SHORT COMMUNICATION
Verrucous Venous Malformation Presenting on the Face: A Case Series of Two Patients
Shih-Jen CHANG1†, Luyujie HUANG1†![]() , Lizhen WANG2, Xiaoxi LIN1* and Yajing QIU1*
, Lizhen WANG2, Xiaoxi LIN1* and Yajing QIU1*
1Department of Plastic and Reconstructive Surgery, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, and 2Department of Oral Pathology, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China. *Emails: linxiaoxi@126.com; hedwig_qiu@live.cn
†These authors contributed equally to this work as co-first authors.
Citation: Acta Derm Venereol 2025; 106: adv-2025-0285. DOI: https://doi.org/10.2340/actadv.v106.adv-2025-0285.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Dec 21, 2025. Accepted after revision: Apr 22, 2026.
Published: May 21, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
This work is supported by the National Natural Science Foundation of China (82272288), Project of Biobank from Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine (YBKA202209), Project of the Vascular Anomalies Specialty Cohort from Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine (2025DLB01), and the AI for Science Seed Program of Shanghai Jiao Tong University (2025AI4S-HY03).
Institutional ethical committee approval for the use and study of complicated vascular malformation specimens was obtained (SH9H2024-T464-1).
Verrucous venous malformation (VVM) is a rare and progressive form of congenital vascular malformation, typically with a predilection for the limbs (1). While extremity involvement is widely documented, occurrences in atypical anatomical sites such as the face remain underreported and poorly characterized. Herein, we present a new subtype of VVMs located in the facial region, which often involve delicate anatomy and pose substantial anaesthetic challenges.
CASE PRESENTATION
A 26-year-old female was referred to our medical centre in 2022, with a history of congenital purple lesions on her forehead and right eyelid. She complained the lesions had persisted in size, colour and general appearance since early childhood, with no regression (Fig. 1A). Approximately 4 years prior to medical consultation, the lesions began to develop subcutaneously, resulting in a heavy, droopy eyelid and occasional bleeding.
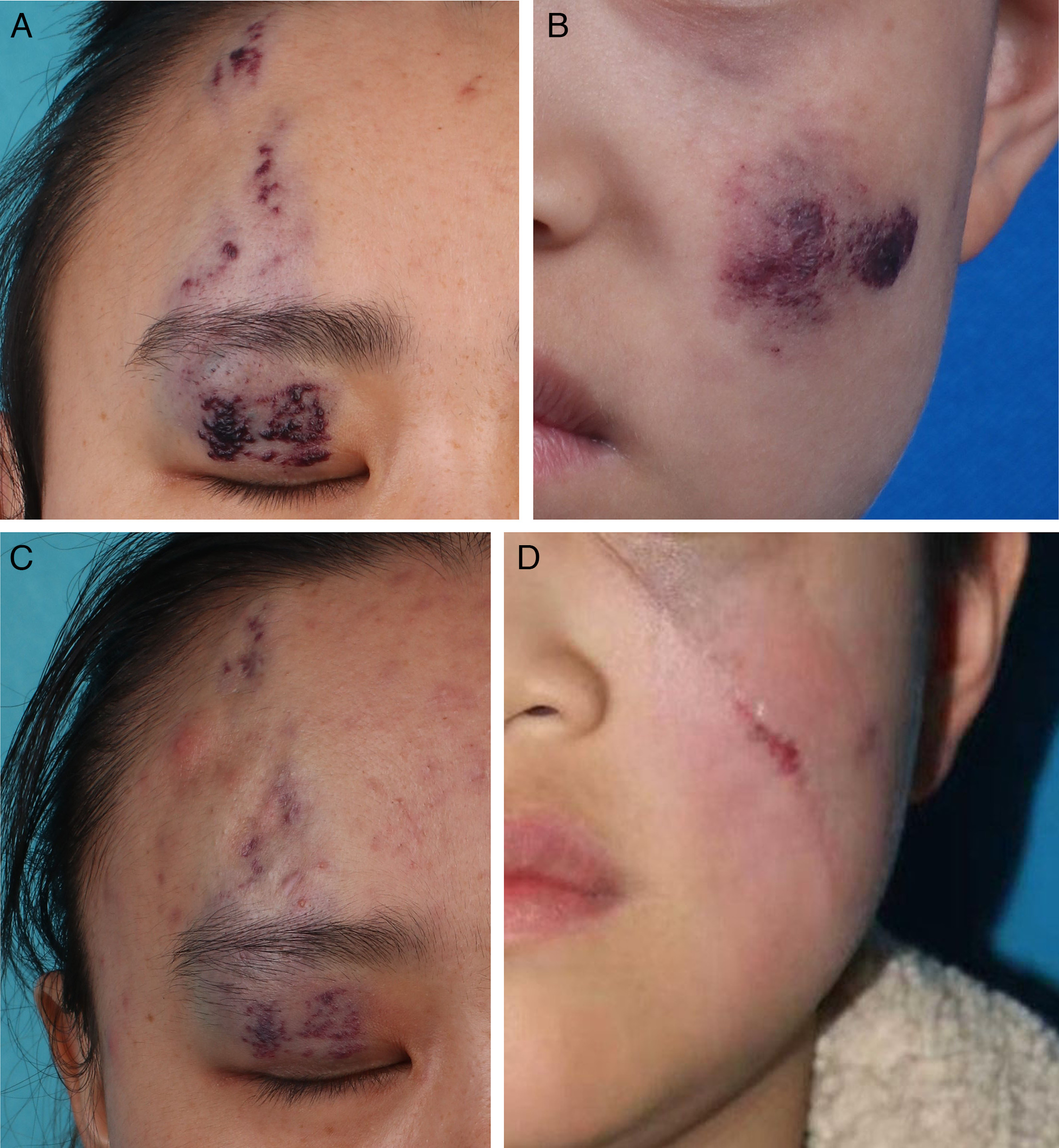
Fig. 1. Clinical presentation of verrucous venous malformation on facial regions. (A) A 26-year-old female with lesions on the right upper eyelid and forehead. (B) A 7-year-old boy with lesions on the left cheek. (C) Image of Fig.1A after surgical excision of subcutaneous mass under the upper eyelid, topical sirolimus on the superficial skin on the upper eyelid and laser therapy on the forehead. (D) Image of Fig. 1B after surgical excision of the facial lesion.
Physical examination showed hyperkeratotic lesions were discretely distributed on the forehead and the right upper eyelid with bluish patches indicating subcutaneous involvement. Magnetic resonance imaging (MRI) revealed patchy areas with low signal intensity on both T1- and T2-weighted images on the forehead, and a nodular area with slightly high T1 and heterogeneously high T2 signal on the right eyelid. Further contrast scan presented irregularly enhanced patchy areas with ill-defined margins on the forehead, and an unevenly enhanced nodule with well-defined borders on the eyelid. No intracranial abnormal signals were detected.
Treatments included an infrabrow incision to excise the subcutaneous mass in the eyelid without skin resection, followed by topical sirolimus for superficial eyelid. Lesions on the forehead were treated with laser therapy. These combined treatments brought effective remission of hyperkeratosis and restoration of smooth skin, indicating substantial clinical improvement (Fig. 1C).
Subsequent histopathological examination demon-strated hyperplasia and dilation of capillaries along with a smaller quantity of veins in subcutaneous tissue (Fig. 2A). Immunohistochemical staining showed negative GLUT-1 in endothelial cells and positive SMA in pericytes (Fig. 2B). Further Sanger sequencing of the resected specimen detected a missense mutation of MAP3K3 (NM_002401.3, c.1323C>G; NP_002392, p.Iso441Met) in this patient (Fig. 2C), confirming VVM diagnosis.
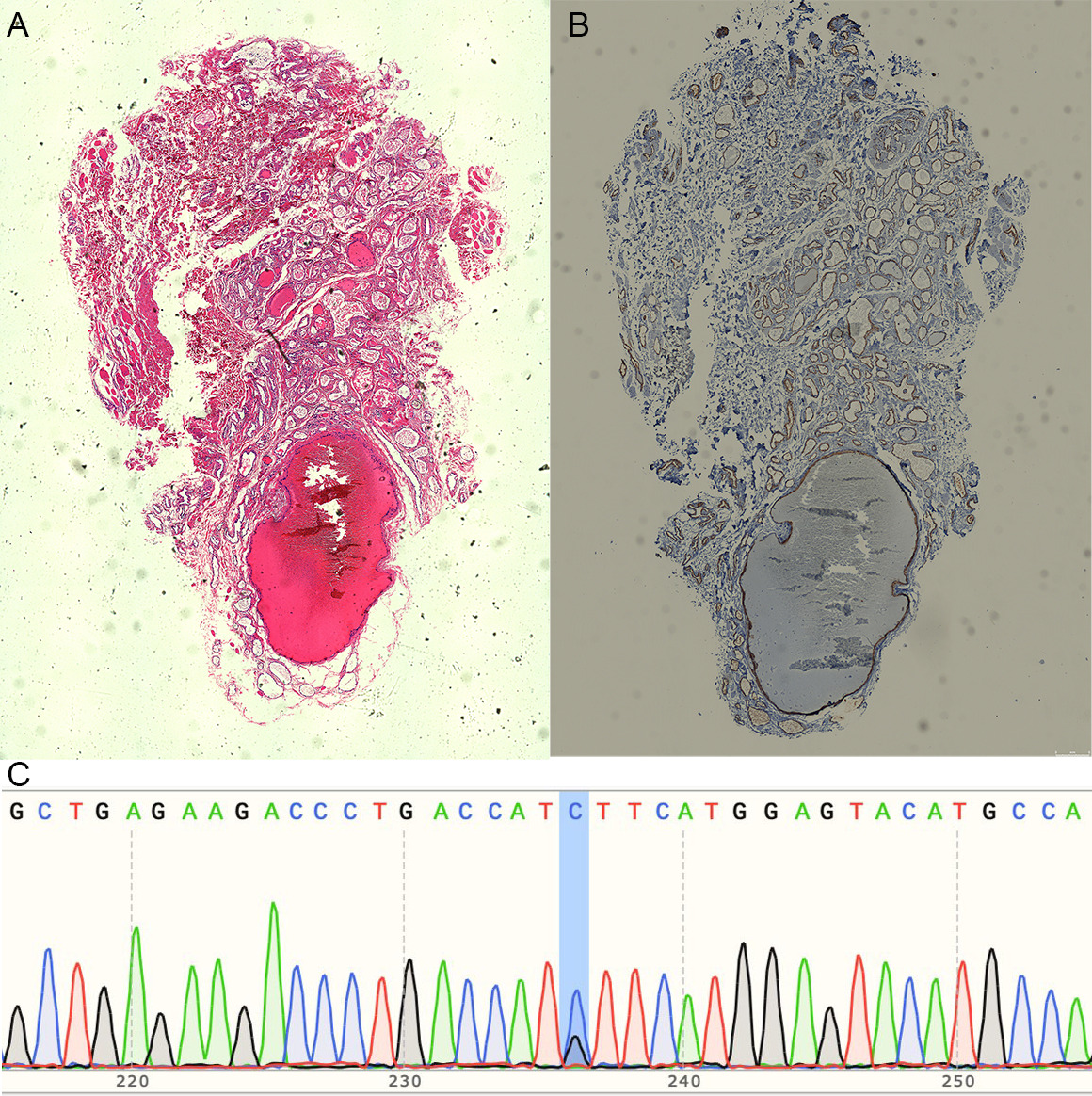
Fig. 2. Pathological examination and genetic detection of the 26-year-old female. (A) Hematoxylin–eosin staining showed hyperplasia and expanding veins in subcutaneous tissue.(B) Immunohistochemical staining for SMA showed positive in pericytes of expanding veins. (C) Sanger sequencing of resected specimen showed MAP3K3 mutation (c.1323C>G).
To determine whether this represented an isolated case and evaluate the prevalence of facial VVM lesions, we conducted a retrospective study in our vascular anomaly centre. We reviewed 155 cases with affirmative diagnosis in VVM cohort of Shanghai Ninth People’s Hospital from 2023 to 2,025. Among these data, we identified another one case presenting facial lesions.
The 2nd case is a 7-year-old boy with congenital red patch on left cheek, which increased proportionally as the child grew and progressed into focal hyperkeratosis, thick crusting and occasional ulceration (Fig. 1B). Surgical excision was performed to remove the lesion in the buccal region (Fig. 1D). Pathological examination demonstrated proliferating capillaries to venous channels. Immunohistochemical staining revealed strong positivity for CD31, CD34, ERG, partial positivity for VEGF, GLUT1 and D2-40, while being negative for WT-1, and a low Ki-67 proliferation index (<5%). Sanger sequencing of the resected specimen also detected the same MAP3K3 missense mutation (NM_002401.3, c.1323C>G; NP_002392, p.Iso441Met), further supporting VVM diagnosis.
DISCUSSION
VVM is a rare congenital venous malformation, which has a strong predilection for the limbs. Based on cohort data in our medical centre, we reviewed two cases of facial involvement, which have never been documented before, thereby expanding present anatomic spectrum of VVM. Diagnosis of VVM was established based on the triad of characteristic clinical presentation of persistent hyperkeratotic plaques, histopathological evidence of expanding vascular channels, and genetic confirmation of the recurrent MAP3K3 missense mutation (NM_002401.3, c.1323C>G; NP_002392, p.Iso441Met).
VVM preferentially involve the limbs, with only occasional cases reported in the oral cavity, penis or trunk (2, 3, 4). In our cohort of 155 cases, the prevalence of facial distribution is 1.29% (2/155), which is relatively lower than other anatomical regions. In contrast, sporadic venous malformation (VM), which is categorized as slow-flow venous malformation together with VVM (5), most commonly arises in the head and neck and can also occur on the limbs, where deeper extension into muscles or joints may lead to functional impairment, limb deformities and pain (6). And the pathognomonic mutation of MAP3K3 for VVM distinguishes its genetic origin from VM associated with mutations of TIE2 and PIK3CA (7, 8). These clinical and pathological characteristics suggest that they represent fundamentally different disease process.
Meanwhile, the management of facial VVM presents unique challenges, given the high aesthetic demands brought from social pressure of patients and the need to preserve delicate facial functions. The nature history of VVM typically presents as erythema progressing into hyperkeratosis (9). Surgical excision is first recommended for hyperkeratosis, while laser therapy is effective for erythema. Given the high-level aesthetic preservation for facial lesions, early diagnosis and treatment of erythematic VVM is essential for avoidance of facial incision therapy. Meanwhile, even if facial lesions have progressed as our 2 cases, surgical excision can remove subcutaneous mass and severe hyperkeratosis to restore facial skin, and laser therapy or topical sirolimus can be applied to more superficial lesions, which constitute a comprehensive and multimodal treatment strategy.
In conclusion, this study establishes a previously unrecognized facial involvement of VVM, thereby broadening its anatomic spectrum. This novel finding calls for a deeper investigation into its pathogenesis process and early diagnosis, as well as comprehensive consideration of multimodal therapy, particularly in aesthetically critical regions like the face.
REFERENCES
- Tennant LB, Mulliken JB, Perez-Atayde AR, Kozakewich HPW. Verrucous hemangioma revisited. Pediatr Dermatol 2006; 23: 208–215. https://doi.org/10.1111/j.1525-1470.2006.00219.x
- Dighe R, Aditya A, Mhapuskar A, Jathar M. Verrucous hemangioma of the oral cavity: a rare diagnostic dilemma. Indian J Dent Res 2015; 26: 644–647. https://doi.org/10.4103/0970-9290.176935
- Akyol I, Jayanthi VR, Luquette MH. Verrucous hemangioma of the glans penis. Urology 2008; 72: 230. https://doi.org/10.1016/j.urology.2007.11.120
- Hayashi H, Shimizu T, Nakamura H, Shimizu H. Linear verrucous haemangioma on the abdomen. Acta Derm Venereol 2003; 84: 79–80. https://doi.org/10.1080/00015550310020576
- ISSVA Classification of Vascular Anomalies ©2025. International Society for the Study of Vascular Anomalies; 2025.
- Steiner F, Taghavi K, FitzJohn T, Tan ST. Stratification and characteristics of common venous malformation by anatomical location. JPRAS Open 2017; 13: 29–40. https://doi.org/10.1016/j.jpra.2017.04.002
- Couto JA, Vivero MP, Kozakewich HPW, Taghinia AH, Mulliken JB, Warman ML, et al. A somatic MAP3K3 mutation is associated with verrucous venous malformation. Am J Hum Genet 2015; 96: 480–486. https://doi.org/10.1016/j.ajhg.2015.01.007
- Jiang X, Hu L, Lai J, Ge S, Chen H, Yang X, et al. Venous malformations: unraveling latest mechanisms and bridging gaps in targeted therapy development. Int J Biol Sci 2025; 21: 7013–7028. https://doi.org/10.7150/ijbs.122569
- Chang SJ, Sun J, Chen Q, Wang L, Lin X, Qiu Y. Diverse clinical course and features of verrucous venous malformation. J Am Acad Dermatol 2026; 94: 1543–1545. https://doi.org/10.1016/j.jaad.2026.01.020