ORIGINAL REPORT
Joint Relationship of Cardiovascular-kidney-metabolic Syndrome and Psoriasis with All-cause and Cause-specific Mortality in Adults: A Population-based Analysis
Junhan ZHOU1, Hongping GE2, Bixin HUANG2, Yingwei WANG2 and Hongkai XIANG2*![]()
1Department of Obstetrics and Gynecology, the Second Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325027, China, and 2Department of Dermatology, the Second Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325027, China
Corr: Hongkai Xiang, Department of Dermatology, the Second Affiliated Hospital of Wenzhou Medical University, No.109, Xueyuanxi Road, Wenzhou, Zhejiang, 325027, China. *Email: xhk811@163.com
Key words: cardiovascular-kidney-metabolic syndrome; psoriasis; mortality; NHANES; epidemiology.
Citation: Acta Derm Venereol 2026; 106: adv-2025-0241. DOI: https://doi.org/10.2340/actadv.v106.adv-2025-0241.
Copyright: 2026 ©Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Dec 2, 2025. Accepted after revision: May 15, 2026.
Published: Jun 10, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
This work was supported by Basic Public Welfare Scientific Research Project of Wenzhou Science and Technology Bureau (Grant No. Y2023019).
NHANES data described in this manuscript are available at https://wwwn.cdc.gov/nchs/nhanes/.
All participants provided written informed consent and study procedures were approved by the National Center for Health Statistics Research Ethics Review Board (Protocol Number: Protocol #98-12, Protocol #2005-06 and Protocol #2011-17).
Psoriasis has been associated with cardiovascular risk, but the combined association of psoriasis and cardiovascular-kidney-metabolic (CKM) syndrome with mortality remains unclear. This study examined the individual and joint associations of CKM syndrome and self-reported psoriasis with all-cause and cardio-cerebrovascular disease (CCD) mortality among 9,598 U.S. adults aged ≥20 years from NHANES 2003–2006 and 2009–2014. CKM syndrome stages were defined according to the 2023 American Heart Association framework, and psoriasis was assessed by self-reported physician diagnosis. Mortality was ascertained through linkage to the National Death Index through 2019. During a median follow-up of 9.3 years, 860 deaths occurred. Advanced CKM syndrome was associated with higher all-cause mortality (HR=3.67; 95% CI: 3.00–4.50) and CCD mortality (HR=8.16; 95% CI: 5.42–12.28). Psoriasis was also associated with higher all-cause mortality (HR=2.06; 95% CI: 1.47–2.90) and CCD mortality (HR=2.69; 95% CI: 1.42–5.08). Participants with both advanced CKM syndrome and psoriasis had the highest observed risks of all-cause mortality (HR=7.09; 95% CI: 4.93–10.19) and CCD mortality (HR=16.47; 95% CI: 7.26–37.33). Formal interaction testing did not show significant multi-plicative interaction for all-cause mortality (p for interaction=0.16) or CCD mortality (p for interaction=0.80). These findings suggest that coexisting advanced CKM syndrome and psoriasis may identify adults with particularly elevated mortality risk.
SIGNIFICANCE
Psoriasis is a chronic inflammatory skin disease that frequently coexists with cardiometabolic abnormalities. However, limited evidence has addressed mortality risk among individuals with both psoriasis and cardiovascular-kidney-metabolic syndrome. In this nationally representative study of U.S. adults, the coexistence of psoriasis and advanced cardiovascular-kidney-metabolic syndrome identified a subgroup with particularly high all-cause and cardio-cerebrovascular mortality. These findings highlight the importance of cardiometabolic risk assessment and long-term risk management in adults with psoriasis.
Psoriasis, which is also known as chronic plaque psoriasis or psoriasis vulgaris, is a persistent inflammatory skin disorder that affects approximately 3.0% of adults in the United States (1). Beyond its visible cutaneous manifestations, psoriasis is increasingly recognized as a systemic condition associated with immune dysregulation and chronic low-grade inflammation (2). Emerging evidence suggests that psoriatic inflammatory cells contribute to vascular dysfunction and atherogenesis and supports the notion of psoriasis as an independent cardiovascular risk factor (3). A wide range of comorbidities have been associated with psoriasis, including cardiovascular, metabolic, gastrointestinal, pulmonary and renal diseases, as well as cancers (4). These comorbid conditions contribute substantially to the overall disease burden and are linked to an elevated risk of mortality, particularly among individuals with severe forms of psoriasis.
Cardiovascular-kidney-metabolic (CKM) syndrome is a recently proposed framework by the American Heart Association (AHA) in 2023 to describe the interconnected pathophysiology and clinical burden of cardiovascular, renal and metabolic diseases (5). CKM syndrome emphasizes the shared mechanisms of chronic inflammation, endothelial dysfunction and metabolic dysregulation that contribute to adverse outcomes across these organ systems. Noncommunicable diseases are projected to become the dominant contributors to the global health burden between 2022 and 2050 (6). Among these, key elements of the CKM syndrome constitute the leading causes of death worldwide, including CVD, CKD (6). There are strong interrelationships among the 5 CKM components. In a retrospective cohort from Taiwan, nearly half (44.4%) of participants with at least one CKM component exhibited 2 or more components, 22.9% had 3 or more and 7.8% had 4 or more components (7). More than 1 in 4 adults in the US were found to have at least one cardiac, renal and metabolic condition, while nearly one in ten had overlapping cardiac, renal and metabolic conditions (8).
The potential association between psoriasis and vascular events was first recognized in 1973 (9). McDonald and Calabresi were the first to report that hospitalized patients with psoriasis had a 2.2-fold higher risk of vascular diseases compared to individuals with other skin disorders (10). The prevalence of metabolic syndrome among individuals with psoriasis has been reported to range between 20% and 50%, which is up to threefold higher than that observed in the general population (11, 12). Coronary artery disease (CAD) has been reported to occur with higher prevalence in individuals with psoriasis (13). Notably, myocardial infarction may represent the initial clinical presentation of CAD in these patients. Conversely, an increased prevalence of psoriasis has also been observed among patients diagnosed with CAD (14). Plenty of components of CKM syndrome, including obesity, type 2 diabetes, dyslipidaemia, nonalcoholic fatty liver disease and cardiovascular disease, are highly prevalent among individuals with psoriasis (15). Therefore, there might be a strong association between psoriasis and cardiometabolic disorders. The coexistence of cardiometabolic syndrome may exacerbate systemic inflammation and further contribute to the increased cardiovascular risk observed in psoriasis. Understanding this interaction is crucial, as it could inform targeted risk stratification and management strategies for patients with psoriasis.
However, prior evidence has largely focused on cardiovascular risk in psoriasis or CKM-related outcomes in isolation. Given the widespread prevalence of CKM syndrome in the general population, the joint influence of psoriasis and CKM syndrome is still unclear. Therefore, this study was aimed to investigate the interplay between psoriasis, CKM syndrome and mortality risk using data from the National Health and Nutrition Examination Survey (NHANES). Specifically, we sought to evaluate the impact of psoriasis, alone and in combination with CKM components on all-cause and cardio-cerebrovascular disease (CCD) mortality.
METHODS
Study population
This study was based on data from the National Health and Nutrition Examination Survey (NHANES), a nationally representative survey conducted by the Centers for Disease Control and Prevention (CDC). We included participants from the fasting subsample of NHANES 2003–2006 and 2009–2014 cycles, during which data on cardiovascular, kidney and metabolic biomarkers; psoriasis status; and mortality linkage were available. All NHANES protocols were approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board, and written informed consent was obtained from all participants.
The flow of participant selection is shown in Fig. 1. A total of 14,754 individuals were identified from the fasting subsample. After excluding participants aged <20 years and those with missing psoriasis data (n=4,840), 9,914 individuals remained. We further excluded pregnant participants (n=305) and those without follow-up mortality information (n=11), resulting in a final analytic sample of 9,598 participants.
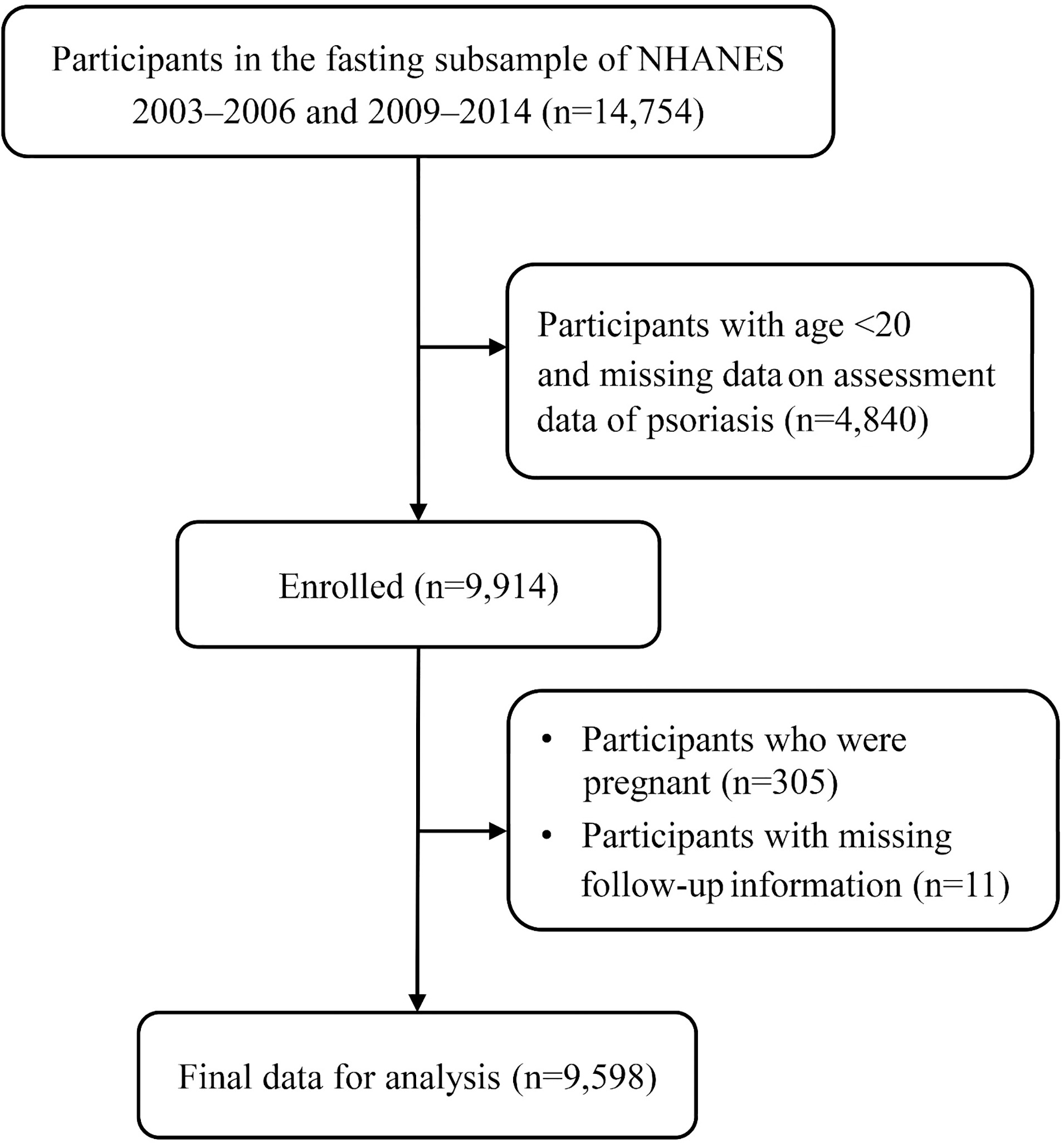
Fig. 1. Flowchart of participant selection.
Definition of cardiovascular-kidney-metabolic syndrome
CKM syndrome stages were defined according to the 2023 AHA Presidential Advisory (16), with modifications based on data availability in NHANES (17). Participants were classified into 5 mutually exclusive stages (Stage 0 to Stage 4) based on the presence and severity of metabolic risk factors, kidney function and cardiovascular disease status. Stage 0 included individuals with no metabolic risk factors. Stage 1 indicated excess or dysfunctional adiposity without additional metabolic abnormalities. Stage 2 represented the presence of metabolic risk factors or moderate-to-high-risk chronic kidney disease (CKD). Stage 3 reflected subclinical cardiovascular disease or very high-risk CKD, and Stage 4 included individuals with clinically established cardiovascular disease. Detailed definitions and classification criteria are presented in Table SI. Consistent with a prior study by Aggarwal et al. (17), individuals in Stage 3 or 4 were further categorized as having advanced CKM syndrome, representing those with subclinical or established cardiovascular involvement and/or severe kidney dysfunction.
Assessment of psoriasis status
Psoriasis was defined based on participants’ self-reported responses to the question, “Has a doctor or other health professional ever told you that you had psoriasis?” Individuals who answered “yes” were classified as having psoriasis, while those who answered “no” were considered not to have psoriasis. Participants with missing responses to this question were excluded from the analysis. This information was obtained from the dermatology questionnaire administered during the NHANES 2003–2006 and 2009–2014 survey cycles.
Outcome variables
The primary outcome was all-cause mortality. The secondary outcome was cardio-cerebrovascular (CCD) mortality, defined as death due to cardiovascular disease or cerebrovascular disease. Mortality status and cause of death were ascertained through linkage to the National Death Index (NDI), with follow-up through December 31, 2019. Causes of death were classified using the International Classification of Diseases, 10th Revision (ICD-10). Cardiovascular mortality included underlying causes coded as I00–I09, I11, I13 and I20–I51, and cerebrovascular mortality included codes I60–I69.
Assessment of covariates
Relevant covariates were selected a priori based on prior evidence linking them to mortality (18, 19, 20). Demographic variables included age (20–39, 40–59 or ≥60 years), sex and race/ethnicity (non-Hispanic White, non-Hispanic Black or other). Socioeconomic factors included education level (less than high school, high school or above high school) and the family poverty income ratio (PIR), calculated as the ratio of total family income to the federal poverty threshold, categorized as ≤1.0, 1.1–3.0 or >3.0. Smoking status was self-reported and categorized as never (<100 cigarettes in a lifetime), former (≥100 cigarettes lifetime but not currently smoking) or current smoker. Alcohol consumption was categorized as nondrinker, low-to-moderate drinker (≤1 drink/day for women or ≤2 drinks/day for men) or heavy drinker (21, 22). Physical activity was assessed based on self-reported leisure-time activity and metabolic equivalent (MET) values, and participants were classified as inactive (no activity), insufficiently active (moderate activity 1–5 times/week or vigorous activity 1–3 times/week) or active (more frequent or intense activity) (21, 22).
Statistical analysis
All analyses accounted for the complex sampling design of NHANES using appropriate sample weights, strata and primary sampling units, as recommended by the NCHS. Continuous variables were expressed as weighted medians with interquartile ranges, and categorical variables were presented as weighted percentages. Differences in baseline characteristics by mortality status were assessed Wilcoxon rank-sum tests for continuous variables and χ2 tests for categorical variables.
The associations between CKM syndrome stages and the prevalence of psoriasis were evaluated using weighted logistic regression models, with results expressed as odds ratios (ORs) and 95% confidence intervals (CIs). Survey-weighted Kaplan–Meier curves and log-rank tests were used to compare cumulative mortality across CKM stages and psoriasis status. Cox proportional hazards regression models were used to estimate hazard ratios (HRs) and 95% CIs for all-cause and CCD mortality associated with CKM syndrome stages and psoriasis, separately and jointly. To assess multiplicative interaction between advanced CKM syndrome and psoriasis, a cross-product term was added to the survey-weighted Cox proportional hazards models.
Subgroup analyses were conducted across age, sex, race/ethnicity, education, PIR, smoking, drinking and physical activity, with interaction terms tested using the Wald test. Sensitivity analyses were performed by (1) excluding participants with missing covariate data and (2) excluding those who died within the first year of follow-up. All statistical analyses were conducted using R version 4.3.1 and the “survey” package. A two-sided p-value <0.05 was considered statistically significant.
RESULTS
Characteristics of the study participants
A total of 9,598 adults from NHANES 2003–2006 and 2009–2014 were included in the final analysis. Participants who died during follow-up were more likely to be older, male, non-Hispanic White, less educated and have lower income. They also had higher proportions of current or former smoking, heavy drinking and physical inactivity. Notably, the prevalence of advanced CKM syndrome (Stage 3 or 4) was significantly higher among those who died (47.9% vs 7.4%, p<0.01). The proportion of participants with psoriasis was also greater in the deceased group than in survivors (7.3% vs 2.8%, p<0.01). Full baseline characteristics stratified by all-cause mortality status are presented in Table I. In addition, baseline characteristics stratified by advanced CKM syndrome status are presented in Table SII.
Table I. Baseline characteristics of adults in NHANES 2003–2006 and 2009–2014, stratified by all-cause mortality status
| Characteristics | Total (n=9,598) | All-cause mortality | p-value | |
|---|---|---|---|---|
| No (n=8,738) | Yes (n=860) | |||
| Age, mean (SD) | <0.01 | |||
| 20–39 years | 3,571 (40.01) | 3,524 (42.43) | 47 (8.09) | |
| 40–59 years | 3,680 (42.27) | 3,434 (42.59) | 246 (37.93) | |
| ≥ 60 years | 2,347 (17.72) | 1,780 (14.97) | 567 (53.98) | |
| Sex, n (%) | <0.01 | |||
| Female | 4,883 (50.89) | 4,533 (51.45) | 350 (43.47) | |
| Male | 4,715 (49.11) | 4,205 (48.55) | 510 (56.53) | |
| Race/ethnicity, n (%) | <0.01 | |||
| Non-Hispanic white | 4,301 (67.71) | 3,786 (67.15) | 515 (75.08) | |
| Non-Hispanic black | 1,935 (11.57) | 1,768 (11.54) | 167 (11.92) | |
| Other | 3,362 (20.73) | 3,184 (21.31) | 178 (13.01) | |
| Education level, n (%) | <0.01 | |||
| Below high school | 2,344 (16.93) | 2,047 (16.18) | 297 (26.82) | |
| High school | 2,141 (22.35) | 1,924 (22.07) | 217 (26.00) | |
| Above high school | 5,113 (60.73) | 4,767 (61.75) | 346 (47.18) | |
| Family poverty income ratio, n (%) | <0.01 | |||
| ≤1.0 | 2,118 (15.10) | 1,912 (14.81) | 206 (18.97) | |
| 1.1–3.0 | 3,859 (35.47) | 3,435 (34.76) | 424 (44.88) | |
| >3.0 | 3,621 (49.42) | 3,391 (50.43) | 230 (36.14) | |
| Smoking status, n (%) | <0.01 | |||
| Never smoker | 5,359 (54.91) | 5,019 (56.21) | 340 (37.80) | |
| Former smoker | 2,146 (22.71) | 1,835 (21.96) | 311 (32.73) | |
| Current smoker | 2,093 (22.37) | 1,884 (21.83) | 209 (29.48) | |
| Drinking status, n (%) | 0.02 | |||
| Nondrinker | 1,881 (16.02) | 1,679 (15.71) | 202 (20.14) | |
| Low-to-moderate drinker | 6,894 (73.89) | 6,319 (74.27) | 575 (68.94) | |
| Heavy drinker | 823 (10.09) | 740 (10.03) | 83 (10.91) | |
| Physical activity, n (%) | <0.01 | |||
| Inactive | 2,347 (20.97) | 1,932 (19.18) | 415 (44.64) | |
| Insufficiently active | 3,595 (41.13) | 3,350 (41.94) | 245 (30.35) | |
| Active | 3,656 (37.90) | 3,456 (38.87) | 200 (25.01) | |
| Psoriasis, n (%) | <0.01 | |||
| No | 9,316 (96.90) | 8,517 (97.22) | 799 (92.71) | |
| Yes | 282 (3.10) | 221 (2.78) | 61 (7.29) | |
| CKM syndrome stage, n (%) | <0.01 | |||
| Stage 0 | 1,015 (12.73) | 999 (13.50) | 16 (2.55) | |
| Stage 1 | 2,013 (21.99) | 1,966 (23.19) | 47 (6.08) | |
| Stage 2 | 5,270 (55.07) | 4,952 (55.95) | 318 (43.43) | |
| Stage 3 | 400 (2.40) | 229 (1.47) | 171 (14.78) | |
| Stage 4 | 900 (7.81) | 592 (5.89) | 308 (33.16) | |
| Advanced CKM syndrome (Stage 3 or 4), n (%) | <0.01 | |||
| No | 8,298 (89.79) | 7,917 (92.64) | 381 (52.06) | |
| Yes | 1,300 (10.21) | 821 (7.36) | 479 (47.94) | |
| Follow-up time, years, median [IQR] | 9.25 [6.92, 13.75] | 9.58 [7.25, 13.92] | 5.42 [3.00, 7.83] | <0.01 |
|
n reflect the study sample while percentages reflect the survey-weighted data. CKM: Cardiovascular-Kidney-Metabolic; IQR: interquartile range; NHANES: National Health and Nutrition Examination Survey; SD: standard deviation. |
||||
Association between cardiovascular-kidney-metabolic syndrome and prevalence of psoriasis
The prevalence of psoriasis increased progressively across CKM syndrome stages (Table II). After full adjustment for demographic, socioeconomic and lifestyle factors, individuals in Stage 2, Stage 3 and Stage 4 had significantly higher odds of having psoriasis compared to those in Stage 0, with adjusted ORs of 2.17 (95% CI, 1.05–4.50), 2.89 (95% CI, 1.19–7.02) and 5.40 (95% CI, 2.34–12.50), respectively. Furthermore, participants classified as having advanced CKM syndrome (Stage 3 or 4) had over twofold higher odds of psoriasis compared with those without advanced CKM syndrome (adjusted OR, 2.40; 95% CI, 1.67–3.46; p<0.01).
Table II. Odds ratio (OR) (95% confidence intervals [CIs]) for the prevalence of psoriasis according to cardiovascular-kidney-metabolic (CKM) syndrome stages in adults: NHANES 2003–2006 and 2009–2014
| Crude | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | OR (95% CI) | p-value | |
| CKM syndrome stages | ||||||
| Stage 0 | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | |||
| Stage 1 | 1.87 (0.75–4.66) | 0.17 | 2.02 (0.81–5.05) | 0.13 | 1.96 (0.78–4.94) | 0.15 |
| Stage 2 | 2.10 (1.03–4.29) | 0.04 | 2.23 (1.08–4.60) | 0.03 | 2.17 (1.05–4.50) | 0.04 |
| Stage 3 | 2.49 (1.02–6.06) | 0.04 | 2.96 (1.26–6.94) | 0.01 | 2.89 (1.19–7.02) | 0.02 |
| Stage 4 | 5.00 (2.30–10.86) | <0.01 | 5.44 (2.39–12.39) | <0.01 | 5.40 (2.34–12.50) | <0.01 |
| P for trend | <0.01 | <0.01 | <0.01 | |||
| Advanced CKM syndrome (Stages 3 or 4) | ||||||
| No | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | |||
| Yes | 2.33 (1.72–3.15) | <0.01 | 2.39 (1.64–3.48) | <0.01 | 2.40 (1.67–3.46) | <0.01 |
|
Model 1 was adjusted for age (20–39, 40–59, or ≥60), sex (male or female) and race/ethnicity (Non-Hispanic White, Non-Hispanic Black or Other); Model 2 was adjusted as model 1 plus education level (below high school, high school, or above high school), family PIR (≤1.0, 1.1–3.0, or >3.0), smoking status (never smoker, former smoker, or current smoker), drinking status (nondrinker, low-to-moderate drinker, or heavy drinker) and physical activity (inactive, insufficiently active, or active). NHANES: National Health and Nutrition Examination Survey; PIR: poverty income ratio. |
||||||
Association of cardiovascular-kidney-metabolic syndrome and psoriasis with all-cause and cardio-cerebrovascular disease mortality
During a median follow-up of 9.3 years, 860 participants died from all causes. As illustrated in Fig. 2A and B, individuals with advanced CKM syndrome or psoriasis had significantly higher cumulative incidence of all-cause mortality compared to those without these conditions (p for log-rank test <0.001 for both). In multivariable-adjusted Cox regression models (Table III), the risk of all-cause mortality increased progressively with advancing CKM syndrome stage. Compared with Stage 0, the fully adjusted hazard ratios (HRs) were 2.27 (95% CI: 1.26–4.09) for Stage 2, 8.84 (95% CI: 4.67–16.73) for Stage 3 and 7.15 (95% CI: 3.81–13.44) for Stage 4. Individuals with advanced CKM syndrome (Stages 3 or 4) had a 267% increased risk of all-cause mortality (HR 3.67; 95% CI: 3.00–4.50) compared with those without. Additionally, psoriasis was associated with a 106% higher risk of all-cause mortality (HR 2.06; 95% CI: 1.47–2.90).
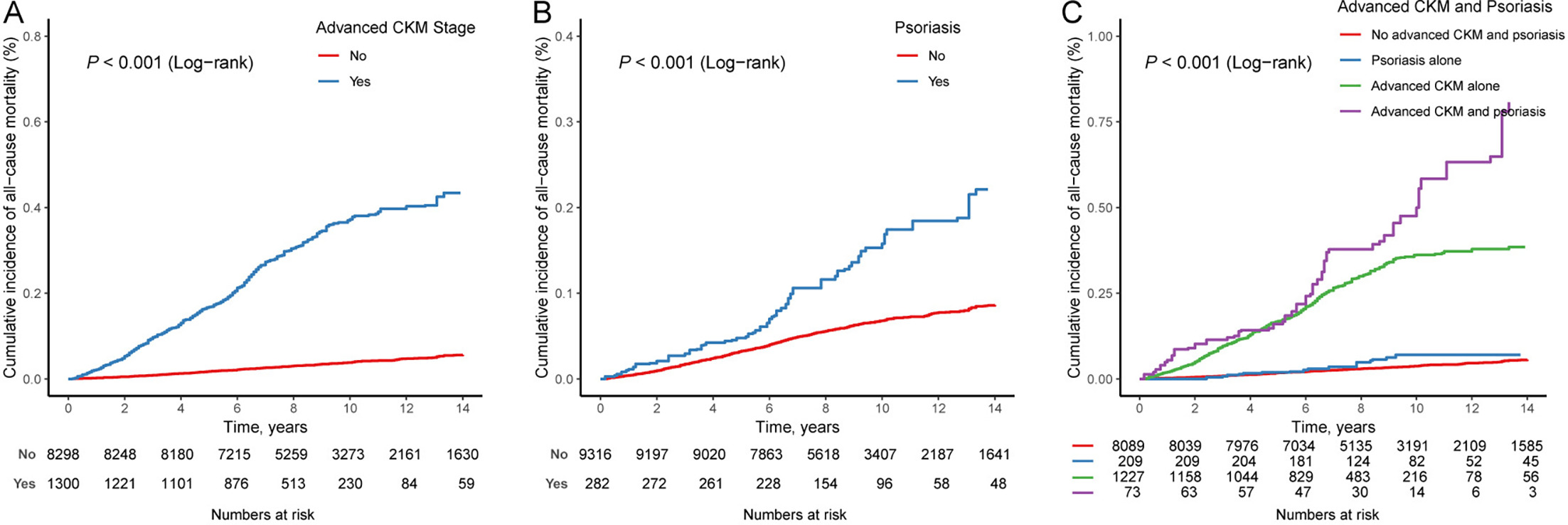
Fig. 2. Kaplan–Meier survival curves for all-cause mortality according to CKM syndrome stages and psoriasis status. (A) All-cause mortality by advanced CKM syndrome status (Stages 3 or 4 vs Stages 0–2). (B) All-cause mortality by presence or absence of psoriasis. (C) Joint association of advanced CKM syndrome and psoriasis with all-cause mortality.
Table III. Hazard ratios (HRs) (95% confidence intervals [CIs]) for all-cause mortality according to cardiovascular-kidney-metabolic (CKM) syndrome stages or psoriasis in adults: NHANES 2003–2006 and 2009–2014
| Crude | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value | |
| CKM syndrome stages | ||||||
| Stage 0 | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | |||
| Stage 1 | 1.53 (0.82–2.84) | 0.18 | 1.22 (0.65–2.30) | 0.54 | 1.21 (0.62–2.34) | 0.58 |
| Stage 2 | 4.31 (2.55–7.26) | <0.01 | 2.50 (1.43–4.37) | 0.001 | 2.27 (1.26–4.09) | 0.01 |
| Stage 3 | 56.30 (33.37–94.96) | <0.01 | 11.99 (6.57–21.87) | <0.01 | 8.84 (4.67–16.73) | <0.01 |
| Stage 4 | 30.15 (17.34–52.43) | <0.01 | 9.54 (5.20–17.50) | <0.01 | 7.15 (3.81–13.44) | <0.01 |
| Advanced CKM syndrome (Stages 3 or 4) | ||||||
| No | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | |||
| Yes | 11.16 (9.21–13.51) | <0.01 | 4.59 (3.71–5.68) | <0.01 | 3.67 (3.00–4.50) | <0.01 |
| Psoriasis | ||||||
| No | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | |||
| Yes | 2.43 (1.81–3.26) | <0.01 | 2.18 (1.54–3.08) | <0.01 | 2.06 (1.47–2.90) | <0.01 |
|
Model 1 was adjusted for age (20–39, 40–59, or ≥60), sex (male or female) and race/ethnicity (Non-Hispanic White, Non-Hispanic Black or Other); Model 2 was adjusted as model 1 plus education level (below high school, high school, or above high school), family PIR (≤1.0, 1.1–3.0, or >3.0), smoking status (never smoker, former smoker, or current smoker), drinking status (nondrinker, low-to-moderate drinker, or heavy drinker) and physical activity (inactive, insufficiently active, or active). NHANES: National Health and Nutrition Examination Survey; PIR: poverty income ratio. |
||||||
Kaplan–Meier curves further demonstrated a higher cumulative incidence of CCD mortality among individuals with advanced CKM syndrome or psoriasis (Fig. S1). In fully adjusted models (Table SIII), participants with advanced CKM syndrome had a markedly elevated risk of CCD mortality (HR=8.16; 95% CI: 5.42–12.28) compared with those without. Similarly, psoriasis was associated with a 169% higher risk of CCD mortality (HR 2.69; 95% CI: 1.42–5.08).
Joint associations of cardiovascular-kidney-metabolic syndrome and psoriasis with all-cause and cardio-cerebrovascular disease mortality
As shown in Fig. 2C, the Kaplan–Meier survival curves indicated that participants with both advanced CKM syndrome and psoriasis had the highest cumulative mortality compared with other groups (p for log-rank <0.001). In the fully adjusted model (Table IV), advanced CKM syndrome alone was associated with higher all-cause mortality (HR=3.45; 95% CI: 2.81–4.23), whereas psoriasis alone was not significantly associated with all-cause mortality (HR=1.28; 95% CI: 0.68–2.39). Participants with both advanced CKM syndrome and psoriasis had the highest observed all-cause mortality risk (HR=7.09; 95% CI: 4.93–10.19). The multiplicative interaction between advanced CKM syndrome and psoriasis was not statistically significant (p for interaction = 0.16).
Table IV. Hazard ratios (HRs) (95% confidence intervals [CIs]) for all-cause mortality according to the joint association of cardiovascular-kidney-metabolic (CKM) syndrome stages and psoriasis in adults: NHANES 2003–2006 and 2009–2014
| Crude | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value | |
| All-cause mortality | ||||||
| No advanced CKM and psoriasis | 1.00 [Reference] | 1.00 [Reference] | 1.00 [Reference] | |||
| Psoriasis alone | 1.36 (0.75–2.45) | 0.31 | 1.29 (0.70–2.38) | 0.41 | 1.28 (0.68–2.39) | 0.44 |
| Advanced CKM alone | 10.71 (8.80–13.02) | <0.01 | 4.33 (3.51–5.34) | <0.01 | 3.45 (2.81–4.23) | <0.01 |
| Advanced CKM and psoriasis | 19.59 (13.87–27.66) | <0.01 | 9.12 (6.13–13.58) | <0.01 | 7.09 (4.93–10.19) | <0.01 |
| P for interaction | 0.33 | 0.13 | 0.16 | |||
|
Model 1 was adjusted for age (20–39, 40–59, or ≥60), sex (male or female) and race/ethnicity (Non-Hispanic White, Non-Hispanic Black or Other); Model 2 was adjusted as model 1 plus education level (below high school, high school, or above high school), family PIR (≤1.0, 1.1–3.0, or >3.0), smoking status (never smoker, former smoker, or current smoker), drinking status (nondrinker, low-to-moderate drinker, or heavy drinker) and physical activity (inactive, insufficiently active, or active). NHANES:National Health and Nutrition Examination Survey; PIR:poverty income ratio. |
||||||
Similarly, Kaplan–Meier curves for CCD mortality (Fig. S1C) revealed the highest mortality among individuals with both advanced CKM syndrome and psoriasis. In fully adjusted models (Table SIV), advanced CKM syndrome alone was associated with higher CCD mortality (HR=7.68; 95% CI: 5.35–11.04), whereas psoriasis alone was not significantly associated with CCD mortality. Participants with both advanced CKM syndrome and psoriasis had the highest observed CCD mortality risk (HR=16.47; 95% CI: 7.26–37.33). No significant multiplicative interaction was observed for CCD mortality (P for interaction=0.80).
Stratified and sensitivity analyses
Stratified analyses showed that the association between the coexistence of advanced CKM syndrome and psoriasis and all-cause mortality was generally consistent across most subgroups (Table SV). Significant interactions were found for smoking status (p=0.01), drinking status (P = 0.03) and physical activity (p<0.01), indicating stronger associations in current smokers, heavy drinkers and those who were insufficiently active. No significant interactions were observed across age, sex, race/ethnicity, education level or family PIR.
Sensitivity analyses confirmed the robustness of the primary findings. After excluding participants with missing covariate data, those with both advanced CKM syndrome and psoriasis remained at increased risk of all-cause mortality (HR=6.91; 95% CI: 4.77–10.02) and CCD mortality (HR=15.54; 95% CI: 6.55–36.88) (Table SVI). Similarly, after excluding individuals who died within the 1st year of follow-up, the associations persisted, with an adjusted HR of 6.99 (95% CI: 4.68–10.45) for all-cause mortality and 16.98 (95% CI: 7.27–39.62) for CCD mortality (Table SVII).
DISCUSSION
In this study, we investigated the joint association of psoriasis and CKM syndrome with all-cause mortality and CCD mortality in 9,598 U.S. adults. We found that both psoriasis and CKM syndrome were associated with increased risks of all-cause and CCD mortality. Moreover, individuals with both psoriasis and advanced CKM syndrome exhibited markedly higher mortality risks than those with either condition alone. However, formal interaction testing did not show a significant multiplicative interaction, suggesting that the joint association may primarily reflect the accumulation of risk across both conditions.
Our study demonstrated a clear, graded association between CKM syndrome severity and the prevalence of psoriasis. Notably, participants with advanced CKM syndrome had more than twice the likelihood of psoriasis. Even after adjusting for multiple demographic, socioeconomic and lifestyle factors, individuals in Stage 2, Stage 3 and Stage 4 had 2.17-, 2.89- and 5.40-fold higher odds of psoriasis compared to those without CKM syndrome. Recent trans-disease meta-analysis has identified shared genetic loci and prioritized genes such as IFIH1 and IL23A, which suggested overlapping inflammatory pathways between psoriasis and CAD (23). Moreover, Mendelian randomization indicated that CAD may causally increase psoriasis risk through systemic inflammation, independent of BMI and waist-to-hip ratio (23). These data reinforce the hypothesis that psoriatic inflammation is not confined to the skin but extends to systemic vasculature and metabolic pathways, which might contribute to a bidirectional relationship between psoriasis and CKM components.
Chronic psoriatic disease is increasingly recognized as a systemic inflammatory condition with significant cardiometabolic consequences (24). Moreover, solid evidence has been shown that psoriasis is associated with high risk of mortality. A recent NHANES-based study of 19,741 U.S. adults reported that moderate-to-severe psoriasis was associated with a 2.5-fold increased risk of CVD mortality (25). Mediation analyses in that study further suggested that 81.4% of the effect of moderate/severe psoriasis on CVD mortality was direct (25). Ashar et al. conducted a meta-analysis of 12 cohort studies and found pooled RRs for all-cause mortality of 1.13 (95% CI: 1.09–1.16) in mild psoriasis and 1.52 (95% CI: 1.35–1.71) in severe psoriasis (26). Similarly, cardiovascular mortality risks were elevated in severe psoriasis (RR: 1.38; 95% CI: 1.09–1.74) (26). Many studies showed that the majority of this effect was direct rather than through traditional cardiovascular risk factors. In our analysis, psoriasis was associated with an increased risk of all-cause and CCD mortality when modelled separately.
A growing body of evidence supports the prognostic value of CKM syndrome staging for mortality risk. In a large prospective cohort of 97,777 Chinese adults from the Kailuan Study, higher CKM stages were strongly associated with increased all-cause mortality over a median follow-up of 15 years (27). Similar findings have been reported in a U.S. population using data from 50,678 adults participating in the 1999–2018 NHANES. In this cohort, higher CKM stages were associated with progressively increased 15-year cumulative incidences of cardiovascular mortality (28). Tsai et al. found that compared with participants without CKM, the presence of CKM syndrome was linked to a 33% higher risk of all-cause mortality and a nearly 3-fold higher risk of cardiovascular mortality in a large-scale Taiwanese cohort study of 515,602 adults (7). Collectively, these findings support CKM staging as a useful framework for identifying individuals at elevated long-term mortality risk.
Notably, patients with both psoriasis and advanced CKM syndrome might face the highest mortality risks. Previous evidence suggests that psoriasis frequently coexists with cardiometabolic risk factors and may identify individuals with greater systemic disease burden. Zhao et al. suggested that individuals with psoriasis exhibited a higher prevalence of hypertension compared with those without psoriasis (29). Furthermore, the coexistence of psoriasis and hypertension was associated with a substantially elevated risk of all-cause mortality (HR=2.33; 95% CI: 1.60–3.40), which exceeded the risk conferred by hypertension alone (HR=1.78; 95% CI: 1.55–2.04) (29). Similarly, individuals with both psoriasis and CKD had a dramatically increased risk of all-cause mortality (HR=5.38; 95% CI: 2.43–11.91) compared to those without either condition (30). Previous evidence also suggested a synergistic interaction between systemic inflammation in psoriasis and metabolic dysregulation (31). In our analysis, advanced CKM syndrome was associated with a 3.45-fold increased risk of all-cause mortality, whereas the coexistence of advanced CKM syndrome and psoriasis further elevated this risk to 7.09-fold. Similar patterns were observed for CCD mortality, where participants with both conditions had a more than 16-fold increased risk compared to those without either condition.
The observed associations may reflect shared pathophysiological pathways between psoriasis and CKM syndrome, including chronic systemic inflammation, immune dysregulation, endothelial dysfunction and accelerated atherosclerosis. Psoriasis has long been recognized as a T cell–mediated inflammatory disease and elevated proinflammatory cytokines such as TNF-α and IL-6, which are also implicated in insulin resistance, dyslipidaemia and vascular injury (32). Although early studies emphasized the role of T helper 1 (Th1) cells, accumulating evidence highlights the pivotal contribution of T helper 17 (Th17) cells and other IL-17–producing subsets to its pathogenesis (3, 33). Importantly, these immune pathways are also critically involved in the development of atherosclerosis. In metabolic disorders, such as diabetes and obesity, IL-23/Th17-driven inflammation has been associated with β-cell dysfunction and adipose tissue immune dysregulation (34). Similar pro-inflammatory mechanisms involving IL-23 and related cytokines have been identified in non-alcoholic fatty liver disease and other conditions linked to metabolic syndrome (34). Similarly, CKM syndrome involves multisystem metabolic derangements that amplify cardiovascular and renal risk. The coexistence of these conditions may reflect a greater inflammatory, metabolic and vascular burden, thereby increasing the risk of adverse outcomes. Furthermore, metabolic factors such as obesity, dyslipidaemia and diabetes are not only highly prevalent in psoriasis patients but are also associated with greater disease severity and reduced response to treatment (35). The “two plaques for one syndrome” concept also highlights shared inflammatory features between psoriatic skin plaques and atherosclerotic vascular plaques (36). These overlapping pathways may partly explain the higher mortality observed among participants with both psoriasis and advanced CKM syndrome, although the underlying mechanisms require further investigation.
To our knowledge, this is the first study to quantify the joint impact of psoriasis and CKM syndrome on long-term mortality. Utilizing data from a large, nationally representative cohort of U.S. adults with long-term follow-up, we assessed different CKM stages and the combinations of CKM syndrome and psoriasis and explored their associated risk with all-cause mortality and CCD mortality. Furthermore, the simultaneous evaluation of psoriasis and CKM syndrome provided novel insights into their individual and combined associations with mortality. The observed stronger associations among smokers, heavy drinkers and physically inactive individuals also suggest that modifiable lifestyle factors may exacerbate mortality risks in this population. Our findings emphasize that psoriasis is not merely a skin disease but a systemic condition. When combined with cardiometabolic dysfunction, it may identify individuals with particularly elevated mortality risk. Clinicians should be vigilant for cardiometabolic comorbidities in psoriasis patients and consider early interventions to mitigate long-term risks.
Limitations
However, several limitations should be acknowledged. First, the observational design of our study precludes causal inference, and residual confounding may persist despite multivariable adjustment. Second, psoriasis was defined by self-reported physician diagnosis, which may have introduced exposure misclassification. In addition, information on psoriasis severity, disease duration, lesion extent, treatment and changes in psoriasis or CKM status during follow-up was unavailable; therefore, the observed associations should be interpreted as estimates for a heterogeneous psoriasis population rather than severity-specific effects. Third, the study population was derived from U.S. adults participating in NHANES, and caution is warranted when generalizing these findings to other populations. Fourth, CKM stage 4 includes clinically established cardiovascular disease, creating partial overlap with CCD mortality and potentially inflating the estimates for advanced CKM syndrome. These results should therefore be viewed as reflecting the prognostic burden captured by CKM staging. Finally, the relatively small number of participants with psoriasis, particularly those with concurrent advanced CKM syndrome, limited the precision of joint and subgroup analyses; therefore, these findings should be interpreted with caution.
Conclusion
In this nationally representative cohort of U.S. adults, both advanced CKM syndrome and psoriasis were associated with increased risks of all-cause and CCD mortality. Furthermore, their coexistence conferred the highest mortality risk, although no significant multiplicative interaction was observed. These findings underscore the importance of comprehensive risk assessment and integrated management strategies for individuals with concurrent metabolic dysfunction and inflammatory skin diseases such as psoriasis.
ACKNOWLEDGEMENTS
We appreciate the people who contributed to the NHANES data we studied.
REFERENCES
- Armstrong AW, Mehta MD, Schupp CW, Gondo GC, Bell SJ, Griffiths CEM. Psoriasis prevalence in adults in the United States. JAMA Dermatol 2021; 157: 940–946. https://doi.org/10.1001/jamadermatol.2021.2007
- Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA 2020; 323: 1945–1960. https://doi.org/10.1001/jama.2020.4006
- Masson W, Lobo M, Molinero G. Psoriasis and cardiovascular risk: a comprehensive review. Adv Ther 2020; 37: 2017–2033. https://doi.org/10.1007/s12325-020-01346-6
- Takeshita J, Grewal S, Langan SM, Mehta NN, Ogdie A, Van Voorhees AS, et al. Psoriasis and comorbid diseases. J Am Acad Dermatol 2017; 76: 377–390. https://doi.org/10.1016/j.jaad.2016.07.064
- Ndumele CE, Rangaswami J, Chow SL, Neeland IJ, Tuttle KR, Khan SS, et al. Cardiovascular-kidney-metabolic health: a presidential advisory from the American Heart Association. Circulation 2023; 148: 1606–1635. https://doi.org/10.1161/CIR.0000000000001184
- Vollset SE, Ababneh HS, Abate YH, Abbafati C, Abbasgholizadeh R, Abbasian M, et al. Burden of disease scenarios for 204 countries and territories, 2022–2050: a forecasting analysis for the Global Burden of Disease Study 2021. Lancet 2024; 403: 2204–2256. https://doi.org/10.1016/S0140-6736(24)00685-8
- Tsai MK, Kao JTW, Wong CS, Liao CT, Lo WC, Chien KL, et al. Cardiovascular-kidney-metabolic syndrome and all-cause and cardiovascular mortality: a retrospective cohort study. PLoS Med 2025; 22: e1004629. https://doi.org/10.1371/journal.pmed.1004629
- Ostrominski JW, Arnold SV, Butler J, Fonarow GC, Hirsch JS, Palli SR, et al. Prevalence and overlap of cardiac, renal, and metabolic conditions in US adults, 1999–2020. JAMA Cardiol 2023; 8: 1050–1060. https://doi.org/10.1001/jamacardio.2023.3241
- McDonald CJ, Calabresi P. Thromboembolic disorders associated with psoriasis. Arch Dermatol 1973; 107: 918.
- McDonald CJ, Calabresi P. Occlusive vascular disease in psoriatic patients. N Engl J Med 1973; 288: 912.
- Singh S, Young P, Armstrong AW. Relationship between psoriasis and metabolic syndrome: a systematic review. G Ital Dermatol Venereol 2016; 151: 663–677.
- Chan WMM, Yew YW, Theng TSC, Liew CF, Oon HH. Prevalence of metabolic syndrome in patients with psoriasis: a cross-sectional study in Singapore. smedj 2020; 61: 194–199. https://doi.org/10.11622/smedj.2019152
- Furue M, Tsuji G, Chiba T, Kadono T. Cardiovascular and metabolic diseases comorbid with psoriasis: beyond the skin. Intern Med 2017; 56: 1613–1619. https://doi.org/10.2169/internalmedicine.56.8209
- Picard D, Bénichou J, Sin C, Abasq C, Houivet E, Koning R, et al. Increased prevalence of psoriasis in patients with coronary artery disease: results from a case–control study. Br J Dermatol 2014; 171: 580–587. https://doi.org/10.1111/bjd.13155
- Pannu S, Rosmarin D. Psoriasis in patients with metabolic syndrome or type 2 diabetes mellitus: treatment challenges. Am J Clin Dermatol 2021; 22: 293–300. https://doi.org/10.1007/s40257-021-00590-y
- Ndumele CE, Neeland IJ, Tuttle KR, Chow SL, Mathew RO, Khan SS, et al. A synopsis of the evidence for the science and clinical management of cardiovascular-kidney-metabolic (CKM) syndrome: a scientific statement from the American Heart Association. Circulation 2023; 148: 1636–1664. https://doi.org/10.1161/CIR.0000000000001186
- Aggarwal R, Ostrominski JW, Vaduganathan M. Prevalence of cardiovascular-kidney-metabolic syndrome stages in US adults, 2011–2020. JAMA 2024; 331: 1858–1860. https://doi.org/10.1001/jama.2024.6892
- Zhu X, Cheang I, Fu Y, Chen S, Liang G, Yuan H, et al. Comparative discrimination of Life’s Simple 7, Life’s Essential 8, and Life’s Crucial 9: evaluating the impact of added complexity on mortality prediction. BMC Med 2025; 23: 265. https://doi.org/10.1186/s12916-025-04116-9
- Li J, Wei X. Association of cardiovascular-kidney-metabolic syndrome with all-cause and cardiovascular mortality: a prospective cohort study. Am J Prev Cardiol 2025; 22: 100985. https://doi.org/10.1016/j.ajpc.2025.100985
- Zheng Q, Cao Z, Teng J, Lu Q, Huang P, Zhou J. Association between atherogenic index of plasma with all-cause and cardiovascular mortality in individuals with Cardiovascular-Kidney-Metabolic syndrome. Cardiovasc Diabetol 2025; 24: 183. https://doi.org/10.1186/s12933-025-02742-4
- Qiu Z, Chen X, Geng T, Wan Z, Lu Q, Li L, et al. Associations of serum carotenoids with risk of cardiovascular mortality among individuals with type 2 diabetes: results from NHANES. Diabetes Care 2022; 45: 1453–1461. https://doi.org/10.2337/dc21-2371
- Zhu X, Cheang I, Tang Y, Shi M, Zhu Q, Gao R, et al. Associations of serum carotenoids with risk of all-cause and cardiovascular mortality in hypertensive adults. J Am Heart Assoc 2023; 12: e027568. https://doi.org/10.1161/JAHA.122.027568
- Patrick MT, Li Q, Wasikowski R, Mehta N, Gudjonsson JE, Elder JT, et al. Shared genetic risk factors and causal association between psoriasis and coronary artery disease. Nat Commun 2022; 13: 6565. https://doi.org/10.1038/s41467-022-34323-4
- Egeberg A, Skov L, Joshi AA, Mallbris L, Gislason GH, Wu JJ, et al. The relationship between duration of psoriasis, vascular inflammation, and cardiovascular events. J Am Acad Dermatol 2017; 77: 650–656.. https://doi.org/10.1016/j.jaad.2017.06.028
- Kan J, Chen Q, Tao Q, Wu L, Wang D, Jiang Z, et al. Prospective evaluation of cardiovascular risk and mortality in patients with psoriasis: an American population-based study. Exp Dermatol 2024; 33: e15010. https://doi.org/10.1111/exd.15010
- Dhana A, Yen H, Yen H, Cho E. All-cause and cause-specific mortality in psoriasis: a systematic review and meta-analysis. J Am Acad Dermatol 2019; 80: 1332–1343. https://doi.org/10.1016/j.jaad.2018.12.037
- Li N, Li Y, Cui L, Shu R, Song H, Wang J, et al. Association between different stages of cardiovascular-kidney-metabolic syndrome and the risk of all-cause mortality. Atherosclerosis 2024; 397: 118585. https://doi.org/10.1016/j.atherosclerosis.2024.118585
- Claudel SE, Schmidt IM, Waikar SS, Verma A. Cumulative incidence of mortality associated with cardiovascular-kidney-metabolic (CKM) syndrome. J Am Soc Nephrol 2025; 36: 1343–1351. https://doi.org/10.1681/ASN.0000000637
- Zhao H, Wu J, Wu Q. Synergistic impact of psoriasis and hypertension on all-cause mortality risk: a prospective cohort study. PLoS One 2024; 19: e0306048. https://doi.org/10.1371/journal.pone.0306048
- Lu J, Li H, Wang S. Interaction effect of psoriasis and chronic kidney disease on the risk of all-cause mortality: a prospective cohort study of NHANES data. Nephrol Dial Transplant 2023; 38: 2474–2484. https://doi.org/10.1093/ndt/gfad089
- Kong X, Wang W. Synergistic effect of psoriasis and metabolic syndrome on risk of all-cause and cardiovascular mortality in US adults: a nationwide cohort study. Clin Exp Dermatol 2024; 50: 113–119. https://doi.org/10.1093/ced/llae340
- Piaserico S, Orlando G, Messina F. Psoriasis and cardiometabolic diseases: shared genetic and molecular pathways. Int J Mol Sci 2022; 23: 23. https://doi.org/10.3390/ijms23169063
- Armstrong AW, Blauvelt A, Callis Duffin K, Huang YH, Savage LJ, Guo L, et al. Psoriasis. Nat Rev Dis Primers 2025; 11: 45. https://doi.org/10.1038/s41572-025-00630-5
- Egeberg A, Gisondi P, Carrascosa JM, Warren RB, Mrowietz U. The role of the interleukin-23/Th17 pathway in cardiometabolic comorbidity associated with psoriasis. J Eur Acad Dermatol Venereol 2020; 34: 1695–1706. https://doi.org/10.1111/jdv.16273
- Pinter A, Schwarz P, Gerdes S, Simon JC, Saalbach A, Rush J, et al. Biologic treatment in combination with lifestyle intervention in moderate to severe plaque psoriasis and concomitant metabolic syndrome: rationale and methodology of the METABOLyx randomized controlled clinical trial. Nutrients 2021; 13: 3015. https://doi.org/10.3390/nu13093015
- Flammer AJ, Ruschitzka F. Psoriasis and atherosclerosis: two plaques, one syndrome? Eur Heart J 2012; 33: 1989–1991. https://doi.org/10.1093/eurheartj/ehr425