ORIGINAL REPORT
European Expert Consensus on Essential Variables for Teledermatological Assessment of Skin Tumours
Alexander DETLEFSEN1*![]() , Tine VESTERGAARD1, Niels Kvorning TERNOV2, Lars KONGE3, Åsa INGVAR4, Kari NIELSEN4 and Kasper Bostlund ASSERSEN1*
, Tine VESTERGAARD1, Niels Kvorning TERNOV2, Lars KONGE3, Åsa INGVAR4, Kari NIELSEN4 and Kasper Bostlund ASSERSEN1*
1Department of Dermatology and Allergy Centre, Odense University Hospital, Odense, Denmark, 2Department of Plastic Surgery, Copenhagen University Hospital – Herlev and Gentofte, Copenhagen, Denmark, 3Copenhagen Academy for Medical Education and Simulation, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark, and 4Department of Dermatology, Skåne University Hospital Lund and Department of Clinical Sciences Lund, Dermatology, Lund University, Lund, Sweden
Corr: Alexander Detlefsen, Department of Dermatology and Allergy Centre, Odense University Hospital, Odense, Denmark and Kasper Bostlund Assersen. *Emails: alexanderdetlefsen@gmail.com; kasper_assersen@hotmail.com
Key words: Teledermatology; teledermoscopy; Delphi; consensus; skin tumours; referral standards.
Citation: Acta Derm Venereol 2026; 106: adv-2026-0512. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0512.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 17, 2026. Accepted after revision: Apr 22, 2026.
Published: May 21, 2026.
Competing interests and funding: The data that support the findings of this study are available from the corresponding author upon reasonable request.
This study was conducted in accordance with the Declaration of Helsinki. All participants provided signed informed consent prior to participation. The study was approved by the Executive Secretariat of the Region of Southern Denmark (J. no. 24/37691).
AD and LK declare no conflicts of interest. KBA educates psoriasis patients in the danish psoriasis association. KN has received speaker honoraria from Galderma Sweden, LEO Pharma Sweden, Novartis Sweden, and UCB Pharma Sweden, and has served as shared head of the National Guidelines for Cutaneous Melanoma in Sweden as well as head of the board of the Swedish Society for Dermatologic Surgery and Oncology (SDKO, 2023–2025). NKT reports stock ownership in Melatech ApS, a company providing a platform enabling dermatological eConsults. TV reports serving as PI on a hidradenitis suppurativa study sponsored by UCB Biosciences, receiving lecture fees from Novartis, and support for congress participation from Sanofi and AbbVie Denmark. She is also a board member of the Danish Melanoma Group and the Danish Skin Cancer Group. ÅI reports research collaborations with Omda/Dermicus on studies evaluating aspects of teledermoscopy. All authors have submitted the conflict-of-interest form.
Teledermatology is increasingly used for the assessment of suspicious skin tumours, yet referral content remains poorly standardized. To develop a European expert consensus on the essential clinical and visual variables required for teledermatological assessment of primary skin tumours. A 3-round modified Delphi study was conducted among experienced dermatologists. In round 1, participants proposed essential variables. In round 2, variables were rated for essentiality, clinical relevance and feasibility. In round 3, binary voting was used to define final consensus. Consensus was predefined as ≥67% agreement. Interquatile ranges were calculated to assess response stability. A total of 47 variables were proposed in round 1. Following quantitative scoring, 34 variables progressed to round 3. Twelve variables met the predefined consensus threshold, primarily related to image quality and lesion characteristics. Sensitivity analyses using geographic subgroups and higher consensus thresholds demonstrated that image-quality variables were the most robust. This European expert consensus defines a focused and clinically practical core dataset for teledermatological assessment of skin tumours. These variables may support standardization of referrals and facilitate future validation and AI-assisted workflows.
SIGNIFICANCE
Remote review of suspicious skin spots is growing, but the information sent with photos varies widely. We asked experienced skin specialists across Europe to agree on the small set of details and images that matter most. The result is a short checklist that can be built into electronic referrals and photo apps. Using it should make remote advice quicker and more reliable, reduce back-and-forth messages and help patients get the right appointment sooner. This is especially useful where specialist services are scarce. It may also cut unnecessary clinic visits and help find skin cancer earlier.
Skin cancer is a common malignancy with rising incidence globally (1). Among these, the highest incidence is found in keratinocyte carcinoma (KC) with~1.2 million new cases and melanoma with 0.3 million new cases each year globally (1). The increasing prevalence of primary skin cancer is believed to be driven by excessive ultraviolet exposure, increasing lifespan and improved early detection efforts (1, 2, 3, 4). Some lesions, particularly melanomas, are aggressive and require timely and accurate diagnosis (1). Patients are therefore referred to dermatologists for further assessment when general practitioners are unable to confidently rule out malignancy.
Use of diagnostic equipment such as dermoscopy has significantly improved the accuracy of melanoma diagnosis and KC (5). However, these benefits depend entirely on sufficient skills in using dermoscopy (6), which have been difficult to monitor (7). Consequently, the risk of error is substantial for the many inexperienced clinicians that either risks over-referral of many benign diseases, or more importantly, risks failing to refer a patient with skin malignancy. Therefore, teledermatology, especially teledermoscopy (TDS), has emerged as an effective tool to expand access to expertise and optimize patient care (8). TDS can reduce referral rates, speed up specialist input and cut costs while maintaining diagnostic performance comparable to face-to-face consultations (9, 10, 11). A prospective study in New Zealand found 88% of patients assessed via TDS avoided in-person follow-up, and 59% were dismissed without further intervention (12, 13). Patient satisfaction with TDS is typically high due to shorter wait times and reduced need for clinic visits (14, 15).
However, broader adoption remains limited by challenges including reimbursement, medico-legal issues, data privacy and integration into routine workflows (16). A fundamental obstacle to broader adoption of TDS is the lack of an international consensus on what constitutes a high-quality TDS referral (7). Many national guidelines overlap, on aspects such as patient history and lesion information but differ significantly in emphasis, some prioritize detailed patient history and clinical context ((e.g.) Australia (8)), others focus on dermoscopic image quality and lesion-specific data ((e.g.) UK (17)), while some, such as the US, emphasize flexibility, continuity of care and legal compliance (18). These discrepancies likely reflect differences in healthcare infrastructure, referral pathways, reimbursement models and TDS training among referring providers (19). As a result, there is a lack of consensus about which clinical and visual variables are essential for safe, effective and scalable TDS (8, 16, 17). Furthermore, skin tumours and inflammatory dermatoses require distinct diagnostic inputs, reinforcing the need for condition-specific rather than generic standards (7, 16).
Currently, no unified, expert-defined set of referral variables exists specifically for skin tumours in teledermatology, limiting interoperability and artificial intelligence integration. To address this gap, we utilized a modified Delphi method (20, 21) to establish international expert consensus on the essential clinical and visual variables for teledermatological referral of primary skin cancers.
METHODS
Study design
This study utilized a modified Delphi process to achieve expert consensus on the essential variables for teledermatological assessment of skin tumours. The Delphi method is a structured, iterative process designed to gather and refine expert opinions through multiple rounds of anonymous surveys (20, 21). The consensus process was conducted in 3 rounds, combining qualitative data collection and quantitative scoring. The process was designed to ensure anonymity and thereby minimize conformity bias. Inclusion criteria were applied after the 1st round to allow a broader collection of qualitative input before restricting the panel to those with substantial expertise in subsequent rounds. This approach ensured that round 1 captured a wide range of perspectives, while rounds 2 and 3 focused on building consensus among experienced experts. All responses from individuals not meeting the predefined criteria were excluded from further rounds, in line with recommended Delphi methodology (20, 21) (Fig. 1).
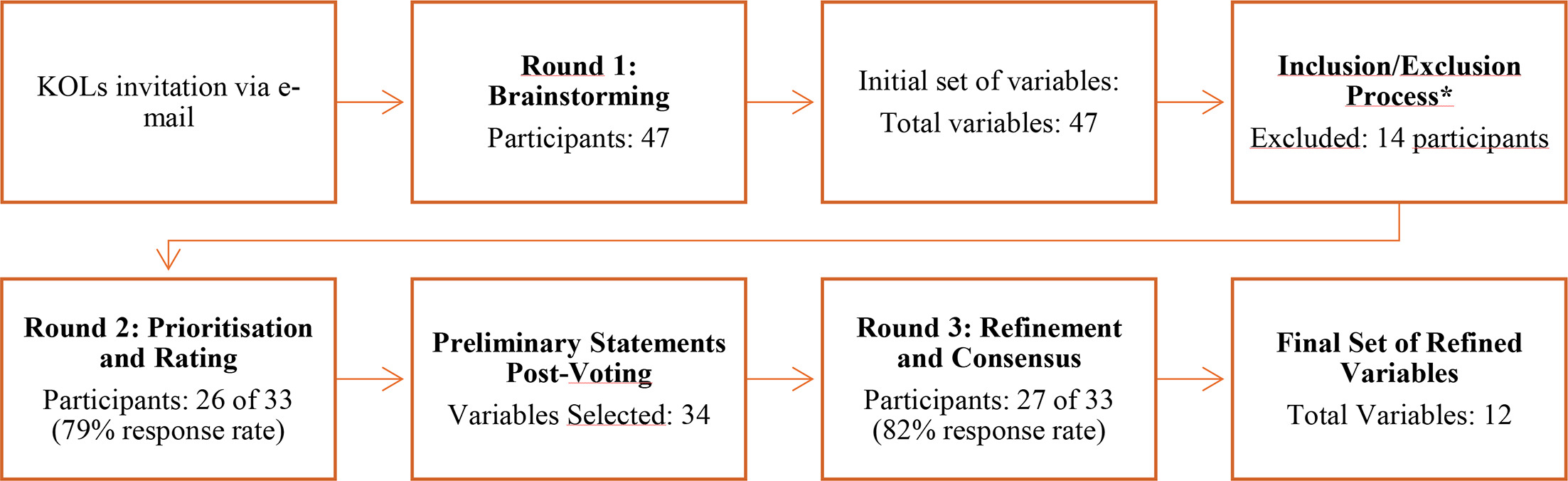
Fig. 1. Consensus study flowchart, key opinion leader (KOL) *: Participants were excluded after round 1 if they did not meet predefined eligibility criteria, ensuring only experienced experts participated in later rounds. See Method section.
Panel selection
Experts in dermatology and TDS were invited to participate in the Delphi process. Selection criteria required Key Opinion Leaders (KOLs) to meet all of the following requirements for inclusion:
A minimum of six years’ clinical experience in dermatology (20)
At least 100 TDS evaluations performed
Active involvement in teledermatological consultations and/or research
KOLs were recruited through professional networks, literature-based identification and snowball sampling, wherein initial participants were encouraged to invite additional experts to improve panel participation. The final panel was designed to include at least 15 dermatologists, in line with sample sizes used in previous Delphi studies in dermatology and telemedicine (20, 22). Participants who did not respond in a given round were not excluded from subsequent rounds but were re-invited for later rounds to maximize participation and preserve the breadth of expert input. No new participants were added after round 1. Analyses for each round were based on complete responses from eligible KOLs. Panel composition and response rates were documented and are reported in the Results.
Delphi-Consensus Process
The Delphi process was conducted, using structured questionnaires to systematically refine assessment criteria.
Round 1: The Exploratory Phase
In the 1st round, experts were asked to propose essential parameters for teledermatological malignant skin tumour assessments. Open-ended survey questions allowed respondents to provide qualitative input on:
Patient information (e.g. age, skin type).
Lesion information (e.g. size, duration).
Visual modalities (e.g. dermoscopy, lesion overview)
Responses were aggregated and thematically analysed to develop a structured list of proposed assessment parameters. Round 1 generated 47 unique variables. All variables progressed to round 2 for quantitative scoring. Predefined consensus criteria (≥66% agreement) were applied consistently across rounds 2 and 3 to determine whether variables progressed or were excluded. This allowed systematic tracking of item retention and elimination, ensuring transparent variable flow throughout the Delphi process.
Round 2: Prioritization and rating phase
Participants were explicitly instructed to consider the referral situation from the perspective of a general practitioner working under time constraints and to prioritize only those variables that were critical for teledermatological decision-making. The structured list of parameters identified in round 1 was presented to the KOLs for quantitative rating using a 5-point Likert scale (1=strongly disagree, 2=disagree, 3=neither agree nor disagree, 4=agree, 5=strongly agree). Variables were scored on three predefined dimensions: Essentiality (need), relevance to patient outcome (applicability) and feasibility, respectively, with summed scores calculated as the mean of individual ratings (23). KOLs were explicitly informed of the cut-off thresholds for variable inclusion and exclusion prior to rating, with variables scoring below 3.5 considered for exclusion, as specified in the survey instructions (Appendix S1). Variables with mean scores <60% were excluded, whereas variables scoring >60% and <70% were placed on the last page of the survey for round 3 as flagged for exclusion (24, 25, 26, 27, 28, 29).
Round 3: The refinement and consensus phase
In the 3rd and final round, KOLs reviewed the prioritized list of parameters to confirm or reject each item using a binary “Yes/No” response. At this stage, no further rating on needs, applicability, or feasibility was conducted, as these assessments had already been completed in round 2. Variables that received a “Yes” vote from more than two-thirds (≥67%) of KOLs were considered to have achieved consensus and were included in the final lists of variables. A consensus threshold of ≥67% agreement was predefined before data collection. In addition, a secondary analysis using a stricter ≥80% threshold was predefined and conducted to assess the robustness of the consensus (24, 25, 26, 27, 28, 29).
Data collection and anonymization
Study data were collected and managed using Research Electronic Data Capture (REDCap) tools hosted at Odense University Hospital (30, 31). The Delphi process was conducted between October 2024 and March 2025. KOLs were invited via email to participate in round 1. Each round was estimated to take approximately 30 min to complete. KOLs were given a five-week deadline, with two reminders sent on days 14 and 28 to encourage completion. The full invitation texts for all 3 rounds are available in Appendix S1.
In extraordinary circumstances, extensions were granted at the discretion of the steering group to optimize response rates; this occurred once. KOLs’ responses were anonymized to prevent bias, with only the data manager having access to identifying information.
Statistical analysis
Summary statistics were calculated and presented as frequencies with percentages for categorical variables and means with standard deviations (SD) for continuous variables. In round 2, mean scores were calculated separately for essentiality, relevance to patient outcomes and feasibility, and then averaged to generate a composite score for each variable. To assess the stability of ratings and agreement across panel members, interquatile ranges (IQRs) were calculated for all Likert-scale items. An IQR≤1 was pre-specified as indicating stable consensus with limited dispersion, in accordance with established Delphi methodology (32). All analyses were conducted using Microsoft Excel (Microsoft Corp., Redmond, WA), which was used to calculate descriptive statistics including means, SDs, percentages and IQRs.
Ethical considerations
This study was conducted following ethical guidelines for expert consensus research. All KOLs provided informed consent before participation. Data handling followed GDPR-compliant practices to ensure participant confidentiality. The study was approved by the Executive Secretariat of the Region of Southern Denmark (J. no. 24/37691).
RESULTS
Initially, 47 dermatologists from 16 countries were invited to participate. Of these, 33 met the predefined inclusion criteria of >6 years” dermatology experience and >100 TDS assessments and were eligible for rounds 2 and 3, representing 15 different countries. Details on clinical setting, country of practice and years of experience are presented in Table I. Participation across rounds is summarized in Table SI. Panel attrition occurred across rounds (round 1: n=47; round 2: n=26; round 3: n=27).
| Institution | Round 1* | Round 2 | Round 3 |
|---|---|---|---|
| Hospital | 15 | 9 | 9 |
| Academic/ Teaching institution | 20 | 11 | 11 |
| Dermatology clinic | 11 | 5 | 6 |
| Other (private office) | 1 | 1 | 1 |
| Region | |||
| Northern Europe | 26 | 17 | 18 |
| Western Europe | 10 | 5 | 5 |
| Eastern Europe | 4 | 2 | 3 |
| Southern Europe | 6 | 1 | 1 |
| Non-European | 1 | 1 | 0 |
| n | 47 | 26 | 27 |
| Years of practice as a dermatologist | |||
| Median, years | 13.5 | 15.5 | 15 |
| Mean, years (SD) | 15.1 (9.3) | 18.7 (8.0) | 18.4 (8.2) |
|
*Data from Phase 1 is before inclusion/exclusion. KOL: Key Opinion Leader; SD: standard deviation. |
|||
The geographical composition of the panel shifted over time (Fig. 2). In round 1, Scandinavian participants constituted 53% of all respondents prior to eligibility screening. After exclusion of ineligible experts, the proportion increased to 61%, suggesting that a higher proportion of Scandinavian participants fulfilled the inclusion criteria. The Scandinavian representation increased further in round 2 (65%) and round 3 (67%), reflecting differential attrition among non-Scandinavian experts.

Fig. 2. Visualization of participants in rounds 1 and 3.
Round 1 generated 47 unique variables across 3 domains: patient information, lesion information and visual modalities. All 47 variables progressed to round 2 for quantitative scoring. Based on predefined NAF exclusion criteria (mean score<3.5), 13 variables were excluded, leaving 34 variables for round 3. In round 3, binary voting was applied. Twelve of 34 variables (35%) reached ≥67% consensus and were retained as essential. Thus, 12 of the original 47 proposed variables were included in the final consensus set.
In round 2, variables relating to visual modalities and lesion characteristics consistently achieved higher mean scores than patient-related variables (Table II). The highest-rated items included sharp, in-focus images, the use of polarized dermoscopy and the inclusion of lesion overview images. In contrast, lower mean scores were observed for non-polarized dermoscopy, immunosuppression status and Fitzpatrick skin type.
Table II. Results of round 2 prioritization and rating phase
| All variables proposed in round 1 | Mean rank of (NAF) (SD) | IQR |
|---|---|---|
| Patient information | ||
| Age | 4.67 (0.57) | 0,5 |
| History of transplantation | 3.97 (0.97) | 1 |
| History of melanoma or other cutaneous malignancies | 3.86 (0.79) | 0,6 |
| Immunosuppression status | 3.86 (0.77) | 1 |
| Fitzpatrick skin type | 3.58 (0.81) | 1,3 |
| Gender | 3.48 (0.94) | 1,3 |
| Genetic mutations (e.g. CDKN2A, MC1R genes) | 3.43 (0.93) | 1,5 |
| Pregnancy | 3.38 (1.01) | 1,5 |
| Family history, especially first-degree relatives with melanoma | 3.30 (0.94) | 1,8 |
| History of chemotherapy or radiation | 3.06 (1.01) | 1,8 |
| Estimated number of moles | 3.03 (0.84) | 1,5 |
| Comorbidities | 2.95 (0.86) | 1 |
| Previous skin surgeries | 2.86 (0.93) | 2 |
| Profession | 2.58 (0.87) | 1,3 |
| History of blistering sunburns | 2.55 (1.05) | 1,8 |
| History of tanning salon use | 2.51 (1.02) | 2,2 |
| Extensive outdoor sports or hobby activities | 2.49 (0.93) | 1,2 |
| Exposure to carcinogenic agents/chemicals | 2.40 (0.83) | 1,2 |
| Frequency of previous dermatological skin examinations | 2.24 (0.72) | 1,2 |
| Use of sunscreen (frequency and SPF) | 1.95 (0.83) | 2 |
| Lesion information | ||
| Previous treatments for the lesion | 4.07 (0.77) | 0,8 |
| Change in colour, size, shape, elevation or growth | 4.01 (0.83) | 1 |
| Development speed (how fast it grows) | 3.87 (0.92) | 1,2 |
| Duration (how long the lesion has been noticed) | 3.76 (1.09) | 1,5 |
| Lesion morphological details | 3.73 (0.98) | 1,7 |
| Nature of changes | 3.67 (0.85) | 1 |
| History of trauma to the lesion | 3.62 (0.72) | 1 |
| Presence of the “ugly duckling sign” (i.e. the lesion different compared to peer lesions) | 3.61 (1.12) | 1,5 |
| Number of lesions/existences of similar lesions | 3.46 (1.02) | 1,5 |
| Reason for evaluation | 3.45 (1.06) | 1,5 |
| Symptoms from the lesion (if any) | 3.44 (0.84) | 1 |
| Findings when palpation the lesion | 3.34 (0.80) | 1,3 |
| Clinical diagnosis of the lesion | 3.33 (0.99) | 1,3 |
| Visual modalities | ||
| Sharp images with the lesion of interest centered and in focus | 4.62 (0.41) | 0,5 |
| Dermoscopy (polarized) | 4.54 (0.58) | 0,7 |
| Lesion overview for location | 4.32 (0.69) | 1 |
| Good surrounding light without reflection on the skin | 4.27 (0.70) | 1 |
| Close-up macroscopic evaluation (texture and topography identifiable) | 4.23 (0.80) | 1,3 |
| Use of contact gel for improved image quality | 4.09 (0.93) | 1,8 |
| Dermoscopy without pressure (to assess vessels) | 4.06 (0.66) | 1,3 |
| Dermoscopy (non-polarized) | 4.02 (0.90) | 2 |
| Photos of sun-damage in exposed skin areas | 3.22 (0.81) | 1,7 |
| Overview from different angles | 3.09 (0.71) | 1 |
| Clinical and dermoscopic images from anterior and posterior aspects of the body/extremities | 2.97 (1.00) | 1,8 |
| UV-dermoscopy (if available) | 2.36 (0.88) | 1,3 |
| Confocal images (if available) | 2.04 (0.83) | 1,7 |
| Multispectral photos (if available) | 1.96 (0.77) | 1,5 |
|
Yellow = marked for exclusion >60% = 3.0 and <70 = 3.5, Red = excluded, Sun Protection Factor (SPF), Needs, applicability, feasibility (NAF), IQR = Interquatile range. |
||
In round 3, consensus was achieved across all three predefined domains. Two patient-related variables, 4 lesion-related variables and 6 variables relating to visual modalities met the predefined ≥67% agreement threshold and are summarized in Table III. Visual modality variables demonstrated particularly high levels of agreement among the panel. Sharp, centred and in-focus images achieved agreement rates of 96.3%, polarized dermoscopy reached 92.6% agreement and lesion overview images were supported by 85.2% of participants. Several variables did not reach the consensus threshold. These included nonpolarized dermoscopy (55.5%), immunosuppression status (55.6%) and Fitzpatrick skin type (39.3%). A complete overview of voting outcomes for all assessed variables is provided in Table SII.
Table III. Consensus statement
| Consensus item | Consensus statement |
|---|---|
| Patient information | |
| 1.1 | The patient’s age is essential for teledermatological assessment. |
| 1.2 | A history of melanoma or other cutaneous malignancies, including actinic keratosis, is essential for teledermatological assessment. |
| Lesion information | |
| 2.1 | Documenting changes in colour, size, shape, elevation or growth is essential for teledermatological assessment. |
| 2.2 | The duration for which the lesion has been noticed is essential for teledermatological assessment |
| 2.3 | The rate of lesion development is essential for teledermatological assessment. |
| 2.4 | Information about previous treatments of the lesion is essential for teledermatological assessment. |
| Visual modalities | |
| 3.1 | Sharp images with the lesion centered and in focus are essential for teledermatological assessment. |
| 3.2 | Good surrounding light without reflections on the skin is essential for teledermatological assessment. |
| 3.3 | An overview image showing the lesion’s location is essential for teledermatological assessment. |
| 3.4 | A close-up image allowing macroscopic evaluation of texture and topography is essential for teledermatological assessment. |
| 3.5 | Polarized dermoscopy is essential for teledermatological assessment. |
| 3.6 | The use of contact gel to improve image quality is essential for teledermatological assessment. |
|
Summary of reached consensus statement. |
|
Sensitivity analysis: Scandinavian vs non-Scandinavian experts
A post hoc sensitivity analysis was conducted to explore the impact of regional representation on consensus outcomes. Responses from Scandinavian participants (Denmark, n=4; Sweden, n=12) were excluded, leaving a subgroup of 11 non-Scandinavian experts. In this analysis, several additional clinical history variables – specifically immunosuppression status, history of transplantation and history of trauma to the lesion – would have achieved consensus, whereas the use of contact gel would not have met the predefined threshold (Table SIII).
Sensitivity analysis using a stricter consensus threshold (≥80%)
A second sensitivity analysis applied a stricter consensus threshold of≥80% to assess the robustness of the final variable set (Table SIV). Under this higher threshold, eight of the original twelve variables remained. These comprised 1 patient-related variable (age), 3 lesion-related variables (documentation of change, rate of development and previous treatments) and 4 visual modality variables (image sharpness, lighting quality, overview images and close-up images). Variables that met the original ≥67% threshold but failed to meet the ≥80% threshold included lesion duration, history of cutaneous malignancy, polarized dermoscopy and the use of contact gel. This finding indicates that image-quality variables represent the most robustly supported elements of teledermatology referrals, while several clinical history variables appear more sensitive to the chosen consensus threshold.
DISCUSSION
This predominantly European Delphi study identified twelve essential clinical and visual variables for teledermatological skin tumour assessment, prioritizing image quality and lesion-specific data. Clinically, high-quality images and documented lesion information support accurate triage and reduce delayed diagnosis risks (7, 15, 17, 18). Embedding these variables into structured referral templates could improve workflow efficiency by reducing incomplete referrals, repeat imaging and unnecessary administrative communication.
The robustness of the final 12 variables is further supported by the dispersion metrics observed during round 2 prioritization phase. Variables that ultimately achieved the predefined ≥67% consensus threshold in round 3 demonstrated early stability, evidenced by narrow Interquatile Ranges (IQR≤1). For instance, highly rated visual modalities such as sharp, centered images and polarized dermoscopy yielded highly stable IQRs of 0.5 and 0.7, respectively. In contrast, variables that ultimately failed to reach consensus, such as Fitzpatrick skin type, displayed greater dispersion early in the process (IQR 1.3). This alignment between quantitative stability in round 2 and the final binary agreement in round 3 underscores the validity of the selected variables; it demonstrates that the Delphi process successfully filtered out genuinely contentious items rather than artificially forcing agreement.
The findings broadly align with teledermatology guidelines from the United Kingdom, Australia and the United States, which emphasize high-quality imaging and adequate clinical context (8, 16, 17, 18). Unlike existing guidelines, which often present long and undifferentiated lists of recommended data points, this study provides a prioritized and operationalizable core dataset derived through structured expert consensus (20, 21).
Similar patterns are seen in non-European frameworks. In India and China, teledermatology models emphasize store-and-forward workflows, rapid triage and reliance on high-quality images with a limited set of essential clinical variables, reflecting high patient volumes and more constrained specialist access (19, 33, 34). Compared with these models, the present consensus aligns particularly in the prioritization of image quality and lean clinical datasets but reflects a European triage-to-in-person care structure, which may limit direct applicability in regions where teledermatology functions as the primary diagnostic pathway (10, 19, 33, 34).
The variables are also directly relevant for AI-driven diagnostic systems. Visual quality parameters such as sharpness, lighting, overview and close-up imaging and polarized dermoscopy correspond closely to established technical requirements for computer vision models (7, 35). These variables could be integrated as mandatory metadata fields or incorporated into automated quality-control pipelines to detect inadequate inputs and prompt corrective actions.
The role of TDS varies between healthcare systems (9, 10, 12, 19, 36, 37). In Scandinavian countries, it is primarily used for triage to in-person assessment, whereas in geographically large or resource-limited regions it may represent the main access point to specialist care (19, 33, 34). These differences likely influenced prioritization of clinical history variables. For example, immunosuppression and transplant history did not reach consensus in the full panel but did reach consensus when Scandinavian participants were excluded. This may reflect a triage-driven workflow in Scandinavia where immunosuppression/transplant status is essential for urgency stratification and to prevent under-triage, whereas in settings where TDS is the primary access point, lesion information and visual modalities may be prioritized over background risk factors.
Applying a stricter ≥80% consensus threshold reduced the final variable set to eight items (Table IV). Visual modalities variables remained across thresholds, consistent with guidance emphasizing focus, lighting, colour and scale (7, 8, 17, 18). In contrast, several variables no longer met the higher consensus criterion, illustrating how prespecified consensus definitions can materially influence which items are retained in Delphi-derived core datasets and should therefore be justified when developing recommendations (22). Importantly, a higher cut-off may favour broadly applicable imaging requirements over context dependent risk and history items, potentially affecting the clinical specificity of referrals in some settings where textual risk stratification contributes more strongly to decision making.
Table IV. Sub analysis 80% consensus
| Consensus item | Consensus statement |
|---|---|
| Patient information | |
| 1.1 | The patient’s age is essential for teledermatological assessment. |
| Lesion information | |
| 2.1 | Documenting changes in colour, size, shape, elevation or growth is essential for teledermatological assessment. |
| 2.2 | The speed of lesion development is essential for teledermatological assessment. |
| 2.3 | Information about previous treatments of the lesion is essential for teledermatological assessment. |
| Visual modalities | |
| 3.1 | Sharp images with the lesion centered and in focus are essential for teledermatological assessment. |
| 3.2 | Good surrounding light without reflections on the skin is essential for teledermatological assessment. |
| 3.3 | An overview image showing the lesion’s location is essential for teledermatological assessment. |
| 3.4 | A close-up image allowing macroscopic evaluation of texture and topography is essential for teledermatological assessment. |
Fitzpatrick skin type did not reach consensus. One interpretation is that experts may infer skin phototype from high quality images and therefore prioritize a concise referral text (25). However, given the increasing Scandinavian representation across rounds, the perceived value of explicitly reporting skin type may differ in regions with greater phototype diversity and/or different referral pathways and resource contexts ((e.g.) access to specialist review, biopsy capacity and technology/training in primary care). Such system-level and socioeconomic differences may influence which variables are most informative (19), suggesting that while the present dataset provides an international minimum, regional add-on modules may be warranted to optimize diagnostic specificity and clinical utility.
The predominance of European participants limits direct global generalizability. Framing the findings as a European consensus reduces the risk of overinterpretation and highlights the need for future studies including greater representation from Asia, Africa and the Americas, where care models and referral workflows differ substantially.
Strengths and limitations
Strengths include a structured, anonymized Delphi approach minimizing dominance bias, an experienced expert panel and transparent sensitivity analyses demonstrating robustness. Limitations include a predominantly European panel with Scandinavian overrepresentation, restricting global generalizability and introducing regional bias. Additionally, panel attrition may have altered composition, and the ≥67% consensus threshold produced threshold-sensitive results.
Conclusion
This Delphi study provides a primarily European expert consensus on essential clinical and visual variables for teledermatological assessment of skin tumours. The identified variables offer a pragmatic framework for standardizing referrals, improving diagnostic consistency and supporting integration into AI-assisted workflows. Future multinational validation studies are required to confirm their impact on patient outcomes, workflow efficiency and global applicability.
REFERENCES
- Wang M, Gao X, Zhang L. Recent global patterns in skin cancer incidence, mortality, and prevalence. Chin Med J (Engl) 2025; 138: 185–192. https://doi.org/10.1097/CM9.0000000000003416
- Observatory Gc. Estimated number of new cases from 2022 to 2050, Males and Females, age [0-85+]. WHO; 2025. Available from: https://gco.iarc.fr/tomorrow/en/dataviz/trends?types=0&sexes=1_2&mode=cancer&group_populations=1&multiple_populations=1&multiple_cancers=1&cancers=17_16&populations=991_992_993_994_995_996&group_cancers=1&scale=log&min_zero=0&print=1
- Olsen CM, Wilson LF, Green AC, Bain CJ, Fritschi L, Neale RE, et al. Cancers in Australia attributable to exposure to solar ultraviolet radiation and prevented by regular sunscreen use. Aust N Z J Public Health 2015; 39: 471–476. https://doi.org/10.1111/1753-6405.12470
- Belbasis L, Stefanaki I, Stratigos AJ, Evangelou E. Non-genetic risk factors for cutaneous melanoma and keratinocyte skin cancers: an umbrella review of meta-analyses. J Dermatol Sci 2016; 84: 330–339. https://doi.org/10.1016/j.jdermsci.2016.09.003
- Vestergaard ME, Macaskill P, Holt PE, Menzies SW. Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: a meta-analysis of studies performed in a clinical setting. Br J Dermatol 2008; 159: 669–676. https://doi.org/10.1111/j.1365-2133.2008.08713.x
- Kittler H, Pehamberger H, Wolff K, Binder M. Diagnostic accuracy of dermoscopy. Lancet Oncol 2002; 3: 159–165. https://doi.org/10.1016/s1470-2045(02)00679-4
- Katragadda C, Finnane A, Soyer HP, Marghoob AA, Halpern A, Malvehy J, et al. Technique standards for skin lesion imaging: a Delphi consensus statement. JAMA Dermatol 2017; 153: 207–213. https://doi.org/10.1001/jamadermatol.2016.3949
- Abbott LM, Miller R, Janda M, Bennett H, Taylor M, Arnold C, et al. Practice guidelines for teledermatology in Australia. Australas J Dermatol 2020; 61: e293–e302. https://doi.org/10.1111/ajd.13301
- Lee KJ, Finnane A, Soyer HP. Recent trends in teledermatology and teledermoscopy. Dermatol Pract Concept 2018; 8: 214–223. https://doi.org/10.5826/dpc.0803a13
- Wang RH, Barbieri JS, Nguyen HP, Stavert R, Forman HP, Bolognia JL, et al. Clinical effectiveness and cost-effectiveness of teledermatology: Where are we now, and what are the barriers to adoption? J Am Acad Dermatol 2020; 83: 299–307. https://doi.org/10.1016/j.jaad.2020.01.065
- Giavina-Bianchi M, Santos AP, Cordioli E. Teledermatology reduces dermatology referrals and improves access to specialists. EClinicalMedicine 2020; 29–30: 100641. https://doi.org/10.1016/j.eclinm.2020.100641
- Lim D, Oakley AMM, Rademaker M. Better, sooner, more convenient: a successful teledermoscopy service. Australas J Dermatol 2012; 53: 22–25. https://doi.org/10.1111/j.1440-0960.2011.00836.x
- Whiting G, Stocks N, Morgan S, Tapley A, Henderson K, Holliday E, et al. General practice registrars’ use of dermoscopy: Prevalence, associations and influence on diagnosis and confidence. Aust J Gen Pract 2019; 48: 547–553. https://doi.org/10.31128/AJGP-11-18-4773
- Moreno-Ramirez D, Ferrandiz L, Nieto-Garcia A, Carrasco R, Moreno-Alvarez P, Galdeano R, et al. Store-and-forward teledermatology in skin cancer triage: experience and evaluation of 2009 teleconsultations. Arch Dermatol 2007; 143: 479–484. https://doi.org/10.1001/archderm.143.4.479
- Bourkas AN, Barone N, Bourkas MEC, Mannarino M, Fraser RDJ, Lorincz A, et al. Diagnostic reliability in teledermatology: a systematic review and a meta-analysis. BMJ Open 2023; 13: e068207. https://doi.org/10.1136/bmjopen-2022-068207
- Abbott LM, Miller R, Janda M, Bennett H, Taylor ML, Arnold C, et al. A review of literature supporting the development of practice guidelines for teledermatology in Australia. Australas J Dermatol 2020; 61: e174–e183. https://doi.org/10.1111/ajd.13249
- Group TWP. Service guidance and standards for the use of teledermatology. British Association of Dermatologists: Transformation and Quality Improvement Unit 2024.
- McKoy K, Antoniotti NM, Armstrong A, Bashshur R, Bernard J, Bernstein D, et al. Practice guidelines for teledermatology. Telemed J E Health 2016; 22: 981–990. https://doi.org/10.1089/tmj.2016.0137
- Dovigi E, Kwok EYL, English JC 3rd. A framework-driven systematic review of the barriers and facilitators to teledermatology implementation. Curr Dermatol Rep 2020; 9: 353–361. https://doi.org/10.1007/s13671-020-00323-0
- Nasa P, Jain R, Juneja D. Delphi methodology in healthcare research: How to decide its appropriateness. World J Methodol 2021; 11: 116–129. https://doi.org/10.5662/wjm.v11.i4.116
- Barrett D, Heale R. What are Delphi studies? Evid Based Nurs 2020; 23: 68–69. https://doi.org/10.1136/ebnurs-2020-103303
- Birko S, Dove ES, Özdemir V. Evaluation of nine consensus indices in Delphi foresight research and their dependency on delphi survey characteristics: a simulation study and debate on Delphi design and interpretation. PLoS One 2015; 10: e0135162. https://doi.org/10.1371/journal.pone.0135162
- Nayahangan LJ, Stefanidis D, Kern DE, Konge L. How to identify and prioritize procedures suitable for simulation-based training: experiences from general needs assessments using a modified Delphi method and a needs assessment formula. Med Teach 2018; 40: 676–683. https://doi.org/10.1080/0142159X.2018.1472756
- Russo T, Piccolo V, Moscarella E, Tschandl P, Kittler H, Paoli J, et al. Indications for digital monitoring of patients with multiple Nevi: recommendations from the international dermoscopy society. Dermatol Pract Concept 2022; 12: e2022182. https://doi.org/10.5826/dpc.1204a182
- Blum A. Re: Expert consensus statement on proficiency standards for dermoscopy education in primary care. J Am Board Fam Med 2023; 36: 695. https://doi.org/10.3122/jabfm.2023.230138R0
- Kashani-Sabet M, Leachman SA, Stein JA, Arbiser JL, Berry EG, Celebi JT, et al. Early detection and prognostic assessment of cutaneous melanoma: consensus on optimal practice and the role of gene expression profile testing. JAMA Dermatol 2023; 159: 545–553. https://doi.org/10.1001/jamadermatol.2023.0127
- Nayahangan LJ, Van Herzeele I, Konge L, Koncar I, Cieri E, Mansilha A, et al. Achieving consensus to define curricular content for simulation based education in vascular surgery: a Europe wide needs assessment initiative. Eur J Vasc Endovasc Surg 2019; 58: 284–291. https://doi.org/10.1016/j.ejvs.2019.03.022
- Vogel C, Zwolinsky S, Griffiths C, Hobbs M, Henderson E, Wilkins E. A Delphi study to build consensus on the definition and use of big data in obesity research. Int J Obes 2019; 43: 2573–2586. https://doi.org/10.1038/s41366-018-0313-9
- Fried LJ, Tan A, Berry EG, Braun RP, Curiel-Lewandrowski C, Curtis J, et al. Dermoscopy proficiency expectations for US dermatology resident physicians: Results of a modified Delphi survey of pigmented lesion experts. JAMA Dermatol 2021; 157: 189–197. https://doi.org/10.1001/jamadermatol.2020.5213
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009; 42: 377–381. https://doi.org/10.1016/j.jbi.2008.08.010
- Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform 2019; 95: 103208. https://doi.org/10.1016/j.jbi.2019.103208
- Gracht HA. Consensus measurement in Delphi studies: review and implications for future quality assurance. Technol Forecast Soc Change 2012; 79: 1525–1536. https://doi.org/10.1016/j.techfore.2012.04.013
- Thomas J, Kumar P. The scope of teledermatology in India. Indian Dermatol Online J 2013; 4: 82–89. https://doi.org/10.4103/2229-5178.110579
- Mu Z, Liu X, Li K, Zhang J. Teledermatology service during the COVID-19 pandemic in China: a mobile application-based retrospective study. Clin Cosmet Investig Dermatol 2021; 14: 1119–1124. https://doi.org/10.2147/CCID.S326105
- Alves J, Moreira D, Alves P, Rosado L, Vasconcelos MJM. Automatic focus assessment on dermoscopic images acquired with smartphones. Sensors (Basel) 2019; 19: 4957. https://doi.org/10.3390/s19224957
- Börve A, Dahlén Gyllencreutz J, Terstappen K, Johansson Backman E, Aldenbratt A, Danielsson M, et al. Smartphone teledermoscopy referrals: a novel process for improved triage of skin cancer patients. Acta Derm Venereol 2015; 95: 186–190. https://doi.org/10.2340/00015555-1906
- Vestergaard T, Andersen MK, Bygum A. Acceptance of teledermoscopy by general practitioners and dermatologists in Denmark. Dermatol Pract Concept 2021; 11: e2021033. https://doi.org/10.5826/dpc.1102a33