ORIGINAL REPORT
Clinical and Pathological Predictors of Unfavourable Outcomes in Thin and In Situ Melanomas: A Retrospective Cohort Study from Taiwan
Guan-Kai LAI1![]() , Yi-Hua LIAO1
, Yi-Hua LIAO1![]() , Ming-Hsien LIN2
, Ming-Hsien LIN2![]() , Chia-Yu CHU1
, Chia-Yu CHU1![]() and Yi-Shuan SHEEN1*
and Yi-Shuan SHEEN1*![]()
1Department of Dermatology, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan, and 2Department of Surgery, National Taiwan University Hospital Hsin-Chu Branch, Hsin-chu, Taiwan
Corr: Yi-Shuan Sheen, Department of Dermatology, National Taiwan University Hospital 7 Chung-Shan S. Rd., Taipei, 100, Taiwan. *Email: sheenyishuan@gmail.com
Key words: age; cutaneous malignant melanoma; melanoma; prognosis; risk factors; survival analysis.
Citation: Acta Derm Venereol 2026; 106: adv-2026-0460. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0460.
Copyright: 2026 ©Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 2, 2026. Accepted after revision: May 27, 2026.
Published: Jun 15, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
This work was supported by grants from the National Science and Technology Council [NSTC 112-2314-B-002-075-MY3] and National Taiwan University Hospital [NTUH-112S0171, NTUH-115S0026]. The funders had no role in study design, data collection, data analysis, manuscript preparation, or publication decisions.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
This study was approved by the Research Ethics Committee of National Taiwan University Hospital (NTUH-REC No. 202503155RINA) and adhered to the Declaration of Helsinki. Informed consent was waived by the committee due to the retrospective nature of the study.
Thin melanoma, defined as tumour thickness ≤1.0 mm, and melanoma in situ are increasingly diagnosed. However, acral-predominant Asian populations appear to experience higher rates of adverse outcomes than Western cohorts. This study aimed to identify prognostic factors among Taiwanese patients with early-stage melanoma. We reviewed 178 melanoma in situ/thin melanoma cases diagnosed from 1995 to 2025 at a tertiary centre and analysed overall survival, melanoma-specific survival, recurrence-free survival, and distant metastasis-free survival using Cox and Fine–Gray competing-risk models. During a mean follow-up of 81 months, adverse events were not uncommon, including recurrence (8.8%), distant metastasis (4.7%) and melanoma-specific mortality (5.1%). Age was the most consistent predictor across endpoints in both Cox and competing-risk analyses. A Breslow thickness ≥0.8 mm independently increased the risk of melanoma-specific mortality, whereas ulceration and mitotic activity were not significant predictors. In conclusion, melanoma in situ and thin melanoma in this acral-predominant Asian cohort are not uniformly low risk. Older patients or those with tumours approaching or exceeding 0.8 mm in thickness warrant closer, risk-adapted surveillance.
SIGNIFICANCE
Melanoma in situ and thin melanoma (1.0 mm or less) are often thought to be low risk. However, our study shows that some patients, especially those older than 60 years and those with Breslow thickness ≥0.8 mm lesions, can still face serious outcomes. By studying patients in Taiwan, where melanoma commonly appears on the feet and hands, we found that even early-stage disease is not always harmless. Our findings help doctors recognise who may need closer follow-up and raise public awareness supporting earlier care and potentially reducing preventable deaths.
The global incidence of melanoma continues to increase, largely due to increased detection of early-stage lesions – melanoma in situ (MIS) and thin melanoma (TM; Breslow thickness ≤1.0 mm) – through screening and awareness (1, 2, 3). Although melanoma has long been regarded as a malignancy of fair-skinned populations in Western countries, recent epidemiological reports from East Asia indicate a growing disease burden (4, 5, 6). Importantly, Asian patients often present with distinct clinicopathologic and molecular features, suggesting Western prognostic data may not apply to Asian populations (6, 7, 8).
In Western populations, early-stage melanoma is generally associated with excellent long-term outcomes, with 5 year melanoma-specific survival (MSS) rates approaching 97–99% for thin lesions (9, 10, 11). Nonetheless, a subset of patients with MIS or TM experience recurrence, distant metastasis or melanoma-specific death, and Breslow thickness ≥0.8 mm has emerged as a clinically relevant risk threshold (11, 12, 13, 14, 15, 16).
In Asian populations, however, prognostic patterns may differ (1). Acral lentiginous melanoma (ALM) accounts for a larger proportion of cases and is frequently diagnosed at a later stage, contributing to poorer outcomes (6, 17, 18). In addition, ALM displays distinct molecular features compared with Western cohorts predominantly composed of superficial spreading melanoma (SSM), raising concerns regarding the direct applicability of Western-derived prognostic models to acral-predominant Asian populations (6, 19, 20).
Despite increasing reports, evidence specifically addressing MIS and TM in Asian patients remains limited. Prior reports from Taiwan and Korea have suggested higher recurrence and mortality than would be expected based on Western data and have highlighted older age, acral location, and male sex as adverse prognostic factors in localized melanoma (21, 22, 23). Because non-melanoma-related death is relatively common in ageing Asian populations and may preclude observation of recurrence or metastasis, competing-risk methods are needed to obtain clinically realistic estimates of absolute risk (16, 24). Accordingly, the present study aimed to identify clinicopathological predictors of recurrence, distant metastasis and death in a Taiwanese cohort of early-stage melanoma. Using Cox proportional hazards models for overall survival (OS) and MSS, together with Fine–Gray competing-risk regression for recurrence and distant metastasis, we specifically examined whether age and Breslow thickness retain independent prognostic value in an acral-predominant population, and whether the commonly used 0.8 mm Breslow thickness threshold remains prognostically relevant in this setting.
MATERIALS AND METHODS
Study design and patient cohort
This retrospective study at National Taiwan University Hospital (NTUH) was approved by the institutional Research Ethics Committee (NTUH-REC No. 202503155RINA) adhering to the Declaration of Helsinki. We identified patients diagnosed with melanoma at NTUH between 1 January 1995 and 28 March 2025 using the electronic medical records. Of 638 records screened (Fig. S1), we excluded cases with Breslow thickness>1.0 mm or American Joint Committee on Cancer (AJCC) 8th edition stage>II (n=458), loss to follow-up (n=1) and unspecified histological subtype (n=1), leaving 178 early-stage (MIS and TM) patients.
We collected demographics, tumour features and follow-up information. Four outcomes were defined from the biopsy date: OS, time to death from any cause; MSS, time to melanoma-related death; distant metastasis–free survival (DMFS), time to first distant metastasis; and recurrence-free survival (RFS), time to first recurrence (local, regional nodal or distant). Causes of death and event dates were ascertained from electronic medical records and verified through linkage with the Taiwan National Death Registry.
Statistical analysis
Continuous variables were summarised as mean±standard deviation (SD), and categorical variables as frequencies and percentages; between-group comparisons used t test for continuous data and χ2 or Fisher exact test for categorical data, as appropriate. Survival analyses were performed using the Kaplan–Meier method to estimate OS, MSS, DMFS and RFS. Group differences were assessed with the log-rank test.
Univariable Cox regression identified factors associated with survival outcomes. Age at diagnosis was modelled primarily as a continuous variable (per year); analyses stratified at ≤60 vs >60 years were provided for clinical interpretability. Variables with p<0.10 in univariable analysis were subsequently entered into multivariable Cox models to determine independent predictors, and results were expressed as hazard ratios (HRs) with 95% confidence intervals (CIs). Because non-melanoma-related deaths were frequent, Fine–Gray competing-risk regression was used as the primary approach for MSS, DMFS and RFS (reporting subdistribution hazard ratios [SHRs]); Kaplan–Meier/Cox results for these endpoints are presented as complementary, descriptive analyses. All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA) and R version 4.3. Statistical significance was defined as 2-tailed p<0.05.
RESULTS
A total of 178 patients with early-stage melanoma were included (Fig. S1). Of these, 89 (50.0%) had MIS and 89 (50.0%) had TM (Table I). Age and sex distribution were comparable between groups. The mean follow-up duration was longer in TM than MIS (89.99±95.74 vs 72.48±76.98 months); however, the difference was not statistically significant.
Table I. Baseline clinicopathological characteristics of melanoma in situ and thin melanoma
| Characteristic | Melanoma in situ (n=89) | Thin melanoma (n=89) | p-value |
|---|---|---|---|
| Sex, n (%) | 0.548 | ||
| Female | 46 (51.7) | 50 (56.2) | |
| Male | 43 (48.3) | 39 (43.8) | |
| Age at diagnosis, years, mean (SD) | 60.12±14.46 | 59.47±15.57 | 0.773 |
| Tumour location, n (%) | <0.0001* | ||
| Trunk | 1 (1.1) | 15 (16.9) | |
| Head and neck | 2 (2.3) | 3 (3.4) | |
| Extremities | 8 (9.0) | 20 (22.5) | |
| Acral | 78 (87.6) | 51 (57.3) | |
| Histological subtype, n (%) | <0.0001* | ||
| ALM | 78 (87.6) | 51 (57.3) | |
| SSM | 7 (7.9) | 32 (36.0) | |
| NM | 1 (1.1) | 3 (3.4) | |
| LMM | 3 (3.4) | 3 (3.4) | |
| Breslow thickness, mm, mean (SD) | 0.67±0.26 | ||
| Ulceration, n (%) | |||
| Absent | 82 (92.1) | ||
| Present | 7 (7.9) | ||
| Mitotic rate, n (%) | 0.045* | ||
| <1/ mm² | 46 (86.8) | 42 (71.2) | |
| ≥1/ mm² | 7 (13.2) | 17 (28.8) | |
| Tumour-infiltrating lymphocytes, n (%) | <0.0001* | ||
| Absent | 44 (88.0) | 7 (11.7) | |
| Nonbrisk | 5 (10.0) | 47 (78.3) | |
| Brisk | 1 (2.0) | 6 (10.0) | |
| Tumour regression, n (%) | 0.046* | ||
| Absent | 45 (93.8) | 45 (80.4) | |
| Present | 3 (6.3) | 11 (19.6) | |
| Associated melanocytic lesion, n (%) | 0.021* | ||
| No | 48 (94.1) | 44 (78.6) | |
| Yes | 3 (5.9) | 12 (21.4) | |
| Surgical wait time, days, mean (SD) | 24.58±16.36 | 28.45±22.76 | 0.227 |
| Follow-up time, months, mean (SD) | 72.48±76.98 | 89.99±95.74 | 0.181 |
|
p-values were obtained using t-test (continuous) and χ2 or Fisher exact test (categorical). Denominators reflect available data for each variable. *Statistically significant. ALM: acral lentiginous melanoma; LMM: lentigo maligna melanoma; NM: nodular melanoma; SSM: superficial spreading melanoma. |
|||
Anatomic distribution and histologic subtype showed marked differences between groups. Acral lesions were more frequent in MIS than in TM (87.6% vs 57.3 %; p<0.0001), consistent with ALM being the predominant histologic subtype among MIS (87.6%). In TM, while the proportion of SSM (36.0%) was significantly higher than in MIS, ALM (57.3%) remained the most frequent histologic subtype. Ulceration was infrequent in TM (7/89, 7.9%) and a mitotic rate ≥1 /mm² was more common in TM than MIS (28.8% vs 13.2%, p=0.045). Tumour-infiltrating lymphocytes also differed significantly (p<0.0001): most MIS lesions had absent TILs (88.0%), whereas nonbrisk TILs predominated in TM (78.3%). Partial regression (19.6% vs 6.3%, p=0.046) and associated melanocytic lesions (21.4% vs 5.9%, p=0.021) were also more frequent in TM. Among TM cases, the mean Breslow thickness was 0.67±0.26 mm. Surgical wait time was shorter for MIS than TM (24.58±16.36 vs 28.45±22.76 days), but the difference was not statistically significant.
Among 171 patients with available recurrence data, 15 recurrences (8.77%) were identified, including 5 recurrences in MIS (5.68%) and 10 in TM (12.05%) (Table II). Among 172 patients with distant metastasis data, 8 distant metastases (4.65%) occurred: 1 (1.14%) in MIS and 7 (8.33%) in TM. Mortality data were available in 177 patients. Overall, 36 patients (20.34%) died, including 11 deaths in MIS (12.36%) and 25 in TM (28.41%). Among 175 patients with known causes of death, melanoma-specific deaths accounted for 9 cases (5.14%) – 2 in MIS (2.27%) and 7 in TM (8.05%) – whereas 27 deaths (15.43%) were unrelated to melanoma (10.23% in MIS vs 20.69% in TM). One patient was recorded as having melanoma-specific death according to the Taiwan National Death Registry despite no documented distant metastasis in the available clinical records, likely reflecting incomplete retrospective information regarding metastatic progression.
Table II. Clinical outcomes in melanoma in situ and thin melanoma
Overall survival showed a borderline difference between MIS and TM (log-rank p=0.0719), whereas MSS and RFS did not differ significantly (p=0.1301 and p=0.1847, respectively). In contrast, DMFS was significantly worse in TM (log-rank p=0.0470) (Fig.S2). By age group (≤ 60 vs >60 years), older patients had increased overall mortality risk (p<0.0001), increased melanoma-specific mortality risk (p=0.0100), and poorer DMFS (p=0.0187), but not RFS (p=0.1778) (Fig.S3).
Cause-specific Cox proportional hazards models were used to estimate melanoma-specific hazard ratios, whereas Fine–Gray subdistribution hazard models were applied to account for the competing risk of non-melanoma-related death. For OS (Table III, Fig. 1), age was a strong predictor both as a continuous variable (HR 1.11 per year; 95% CI, 1.07–1.15; p<0.0001) and as a dichotomous variable (>60 vs≤60 years: HR 12.60; 95% CI, 4.31–36.82; p<0.0001). TM showed a borderline association with increased overall mortality risk compared with MIS (HR 1.91; 95% CI, 0.93–3.93; p=0.077). Acral location (HR 2.11; 95% CI, 0.91–4.88; p=0.081) and ulceration (HR 2.63; 95% CI, 0.92–7.53; p=0.072) showed similar borderline associations with increased overall mortality. In multivariable analysis, age remained the only independent predictor of OS (adjusted HR 1.10; 95% CI, 1.07–1.14; p<0.0001), whereas TM retained a near-significant association (adjusted HR 2.13; 95% CI, 0.98–4.61; p=0.056).
Table III. Univariable and multivariable Cox regression analyses for overall mortality and melanoma-specific mortality
| Variable | Overall mortality | Melanoma-specific mortality | ||
|---|---|---|---|---|
| Univariable HR (95% CI); p |
Multivariable HR (95% CI); p |
Univariable HR (95% CI); p |
Multivariable HR (95% CI); p |
|
| Sex | ||||
| Female | Reference | Reference | ||
| Male | 1.24 (0.64–2.41); 0.520 | 0.85 (0.23–3.16); 0.808 | ||
| Age | ||||
| Continuous (per year) | 1.11 (1.07–1.15);<0.0001* | 1.10 (1.07–1.14);<0.0001* | 1.07 (1.01–1.13); 0.027* | 1.06 (1.01–1.12); 0.022* |
| Group >60 y (vs ≤60) | 12.60 (4.31–36.82);<0.0001* | 9.46 (1.18–75.96); 0.035* | ||
| Tumour location | ||||
| Trunk | Reference | |||
| Head and neck | 1.07 (0.12–9.82); 0.954 | |||
| Extremities | 0.26 (0.05–1.42); 0.120 | |||
| Acral | 1.15 (0.39–3.39); 0.798 | |||
| Tumour site (Binary) | ||||
| Nonacral | Reference | Reference | ||
| Acral | 2.11 (0.91–4.88); 0.081 | 1.34 (0.54–3.32); 0.530 | ||
| Histological subtype | ||||
| ALM | Reference | |||
| SSM | 0.47 (0.18–1.21); 0.117 | |||
| NM | 0.34 (0.04–2.65); 0.306 | |||
| LMM | 0.82 (0.11–6.05); 0.845 | |||
| Melanoma type | ||||
| Melanoma in situ | Reference | Reference | Reference | |
| Thin melanoma | 1.91 (0.93–3.93); 0.077 | 2.13 (0.98–4.61); 0.056 | 3.16 (0.66–15.23); 0.152 | |
| Breslow thickness | ||||
| In situ | Reference | Reference | Reference | |
| <0.8 mm | 2.21 (0.99–4.90); 0.052 | 1.75 (0.25–12.43); 0.576 | 1.80 (0.25–12.81); 0.559 | |
| ≥0.8 mm | 1.63 (0.70–3.81); 0.259 | 4.68 (0.90–24.17); 0.066 | 4.80 (0.93–24.80); 0.061 | |
| Ulceration | ||||
| Absent | Reference | Reference | Reference | |
| Present | 2.63 (0.92–7.53); 0.072 | 1.04 (0.35–3.13); 0.944 | 2.30 (0.29–18.45); 0.432 | |
| Mitotic rate | ||||
| <1/mm² | Reference | Reference | ||
| ≥1 /mm² | 1.50 (0.51–4.41); 0.459 | 4.35 (0.38–49.48); 0.236 | ||
| Tumour-infiltrating lymphocytes | ||||
| Absent | Reference | |||
| Brisk | 2.46 (0.52–11.59); 0.254 | |||
| Nonbrisk | 1.93 (0.26–14.00); 0.518 | |||
| Tumour regression | ||||
| Absent | Reference | |||
| Partial | 0.32 (0.04–2.59); 0.287 | |||
| Associated melanocytic lesion | ||||
| Absent | Reference | Reference | ||
| Present | 0.57 (0.12–2.64); 0.468 | 1.47 (0.13–17.09); 0.757 | ||
| Surgical wait time (days) | 1.00 (0.99–1.00); 0.581 | 0.95 (0.87–1.04); 0.241 | ||
|
The multivariable models included variables with P <0.10 in the univariable analysis. *Statistically significant. ALM:acral lentiginous melanoma; CI:confidence interval; HR:hazard ratio; LMM:lentigo maligna melanoma; NM:nodular melanoma; SSM:superficial spreading melanoma. |
||||
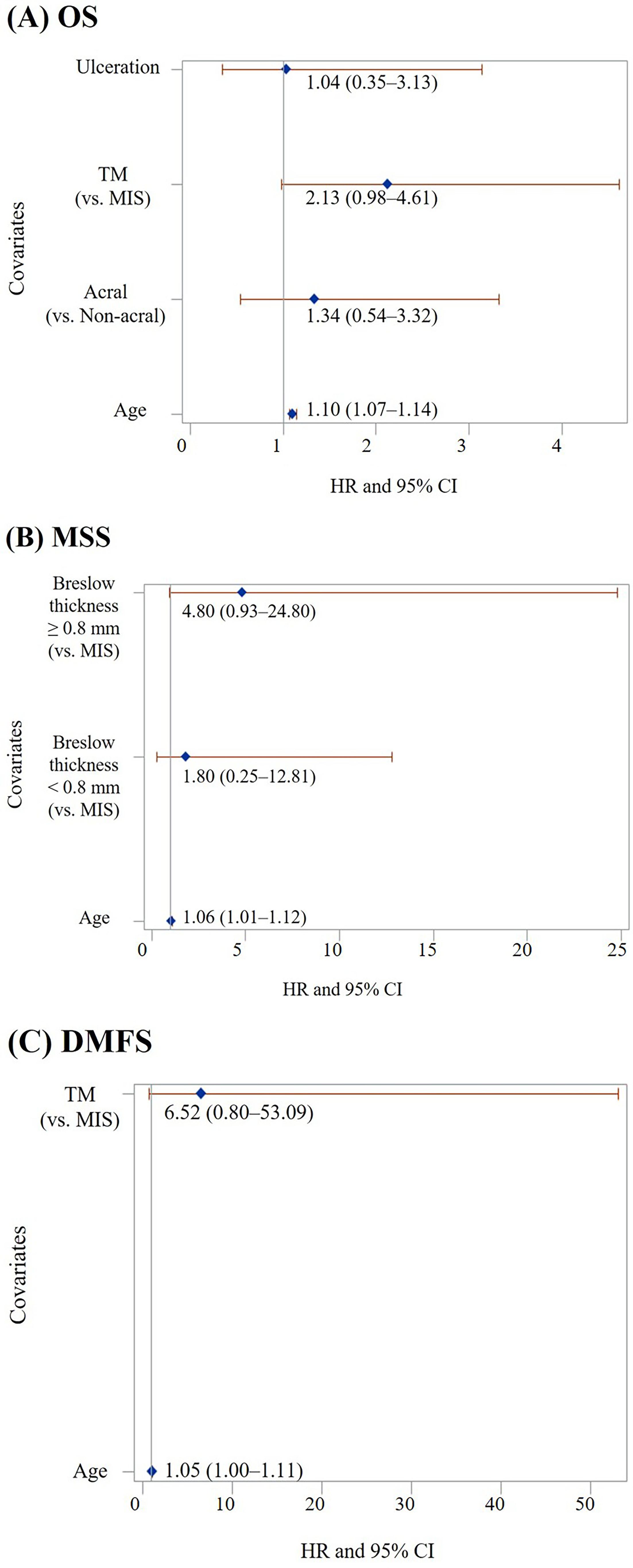
Fig. 1. Forest plots of multivariable Cox proportional hazards regression analyses for (A) overall survival, (B) melanoma-specific survival, (C) distant metastasis-free survival.
For MSS, age remained significant in both univariable and multivariable models (continuous: HR 1.07; 95% CI, 1.01–1.13; p=0.027; adjusted HR 1.06; 95% CI, 1.01–1.12; p=0.022). In Cox analysis, Breslow thickness ≥0.8 mm showed a borderline association with increased melanoma-specific mortality but did not reach statistical significance after multivariable adjustment (adjusted HR 4.80; 95% CI, 0.93–24.80; p=0.061) (Table III, Fig. 1).
For RFS, age (continuous) was associated with an increased risk of recurrence (HR 1.05 per year; 95% CI, 1.01–1.10; p=0.026), whereas age >60 years and other clinicopathologic variables were not significant (Table SI). For DMFS, age >60 years was associated with a higher hazard of distant metastasis (HR 8.28; 95% CI, 1.01–67.65; p=0.049) with a similar trend for age as a continuous variable (HR 1.05; 95% CI, 0.99–1.11; p=0.082) (Table SI, Fig. 1).
Competing-risk analyses using Fine-Gray models are presented in Table SII. For MSS, age remained an independent predictor after accounting for competing deaths (SHR 1.05 per year; 95% CI, 1.02–1.08; p=0.001) and age >60 years was associated with markedly increased risk (SHR 8.25; 95% CI, 1.08–62.79; p=0.042). In the competing-risk framework, Breslow thickness ≥0.8 mm remained prognostically relevant and reached statistical significance (SHR 5.17; 95% CI, 1.02–26.20; p=0.048).
For DMFS (Table SII), age (continuous) remained significant (SHR 1.04; 95% CI, 1.01–1.06; p=0.005). TM, compared with MIS, showed a large effect size with wide CIs (SHR 6.13; 95% CI, 0.75–50.06; p=0.091). Breslow thickness ≥0.8 mm showed a borderline association with DMFS in univariable Fine–Gray analysis (SHR 8.02; 95% CI, 0.90–71.27; p=0.062) but did not reach statistical significance. Gray test demonstrated a borderline difference in DMFS between MIS and TM (p=0.0520) (Fig.S4).
For RFS (Table SII), age (continuous) was the only consistent predictor (SHR 1.03 per year; 95% CI, 1.01–1.06; p=0.013).
The 8 patients who developed distant metastasis are described in Table SIII. Primary tumours ranged from MIS to Breslow thickness 1.0 mm; metastasis occurred 14–119 months after diagnosis; and metastatic sites included liver, bone, central nervous system, spleen, lung and lymph node. The occurrence of distant disease and melanoma-related death in patients with very thin lesions underscores the heterogeneity of risk even within MIS/TM.
DISCUSSION
In this cohort of patients with MIS and TM, adverse outcomes were not negligible despite restriction to early-stage disease. Across analytic approaches, older age and Breslow thickness ≥0.8 mm emerged as the most consistent prognostic determinants, underscoring clinically meaningful risk heterogeneity among lesions traditionally considered low risk.
Our observed event rates exceeded those reported in Western reports. According to the AJCC 8th edition, 5-year MSS rates approach 99 % for T1a and 97–99% for T1b tumours, reflecting the generally favourable outcomes of TMs in Western populations, where melanomas predominantly arise in intermittently sun-exposed sites such as the trunk (9, 25). In contrast, our acral-predominant cohort demonstrated a cumulative melanoma-specific mortality rate of 5.1 % over a mean follow-up of 81 months. This discrepancy suggests that prognostic patterns in acral-predominant Asian populations may differ from those reported in predominantly nonacral Western cohorts. However, neither ALM subtype nor acral location independently predicted increased mortality risk within our cohort, likely reflecting limited statistical power due to the small number of events, and these findings should therefore be interpreted cautiously (1, 6, 9, 15).
In our cohort, TM and MIS each accounted for half of the cases, with ALM representing the leading histologic subtype. Even patients with MIS experienced measurable adverse events, contrasting with the uniformly favourable prognosis often described in Western populations, where SSM predominates (1, 6, 9, 15). Prior studies from East Asia have similarly documented higher recurrence or mortality rates in localized acral melanoma, suggesting that anatomic site, delayed recognition, and distinct clinicopathologic features may exert greater influence on outcomes in this setting (6, 18, 23). The higher burden of acral disease, together with the older age distribution of our patients, likely contributes to the comparatively less favourable real-world outcomes observed in this Asian population (6, 26).
Breslow thickness ≥0.8 mm retained independent prognostic significance for melanoma-specific mortality after competing-risk adjustment, supporting its continued relevance as a clinically meaningful threshold in acral-predominant Asian populations (11, 12, 16). Our findings align with large Australian registry data demonstrating a substantially increased risk of death for tumours measuring 0.8–1.0 mm compared with those <0.8 mm (16). These observations reinforce the global validity of the 0.8 mm cut-off adopted in the AJCC 8th edition (25) and extend its applicability to older Asian cohorts. Importantly, they highlight that submillimetre differences within the TM category remain clinically informative across diverse populations (16, 27).
The prognostic impact of age persisted across survival endpoints, including melanoma-specific survival and distant metastasis-free survival, even after accounting for competing mortality. This indicates that the association between older age and adverse outcomes cannot be explained solely by non-melanoma-related death. In our cohort, patients older than 60 years demonstrated a markedly increased risk of melanoma-specific death. While age is a recognised prognostic factor in Western populations, it often carries less relative weight than tumour thickness in large registry analyses (27). In contrast, in our acral-predominant cohort, age emerged as the most consistent predictor across models, suggesting that host-related factors may exert a comparatively stronger influence in this clinical context.
Notably, several risk factors established in Western cohorts – including male sex, nonacral anatomic sites such as the head, neck, or posterior trunk, ulceration, and mitotic activity – did not demonstrate independent prognostic significance in our multivariable analysis (15, 16). This divergence likely reflects the distinct clinical composition of our cohort. The predominance of ALM and the limited number of nonacral cases reduced statistical power to detect associations for site-specific variables. These findings suggest that prognostic patterns derived from predominantly nonacral Western populations may not be directly transferable to acral-predominant Asian cohorts, particularly in early-stage disease (15, 16). In addition, differences in tumour thickness distribution may partly explain the less favourable outcomes observed in our cohort, as the mean Breslow thickness in our TM cohort (0.67 mm) was slightly higher than that reported in the Swedish population (0.6 mm) (9).
Taken together, these results challenge the assumption that MIS and TM uniformly confer minimal risk in Asian populations. Meaningful rates of distant metastasis and melanoma-specific mortality were observed even within the ≤1 mm category. Older age and Breslow thickness ≥0.8 mm consistently identified patients at higher risk, supporting consideration of risk-adapted surveillance strategies in this setting. Heightened vigilance in the evaluation of subtle acral lesions may also be warranted (10, 12). Future investigations integrating molecular and objective measures of tumour biology and host response may further refine individualized risk stratification, particularly given the occurrence of late distant events arising from very thin primaries (7, 28).
Limitations
This retrospective, single-centre design and modest sample size limit the generalisability and constrain subgroup precision. Molecular testing was incomplete, reflecting real-world practice and limiting assessment of genotype–prognosis relationships. Nonetheless, the prolonged observation window and uniform data capture provide clinically relevant, long-term outcomes for an underrepresented, acral-predominant Asian cohort.
Conclusion
In this acral-predominant Taiwanese cohort, MIS/TM were not uniformly low risk. Older age and Breslow thickness ≥0.8 mm independently identified patients at increased risk, supporting risk-adapted surveillance in Asian populations.
ACKNOWLEDGEMENTS
The authors thank the Center of Statistical Consultation and Research and the Statistical Center of the Clinical Trial Center, Department of Medical Research, National Taiwan University Hospital; the Integrated Medical Database (NTUH-iMD); and the Taiwan Cancer Registry for their statistical and data support.
REFERENCES
- Rastrelli M, Tropea S, Rossi CR, Alaibac M. Melanoma: epidemiology, risk factors, pathogenesis, diagnosis and classification. In Vivo 2014; 28: 1005–1011.
- Conforti C, Zalaudek I. Epidemiology and risk factors of melanoma: a review. Dermatol Pract Concept 2021; 11: e2021161S. https://doi.org/10.5826/dpc.11S1a161S
- van der Leest RJT, Zoutendijk J, Nijsten T, Mooi WJ, van der Rhee JI, de Vries E, et al. Increasing time trends of thin melanomas in The Netherlands: What are the explanations of recent accelerations? Eur J Cancer 2015; 51: 2833–2841. https://doi.org/10.1016/j.ejca.2015.09.008
- Xu J, Wang X, Liu W, Liu X, Li G. Analysis and comparison of the trends in burden of malignant cutaneous melanoma in East Asian countries and regions and worldwide from 1991 to 2021. Front Public Health 2025; 13: 1487177. https://doi.org/10.3389/fpubh.2025.1487177
- Yu L, Yan F, Qi J, Wang L, Zhou M, Yin P. Burden of melanoma in China and its provinces from 1990 to 2021: an analysis for the Global Burden of Disease Study 2021. Front Public Health 2024; 12: 1486617. https://doi.org/10.3389/fpubh.2024.1486617
- Chang JWC, Guo J, Hung CY, Lu S, Shin SJ, Quek R, et al. Sunrise in melanoma management: time to focus on melanoma burden in Asia. Asia Pac J Clin Oncol 2017; 13: 423–427. https://doi.org/10.1111/ajco.12670
- Lee HY, Chay WY, Tang MB, Chio MT, Tan SH. Melanoma: differences between Asian and Caucasian patients. Ann Acad Med Singap 2012; 41: 17–20. https://doi.org/10.47102/annals-acadmedsg.V41N1p17
- Sheen YS, Tan KT, Tse KP, Liao YH, Lin MH, Chen JS, et al. Genetic alterations in primary melanoma in Taiwan. Br J Dermatol 2020; 182: 1205–1213. https://doi.org/10.1111/bjd.18425
- Isaksson K, Mikiver R, Eriksson H, Lapins J, Nielsen K, Ingvar C, et al. Survival in 31 670 patients with thin melanomas: a Swedish population-based study. Br J Dermatol 2021; 184: 60–67. https://doi.org/10.1111/bjd.19015
- Green AC, Baade P, Coory M, Aitken JF, Smithers M. Population-based 20-year survival among people diagnosed with thin melanomas in Queensland, Australia. J Clin Oncol 2012; 30: 1462–1467. https://doi.org/10.1200/JCO.2011.38.8561
- Lo SN, Scolyer RA, Thompson JF. Long-term survival of patients with thin (T1) cutaneous melanomas: a Breslow thickness cut point of 0.8 mm separates higher-risk and lower-risk tumors. Ann Surg Oncol 2018; 25: 894–902. https://doi.org/10.1245/s10434-017-6325-1
- Claeson M, Baade P, Brown S, Soyer HP, Smithers BM, Green AC, et al. Clinicopathological factors associated with death from thin (≤ 1.00 mm) melanoma. Br J Dermatol 2020; 182: 927–931. https://doi.org/10.1111/bjd.18560
- Claeson M, Tan SX, Lambie D, Brown S, Walsh MD, Baade PD, et al. The association between BRAF-V600E mutations and death from thin (≤1.00 mm) melanomas: a nested case-case study from Queensland, Australia. J Eur Acad Dermatol Venereol 2023; 37: e1168–e1172. https://doi.org/10.1111/jdv.19173
- Slingluff CL Jr, Vollmer RT, Reintgen DS, Seigler HF. Lethal “thin” malignant melanoma. Identifying patients at risk. Ann Surg 1988; 208: 150–161. https://doi.org/10.1097/00000658-198808000-00004
- Gontijo JRV, Nelson JH, Diehl K, Korcheva VB, Bittencourt FV, Leachman SA. Thin and in situ melanomas of unfavorable prognosis: a retrospective observational analysis of local recurrence, metastasis, and death in early-stage disease. J Am Acad Dermatol 2025; 92: 325–327. https://doi.org/10.1016/j.jaad.2024.09.057
- Lo SN, Williams GJ, Cust AE, Ollila DW, Varey AHR, Ch’ng S, et al. Risk of death due to melanoma and other causes in patients with thin cutaneous melanomas. JAMA Dermatol 2025; 161: 167–174. https://doi.org/10.1001/jamadermatol.2024.4900
- Chan KKW, Chan RCL, Ho RSL, Chan JYW. Clinical patterns of melanoma in Asians: 11-year experience in a tertiary referral center. Ann Plast Surg 2016; 77 Suppl 1: S6–S11. https://doi.org/10.1097/SAP.0000000000000731
- Fujisawa Y, Yoshikawa S, Takenouchi T, Mori S, Asai J, Uhara H, et al. Melanoma skin cancer statistics derived from 7442 Japanese patients: Japanese melanoma study. Int J Clin Oncol 2025; 30: 844–855. https://doi.org/10.1007/s10147-025-02747-9
- Jang H, Ryu HJ, Kim SK. Genetic characteristics of primary cutaneous malignant melanoma in Koreans compared with Western populations. In Vivo 2023; 37: 862–867. https://doi.org/10.21873/invivo.13154
- Kado S, Komine M. Recent advances in molecular research and treatment for melanoma in Asian populations. Int J Mol Sci 2025; 26: 26. https://doi.org/10.3390/ijms26115370
- Lee TL, Liao YH, Liau JY, Sheen YS. Risk factors of recurrence and distant metastasis in primary cutaneous melanoma in Taiwan. Sci Rep 2021; 11: 21012. https://doi.org/10.1038/s41598-021-00386-4
- Oh Y, Choi S, Cho MY, Nam KA, Shin SJ, Chang JS, et al. Male sex and Breslow thickness are important risk factors for recurrence of localized melanoma in Korean populations. J Am Acad Dermatol 2020; 83: 1071–1079. https://doi.org/10.1016/j.jaad.2019.09.029
- Lv J, Dai B, Kong Y, Shen X, Kong J. Acral melanoma in Chinese: a clinicopathological and prognostic study of 142 cases. Sci Rep 2016; 6: 31432. https://doi.org/10.1038/srep31432
- Chang CK, Hsieh YS, Chen PN, Chu SC, Huang JY, Wang YH, et al. A cohort study: comorbidity and stage affected the prognosis of melanoma patients in Taiwan. Front Oncol 2022; 12: 846760. https://doi.org/10.3389/fonc.2022.846760
- Gershenwald JE, Scolyer RA, Hess KR, Sondak VK, Long GV, Ross MI, et al. Melanoma staging: evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin 2017; 67: 472–492. https://doi.org/10.3322/caac.21409
- Zheng YJ, Ho C, Lazar A, Ortiz-Urda S. Poor melanoma outcomes and survival in Asian American and Pacific Islander patients. J Am Acad Dermatol 2021; 84: 1725–1727. https://doi.org/10.1016/j.jaad.2020.08.086
- Leiter U, Buettner PG, Eigentler TK, Garbe C. Prognostic factors of thin cutaneous melanoma: an analysis of the central malignant melanoma registry of the german dermatological society. J Clin Oncol 2004; 22: 3660–3667. https://doi.org/10.1200/JCO.2004.03.074
- Yang J, Lian JW, Chin YPH, Wang L, Lian A, Murphy GF, et al. Assessing the prognostic significance of tumor-infiltrating lymphocytes in patients with melanoma using pathologic features identified by natural language processing. JAMA Netw Open 2021; 4: e2126337. https://doi.org/10.1001/jamanetworkopen.2021.26337