ORIGINAL REPORT
Long-term Recurrence after Curettage ± Electrodesiccation for Basal Cell Carcinoma: A Nationwide Cohort Study of 47,358 Tumours from Dermatology Practices
Emilie W. KJELDSEN1*![]() , Susanne K. KJÆR2,3,4
, Susanne K. KJÆR2,3,4![]() , Johan SIEBORG1
, Johan SIEBORG1![]() , Henrik SØLVSTEN5
, Henrik SØLVSTEN5![]() and Merete HÆDERSDAL1,4
and Merete HÆDERSDAL1,4![]()
1Department of Dermatology, Copenhagen University Hospital – Bispebjerg, Copenhagen, Denmark, 2Unit of Virus, Lifestyle and Genes, Danish Cancer Society Research Center, Copenhagen, Denmark, 3Department of Gynaecology, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark, 4Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark, and 5Dermatology Clinic, Aalborg, Denmark
Corr: Emilie W. Kjeldsen, Department of Dermatology, Copenhagen University Hospital – Bispebjerg, Nielsine Nielsens Vej 9, DK-2400, Copenhagen, Denmark. *Email: emilie.westerlin.kjeldsen.01@regionh.dk
Key words: basal cell carcinoma; curettage; dermatology practice; epidemiology; recurrence; surgery.
Citation: Acta Derm Venereol 2026; 106: adv-2025-0079. DOI: https://doi.org/10.2340/actadv.v106.adv-2025-0079.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Oct 6, 2025. Accepted after revision: May 11, 2026.
Published: Jun 2, 2026.
Competing interests and funding: The work was funded by the Danish Research Center for Skin Cancer (www.researchcenterforskincancer.org), a public-private research partnership between Private Hospital Mølholm, Aalborg University Hospital and Copenhagen University Hospital, Bispebjerg and Frederiksberg.
The data underlying this study cannot be shared publicly as Danish law does not allow transfer of these data.
The project was registered at the Capital Region’s inventory (Videnscenter for Dataanmeldelser, ref.P‐2022‐184). No approval by an ethics committee is needed according to the Danish law (Lov om videnskabsetisk behandling af sundhedsvidenskabelige forskningsprojekter, § 14, stk. 2).
EWK, SKK, JS and HS have nothing to declare. MH reports research grants, consulting fees, lecture or teaching honoraria, and/or equipment receipt from Leo Pharma, LÒréal / La Roche-Posay, Procter & Gamble, Galderma, Cynosure-Lutronic, GME Medical, and Venus Concept outside the submitted work.
The incidence of basal cell carcinoma is increasing globally, with Denmark showing a 220% rise between 2013 and 2021, underscoring the need to optimize treatment strategies. Curettage with or without electrodesiccation (C±E) is commonly used, yet updated tumour-specific recurrence data are limited. Using the Danish Skin Cancer Registry, we assessed long-term recurrence after C±E for 47,358 basal cell carcinomas treated in office-based dermatological practices between 2013 and 2022. Follow-up began one year after treatment, and recurrence was evaluated using Kaplan–Meier analysis and Cox regression to estimate cumulative recurrence rates and hazard ratios (HR) by tumour characteristics. The 5-year recurrence rate was 9.9% (95% CI 9.4–10.3), increasing to 13.3% (12.6–14.1) at 8 years. Head and neck tumours had the highest recurrence (25.1% at 8 years; HR 2.25, 2.00–2.53), as did tumours >10 mm (16.7% at 8 years; HR 1.80, 1.62–1.99), while superficial basal cell carcinomas had the lowest recurrence (8.4% at 8 years; HR 0.46, 0.38–0.56). Incomplete follow-up may have introduced bias in recurrence estimates. This nationwide study, the largest to date with up to 8 years of follow-up, shows that C±E remains a viable treatment, but careful tumour selection is essential to optimize long-term outcomes.
Significance
Basal cell carcinoma is the most common skin cancer, and its numbers are increasing worldwide. Scraping (curettage) is a quick, simple and cost-effective treatment that is widely used, yet long-term knowledge on how often the cancer returns has been limited. By analysing more than 47,000 tumours with up to 8 years of follow-up, this study provides valuable real-world data to guide treatment decisions. The findings show that scraping remains a practical option for many patients, but that surgical excision may be preferable for head and neck tumours to ensure the best outcomes.
Basal cell carcinoma (BCC) is the most common form of skin cancer, with its incidence steadily rising worldwide (1). In Denmark, the incidence of BCC has risen by 220% from 2013 to 2021 (2), with currently at least 15,000 new cases annually (3). As this number grows, the demand for optimizing treatment strategies becomes increasingly important to ensure high-quality patient care and sustainable use of healthcare resources. Various treatment modalities are available, inclu- ding cryotherapy, photodynamic therapy, curettage with or without electrodesiccation (C±E), surgical excision and Mohs micrographic surgery (4). Among these, C±E is widely used due to its simplicity, relatively low cost and short procedural time. In addition, immediate treatment with C±E following a clinical diagnosis may reduce the number of healthcare visits compared with most other treatment options, thereby offering potential overall cost savings (5). The effectiveness of C±E, however, is largely based on studies conducted decades ago with small sample sizes and short follow-up periods, highlighting the need for updated evidence reflecting current clinical practice (6, 7, 8, 9, 10, 11).
C±E is a widely accepted technique and generally recommended for primary BCCs located outside the high-risk H-zone, smaller than 10 mm, and with a nodular or superficial growth pattern (12). However, no standardized international protocol for C±E exists, and the recurrence risk appears to be influenced by tumour characteristics and operator skills (4, 7, 8, 9). Reported 5-year recurrence rates for C±E range from 1% to 27%, but prior studies were limited by small sample sizes (N<2500) and focused on 5-year recurrence estimates or less, with limited reporting of longer-term recurrence (7, 8, 9, 10). Based on these studies, recurrence risk appears particularly high for tumours on the head and neck, aggressive histological subtypes and recurrent BCCs, making C±E less suitable for these cases (7, 8, 9, 10).
A key clinical challenge is identifying which BCCs are most appropriately treated with C±E based on tumour features and expected long-term outcomes. While C±E remains a convenient and cost-effective option, its effectiveness is difficult to evaluate due to the lack of histological margin assessment, unlike surgical excision or Mohs micrographic surgery (4). This limitation makes real-world data essential for evaluating effectiveness, with recurrence rates offering insights into the practical utility of C±E.
Therefore, the study aimed to prospectively assess real-world, long-term recurrence data from dermatology specialist practices in Denmark to better understand the BCC tumours for which C±E is most appropriate. We assessed overall cumulative recurrence rates (CRRs) of BCC following C±E treatment in a dermatological nationwide cohort from 2013 to 2022. Additionally, we examined recurrence risk according to tumour location, histological subtype and size using both CRRs and hazard ratios.
METHODS
Data sources
Data for this study were extracted from the Danish Skin Cancer Registry, a part of the Danish Clinical Quality Program (RKKP) (13). It is an online nationwide database including records of keratinocyte cancer from all office-based dermatological practices in Denmark’s state-funded public healthcare system (2). The registry was established in 2011 with continuous data collection onwards and the latest data update in June 2022. It contains comprehensive records on keratinocyte cancers including a unique tumour ID, date of diagnosis, a unique treatment ID, treatment method, procedure code, date of last control, recurrence registration and tumour characteristics including histological subtype, lateral tumour size and anatomical location. In Denmark, all citizens are assigned a unique personal identification number (PIN), which is used universally in all administrative systems in Denmark. Patient demographic and socioeconomic information, including PIN, age, sex, individual disposable income and education level, was obtained from the Civil Registration System, the Income Statistics Register and the Danish Education Register (14). Information on each patient’s diagnoses from hospital admissions, discharges and outpatient visits were obtained from The Danish National Patient Registry.
Study population and inclusion/exclusion criteria
The study population consisted of primary BCCs, regardless of subtype, treated with C±E between June 2013 and June 2022. Tumours without any registered follow-up were excluded from the dataset. More than one BCC tumour treated with C±E could be registered per patient.
Variable definitions and outcome
Tumours recurring within the 1st year after treatment were considered treatment failures rather than recurrences. Follow-up was therefore defined as starting 1 year after C±E treatment and continuing until detection of a recurrent tumour or the last recorded follow-up visit for the specific tumour course.
C±E treatment was recorded by dermatologists as curettage, single curettage with electrodesiccation, double curettage with electrodesiccation, curettage combined with cryotherapy, or curettage combined with silver nitrate.
Tumour characteristics included anatomical location, histological subtype and tumour size. The anatomical location of tumours was documented using SNOMED (Systematized Nomenclature of Medicine – Clinical Terms) 10-ICD codes and grouped into locations of head and neck, trunk, extremities or unspecified. Clinical diagnoses were included when histological verification was unavailable, and histologically verified subtypes overruled clinical diagnoses when both were recorded. BCC subtype was categorized as nodular, superficial, aggressive (infiltrated, morpheaform, micronodular, basosquamous) or unspecified. Tumour size was defined as the maximum clinical diameter measured in millimetres. Size was categorized as ≤10 mm, >10 mm or unspecified, where “unspecified” indicated missing information or unmeasurable size.
Yearly individual disposable income was categorized into 3 groups based on quartiles of the study population’s disposable income: 1st quartile, 2nd–3rd quartile and 4th quartile. Education was classified into 3 levels according to Statistics Denmark’s recommendations: short education (basic or youth education, 7–12 years of schooling), medium education (vocational education, 10–12 years) and long education (higher education >13 years).
Number of registered hospital diagnoses was identified based on hospital admissions, discharges and outpatient visits preceding tumour registration. Each registered hospital diagnosis was classified according to the International Classification of Diseases, 10th Revision (ICD-10). The total number of registered diagnoses per patient was calculated as the sum of all distinct diagnoses recorded across these categories, allowing for multiple registrations within the same category. A detailed description of the categorization is provided in the Appendix S1.
The primary outcome was recurrence of BCC following C±E, defined as histologically confirmed or clinically verified recurrence during follow-up.
Statistical analyses
Descriptive statistics were used to summarize patient and tumour characteristics. Continuous variables were reported as medians with interquartile ranges (IQRs). Categorical variables were presented as counts and percentages.
At study inclusion, defined as the first recorded BCC treated with C±E, baseline patient characteristics were stratified by the total number of tumours per patient at baseline (1 or ≥2) and included age, sex, annual disposable income, educational level and number of registered hospital diagnoses.
Tumour characteristics based on tumour-level data and stratified by recurrence status included age at BCC C±E treatment, anatomical location, histological subtype and tumour size. Tumour characteristics stratified by control follow-up status was also performed. The cumulative distribution of time from BCC C±E treatment to first control was assessed.
Kaplan–Meier survival analyses, with tumour follow-up starting 1 year after C±E treatment date, were conducted to estimate overall cumulative BCC tumour recurrence rates, as well as stratified by histological subtype, anatomical location and tumour size reported as percentages with 95% confidence intervals (CIs). Additionally, inverse Kaplan–Meier plots were generated to visualize the overall CRR and stratified CRRs.
The Cox proportional hazards assumption was assessed using Schoenfeld residuals, with no indication of non-proportionality. Uni- and multivariable Cox proportional hazards regression models were used to evaluate predictors of recurrence, adjusting for age, sex, income, education, BCC histological subtype, anatomical location and tumour size. Results were reported as hazard ratios (HRs) with 95% CIs. All analyses were conducted using R (version [4.4.1]).
RESULTS
Patient and tumour characteristics
The cohort selection process is shown in Fig. S1. In total, 47,358 BCC tumours treated with C±E were included in the analyses. These tumours occurred in 24,771 patients of whom 15.7% (n=3,878) had multiple BCC tumours diagnosed at baseline (first registered visit) (Table SI). Men were more likely to have multiple tumours compared to women (54.0% vs 48.5%). Socioeconomic characteristics were similar between groups regarding income and educational level, and no differences were observed for number of previous registered hospital diagnoses.
Of the included tumours, 98.6% were histopathologically verified, while the remaining were diagnosed based on clinical and dermoscopic assessment. Histological subtyping was not specified in 34% of tumours and these were therefore categorized as “unspecified”. Among recurrent tumours, 1.7% lacked histopathological verification and 29% could not be histologically subtyped.
Among the included tumours treated with C±E (n=47,358), 4.9% (n=2,336) were registered as recurring (Table I). Recurrence was more frequent for head and neck tumours (8.2%) compared to the trunk (4.0%) and extremities (3.2%). Nodular BCCs had the highest recurrence frequency (5.7%), while superficial BCCs had the lowest (2.8%). Larger BCC tumours (>10 mm) were more frequently recurring (6.2%) than smaller tumours (4.5%).
Table I. Basal cell carcinoma characteristics of 47,358 tumours stratified by recurrence status following C±E treatment
| Tumours without recurrence N=45,022(95.1%) | Tumours with recurrence N=2,336(4.9%) | |
|---|---|---|
| Age, years (median, IQR) | 72.2 (64.3–78.0) | 72.1 (63.2–78.6) |
| Anatomical locations, n (%) | ||
| Trunk | 10,310(96.0%) | 433(4.0%) |
| Extremities | 3,038(96.8%) | 102(3.2%) |
| Head and neck | 10,768(91.8%) | 961(8.2%) |
| Unspecified | 20,906(96.1%) | 840(3.9%) |
| Histological subtype, n (%) | ||
| Nodular | 24,573(94.3%) | 1,477(5.7%) |
| Superficial | 3,909(97.2%) | 111(2.8%) |
| Aggressive subtypes | 385(95.3%) | 19(4.7%) |
| Unspecified | 16,155(95.7%) | 729(4.3%) |
| Tumour size, n (%) | ||
| ≤10mm | 34,791(95.5%) | 1,640(4.5%) |
| >10mm | 7,374(93.8%) | 488(6.2%) |
| Unspecified | 2,857(93.2%) | 208(6.8%) |
|
Aggressive subtypes were infiltrated, morpheaform, micronodular or basosquamous. C±E: curettage with or without electrodesiccation; IQR: interquartile range. |
||
Characteristics of tumours without registered follow-up are presented in Table SII. Tumours without any follow-up were slightly more often located in the head and neck area, of superficial subtype, of unspecified tumour size, and the median age at treatment was higher (74.3 years versus 72.2 years).
Cumulative recurrence rates of BCCs treated with curettage ± electrodesiccation.
The overall CRR increased over time, reaching 6.1% (95% CI: 5.8–6.4) at 3 years, 9.9% (9.4–10.3) at 5 years, and 13.3% (12.6–14.1) at 8 years post-treatment (Fig. 1). The inverse Kaplan–Meier curve did not plateau, indicating a continued risk of recurrence (Fig. 1).
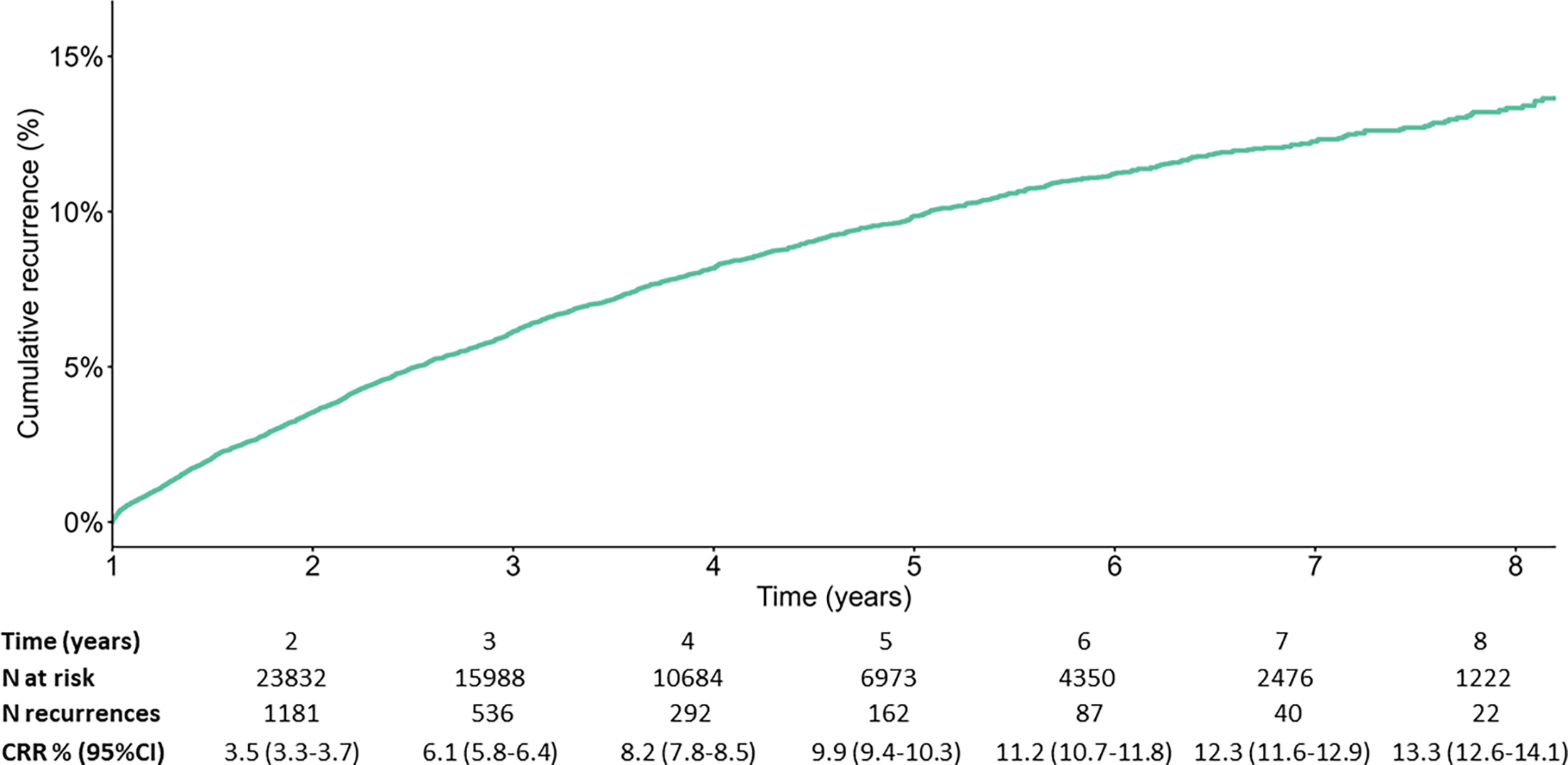
Fig. 1. Overall cumulative recurrence rates. Cumulative recurrence of basal cell carcinoma (BCC) following curettage with or without electrodesiccation (C±E) treatment, with cumulative recurrence rates from 2 to 8 years post-treatment based on 47,358 tumours. CRR: cumulative recurrence rate; N=number
In subgroup analyses, CRRs varied by anatomical location, histological subtype and tumour size. For anatomical locations, head and neck tumours had the highest CRR at 8 years of 25.1% (22.9–27.3), followed by trunk tumours with a CRR of 12.1% (10.5–13.7) (Fig. 2). The 8-year CRR for tumours located on extremities was 8.3% (6.3–10.2).
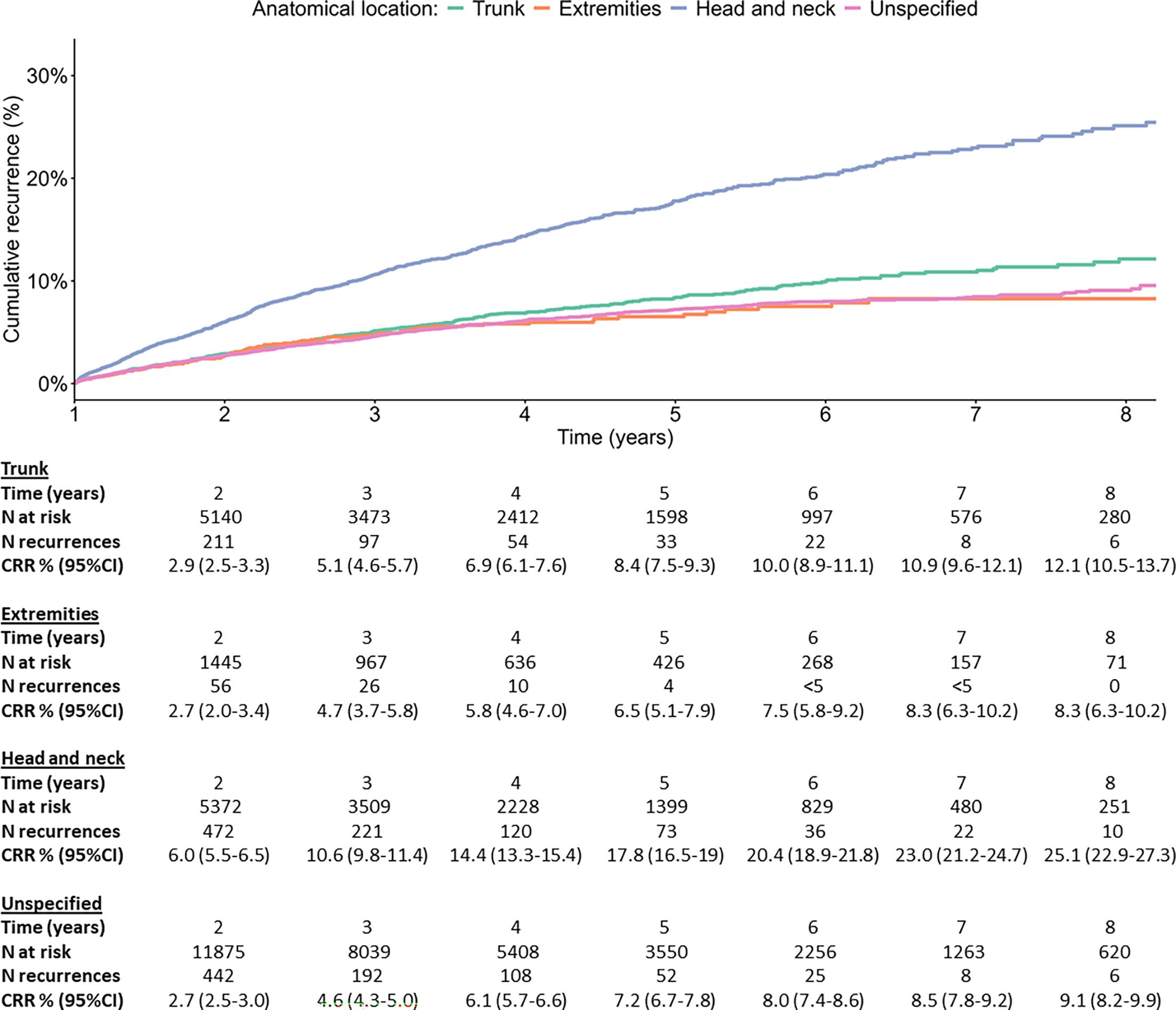
Fig. 2. Cumulative recurrence rates by anatomical location. Cumulative recurrence of basal cell carcinoma (BCC) following curettage with or without electrodesiccation (C±E) treatment, with cumulative recurrence rates from 2 to 8 years post-treatment stratified by anatomical location (head and neck, trunk, extremities and unspecified). Numbers provided as “<” in the table are censored to prevent personally identifiable data. CRR: cumulative recurrence rate; N: number
For histological subtypes, nodular BCCs had the highest CRR at 8 years of 17.8% (16.3–19.2), whereas superficial BCCs had a lower CRR of 8.4% (5.8–10.9) (Fig. 3). In BCCs of aggressive subtypes (infiltrated, morpheaform, micronodular or basosquamous), the 8-year CRR was 13.7% (2.2–23.8%). In the inverse Kaplan-Meier plot, CRRs for aggressive subtypes increased steeply in the first years but plateaued over time, likely due to limited data in later years.
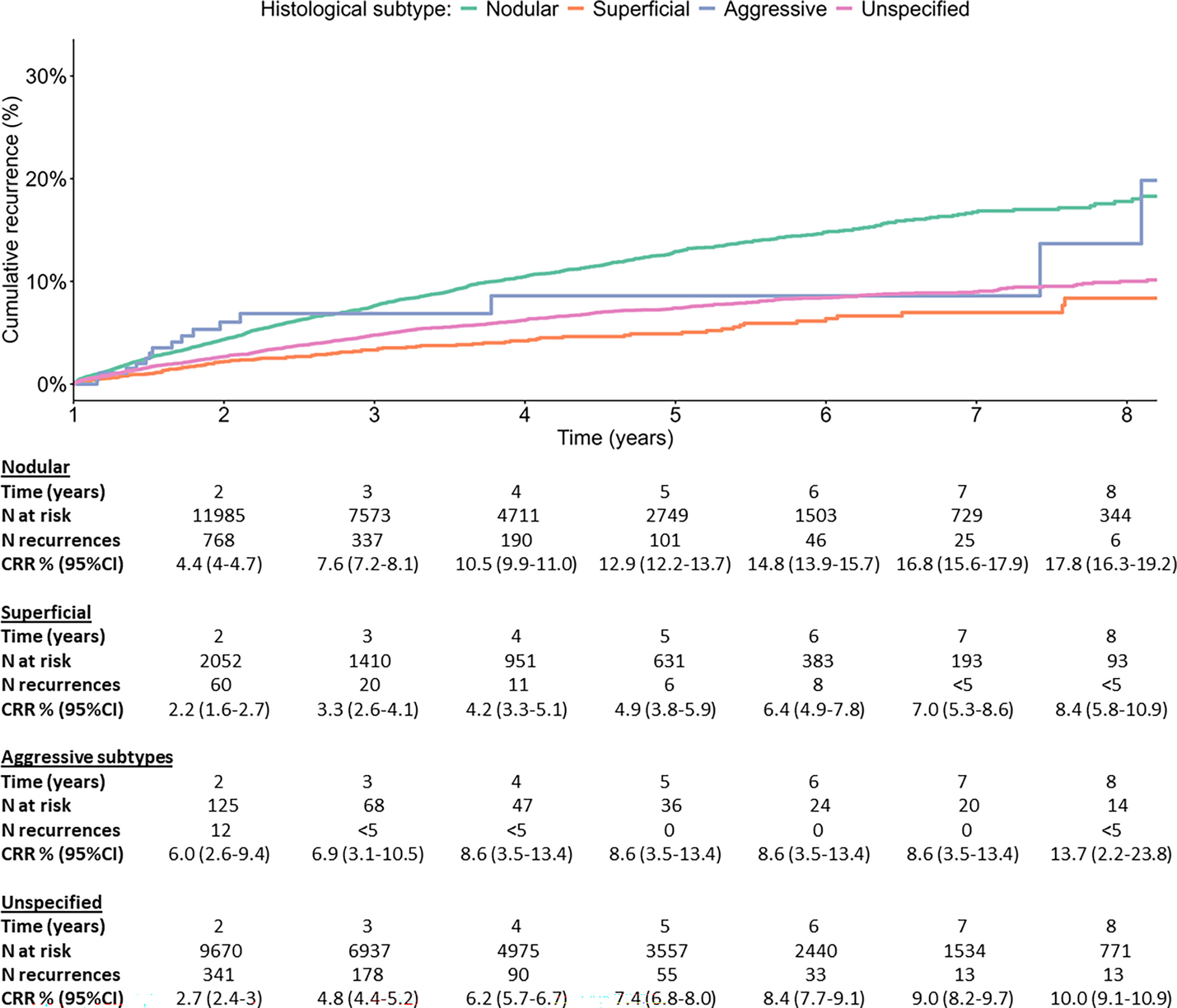
Fig. 3. Cumulative recurrence rates by histological subtype. Cumulative recurrence of basal cell carcinoma (BCC) following curettage with or without electrodesiccation (C±E) treatment, with cumulative recurrence rates from 2 to 8 years post-treatment stratified by histological subtype (nodular, superficial aggressive and unspecified). Numbers provided as “<” in the table are censored to prevent personally identifiable data. CRR: cumulative recurrence rate; N: number
Regarding BCC tumour size, larger tumours (>10 mm) had a CRR of 16.7% (14.7–18.6) at 8 years, compared to 12.4% (11.5–13.2) for smaller tumours (≤10 mm) (Fig. 4).
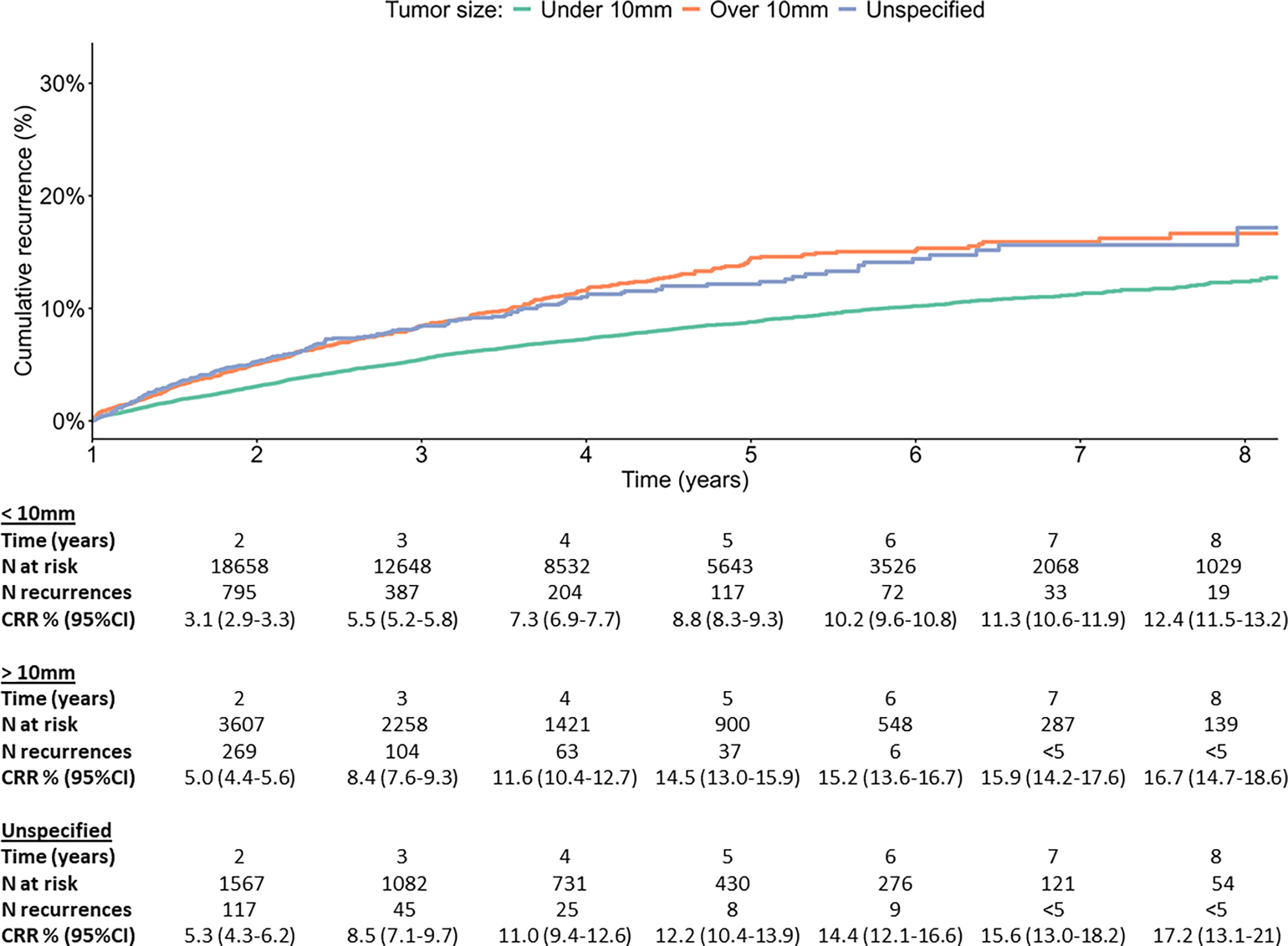
Fig. 4. Cumulative recurrence rates by BCC tumour size. Cumulative recurrence of basal cell carcinoma (BCC) following curettage with or without electrodesiccation (C±E) treatment, with cumulative recurrence rates from 2 to 8 years post-treatment stratified by tumour size (≤10 mm,>10 mm or unspecified). Numbers provided as “<” in the table are censored to prevent personally identifiable data. CRR: cumulative recurrence rate; N: number.
Predictors of BCC recurrence following curettage ± electrodesiccation treatment
Cox proportional hazards analysis identified anatomical location, histological subtype and tumour size as the strongest predictors of BCC recurrence following C±E treatment (Fig. 5). Head and neck tumours had the highest recurrence hazard, HR 2.25 (2.00–2.53), compared to tumours on the trunk (reference), while tumours located on extremities showed no difference in HRs. Superficial BCCs had a lower hazard of recurrence, HR 0.46 (0.38–0.56), than nodular BCCs (reference), while aggressive subtypes showed no difference, HR 1.02 (0.65–1.61). Larger tumours (>10 mm) had an increased recurrence hazard, HR 1.80 (1.62–1.99), compared to smaller tumours (≤10 mm) (reference).
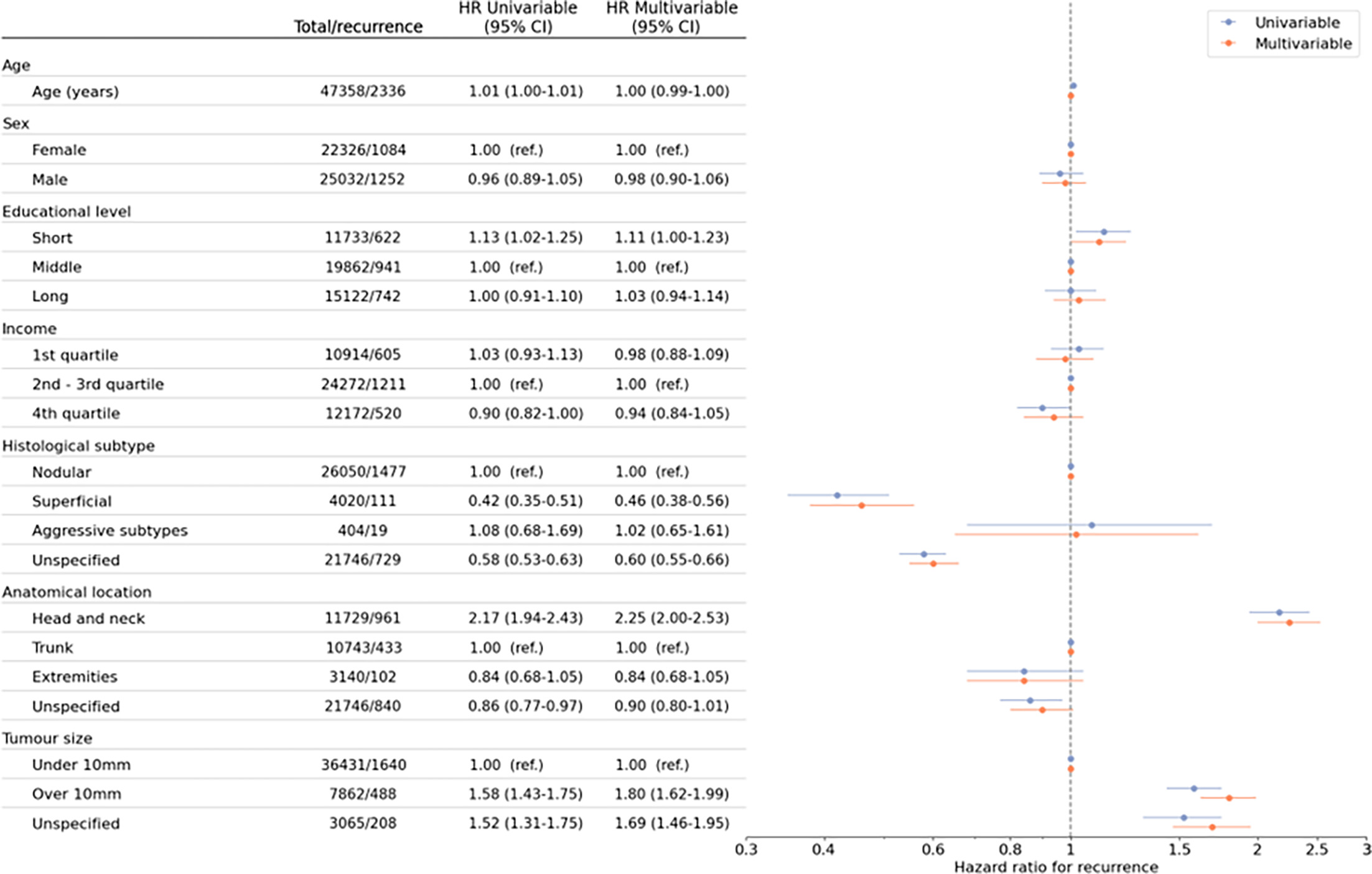
Fig. 5. Hazard ratios for predictors associated with basal cell carcinoma (BCC) recurrence following curettage with or without electrodesiccation (C±E) treatment based on 47,358 tumours. Univariable (blue) and multivariable (orange) hazard ratios (HRs) with 95 % confidence intervals (CIs) are shown for age, sex, educational level, income, histological subtype, anatomical location and tumour size. In the multivariable analysis, all variables were mutually adjusted.
Demographic factors showed limited impact on recurrence including age, sex, educational level and income.
DISCUSSION
This nationwide study, including 47,358 BCC tumours, provides contemporary real-world data on long-term recurrence following C±E treatment in dermatology specialist practices. The overall cumulative recurrence rate reached 13.3% at 8 years. Tumours on the head and neck and those >10 mm were associated with a significantly increased risk of recurrence, while superficial BCCs had a substantially lower risk than nodular BCCs. These findings emphasize the importance of tumour characteristics in guiding treatment selection and highlight the need for careful consideration of C±E as a treatment modality for high-risk tumours.
The overall cumulative recurrence rate of 13.3% at 8 years falls within the range reported in previous studies, where rates have varied widely from 1% to 27%, largely depending on follow-up duration, tumour characteristics, operator skills and treatment protocols (7, 8, 9, 10, 11, 15, 16, 17, 18, 19). However, earlier studies often had short follow-up periods, small sample sizes, limited subgroup analyses or were of older date, thus underscoring the need for larger and updated studies. Our study provides useful estimates of recurrence due to real-world data from dermatology practices, the largest dataset to date, long-term follow-up, and substantial subgroup analyses.
A unique aspect of this study is that all included tumours were treated in office-based dermatology practices, where specialist dermatologists performed the curettage procedures. This setting likely ensures a high level of procedural expertise as recurrence rates may be higher when C±E is performed by less experienced physicians. Previous studies have shown that operator skill significantly impacts recurrence, with higher rates observed among less experienced practitioners (7, 9, 20). This suggests that the recurrence rates observed in this study may represent outcomes from a best-case scenario. Together, these findings point to the importance of structured training programmes to ensure adequate curettage technique. Additionally, adjunctive imaging modalities such as line-field confocal optical coherence tomography (LC-OCT) and artificial intelligence could potentially assist junior or less experienced dermatologists in both pre-treatment tumour delineation and post-treatment assessment to confirm complete removal.
A major strength of this study is the nationwide data from over 47,000 BCC tumours treated with C±E in office-based dermatology clinics. The large sample size and long-term follow-up of at least 8 years provide robust estimates of recurrence rates and predictors for recurrence. Moreover, we were able to show recurrence rates and hazards stratified by anatomical location, histological subtype and tumour size. Lastly, the inclusion of all dermatology practices in the Danish Skin Cancer Registry enhances the generalizability of findings to routine dermatological care. However, some limitations should be considered. Recurrences were identified through routine clinical reporting without mandatory histopathological confirmation, potentially leading to misclassification or underestimation of recurrence estimates; however, only 1.7% of recurrences were not histologically verified. Recurrence may also have been misclassified if a new tumour developed near the original site, or underreported if patients were treated outside dermatological practices or if the treating dermatologist failed to register it as a recurrence. Although recurrence data were systematically recorded, missing information on tumour characteristics and follow-up visits could introduce bias. Most tumours had follow-up; however, a proportion did not, and whether this reflects absence of follow-up or incomplete registration is unknown. Nonetheless, baseline characteristics between the 2 groups were comparable. As follow-up was defined beginning one year after treatment, tumours recurring within the 1st year were excluded and classified as treatment failures rather than recurrences. This may have led to underestimation of overall recurrence risk. Histological subtype was “unspecified” in 34% of tumours, due to lack of pathological subtyping, while only 1.4% lacked histopathological confirmation. Incomplete subtype information and potential clinical misclassification may therefore have influenced subtype-specific recurrence estimates. Although data on different C±E techniques were available, comparisons between methods were limited by confounding related to operator preference and clinic-level practice patterns, making it difficult to isolate the independent effect of technique on recurrence. As a result, we could not assess the impact of different curettage methods on recurrence risk. Future studies should investigate optimal curettage protocols to enhance treatment consistency and effectiveness. Moreover, while head and neck tumours showed the highest recurrence rates, anatomical data lacked specificity regarding high-risk zones, such as the nose, lips or periorbital area. More precise anatomical classification would allow for improved risk stratification and treatment recommendations. Finally, while C±E is widely used in Denmark and other European countries, the applicability of our findings to other healthcare settings and countries remains unknown and would need confirmation in future studies.
In conclusion, this nationwide study provides robust long-term real-world data on recurrence following C±E treatment in dermatological practice. The higher recurrence risk observed for head and neck tumours and larger tumours underscore that C±E should be used cautiously in these settings, where surgical excision may be preferable. Conversely, the favourable outcomes for superficial BCCs on low-risk anatomical sites support the continued use of C±E in appropriately selected cases.
Overall, these findings reinforce the importance of careful tumour selection when considering C±E and provide up-to-date evidence to inform clinical decision-making and future treatment guidelines.
ACKNOWLEDGEMENTS
The research was executed at the Danish Research Center for Skin Cancer (www.researchcenterforskincancer.org), a public-private research partnership between Private Hospital Mølholm, Aalborg University Hospital and Copenhagen University Hospital, Bispebjerg and Frederiksberg.
REFERENCES
- Urban K, Mehrmal S, Uppal P, Giesey RL, Delost GR. The global burden of skin cancer: a longitudinal analysis from the Global Burden of Disease Study, 1990-2017. JAAD Int 2021; 2: 98–108. https://doi.org/10.1016/j.jdin.2020.10.013
- Sieborg J, Haedersdal M, Lei U, Sølvsten H, Olesen AB, Vinding GR, et al. Incidence and geographic differences in keratinocyte carcinoma and Bowen’s disease in office‐based dermatological practice between 2013 and 2022: a nationwide Danish registry‐based study. JEADV Clinical Practice 2024; 3: 1164–1174. https://doi.org/10.1002/jvc2.478
- Gjerstorff ML. The Danish cancer registry. Scand J Public Health 2011; 39: 42–45. https://doi.org/10.1177/1403494810393562
- Peris K, Fargnoli MC, Kaufmann R, Arenberger P, Bastholt L, Seguin NB, et al. European consensus-based interdisciplinary guideline for diagnosis and treatment of basal cell carcinoma-update 2023. Eur J Cancer 2023; 192: 113254. https://doi.org/10.1016/j.ejca.2023.113254
- Patel PV, Pixley JN, Dibble HS, Feldman SR. Recommendations for cost-conscious treatment of basal cell carcinoma. Dermatol Ther 2023; 13: 1959–1971. https://doi.org/10.1007/s13555-023-00989-x
- Spiller WF, Spiller RF. Treatment of basal cell epithelioma by curettage and electrodesiccation. J Am Acad Dermatol 1984; 11: 808–814. https://doi.org/10.1016/s0190-9622(84)80457-0
- Silverman MK, Kopf AW, Grin CM, Bart RS, Levenstein MJ. Recurrence rates of treated basal cell carcinomas. Part 2: curettage-electrodesiccation. J Dermatol Surg Oncol 1991; 17: 720–726. https://doi.org/10.1111/j.1524-4725.1991.tb03425.x
- Rodriguez-Vigil T, Vázquez-López F, Perez-Oliva N. Recurrence rates of primary basal cell carcinoma in facial risk areas treated with curettage and electrodesiccation. J Am Acad Dermatol 2007; 56: 91–95. https://doi.org/10.1016/j.jaad.2006.07.007
- Kopf AW, Bart RS, Schrager D, Lazar M, Popkin GL. Curettage-electrodesiccation treatment of basal cell carcinomas. Arch Dermatol 1977; 113: 439–443. https://doi.org/10.1001/archderm.1977.01640040047006
- Blixt E, Nelsen D, Stratman E. Recurrence rates of aggressive histologic types of basal cell carcinoma after treatment with electrodesiccation and curettage alone. Dermatol Surg 2013; 39: 719–725. https://doi.org/10.1111/dsu.12122
- Rowe DE, Carroll RJ, Day CL. Long-term recurrence rates in previously untreated (primary) basal cell carcinoma: implications for patient follow-up. J Dermatol Surg Oncol 1989; 15: 315–328. https://doi.org/10.1111/j.1524-4725.1989.tb03166.x
- Kim JYS, Kozlow JH, Mittal B, Moyer J, Olencki T, Rodgers P, et al. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol 2018; 78: 540–559. https://doi.org/10.1016/j.jaad.2017.10.006
- Lamberg AL, Sølvsten H, Lei U, Vinding GR, Stender IM, Jemec GBE, et al. The Danish nonmelanoma skin cancer dermatology database. Clin Epidemiol 2016; 8: 633–636. https://doi.org/10.2147/CLEP.S99464
- Schmidt M, Schmidt SAJ, Adelborg K, Sundbøll J, Laugesen K, Ehrenstein V, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol 2019; 11: 563–591. https://doi.org/10.2147/CLEP.S179083
- Salasche SJ. Curettage and electrodesiccation in the treatment of midfacial basal cell epithelioma. J Am Acad Dermatol 1983; 8: 496–503. https://doi.org/10.1016/s0190-9622(83)70055-1
- Thissen MR, Neumann MH, Schouten LJ. A systematic review of treatment modalities for primary basal cell carcinomas. Arch Dermatol 1999; 135: 1177–1183. https://doi.org/10.1001/archderm.135.10.1177
- Chren MM, Linos E, Torres JS, Stuart SE, Parvataneni R, Boscardin WJ. Tumor recurrence 5 years after treatment of cutaneous basal cell carcinoma and squamous cell carcinoma. J Invest Dermatol 2013; 133: 1188–1196. https://doi.org/10.1038/jid.2012.403
- Lubeek SFK, Arnold WP. A retrospective study on the effectiveness of curettage and electrodesiccation for clinically suspected primary nodular basal cell carcinoma. Br J Dermatol 2016; 175: 1097–1098. https://doi.org/10.1111/bjd.14770
- Werlinger KD, Upton G, Moore AY. Recurrence rates of primary nonmelanoma skin cancers treated by surgical excision compared to electrodesiccation-curettage in a private dermatological practice. Dermatol Surg 2002; 28: 1138–1142. https://doi.org/10.1046/j.1524-4725.2002.02110.x
- Williamson GS, Jackson R. Treatment of basal cell carcinoma by electrodesiccation and curettage. Can Med Assoc J 1962; 86: 855–862.