ORIGINAL REPORT
Association of Skin Dryness and Disease-related Parameters with Mechanical Alloknesis in Atopic Dermatitis: A Cross-sectional and Prospective Cohort Study
Masaru UTO1,2![]() , Eriko KOMIYA1,3*
, Eriko KOMIYA1,3*![]() , Go KOJIMA1,2
, Go KOJIMA1,2![]() , Yayoi KAMATA1
, Yayoi KAMATA1![]() , Sumika TOYAMA1
, Sumika TOYAMA1![]() , Kotaro HONDA1
, Kotaro HONDA1![]() , Takahide KANEKO2
, Takahide KANEKO2![]() , Yasushi SUGA2
, Yasushi SUGA2![]() , Mitsutoshi TOMINAGA1
, Mitsutoshi TOMINAGA1![]() and Kenji TAKAMORI1,2*
and Kenji TAKAMORI1,2*![]()
1Juntendo Itch Research Center (JIRC), Institute for Environmental and Gender-Specific Medicine, Juntendo University Graduate School of Medicine, 2-1-1 Tomioka, Urayasu, Chiba 279-0021, Japan, 2Department of Dermatology, Juntendo University Urayasu Hospital, 2-1-1 Tomioka, Urayasu, Chiba 279-0021, Japan, and 3Laboratory of Functional Morphology, Faculty of Pharmacy/Graduate School of Pharmacy and Pharmaceutical Science, Juntendo University, 6-8-1 Hinode, Urayasu, Chiba 279-0013, Japan
Corr: Eriko Komiya, Juntendo Itch Research Center (JIRC), Institute for Environmental and Gender-Specific Medicine, Juntendo University Graduate School of Medicine, 2-1-1 Tomioka, Urayasu, Chiba, Japan and Kenji Takamori, Juntendo Itch Research Center (JIRC), Institute for Environmental and Gender-Specific Medicine, Juntendo University Graduate School of Medicine, 2-1-1 Tomioka, Urayasu, Chiba, Japan. *Emails: ekomiya@juntendo.ac.jp; ktakamor@juntendo.ac.jp
Key words: observational study; atopic dermatitis; pruritus; chemokine CCL17; dupilumab.
Citation: Acta Derm Venereol 2026; 106: adv-2025-0246. DOI: https://doi.org/10.2340/actadv.v106.adv-2025-0246.
Copyright: 2026 ©Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Dec 5, 2025. Accepted after revision: Apr 15, 2026.
Published: Jun 10, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
Data are available from the corresponding author upon reasonable request.
This study complied with the Declaration of Helsinki and was approved by the Ethics Committee of Juntendo University (U20-0057). Written informed consent was obtained from all participants. The study was originally registered in UMIN (UMIN000059524), but no intervention was performed after protocol amendment; only the observational component is reported.
Mechanical alloknesis, namely itch hypersensitivity evoked by normally innocuous mechanical stimuli, may exacerbate the itch–scratch cycle in atopic dermatitis. Although various molecular and neural pathways have been identified in animal models, the clinical mechanisms underlying mechanical alloknesis remain unclear, particularly in relation to disease severity and biomarkers. We hypothesized that atopic dermatitis severity-related parameters are associated with mechanical alloknesis. To investigate this, we performed a cross-sectional study comparing healthy controls and atopic dermatitis patients and a prospective cohort study evaluating atopic dermatitis patients receiving dupilumab. In the cross-sectional study, mechanical alloknesis scores were significantly higher in lesional than in non-lesional or healthy skin. Skin dryness parameters (transepidermal water loss and stratum corneum hydration) showed no significant correlation with mechanical alloknesis. Among serum biomarkers, only thymus and activation-regulated chemokine (TARC) levels showed a moderate positive correlation with mechanical alloknesis but not with spontaneous itch. In the prospective study, dupilumab significantly reduced eosinophil counts, IgE, TARC, spontaneous itch and mechanical alloknesis scores, although TARC remained correlated with mechanical alloknesis after treatment. These findings suggest that TARC may be involved in the induction of mechanical alloknesis and represent a potential biomarker or therapeutic target for mechanical alloknesis in atopic dermatitis.
SIGNIFICANCE
Atopic dermatitis patients often experience not only spontaneous itch but mechanical alloknesis, namely itch triggered by normally innocuous mechanical stimuli. mechanical alloknesis, especially in lesional skin, may promote a vicious itch–scratch cycle that aggravates inflammatory skin pathology. Although many molecules and neural circuits involved in mechanical alloknesis have been identified in animal models, the underlying factors in clinical settings remain unclear. In this study involving healthy controls and atopic dermatitis patients, serum TARC levels were found to be correlated with mechanical alloknesis but not spontaneous itch, suggesting TARC may be at least partly involved in the mechanisms underlying mechanical alloknesis in atopic dermatitis.
Atopic dermatitis (AD) is a chronic inflammatory skin disease characterized by intense itching and recurrent eczematous lesions (1, 2). Pruritus (itch) is one of the most burdensome and distressing symptoms in patients with AD (3). In addition to persistent spontaneous itch, patients with AD frequently exhibit “mechanical alloknesis (MA)," a form of itch hypersensitivity elicited by normally innocuous mechanical stimuli (4, 5). MA, particularly in lesional skin, can occur as a result of scratching behaviour itself acting as a mechanical stimulus, and is thought to serve as a trigger for the vicious itch–scratch cycle, thereby exacerbating inflammatory conditions (6).
Animal studies have identified multiple molecular and neural pathways involved in MA, including mechanoreceptors, spinal neuronal circuits, and type 2 cytokine–mediated neuronal sensitization (7, 8, 9, 10, 11, 12, 13). However, the extent to which these experimental findings are relevant to AD in clinical practice remains unclear, as does the relationship between commonly used clinical parameters and MA.
We hypothesized that disease-related parameters used in routine clinical practice may be associated with the induction or modulation of MA in AD. To clarify the clinical characteristics and potential mechanisms of MA in AD, we performed a cross-sectional study comparing healthy controls and patients with AD, followed by a prospective cohort study of dupilumab-treated AD patients. Both studies examined the associations of MA with skin dryness parameters; transepidermal water loss (TEWL) and stratum corneum (SC) hydration; and disease-related parameters, including Eczema Area and Severity Index (EASI), eosinophil counts (Eos), immunoglobulin E (IgE), and thymus and activation-regulated chemokine (TARC).
MATERIALS AND METHODS
Study design and participants
This clinical study comprised a cross-sectional study (STEP 1 and STEP 2, shown in Fig. 1) and a prospective cohort study (STEP 3, shown in Fig. 1). In STEP 1, spontaneous itch, mechanical alloknesis (MA), and skin dryness were compared between healthy controls (n=30) and patients with atopic dermatitis (AD) (n=32). In STEP 2, a cross-sectional sub-analysis was conducted in 24 AD patients to examine correlations between MA scores and disease-related parameters, including Eczema Area and Severity Index (EASI), eosinophil counts (Eos), IgE, and thymus and activation-regulated chemokine (TARC). In STEP 3, a prospective cohort analysis was conducted in AD patients who selected dupilumab treatment (n=17 at enrollment), of whom 10 patients who completed all scheduled visits were included in the final analysis. Recruitment was conducted continuously from April 2021 through March 2025. Detailed eligibility criteria and study procedures are provided in the Appendix S1.
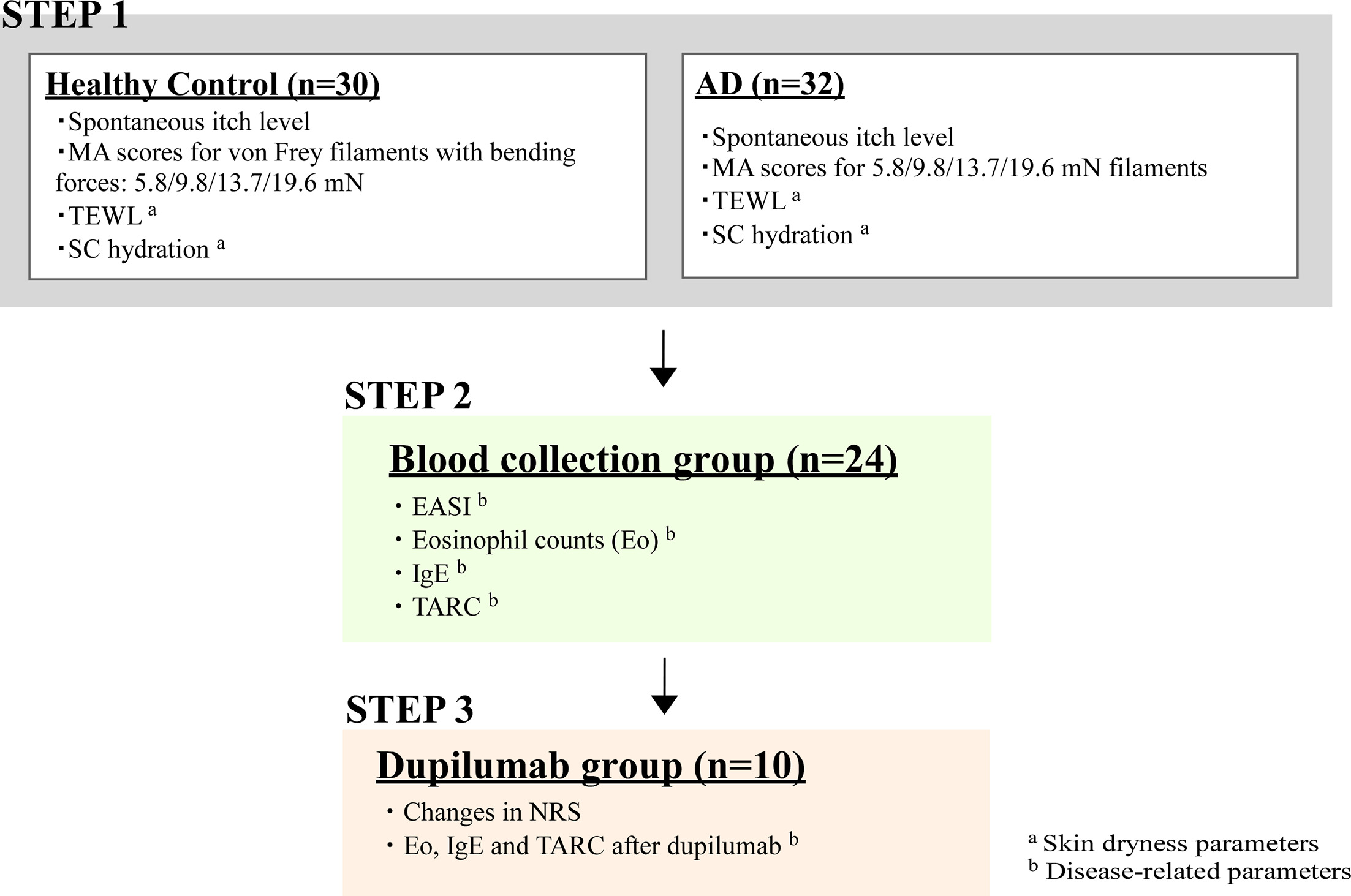
Fig. 1. Outline and participants of this study. Healthy controls and atopic dermatitis (AD) patients aged 20–89 years participated in this study. In STEP 1, the levels of spontaneous itch, mechanical alloknesis (MA), and skin dryness were assessed in 30 controls and 32 AD patients. Itch intensity was evaluated using an numeric rating scale (NRS) from 0 to 10 under unstimulated conditions for spontaneous itch, and under stimulation with von Frey filaments (5.8, 9.8, 13.7 and 19.6 mN) for MA scores. Skin dryness was assessed by measuring transepidermal water loss (TEWL) and stratum corneum (SC) hydration. In STEP 2, 24 AD patients underwent blood sampling for the evaluation of disease-related parameters, including Eczema Area and Severity (EASI), eosinophil count (Eos), serum IgE and thymus- and activation-regulated chemokine (TARC) levels. Finally, in STEP 3, 17 AD patients with insufficient responses to standard treatments initiated dupilumab therapy; of these, 7 discontinued follow-up mainly due to scheduling difficulties and were excluded from the final analysis, while 10 patients completed nine consecutive administrations. Changes in spontaneous itch, MA scores, Eos, IgE and TARC levels were evaluated throughout the treatment period.
Outcomes and statistical analysis
This report followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations (14). The primary outcome was the MA score; secondary outcomes were spontaneous itch intensity, skin dryness and disease-related parameters. Spontaneous itch and MA were assessed by numerical rating scale, and skin dryness by transepidermal water loss and stratum corneum hydration. Group comparisons were analyzed using Student’s t-test or one-way ANOVA followed by Tukey’s or Dunnett’s post hoc test, as appropriate. Correlations were assessed using Pearson’s correlation coefficient, and categorical variables using Fisher’s exact test. A p-value < 0.05 was considered statistically significant. Detailed methods are provided in the Appendix S1.
Ethics
This study was approved by the Juntendo University ethics committee (U20-0057), conducted in accordance with the Declaration of Helsinki, and based on written informed consent from all participants. The study was conducted as an observational study; although initially registered with UMIN (UMIN000059524) based on the original protocol, the intervention was not implemented due to a change in plan.
RESULTS
Study outline and participants
This study was an observational investigation comprising cross-sectional and prospective cohort components. The study outline is shown in Fig. 1. A total of 62 participants were enrolled (32 patients with AD and 30 healthy controls), and STEP 1 was performed on all participants. Among them, 24 and 17 patients proceeded to STEPS 2 and 3, respectively (Fig. 1 and Table I). In STEP 3, 17 patients initiated dupilumab treatment (Fig. 1); however, 7 discontinued due to failure to maintain regular visits. Table I presents data from the 10 patients who completed all scheduled visits.
Table I. Demographic characteristics of study participants in STEPS 1–3
| Healthy controls (n=30) | AD (n=32) | p-value | |
|---|---|---|---|
| STEP 1 | |||
| Number of subjects | 30 | 32 | - |
| Age (years,mean±SD) | 45.3±12.2 | 33.3±11.1 | 0.0002** |
| Male:Female | 22:8 | 22:10 | 0.783 |
| STEP 2 | |||
| Number of subjects | - | 24 | |
| Age (years, mean±SD) | - | 31.5±10.4 | |
| Male:Female | - | 17:7 | |
| EASI (mean±SD) | - | 26.4±8.6 | |
| Eos (×109 cells/L, mean±SD) | - | 782.9±838.1 | |
| IgE (IU/ml, mean±SD) | - | 11973.2±15856.9 | |
| TARC (pg/ml, mean±SD) | - | 5265.8±5934.4 | |
| STEP 3 | |||
| Number of subjects | - | 10 | |
| Age (years, mean±SD) | - | 29.1±11.2 | |
| Male:Female | - | 6:4 | |
| EASI (mean±SD) | - | 29.0±6.2 | |
| Eos (×109 cells/L, mean±SD) | - | 605±333.2 | |
| IgE (IU/ml, mean±SD) | - | 11219±13024.2 | |
| TARC (pg/ml, mean±SD) | - | 4223.4±4038.1 | |
|
Demographic characteristics of study participants in STEP 1, STEP 2, and STEP 3. In STEP 1, the age of AD patients was significantly lower than that of healthy controls, while no significant difference was observed in the sex ratio between the two groups. Age was compared using a two-tailed Student’s t-test, and sex ratio was analyzed by Fisher’s exact test. STEP 2 involved 24 AD patients who underwent blood sampling for evaluation of disease-related parameters, including EASI, Eos, serum IgE and TARC levels. STEP 3 included 10 AD patients who received dupilumab therapy according to the standard regimen (a 600 mg loading dose followed by 300 mg every 2 weeks). Disease-related parameters (EASI, Eos, IgE and TARC) were obtained prior to treatment initiation. Data are expressed as the mean±SD. **p<0.01. AD:atopic dermatitis; EASI:Eczema Area and Severity Index; Eos:eosinophil count; IgE:immunoglobulin E; SD:standard deviation; TARC:thymus and activation-regulated chemokine. |
|||
Patterns of spontaneous itch and mechanical alloknesis in atopic dermatitis patients
In STEP 1, a cross-sectional study was performed in 32 AD patients and 30 healthy individuals (Fig. 1). Their demographic characteristics are shown in Table I. While AD patients were younger, there was no statistically significant sex difference between groups. The sites of healthy skin in controls and non-lesional skin in AD patients were confirmed to have an NRS score of 0 for spontaneous itch, and the AD lesional skin group showed significantly higher NRS scores compared to the other groups (Fig. 2a). MA scores were recorded as itch elicited by each mechanical stimulus itself, rather than as a change from ongoing spontaneous itch. MA scores were significantly higher in lesional AD skin than in healthy control skin or non-lesional AD skin at all filament forces (Fig. 2b). In contrast, healthy control skin and non-lesional AD skin showed a force-dependent increase in MA, with higher scores at stronger filament forces, whereas this trend was not evident in lesional AD skin. Detailed summary statistics are provided in Tables S2–S4.
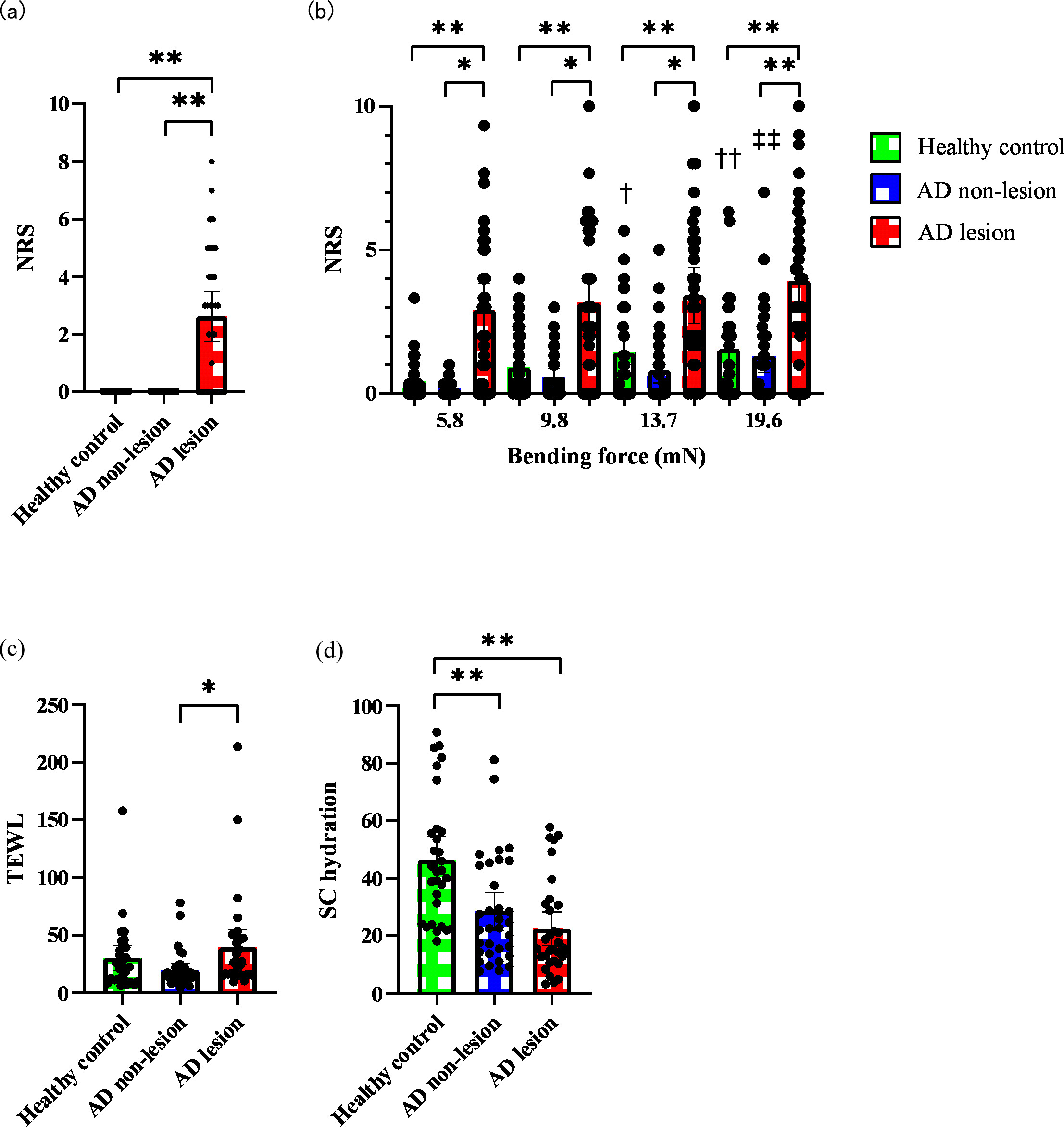
Fig. 2. Comparison of spontaneous itch, mechanical alloknesis (MA) scores and skin dryness in healthy controls and atopic dermatitis (AD) patients in STEP 1. Levels of (A) spontaneous itch, (B) MA (numeric rating scale scores) at bending forces of 5.8, 9.8, 13.7 and 19.6 mN, (C) transepidermal water loss, and (D) stratum corneum hydration were compared among healthy control, non-lesional and lesional skin sites in patients with AD. Statistical analyses were performed using one-way ANOVA followed by Tukey’s multiple-comparison test (*) to evaluate differences among groups (control, non-lesional and lesional skin), and Dunnett’s multiple-comparison test (†) to examine force-dependent changes in MA scores within each skin condition. *p<0.05, **p<0.01, †p<0.05, ††p<0.01, ‡‡p<0.01.
Correlation between itch level and skin dryness in atopic dermatitis patients
To evaluate skin dryness, TEWL and SC hydration were compared among healthy control skin, non-lesional AD skin and lesional AD skin (Fig. 2c, d). TEWL values in the lesional skin of AD patients were significantly higher than those in the non-lesional skin area, but no significant difference was observed compared with TEWL values in healthy skin (Fig. 2c, p=0.472). SC hydration values were significantly lower in both non-lesional and lesional AD skin than in healthy controls (Fig. 2d). Detailed values are shown in Tables S5 and S6. Pearson correlation analysis in the AD group revealed no significant correlation between spontaneous itch or MA scores and either TEWL or SC hydration in either lesional or non-lesional skin (Table S7).
Correlation between itch level and disease-related parameters in atopic dermatitis patients
STEP 2 was conducted as a cross-sectional sub-analysis among the AD patients included in STEP 1. Among the AD patients in STEP 1, 24 who underwent blood sampling during routine medical examinations were included. The demographic characteristics and measured values of disease-related parameters (EASI, Eos, IgE and TARC) are shown in Table I. Pearson correlation analysis was performed to examine the relationships between these parameters and each itch measure (Table II; Fig. S1). No significant correlations were found between spontaneous itch or MA and EASI, blood Eos or serum IgE levels. Among the disease-related parameters, however, only serum TARC levels showed a significant moderate correlation with MA scores at bending forces of 5.8 mN, 9.8 mN and 13.7 mN, while no significant correlations were found for spontaneous itch scores or for MA at 19.6 mN (r=0.362, p=0.082). These findings suggest that TARC was the disease-related parameter most consistently associated with MA in STEP 2. Scatterplots for each of the data in Table II are shown in Fig. S1.
Table II. Correlation between itch NRS scores and disease-related parameters in STEP 2 AD patients
| EASI | Eos | IgE | TARC | ||||||
|---|---|---|---|---|---|---|---|---|---|
| r | p-value | r | p-value | r | p-value | r | p-value | ||
| NRS | Spontaneous itch | -0.145 | 0.521 | 0.255 | 0.230 | 0.143 | 0.506 | 0.342 | 0.102 |
| 5.8 mN | -0.006 | 0.977 | 0.353 | 0.090 | 0.238 | 0.264 | 0.446 | 0.029* | |
| 9.8 mN | -0.012 | 0.959 | 0.342 | 0.101 | 0.187 | 0.381 | 0.440 | 0.031* | |
| 13.7 mN | -0.063 | 0.781 | 0.362 | 0.083 | 0.151 | 0.483 | 0.454 | 0.026* | |
| 19.6 mN | -0.147 | 0.514 | 0.316 | 0.132 | 0.153 | 0.475 | 0.362 | 0.082 | |
|
Correlation coefficients (r) and p-values are shown for relationships between itch NRS scores (spontaneous itch and MA) and disease-related parameters, including EASI, Eos, serum IgE and TARC levels, in AD patients. Correlation coefficients were calculated using Pearson’s correlation test. *p<0.05. AD:atopic dermatitis; EASI:Eczema Area and Severity Index; Eos:eosinophil count; IgE:immunoglobulin E; MA:mechanical alloknesis; NRS:numeric rating scale; TARC:thymus and activation-regulated chemokine. |
|||||||||
Time-dependent effects of dupilumab on mechanical alloknesis scores and spontaneous itch
In STEP 3, longitudinal changes were evaluated in 10 AD patients who completed follow-up during dupilumab treatment (Table I). Both spontaneous itch and MA scores showed a clear decreasing trend during the early phase of treatment, from baseline to the 5th administration (Fig. 3a–e). The reduction was statistically significant for spontaneous itch and MA at all filament forces (5.8–19.6 mN, Tables S8–S12). Additional analysis showed a significant negative correlation between dose number and itch scores up to the 5th administration, but not thereafter, suggesting that symptom improvement plateaued after approximately 5 doses (Table S13; see also Fig. S2).
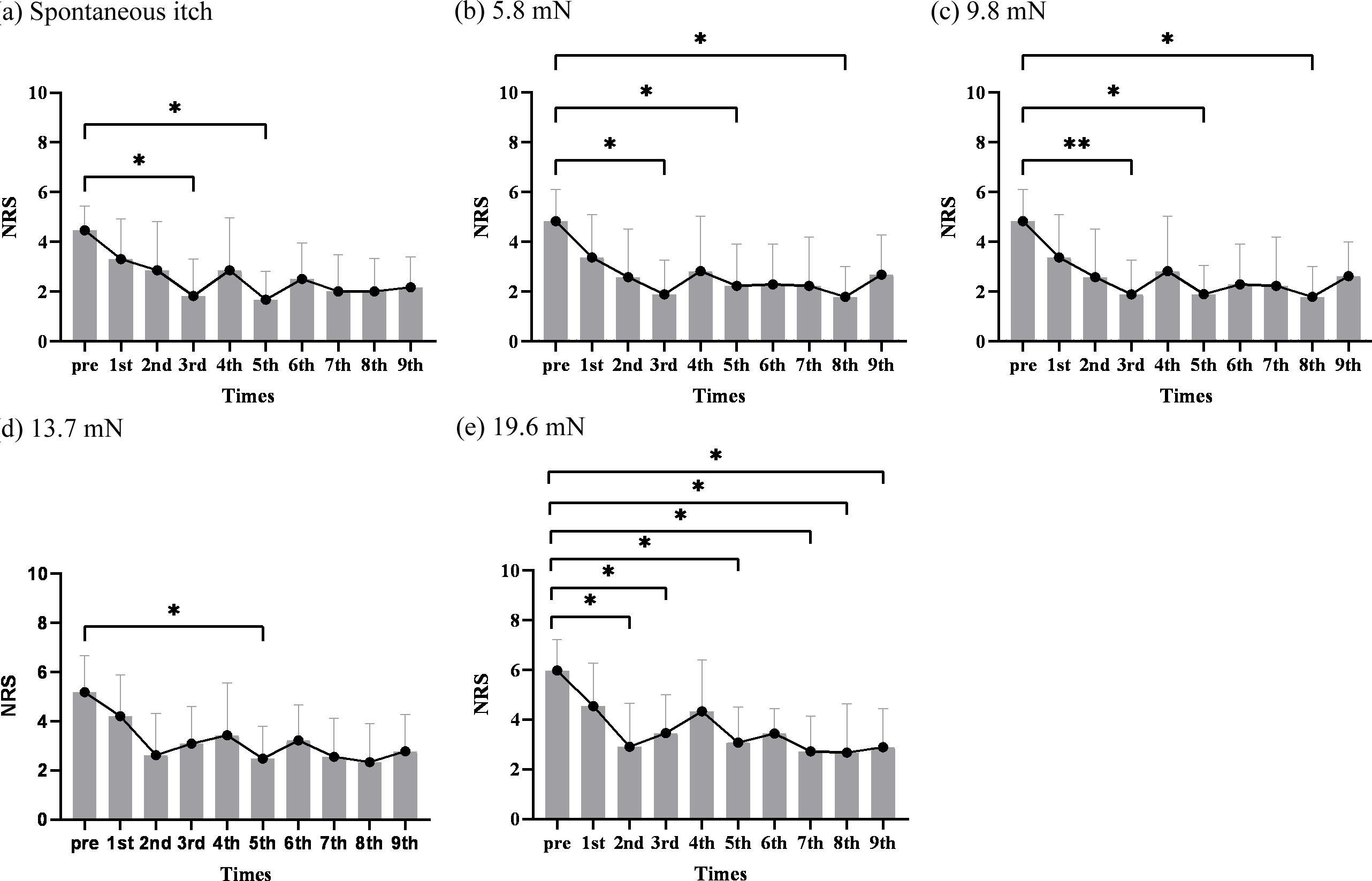
Fig. 3. Time-dependent changes in spontaneous itch and mechanical alloknesis (MA) scores in atopic dermatitis (AD) patients treated with dupilumab in STEP 3. (a–e) Itch numeric rating scale (NRS) scores for (A) spontaneous itch and MA at bending forces of (B) 5.8, (C) 9.8, (D) 13.7 and (E) 19.6 mN were evaluated from pre-treatment (pre, baseline) to the 9th dupilumab administration at each consecutive visit in AD patients. Statistical analyses were performed using one-way ANOVA followed by Dunnett’s multiple-comparison test to examine time-dependent differences in NRS scores across visits (from pre to 9th dose). *p<0.05, **p<0.01.
Correlation between disease-related parameters and itch scores after continuous dupilumab administration in STEP 3
At the visit for the 9th administration of dupilumab, blood samples were collected and Eos, IgE and TARC levels were measured in the 10 patients in STEP 3. Serum IgE and TARC levels at the 9th administration (Post) showed a significant decrease from baseline levels (Pre) (Fig. S3b, c, Tables S15 and S16). Eos also showed a decreasing trend (Fig. 3a, Table S14). At the 9th dupilumab administration, neither Eos nor IgE levels showed significant correlations with spontaneous itch or MA, whereas TARC levels displayed significant positive correlations with MA scores at 5.8 mN, 9.8 mN and 13.7 mN. No significant correlations were observed for spontaneous itch scores or MA at 19.6 mN. TARC remained the parameter most consistently associated with MA (Table III; see also Fig. S4).
Table III. Correlation between itch NRS scores and disease-related parameters (Eos, IgE, TARC) at the 9th dupilumab administration in STEP 3 AD patients
| Eos | IgE | TARC | |||||
|---|---|---|---|---|---|---|---|
| r | p-value | r | p-value | r | p-value | ||
| NRS | Spontaneous itch | -0.203 | 0.574 | 0.299 | 0.401 | 0.412 | 0.237 |
| 5.8 mN | -0.017 | 0.962 | 0.060 | 0.869 | 0.665 | 0.036* | |
| 9.8 mN | 0.289 | 0.418 | 0.129 | 0.722 | 0.836 | 0.003** | |
| 13.7 mN | 0.188 | 0.603 | 0.116 | 0.750 | 0.667 | 0.035* | |
| 19.6 mN | 0.237 | 0.509 | 0.105 | 0.774 | 0.583 | 0.077 | |
|
Correlation coefficients (r) and p-values are shown for relationships between itch NRS scores (spontaneous itch and MA) and disease-related parameters (Eos, IgE, and TARC) after 9 or more dupilumab doses. Correlation coefficients were calculated using Pearson correlation test. *p<0.05, **p<0.01. AD:atopic dermatitis; Eos:eosinophil count; IgE:immunoglobulin E; MA:mechanical alloknesis; NRS:numeric rating scale; TARC:thymus and activation-regulated chemokine. |
|||||||
DISCUSSION
In the present study, we evaluated MA in AD using cross-sectional and prospective cohort analyses. The principal findings were as follows: (i) MA was markedly enhanced in lesional AD skin compared with healthy control skin and non-lesional AD skin; (ii) skin dryness parameters were not significantly correlated with spontaneous itch or MA; (iii) among disease-related parameters, only serum TARC showed significant positive correlations with MA at 5.8–13.7 mN, whereas no significant correlation was observed with spontaneous itch; and (iv) dupilumab reduced spontaneous itch and MA, especially up to the 5th administration, but TARC remained correlated with MA after treatment. The association between TARC and MA suggests that TARC may contribute to MA in AD through mechanisms beyond systemic Th2 immune activation, potentially including the promotion of neuronal sensitization.
Whereas spontaneous itch is considered ongoing itch present at baseline, MA is defined as itch evoked by normally innocuous mechanical stimuli, indicating that the two are conceptually distinct. However, in areas where itch is nearly constant, such as the lesional skin of AD patients in the present study, complete separation of the two may be challenging. Nevertheless, we evaluated them separately using questions designed to distinguish them as clearly as possible. Moreover, serum TARC was associated with MA but not with spontaneous itch, both at baseline and after dupilumab treatment, supporting the view that MA in the present study was not merely a reflection of baseline spontaneous itch. This interpretation is also consistent with previous reports suggesting that mechanically evoked itch and ongoing spontaneous itch are mediated, at least in part, by distinct neural mechanisms (10, 15, 16).
The finding that MA was highest in lesional AD skin is consistent with previous clinical reports showing enhanced mechanically evoked itch in AD (4), particularly in lesional areas. In contrast to that report (4), we did not detect a significant difference between healthy skin and non-lesional AD skin. One possible explanation is the difference in demographic background between our cohort and previous studies, as our participants were older overall and the healthy control group was older than the AD group. Since ageing has been reported to increase mechanical itch sensitivity in animal studies (15, 17), age-related effects may have increased baseline mechanical itch sensitivity in healthy controls.
Nonetheless, within-group comparisons still showed that healthy skin and non-lesional AD skin exhibited a force-dependent increase in MA, similar to a previous report (18), whereas lesional AD skin did not. This plateau-like pattern in lesional skin may reflect a ceiling effect caused by peripheral and/or central sensitization (19).
With respect to skin barrier parameters, lesional AD skin showed higher TEWL than non-lesional skin, and SC hydration was lower in lesional AD skin than in non-lesional skin and healthy skin, supporting impaired barrier function in AD, consistent with previous reports (20, 21, 22). However, neither TEWL nor SC hydration was significantly correlated with spontaneous itch or MA. Although skin dryness parameters are influenced by environmental conditions and interindividual variability, which may have attenuated detectable associations, these findings suggest that barrier dysfunction alone does not fully explain itch severity.
In STEP 2, we analysed correlations between disease-related parameters and itch scores in AD patients. EASI, Eos, serum IgE, and TARC are established indices of AD severity and disease activity (2, 23). Among these parameters, only serum TARC was correlated with MA at 5.8, 9.8, and 13.7 mN, but not with spontaneous itch or MA at 19.6 mN.
In STEP 3, we prospectively evaluated AD patients treated with dupilumab. Both spontaneous itch and MA were reduced by the 5th administration, consistent with a previous report showing early improvement in touch-evoked itch after dupilumab treatment (24). At the 9th administration, serum IgE and TARC had decreased and Eos showed a decreasing trend, supporting the anti-inflammatory effect of dupilumab. Further improvement after the 5th administration was limited, suggesting that the antipruritic effect of dupilumab largely plateaued thereafter.
After 9 doses, the correlation pattern remained similar to baseline: TARC was again associated only with MA at 5.8, 9.8, and 13.7 mN, and these correlations were numerically stronger despite the small sample size. This differs from previous studies, including our own, in which spontaneous itch correlated with Eos, serum IgE or TARC (23, 25, 26). One possible explanation is differences in disease severity and population heterogeneity, as the present cohort included a broader range of AD severity than our previous dupilumab-eligible cohort (23).
These findings suggest that the role of TARC may vary with the inflammatory milieu. TARC is induced by Th2 cytokines and promotes Th2 inflammation (27, 28, 29, 30), but may also contribute to sensory hypersensitivity through peripheral neurons and CCR4-related pathways (31, 32, 33). In less inflammatory settings, this neural-sensitization component may become more apparent, potentially explaining why TARC was more closely associated with MA than with spontaneous itch.
Conversely, in milder AD, the inflammatory contribution of TARC may be limited while its role in neuronal hypersensitivity may become more evident, making its association with MA stronger than with spontaneous itch. The persistence of TARC–MA correlations after dupilumab treatment suggests a partly Th2-independent pathway. Because Th2 cytokines enhance mechanical alloknesis via neuronal sensitization (6, 12, 13), baseline MA was also likely influenced by Th2 cytokine activity, and its blockade by dupilumab may explain the stronger post-treatment TARC–MA correlation.
This interpretation is consistent with our previous experimental finding that weaker pruritogenic input may induce MA alone, whereas stronger input can evoke both MA and spontaneous itch, suggesting a continuum of peripheral neuronal sensitization (34).
Finally, the absence of correlation at 19.6 mN may reflect recruitment of different peripheral sensory neuron populations by stronger mechanical stimuli, including high-threshold mechanoreceptors, resulting in a more TARC-independent response (35).
Limitations of this study include the modest sample size, demographic imbalance, possible interference of spontaneous itch with MA assessment in AD lesions, variability in TEWL and SC hydration, and the observational design, which precludes causal inference between TARC and MA. Although serum TARC levels have been reported to correlate with local TARC levels and disease activity in AD (2, 23, 26, 36), demonstrating the role of TARC in MA in AD requires multifaceted experiments, including analysis of local expression levels of TARC and CCR4 in human skin, as well as animal behavioural experiments.
In conclusion, serum TARC was selectively associated with MA but not spontaneous itch, both before and after dupilumab treatment, suggesting a contribution of TARC to mechanically evoked itch that is at least partly independent of Th2-mediated inflammation. TARC may therefore reflect not only systemic inflammation but also peripheral neuronal sensitization in AD. Clinically, assessment of MA may complement conventional disease severity indices, particularly for evaluating residual itch sensitivity during biologic therapy. Although validation in larger multicentre cohorts is needed, these findings support incorporating MA and TARC assessment into a more comprehensive evaluation of itch in AD.
ACKNOWLEDGEMENTS
We thank the participants, the staff of the Department of Dermatology, Juntendo University Urayasu Hospital, and David Price for proofreading. This work was supported by JSPS KAKENHI (20H03568, 25K22714, 20K08680, 23K18407, 24K02265, 22H02956, 24K22237). The funders had no role in the study.
REFERENCES
- Weidinger S, Novak N. Atopic dermatitis. Lancet 2016; 387: 1109–1122. https://doi.org/10.1016/S0140-6736(15)00149-X
- Saeki H, Ohya Y, Arakawa H, Ichiyama S, Katsunuma T, Katoh N, et al. Executive summary: Japanese guidelines for atopic dermatitis (ADGL) 2024. Allergol Int 2025; 74: 210–221. https://doi.org/10.1016/j.alit.2025.01.003
- Murota H, Koike Y, Ishii K, Calimlim BM, Ludwikowska M, Toumi M, et al. Evaluating the burden of pruritus due to atopic dermatitis in Japan by patient-reported outcomes. J Med Econ 2021; 24: 1280–1289. https://doi.org/10.1080/13696998.2021.2002559
- Andersen HH, Elberling J, Sølvsten H, Yosipovitch G, Arendt-Nielsen L. Nonhistaminergic and mechanical itch sensitization in atopic dermatitis. Pain 2017; 158: 1780–1791. https://doi.org/10.1097/j.pain.0000000000000980
- Tominaga M, Takamori K. Peripheral itch sensitization in atopic dermatitis. Allergol Int 2022; 71: 265–277. https://doi.org/10.1016/j.alit.2022.04.003
- Toyosawa Y, Komiya E, Kaneko T, Suga Y, Tominaga M, Takamori K. Type 2 cytokine-JAK1 signaling is involved in the development of dry skin-induced mechanical alloknesis. J Dermatol Sci 2025; 117: 52–60. https://doi.org/10.1016/j.jdermsci.2024.10.002
- Akiyama T, Carstens MI, Ikoma A, Cevikbas F, Steinhoff M, Carstens E. Mouse model of touch-evoked itch (alloknesis). J Invest Dermatol 2012; 132: 1886–1891. https://doi.org/10.1038/jid.2012.52
- Hill RZ, Loud MC, Dubin AE, Peet B, Patapoutian A. PIEZO1 transduces mechanical itch in mice. Nature New Biol 2022; 607: 104–110. https://doi.org/10.1038/s41586-022-04860-5
- Acton D, Ren X, Di Costanzo S, Dalet A, Bourane S, Bertocchi I, et al. Spinal neuropeptide Y1 receptor-expressing neurons form an essential excitatory pathway for mechanical itch. Cell Rep 2019; 28: 625–639. https://doi.org/10.1016/j.celrep.2019.06.033
- Pan H, Fatima M, Li A, Lee H, Cai W, Horwitz L, et al. Identification of a spinal circuit for mechanical and persistent spontaneous itch. Neuron 2019; 103: 1135–1149. https://doi.org/10.1016/j.neuron.2019.06.016
- Bourane S, Duan B, Koch SC, Dalet A, Britz O, Garcia-Campmany L, et al. Gate control of mechanical itch by a subpopulation of spinal cord interneurons. Science 2015; 350: 550–554. https://doi.org/10.1126/science.aac8653
- Oetjen LK, Mack MR, Feng J, Whelan TM, Niu H, Guo CJ, et al. Sensory neurons co-opt classical immune signaling pathways to mediate chronic itch. Cell 2017; 171: 217–228. https://doi.org/10.1016/j.cell.2017.08.006
- Ichimasu N, Chen Y, Kobayashi K, Suzuki S, Chikazawa S, Shimura S, et al. Possible involvement of type 2 cytokines in alloknesis in mouse models of menopause and dry skin. Exp Dermatol 2021; 30: 1745–1753. https://doi.org/10.1111/exd.14422
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg 2014; 12: 1495–1499. https://doi.org/10.1016/j.ijsu.2014.07.013
- Feng J, Luo J, Yang P, Du J, Kim BS, Hu H. Piezo2 channel-Merkel cell signaling modulates the conversion of touch to itch. Science 2018; 360: 530–533. https://doi.org/10.1126/science.aar5703
- Sakai K, Akiyama T. New insights into the mechanisms behind mechanical itch. Exp Dermatol 2020; 29: 680–686. https://doi.org/10.1111/exd.14143
- Kojima G, Komiya E, Honda K, Kaneko T, Suga Y, Tominaga M, et al. Model of chronic itch in aged mice: beneficial effects of drugs affecting descending modulatory systems. Acta Derm Venereol 2024; 104: adv39950. https://doi.org/10.2340/actadv.v104.39950
- Andersen HH, Elberling J, Lo Vecchio S, Arendt-Nielsen L. Topography of itch: evidence of distinct coding for pruriception in the trigeminal nerve. Itch (Phila) 2017; 2: e2. https://doi.org/10.1097/itx.0000000000000002
- Talagas M, Le Garrec R, Le Bon-Jégo M, Le Gall-Ianotto C, Schreiber L, Brenaut E, et al. Alloknesis: a severe form of itch. Br J Dermatol 2026; 194: 18–24. https://doi.org/10.1093/bjd/ljaf337
- Lee CH, Chuang HY, Shih CC, Jong SB, Chang CH, Yu HS. Transepidermal water loss, serum IgE and beta-endorphin as important and independent biological markers for development of itch intensity in atopic dermatitis. Br J Dermatol 2006; 154: 1100–1107. https://doi.org/10.1111/j.1365-2133.2006.07191.x
- Leung DYM, Berdyshev E, Goleva E. Cutaneous barrier dysfunction in allergic diseases. J Allergy Clin Immunol 2020; 145: 1485–1497. https://doi.org/10.1016/j.jaci.2020.02.021
- Knor T, Meholjić-Fetahović A, Mehmedagić A. Stratum corneum hydration and skin surface pH in patients with atopic dermatitis. Acta Dermatovenerol Croat 2011; 19: 242–247.
- Kishi R, Toyama S, Tominaga M, Kamata Y, Komiya E, Kaneko T, et al. Effects of dupilumab on itch-related events in atopic dermatitis: implications for assessing treatment efficacy in clinical practice. Cells 2023; 12: 12. https://doi.org/10.3390/cells12020239
- Hashimoto T, Okuno S, Okuzawa M, Satoh T. Dupilumab improves both histaminergic and touch-evoked itch sensitization (hyperknesis) in atopic dermatitis: a pilot study. J Eur Acad Dermatol Venereol 2022; 36: e911–e912. https://doi.org/10.1111/jdv.18356
- Kimura T, Sugaya M, Suga H, Morimura S, Miyamoto A, Kai H, et al. Variations in serum TARC and I-TAC levels reflect minor changes in disease activity and pruritus in atopic dermatitis. Acta Derm Venereol 2014; 94: 331–332. https://doi.org/10.2340/00015555-1709
- van der Rijst LP, Knol EF, Zuithoff NPA, den Hartog Jager CF, van Wijk F, de Bruin-Weller MS, et al. Complementary analysis of local and systemic effects of dupilumab in paediatric AD using tape strips and serum. Clin Exp Allergy 2025; 55: 552–563. https://doi.org/10.1111/cea.70082
- Wirnsberger G, Hebenstreit D, Posselt G, Horejs-Hoeck J, Duschl A. IL-4 induces expression of TARC/CCL17 via two STAT6 binding sites. Eur J Immunol 2006; 36: 1882–1891. https://doi.org/10.1002/eji.200635972
- Saeki H, Tamaki K. Thymus and activation regulated chemokine (TARC)/CCL17 and skin diseases. J Dermatol Sci 2006; 43: 75–84. https://doi.org/10.1016/j.jdermsci.2006.06.002
- Lupancu TJ, Eivazitork M, Hamilton JA, Achuthan AA, Lee KMC. CCL17/TARC in autoimmunity and inflammation-not just a T-cell chemokine. Immunol Cell Biol 2023; 101: 600–609. https://doi.org/10.1111/imcb.12644
- Vestergaard C, Deleuran M, Gesser B, Larsen CG. Thymus- and activation-regulated chemokine (TARC/CCL17) induces a Th2-dominated inflammatory reaction on intradermal injection in mice. Exp Dermatol 2004; 13: 265–271. https://doi.org/10.1111/j.0906-6705.2004.00149.x
- Raymondi Silva J, Iftinca M, Fernandes Gomes FI, Segal JP, Smith OMA, Bannerman CA, et al. Skin-resident dendritic cells mediate postoperative pain via CCR4 on sensory neurons. Proc Natl Acad Sci USA 2022; 119: 119. https://doi.org/10.1073/pnas.2118238119
- Zheng X, Nakamura K, Furukawa H, Nishibu A, Takahashi M, Tojo M, et al. Demonstration of TARC and CCR4 mRNA expression and distribution using in situ RT-PCR in the lesional skin of atopic dermatitis. J Dermatol 2003; 30: 26–32. https://doi.org/10.1111/j.1346-8138.2003.tb00329.x
- Steinhoff M, Steinhoff A, Homey B, Luger TA, Schneider SW. Role of vasculature in atopic dermatitis. J Allergy Clin Immunol 2006; 118: 190–197. https://doi.org/10.1016/j.jaci.2006.04.025
- Komiya E, Tominaga M, Hatano R, Kamikubo Y, Toyama S, Sakairi H, et al. Peripheral endomorphins drive mechanical alloknesis under the enzymatic control of CD26/DPPIV. J Allergy Clin Immunol 2022; 149: 1085–1096. https://doi.org/10.1016/j.jaci.2021.08.003
- Abraira VE, Ginty DD. The sensory neurons of touch. Neuron 2013; 79: 618–639. https://doi.org/10.1016/j.neuron.2013.07.051
- Morita E, Takahashi H, Niihara H, Dekio I, Sumikawa Y, Murakami Y, et al. Stratum corneum TARC level is a new indicator of lesional skin inflammation in atopic dermatitis. Allergy 2010; 65: 1166–1172. https://doi.org/10.1111/j.1398-9995.2010.02361.x