QUIZ SECTION
Painful Destructive Plaques of the Face and Scalp: A Quiz
Rundong ZHANG1†![]() , Zequn QIU1†, Hongyin CHEN2 and Hao CHEN3*
, Zequn QIU1†, Hongyin CHEN2 and Hao CHEN3*
1Hospital for Skin Diseases, Institute of Dermatology, Chinese Academy of Medical Sciences & Peking Union Medical College, Nanjing, China, 2Department of Physical Therapy, Hospital for Skin Diseases, Institute of Dermatology, Chinese Academy of Medical Sciences & Peking Union Medical College, Nanjing, China, and 3Department of Pathology, Hospital for Skin Diseases, Institute of Dermatology, Chinese Academy of Medical Sciences & Peking Union Medical College, Nanjing, China. *Email: ch76ch@163.com
Citation: Acta Derm Venereol 2026; 106: adv-2026-0718. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0718.
Copyright: 2026 ©Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Accepted after revision:
Published: Jun 15, 2026.
Competing interests and funding:
A man in his 70s presented with a 1 month history of rapidly progressive painful lesions involving the nose, left periorbital region, vertex scalp and bilateral temporal scalp. The eruption began as a cyst-like lesion on the nasal tip and alae and evolved into destructive vegetative plaques with nasal deformity (Fig. 1). A prominent left periocular lesion showed marked swelling, pain and purulent discharge. He had persistent fever and had received multiple antibacterial and antifungal treatments without improvement. The lesions worsened after crust removal. Laboratory tests showed pancytopenia, elevated C-reactive protein and an erythrocyte sedimentation rate of 131 mm/h. Bone marrow biopsy, flow cytometry and genetic studies showed reactive hyperplasia without definitive evidence of myelodysplastic syndrome or haematological malignancy. Targeted UBA1 sequencing was negative. Skin biopsy showed marked pseudoepitheliomatous hyperplasia and dense neutrophilic inflammation involving the epidermis and dermis (Fig. 2). Periodic acid-Schiff, acid-fast and silver stains, tissue cultures and metagenomic next-generation sequencing were negative.

Fig. 1. Clinical findings at presentation. Destructive vegetative plaques involving the nose with nasal deformity, accompanied by left periocular swelling and bilateral temporal and vertex scalp lesions.
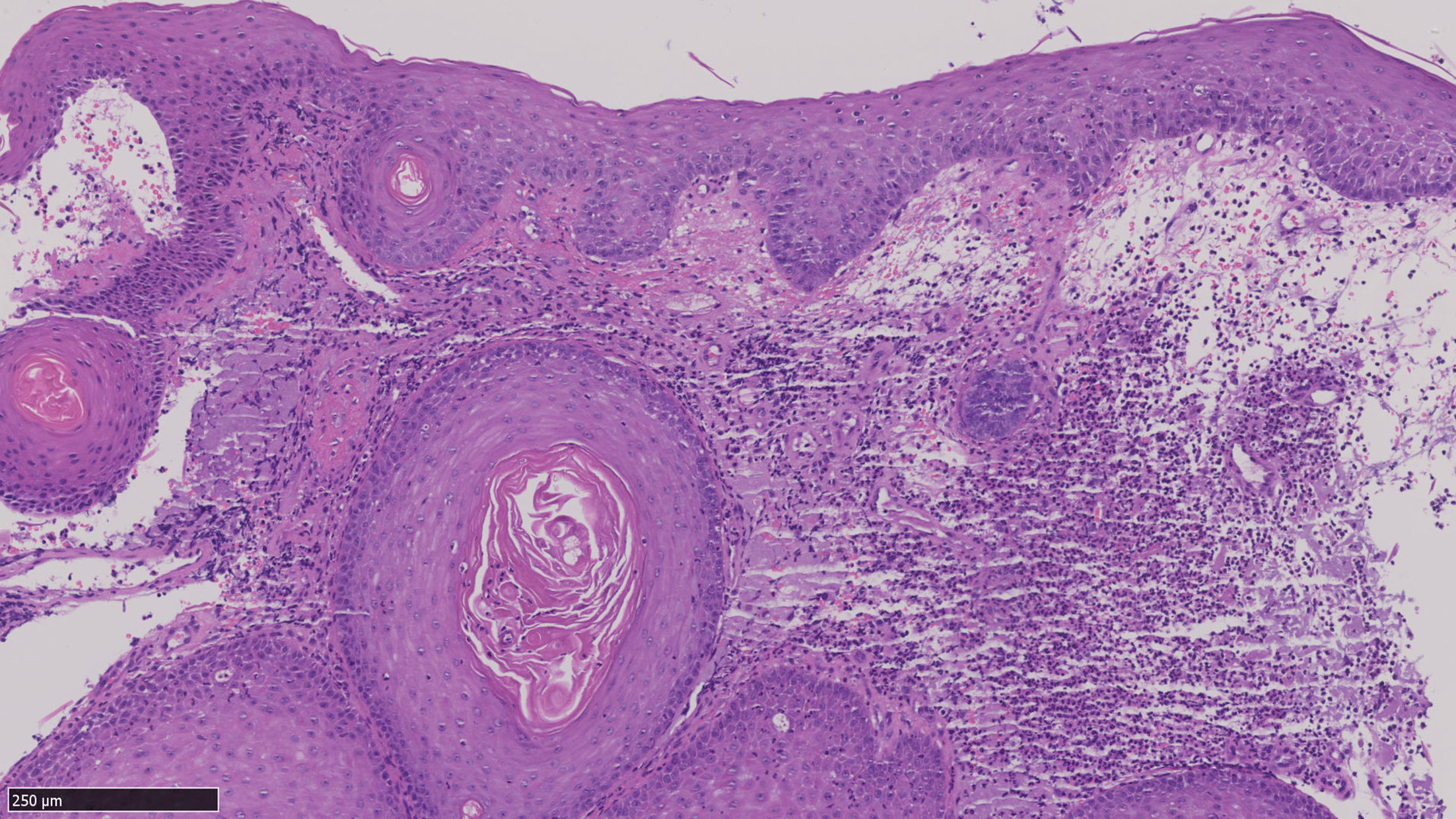
Fig. 2. Histopathological findings. Skin biopsy showing marked pseudoepitheliomatous hyperplasia with reactive squamous downgrowth and dense neutrophilic inflammation involving the epidermis and dermis (haematoxylin-eosin, original magnification ×20).
What is your diagnosis?
1: Pyoderma gangrenosum.
2: Granulomatosis with polyangiitis.
3: Deep fungal infection.
4: Cutaneous squamous cell carcinoma.
See next page for answer.
ANSWERS TO QUIZ
Painful Destructive Plaques of the Face and Scalp: A Commentary
Diagnosis: Pyoderma gangrenosum.
This case is most consistent with pyoderma gangrenosum (PG) in an atypical proliferative or vegetative spectrum. The diagnosis was supported by rapid painful progression, paradoxical worsening after manipulation suggesting pathergy, dense neutrophilic inflammation on biopsy, repeated negative microbiological studies, lack of response to anti-infective therapy and prompt improvement after systemic glucocorticoids plus cyclosporine. The subsequent development of cribriform scarring and parallel improvement in systemic inflammation further supported PG. Although Delphi criteria were developed for classic ulcerative PG, this patient fulfilled several supportive features, including exclusion of infection, pathergy, neutrophilic histopathology, cribriform scarring and clinical improvement within 1 month of immunosuppression (1).
The main alternative diagnoses were granulomatosis with polyangiitis, deep fungal infection and cutaneous squamous cell carcinoma. Granulomatosis with polyangiitis was considered because of destructive nasal involvement, periocular inflammation, fever and systemic inflammation. However, biopsy did not show granulomatous inflammation or vasculitis, and the overall pattern was more consistent with a neutrophilic dermatosis. Deep fungal infection was also plausible because the lesions were infiltrative and purulent and involved the face, where infectious mimics are common (2, 3). However, special stains, cultures and metagenomic next-generation sequencing were negative, prior anti-infective treatment was ineffective and the lesions improved rapidly after immunosuppression. Cutaneous squamous cell carcinoma was less likely because histopathology lacked significant cytological atypia, atypical mitotic activity, infiltrative irregular nests and keratin pearl formation; the pseudoepitheliomatous hyperplasia was interpreted as a reactive epithelial change within a destructive inflammatory process.
This case highlights the importance of recognizing atypical facial and scalp PG before harmful procedures are performed. Head and neck PG is uncommon and frequently misdiagnosed, with infection, vasculitis and malignancy among the reported initial impressions (2, 3). Facial disease may present with non-classical inflammatory, vegetative or superficial granulomatous features, and vegetative lesions may show marked pseudoepitheliomatous hyperplasia (4, 5). Our patient fits this published spectrum but is notable for simultaneous destructive involvement of the nose, periocular region and scalp, a combination that may easily direct attention toward infection or vasculitis rather than PG. Periocular involvement is especially important because diagnostic delay may expose patients to repeated drainage, debridement or reconstructive procedures that worsen disease through pathergy and may threaten adjacent ocular structures (6).
The case also illustrates how clinicopathological correlation should be weighted in proliferative PG. Histology in PG is supportive rather than pathognomonic, and findings vary with lesion age and biopsy site. In vegetative or superficial granulomatous forms, pseudoepitheliomatous hyperplasia and exuberant inflammation may dominate the biopsy and obscure the underlying neutrophilic dermatosis. Therefore, a negative infectious work-up, disproportionate pain, rapid multifocal progression, manipulation-induced worsening and response to immunosuppression are essential diagnostic clues. These features are particularly useful in facial lesions, where both infection and neoplasia are frequent initial concerns.
The patient’s age, fever and pancytopenia also made VEXAS syndrome an important modern differential diagnosis. VEXAS is an adult-onset autoinflammatory disorder caused by somatic UBA1 mutations and may present with neutrophilic dermatoses, systemic inflammation and haematological abnormalities (7, 8). Historical cases of PG associated with myelodysplastic syndrome or chronic myelomonocytic leukaemia may overlap with this entity (9). In the present case, negative UBA1 sequencing argued against VEXAS, while continued haematological follow-up remained appropriate because PG can also occur in association with haematological disorders (10).
Systemic corticosteroids and cyclosporine remain established treatments for moderate-to-severe PG. In this patient, rapid defervescence and regression of skin lesions after these agents provided both therapeutic benefit and diagnostic support. The key teaching point is that painful, rapidly progressive, culture-negative destructive plaques of the face or scalp, especially when worsened by manipulation and accompanied by neutrophilic inflammation, should raise suspicion for PG even when infection initially appears more likely. Early recognition can prevent unnecessary procedures, reduce pathergy-related tissue loss and facilitate timely immunosuppressive treatment.
REFERENCES
- Maverakis E, Ma C, Shinkai K, Fiorentino D, Callen JP, Wollina U, et al. Diagnostic criteria of ulcerative pyoderma gangrenosum: a Delphi consensus of international experts. JAMA Dermatol 2018; 154: 461–466. https://doi.org/10.1001/jamadermatol.2017.5980
- Reese AM, Gupta AS, Latour E, Loyo M, Kaffenberger B, Creadore A, et al. Clinical characteristics and misdiagnosis of pyoderma gangrenosum of the head and neck: a retrospective study. J Am Acad Dermatol 2022; 87: 1130–1133. https://doi.org/10.1016/j.jaad.2022.02.008
- Kaur M, Anthony MR, Yamakoshi C, Schildmeyer A, Mallela T, Diaz MJ, et al. Clinical characteristics, treatments, and outcomes of pyoderma gangrenosum of the face: a systematic review. Int Wound J 2025; 22: e70334. https://doi.org/10.1111/iwj.70334
- Shavit E, Cecchini M, Limacher JJ, Walsh S, Wentworth A, Davis MDP, et al. Superficial granulomatous pyoderma gangrenosum involving the face: a case series of five patients and a review of the literature. J Cutan Med Surg 2021; 25: 371–376. https://doi.org/10.1177/1203475420988864
- Hoang M, Maymone MBC, Telang GH, Seo SJ, Robinson-Bostom L. Vegetative pyoderma gangrenosum mimicking squamous cell carcinoma: a poorly recognized diagnostic challenge. Am J Dermatopathol 2025; 47: e47–e49. https://doi.org/10.1097/DAD.0000000000002919
- Gupta AS, Ortega-Loayza AG. Ocular pyoderma gangrenosum: a systematic review. J Am Acad Dermatol 2017; 76: 512–518. https://doi.org/10.1016/j.jaad.2016.08.049
- Beck DB, Ferrada MA, Sikora KA, Ombrello AK, Collins JC, Pei W, et al. Somatic mutations in UBA1 and severe adult-onset autoinflammatory disease. N Engl J Med 2020; 383: 2628–2638. https://doi.org/10.1056/NEJMoa2026834
- Tan IJ, Ferrada MA, Ahmad S, Fike A, Quinn KA, Groarke EM, et al. Skin manifestations of VEXAS syndrome and associated genotypes. JAMA Dermatol 2024; 160: 822–829. https://doi.org/10.1001/jamadermatol.2024.1657
- Croitoru DO, Huang RS, McMullen EP, Maazi M, Piguet V. Investigating historic cases of pyoderma gangrenosum in myelodysplastic syndrome and chronic myelomonocytic leukemia for possible VEXAS syndrome: a systematic review. J Am Acad Dermatol 2024; 91: 712–714. https://doi.org/10.1016/j.jaad.2024.05.086
- Montagnon CM, Fracica EA, Patel AA, Camilleri MJ, Murad MH, Dingli D, et al. Pyoderma gangrenosum in hematologic malignancies: a systematic review. J Am Acad Dermatol 2020; 82: 1346–1359. https://doi.org/10.1016/j.jaad.2019.09.032