 39 (33.9) | 42 (37.5) | 21 (36.8) | 96 (44.7) |
| BSA % involvement, mean (SD) | 45.7 (22.5) | 46.9 (22.5) | 44.2 (23.3) | 45.5 (20.6) | 42.6 (21.9) | 47.6 (23.3) |
|
a Pooled from the ADvocate1 ITT population and the ADvocate2 mITT population, the latter of which excluded 18 patients from a single site because their eligibility could not be confirmed. b Includes American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, Other, Multiple, and Not Reported. AD:atopic dermatitis; BSA:body surface area; EASI:Eczema Area and Severity Index; IGA:Investigator’s Global Assessment; ITT:intent-to-treat; LEB:lebrikizumab; mITT:modified intent-to-treat; PBO:placebo; Q2W:every two weeks; Q4W:every four weeks; SD:standard deviation. |
||||||
Among patients with very severe baseline EASI, there was a slight imbalance between the proportion of female patients in the LEB subgroup (28.6%) vs the placebo subgroup (43.5%), likely due to the small sample sizes (Table SI).
Week-16 response rates
During induction, a significant treatment effect (i.e. difference between proportions of LEB and placebo responders) was observed. Higher percentages of patients in the LEB group than in the placebo group achieved all four absolute EASI responses (Fig. 1). At week 16, 56.7% of patients receiving LEB achieved EASI≤7, 50.1% achieved EASI≤5, 37.5% achieved EASI≤3, and 21.2% achieved EASI≤1. By contrast, no more than 20.0% of patients receiving placebo achieved any absolute EASI response. Significant differences between the LEB and placebo groups were observed as early as week 4 and were sustained throughout induction.
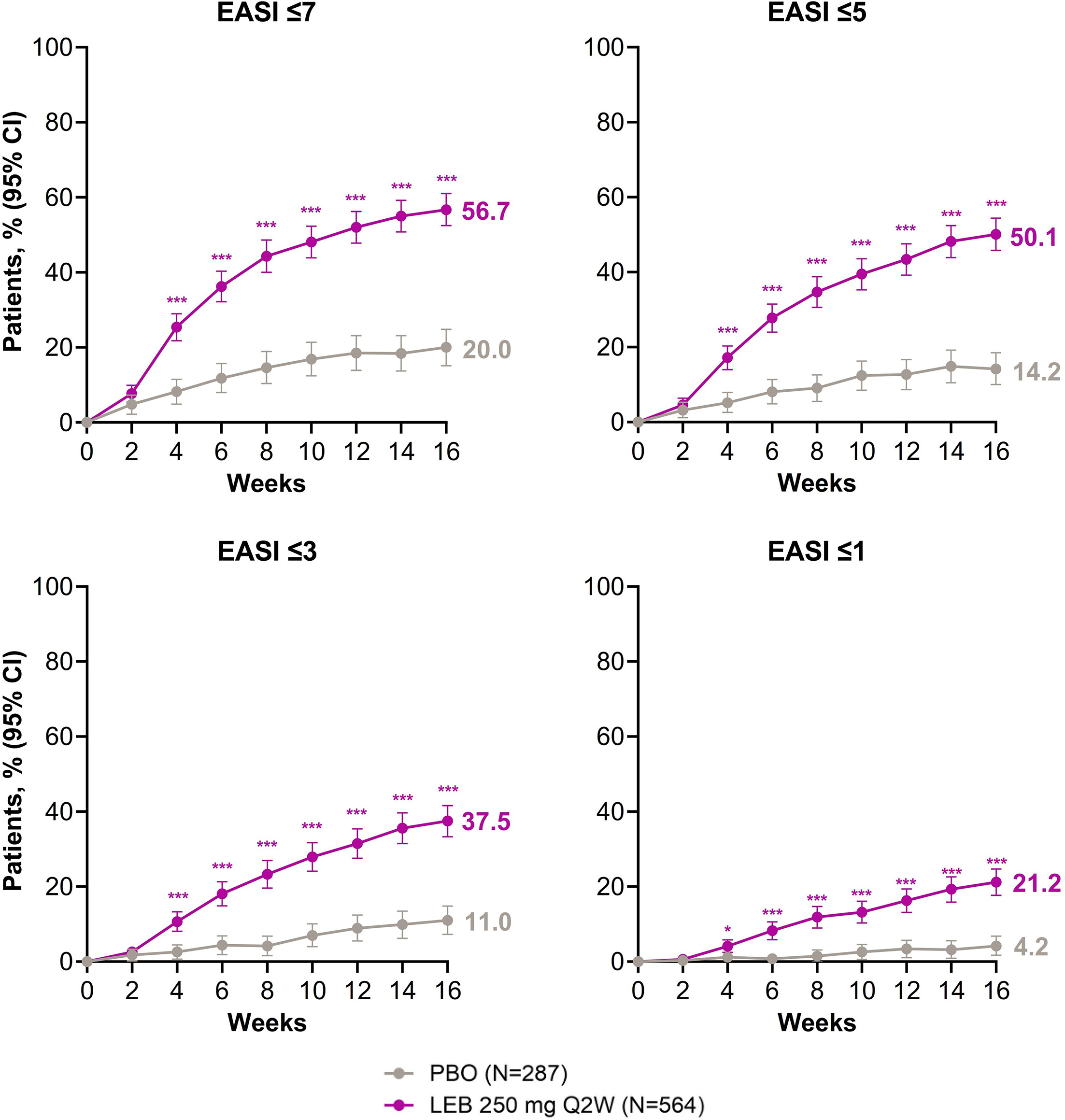
Fig. 1. Week-16 absolute EASI response rates, LEB vs PBO. Each chart shows EASI response rates in the LEB 250 mg Q2W (purple) group vs the PBO (grey) group, with p<0.001 for all week-16 comparisons. Data after the use of rescue medication or discontinuation of treatment due to lack of efficacy were set to baseline value; remaining missing data were imputed using multiple imputation. Statistical tests were two-sided and were evaluated at a significance level of 0.05 using SAS software, version 9.4. Abbreviations: CI, confidence interval; EASI, Eczema Area and Severity Index; LEB, lebrikizumab; PBO, placebo; Q2W, every 2 weeks; SAS, Statistical Analysis System. *p<0.05; **p<0.01; ***p<0.001.
Across the moderate (EASI 16–21), severe (EASI 21.1–50) and very severe (EASI>50) baseline EASI subgroups, significantly higher percentages receiving LEB than placebo achieved each absolute EASI response (Fig. 2) at week 16. The treatment effect was generally consistent across subgroups but appeared to be larger in the more severe baseline EASI subgroups (p-values for interaction were <0.1 for EASI≤7, EASI≤3, and EASI≤1 thresholds). In both baseline IGA subgroups, significantly higher percentages of patients receiving LEB than placebo achieved each absolute EASI response (Fig. 3). These treatment effects appeared to be comparable regardless of baseline severity as measured by IGA scores (p-values for interaction were >0.1 for all absolute EASI thresholds).
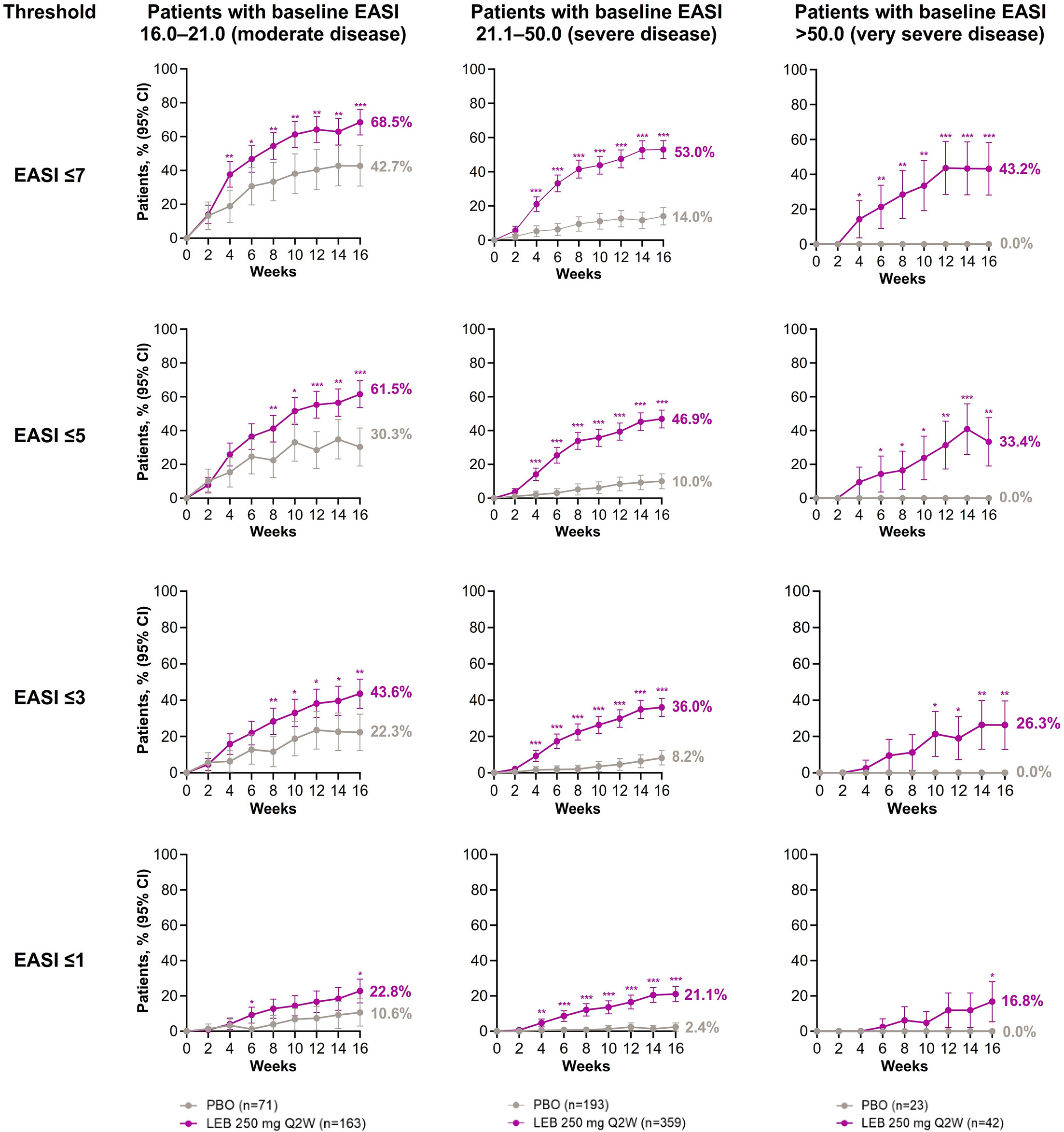
Fig. 2. Week-16 absolute EASI response rates by baseline EASI, LEB vs PBO. Each chart compares EASI response rates by baseline EASI in the LEB 250 mg Q2W group (purple) vs PBO group (grey). Data after the use of rescue medication or discontinuation of treatment due to lack of efficacy were set to baseline value; remaining missing data were imputed using multiple imputation. Statistical tests were two-sided and were evaluated at a significance level of 0.05 using SAS software, version 9.4. Abbreviations: CI, confidence interval; EASI, Eczema Area and Severity Index; LEB, lebrikizumab; PBO, placebo; Q2W, every 2 weeks; SAS, Statistical Analysis System. *p<0.05; **p<0.01; ***p<0.001.
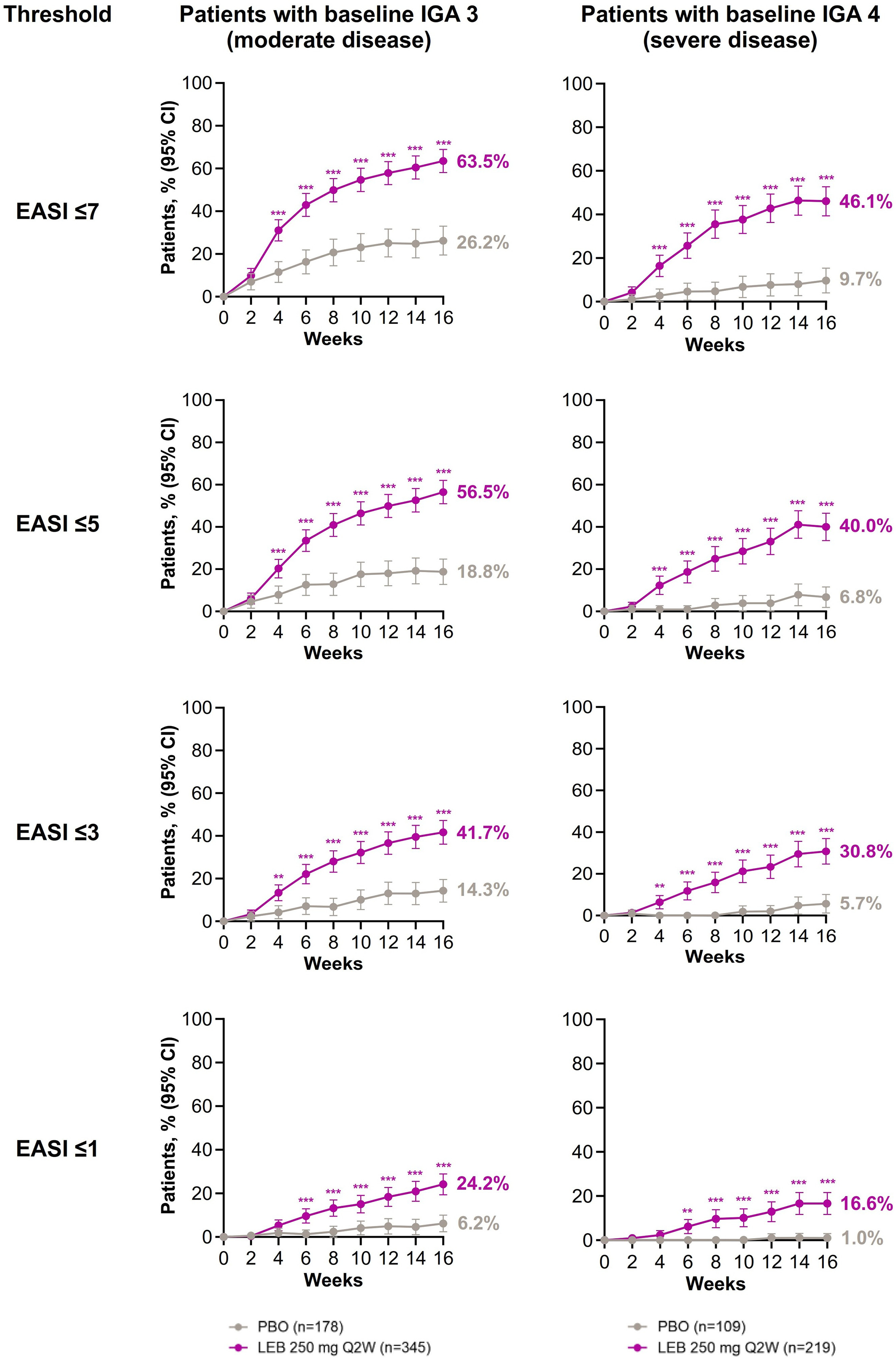
Fig. 3. Week-16 absolute EASI response rates by baseline IGA score, LEB vs PBO. Each chart shows EASI response rates by baseline IGA score in the LEB 250 mg Q2W group (purple) vs the PBO group (grey). Data after the use of rescue medication or discontinuation of treatment due to lack of efficacy were set to baseline value; remaining data were imputed using multiple imputation. Statistical tests were two-sided and were evaluated at a significance level of 0.05 using SAS software, version 9.4. Abbreviations: CI, confidence interval; EASI, eczema area and severity index; IGA, investigator’s Global Assessment; LEB, lebrikizumab; PBO, placebo; Q2W, every 2 weeks; SAS, Statistical Analysis System. *p<0.05; **p<0.01; ***p<0.001.
Additionally, across moderate, severe and very severe baseline EASI subgroups, significantly higher percentages of patients receiving LEB than placebo achieved percent EASI improvement thresholds (EASI 50, EASI 75 and EASI 90) at week 16 (Fig. S1). Treatment effect appeared to be greater in patients with baseline severe or very severe disease than with moderate disease (p-values for interaction were <0.1 for EASI 50 endpoint and <0.05 for EASI 75 and EASI 90 endpoints). Across the moderate and severe baseline IGA score subgroups, significantly higher percentages of patients receiving LEB than placebo achieved percent EASI improvement thresholds (Fig. S2). The treatment effect was comparable in both baseline IGA subgroups (p-values for interaction were >0.1 for all percent EASI improvement endpoints).
Week-52 response rates
Among week-16 LEB EASI 75 responders (n=284), high rates of absolute EASI responses were generally sustained throughout maintenance (Fig. 4). At week 52, EASI≤7 response rates were 83.7% for LEB Q4W patients, 75.7% for LEB Q2W patients, and 67.7% for LEB withdrawal patients. EASI≤5 response rates were 77.0% for LEB Q4W patients, 70.7% for LEB Q2W patients, and 62.1% for LEB withdrawal patients. EASI≤3 response rates were 66.9% for LEB Q4W patients, 64.8% for LEB Q2W patients, and 49.5% for LEB withdrawal patients. Finally, from week 16 to week 52, EASI≤1 response rates increased for LEB Q4W patients (45.5%) and LEB Q2W patients (49.9%) but were largely stable for LEB withdrawal patients (26.6%). Among all week-16 LEB responders, 15.1% used rescue medication and 13.7% used topical therapy, with 11.3% using topical corticosteroids. Thus, 84.9% received strictly LEB monotherapy.
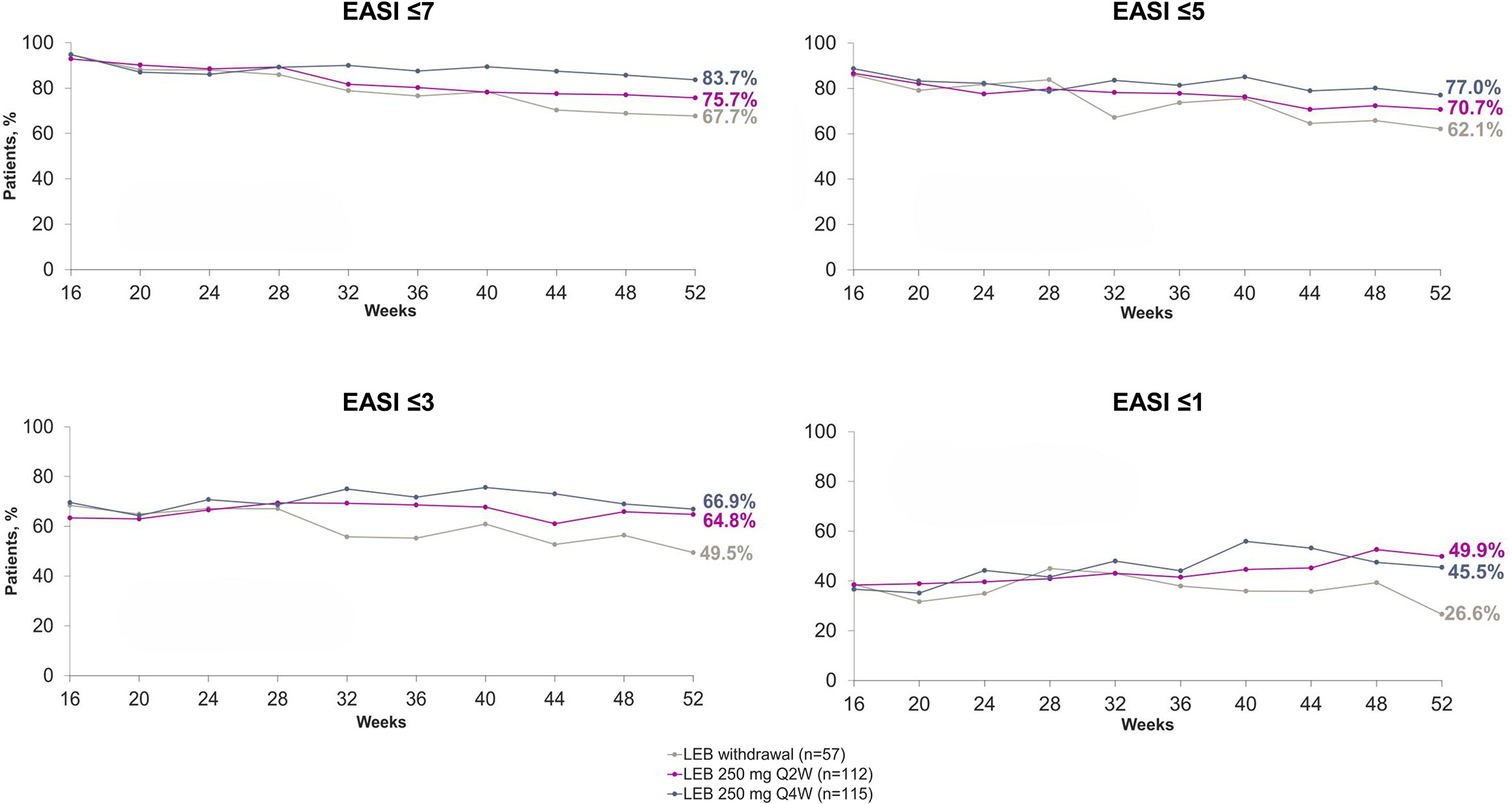
Fig. 4. Response rates at week 52 among week-16 EASI 75 LEB responders. Each chart compares EASI response rates among week-16 EASI 75 LEB responders who were re-randomized into two LEB treatment arms and one LEB withdrawal arm. Data from weeks 16–52 are provided. Week-16 EASI 75 LEB responders who received systemic rescue medication, discontinued treatment due to lack of efficacy or transferred to the escape arm had values set to their baseline value after that time point through week 52. Those who received topical rescue medication or discontinued treatment for other reasons had values set to “missing” after that time point through week 52. Multiple imputation was used to handle missing data. Abbreviations: EASI, eczema area and severity index; LEB, lebrikizumab; Q2W, every 2 weeks; Q4W, every 4 weeks.
Among week-16 LEB non-responders (n=215) assigned to the escape arm during maintenance, all absolute EASI response rates increased (Fig. S3). Of them, 29.3% used rescue medication and 28.8% used topical therapy, with 27.9% using topical corticosteroids.
DISCUSSION
This post-hoc analysis investigated absolute EASI response rates in adults and adolescents with moderate-to-severe AD treated with LEB for up to 1 year. At week 16, across baseline EASI subgroups and baseline IGA score subgroups, significantly higher percentages of absolute EASI response were identified in patients receiving LEB vs placebo. Through week 52, most absolute EASI response rates remained stable among week-16 LEB EASI 75 responders, while rates increased among week-16 LEB non-responders receiving LEB 250 mg Q2W in the escape arm. LEB therapy was associated with high rates of absolute EASI responses and durable improvements, even in cases of severe/very severe disease or where initial treatment outcomes were not optimal.
Week-16 results show that LEB monotherapy was significantly associated with improved disease severity in the induction period. Most patients receiving LEB achieved EASI≤7, representing mild disease or better, and 21.2% receiving LEB (vs 4.2% receiving placebo) achieved EASI≤1, indicating clear/almost clear skin. Across baseline EASI subgroups and IGA score subgroups, significantly higher percentages of patients receiving LEB than placebo achieved absolute EASI responses, with substantial treatment effect and little/no placebo effect observed in patients with more severe baseline disease. Additionally, similar patterns were seen with percent improvement in EASI (EASI 50, EASI 75 and EASI 90): across baseline EASI subgroups, LEB was associated with consistent and robust efficacy of skin improvement, with greater improvements in patients with more severe baseline disease; across IGA score subgroups, LEB was associated with treatment efficacy regardless of baseline severity. Whereas previous studies exclusively explored percent improvement in EASI resulting from LEB monotherapy (9, 10, 11), the present analysis of absolute EASI responses by different thresholds reveals that optimal therapeutic targets were met across a broad spectrum of baseline severities, reflecting clinically meaningful improvements achieved with LEB monotherapy within the induction period.
Week-52 results suggest that absolute EASI responses achieved during induction were durable in the maintenance period. High percentages of week-16 EASI 75 LEB responders achieved EASI≤7, ≤5 or ≤3 through week 52, with only minor differences between the treatment arms and LEB withdrawal arm; for EASI≤1, denoting clear or almost clear skin, the treatment arms saw slight increases through week 52, while the LEB withdrawal arm was stable. Rates of rescue medication use were low, with 84.9% of week-16 EASI 75 LEB responders receiving strictly LEB monotherapy during maintenance. Per the study design, durability was assessed only in week-16 EASI 75 LEB responders who underwent re-randomization; results should be interpreted accordingly. Results suggest that improvements during LEB Q2W monotherapy may be maintained with longer approved dosing intervals such as Q4W, which may be more convenient for patients than stricter regimens. Results align with previous findings on percent improvement in EASI among week-16 LEB responders, which showed higher rates of EASI 75 in the treatment arms than the withdrawal arm and suggested induction LEB Q2W followed by maintenance LEB Q4W can be sufficient to sustain a response in patients with moderate-to-severe AD (9).
Week-52 results further show that patients with high absolute EASI after induction often saw reductions with continued treatment. High percentages of week-16 LEB non-responders receiving LEB 250 mg Q2W in the escape arm achieved EASI ≤7, ≤5 or ≤3 during maintenance. Results align with a previous analysis showing percent EASI improvement in week-16 non-responders who received continued treatment (12). Moreover, limited use of rescue medication among week-16 LEB non-responders (29.3%) further supports the efficacy of LEB monotherapy. These findings indicate potential benefits from continued LEB therapy (alongside intermittent topical medications as deemed appropriate by the physician) for patients with suboptimal outcomes after 16 weeks.
A strength of this study was analysing absolute EASI responses in addition to percent improvements, affording insights that studies of percent improvement in EASI alone may not provide. Therapeutic targets (e.g. EASI≤7) were achieved during induction at significantly higher rates than placebo across severity levels: moderate, severe and very severe baseline EASI, as well as moderate and severe baseline IGA scores. As absolute EASI responses are increasingly featured in treat-to-target recommendations in Europe especially (15, 17), these data provide valuable insights to help physicians select treatment goals. Absolute Psoriasis Area and Severity Index scores were similarly studied and shown to represent meaningful improvement in patients with moderate-to-severe plaque psoriasis (18). Moreover, analysing results from the induction and maintenance periods as well as from both week-16 EASI 75 LEB responders and non-responders afforded a comprehensive view of LEB therapy, including how suboptimal initial outcomes were improved with continued treatment. Another strength was the large sample pooled from two major trials involving LEB monotherapy. While intermittent topical rescue medications for AD were permitted during maintenance, 84.9% of week-16 LEB responders received no rescue medications, and 88.7% received no topical corticosteroids. No topical or systemic treatments apart from LEB were permitted during induction. Thus, our results strongly represent the clinical profile of LEB monotherapy and cannot be attributed to combination therapies with topicals.
One study limitation involved the use of post-hoc analyses with multiple endpoints and subgroup comparisons. All p-values reported are nominal and unadjusted for multiple comparisons, and statistical significance should be interpreted with caution. Additionally, though repeated measurements were available, longitudinal modelling was not performed. Instead, this analysis aimed to estimate visit-specific treatment effects; results should be interpreted in this context.
In this post-hoc analysis, LEB therapy was significantly associated with high rates of absolute EASI response and high rates of percent improvement in EASI, in adults and adolescents with moderate-to-severe AD. This was evident across disease severities as measured by baseline EASI and IGA scores. Furthermore, patients improved over time: continued LEB therapy was associated with high rates of absolute EASI response. Results suggest that LEB therapy may lead to durable EASI responses and that continued LEB therapy has potential clinical benefits for improving disease severity. Our analysis complements previous analyses of percent improvement in EASI, providing clinically important information to help physicians assess current disease status, follow treat-to-target recommendations and tailor appropriate treatments for each patient.
ACKNOWLEDGEMENTS
Eli Lilly and Company and Almirall, S.A. extend their gratitude to the clinical trial participants and their caregivers, whose participation and contributions made this work possible. Medical writing was provided in accordance with Good Publication Practice guidelines by Adam Fix, PhD (PPD clinical research business of Thermo Fisher Scientific) and was paid for by Eli Lilly and Company. Data in this study were previously presented in posters at the European Academy of Dermatology and Venereology (EADV) annual congress, 2023 and 2024.
REFERENCES
- Sacotte R, Silverberg JI. Epidemiology of adult atopic dermatitis. Clin Dermatol 2018; 36: 595–605. https://doi.org/10.1016/j.clindermatol.2018.05.007
- Weidinger S, Novak N. Atopic dermatitis. Lancet 2016; 387: 1109–1122. https://doi.org/10.1016/S0140-6736(15)00149-7
- Bylund S, Kobyletzki LB, Svalstedt M, Svensson Å. Prevalence and incidence of atopic dermatitis: a systematic review. Acta Derm Venereol 2020; 100: adv00160. https://doi.org/10.2340/00015555-3510
- Drucker AM, Lam M, Elsawi R, Prieto-Merino D, Malek R, Ellis AG, et al. Comparing binary efficacy outcomes for systemic immunomodulatory treatments for atopic dermatitis in a living systematic review and network meta-analysis. Br J Dermatol 2024; 190: 184–190. https://doi.org/10.1093/bjd/ljad393
- Silverberg JI, Boguniewicz M, Hanifin J, Papp KA, Zhang H, Rossi AB, et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis is efficacious regardless of age of disease onset: a post hoc analysis of two phase 3 clinical trials. Dermatol Ther (Heidelb) 2022; 12: 2731–2746. https://doi.org/10.1007/s13555-022-00822-x
- Silverberg JI, Thyssen JP, Fahrbach K, Mickle K, Cappelleri JC, Romero W, et al. Comparative efficacy and safety of systemic therapies used in moderate-to-severe atopic dermatitis: a systematic literature review and network meta-analysis. J Eur Acad Dermatol Venereol 2021; 35: 1797–1810. https://doi.org/10.1111/jdv.17351
- Evaluation of the Efficacy and Safety of Lebrikizumab (LY3650150) in Moderate to Severe Atopic Dermatitis. National Library of Medicine; 2022. Available from: https://clinicaltrials.gov/study/NCT04146363]
- Evaluation of the Efficacy and Safety of Lebrikizumab (LY3650150) in Moderate to Severe Atopic Dermatitis. National Library of Medicine; 2023. Available from: https://clinicaltrials.gov/study/NCT04178967]
- Blauvelt A, Thyssen JP, Guttman-Yassky E, Bieber T, Serra-Baldrich E, Simpson E, et al. Efficacy and safety of lebrikizumab in moderate-to-severe atopic dermatitis: 52-week results of two randomized double-blinded placebo-controlled phase III trials. Br J Dermatol 2023; 188: 740–748. https://doi.org/10.1093/bjd/ljad022
- Silverberg JI, Guttman-Yassky E, Thaçi D, Irvine AD, Stein Gold L, Blauvelt A, et al. Two phase 3 trials of lebrikizumab for moderate-to-severe atopic dermatitis. N Engl J Med 2023; 388: 1080–1091. https://doi.org/10.1056/NEJMoa2206714
- Simpson E, Fernández-Peñas P, de Bruin-Weller M, Lio PA, Chu CY, Ezzedine K, et al. Improvement across dimensions of disease with lebrikizumab use in atopic dermatitis: two phase 3, randomized, double-blind, placebo-controlled monotherapy trials (ADvocate1 and ADvocate2). Adv Ther 2025; 42: 132–143. https://doi.org/10.1007/s12325-024-02974-y
- Guttman-Yassky E, Rosmarin D, de Bruin-Weller M, Weidinger S, Bieber T, Hong HCH, et al. The efficacy of longer-term lebrikizumab treatment in patients with moderate-to-severe atopic dermatitis who did not meet protocol-defined response criteria at week 16 in 2 randomized controlled clinical trials. J Am Acad Dermatol 2025; 92: 1024–1031. https://doi.org/10.1016/j.jaad.2024.12.026
- Hanifin JM, Baghoomian W, Grinich E, Leshem YA, Jacobson M, Simpson EL. The Eczema area and severity index-A practical guide. Dermatitis 2022; 33: 187–192. https://doi.org/10.1097/DER.0000000000000895
- Leshem YA, Hajar T, Hanifin JM, Simpson EL. What the Eczema area and severity index score tells us about the severity of atopic dermatitis: an interpretability study. Br J Dermatol 2015; 172: 1353–1357. https://doi.org/10.1111/bjd.13662
- Silverberg JI, Gooderham M, Katoh N, Aoki V, Pink AE, Binamer Y, et al. Combining treat‐to‐target principles and shared decision‐making: International expert consensus‐based recommendations with a novel concept for minimal disease activity criteria in atopic dermatitis. Acad Dermatol Venereol 2024; 38: 2139–2148. https://doi.org/10.1111/jdv.20229
- Schram ME, Spuls PI, Leeflang MMG, Lindeboom R, Bos JD, Schmitt J. EASI, (objective) SCORAD and POEM for atopic eczema: responsiveness and minimal clinically important difference. Allergy 2012; 67: 99–106. https://doi.org/10.1111/j.1398-9995.2011.02719.x
- Yeung J, Gooderham MJ, Hong HCH, Lynde C, Prajapati VH, Lansang P, et al. Treat-to-target in the management of moderate-to-severe atopic dermatitis in adults: a Canadian perspective. J Am Acad Dermatol 2023; 89: 372–375. https://doi.org/10.1016/j.jaad.2023.01.053
- Puig L, Dossenbach M, Berggren L, Ljungberg A, Zachariae C. Absolute and relative psoriasis area and severity indices (PASI) for comparison of the efficacy of ixekizumab to etanercept and placebo in patients with moderate-to-severe plaque psoriasis: an integrated analysis of UNCOVER-2 and UNCOVER-3 outcomes. Acta Derm Venereol 2019; 99: 971–977. https://doi.org/10.2340/00015555-3245
- Thyssen JP, Bieber T, Kleyn CE, Nosbaum A, Grond S, Petto H, et al. Baricitinib provides rapid and sustained improvements in absolute EASI and SCORAD outcomes in adults with moderate-to-severe atopic dermatitis. J Dermatolog Treat 2023; 34: 2216322. https://doi.org/10.1080/09546634.2023.2216322
- Silverberg JI, Lei D, Yousaf M, Janmohamed SR, Vakharia PP, Chopra R, et al. What are the best endpoints for Eczema area and severity index and scoring atopic dermatitis in clinical practice? A prospective observational study*. Br J Dermatol 2021; 184: 888–895. https://doi.org/10.1111/bjd.19457
- Long-term Safety and Efficacy Study of Lebrikizumab (LY3650150) in Participants With Moderate-to-Severe Atopic Dermatitis (ADjoin). National Library of Medicine; 2025. Available from: https://clinicaltrials.gov/study/NCT04392154]
- Guttman-Yassky E, Weidinger S, Simpson EL, Gooderham M, Irvine AD, Spelman L, et al. Two-year efficacy and safety of lebrikizumab in patients with moderate-to-severe atopic dermatitis: a long-term extension (ADjoin). Dermatol Ther (Heidelb) 2025; 15: 2217–2232. https://doi.org/10.1007/s13555-025-01452-9
- Eichenfield LF, Tom WL, Chamlin SL, Feldman SR, Hanifin JM, Simpson EL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol 2014; 70: 338–351. https://doi.org/10.1016/j.jaad.2013.10.010