ORIGINAL REPORT
The Diagnostic Accuracy of Ex Vivo Confocal Laser Scanning Microscopy for Basal Cell Carcinoma: A Systematic Review and Meta-analysis
Sarah LUKACS1, Luis MESSNER1![]() , Michael FLAIG1
, Michael FLAIG1![]() , Andreas OHLMANN2
, Andreas OHLMANN2![]() , Daniela HARTMANN1,3
, Daniela HARTMANN1,3![]() and Benjamin KENDZIORA1,3*
and Benjamin KENDZIORA1,3*![]()
1Department of Dermatology and Allergy, University Hospital, LMU, Munich, Germany, 2Department of Ophthalmology, University Hospital, LMU, Munich, Germany, and 3Department of Dermatology, Thalkirchner Street Hospital, Munich Municipial Hospital Group, Munich, Germany
Corr: Benjamin Kendziora, Department of Dermatology and Allergy, University Hospital, Ludwig Maximilian University (LMU), Frauenlobstr. 9-11, 80337 Munich, Germany. *Email: benjamin.kendziora@med.uni-muenchen.de
Key words: basal cell carcinoma; confocal laser scanning microscopy; diagnostic accuracy; dermatologic surgical procedures; Mohs surgery; meta-analysis.
Citation: Acta Derm Venereol 2026; 106: adv-2026-0393. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0393.
Copyright: 2026 ©Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 2, 2026. Accepted after revision: May 26, 2026.
Published: Jun 15, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request. Access to the data will be granted for legitimate academic purposes.
Ethical approval was not required for this systematic review and meta-analysis, as it relied solely on previously published and anonymized data.
This systematic review and meta-analysis evaluated available data on the diagnostic accuracy of ex vivo confocal laser scanning microscopy (EVCM) for the diagnosis of basal cell carcinoma (BCC) in tissue specimens and for margin assessment in micrographic surgery, using conventional histopathological analysis as reference standard. MEDLINE and Embase were systematically searched in November 2024 in accordance with PRISMA guidelines to identify diagnostic accuracy studies evaluating EVCM for BCC. Pooled sensitivity and specificity were estimated using bivariate random-effects models. Sixteen studies comprising 1,387 specimens were included. The pooled mean EVCM acquisition time was 7.0 min (95% confidence interval [CI]: 5.3–9.4). For BCC diagnosis in tissue specimens, pooled sensitivity was 91.4% (95% CI: 85.9–94.9) and pooled specificity was 91.1% (95% CI: 79.2–94.5). Regarding margin assessment, pooled sensitivity and specificity were 79.5% (95% CI: 65.0–89.0) and 92.2% (95% CI: 85.5–95.9). In conclusion, EVCM shows high sensitivity and specificity for BCC diagnosis in tissue specimens and may selectively replace conventional histology when rapid diagnosis is desired. For margin assessment, EVCM has high specificity but moderate sensitivity. Therefore, conventional histology should still be considered as a subsequent step, particularly after the final excision stage of stepwise micrographic surgery.
SIGNIFICANCE
Basal cell carcinoma (BCC) is the most common skin cancer. By identifying and analysing published data, we aimed to find out how accurate a newer microscope technique, called ex vivo confocal laser scanning microscopy (EVCM), is for diagnosing BCC and checking whether the cancer has been completely removed during surgery. We found that EVCM correctly diagnosed BCC in about 9 out of 10 tissue samples. When used to assess surgical margins, tumour involvement and thus the need for re-excision was correctly identified in about 8 out of 10 cases and consequently missed in about 2 out of 10 cases.
Basal cell carcinoma (BCC) is the most frequently occurring skin cancer in fair-skinned populations, comprising around 3 quarters of all diagnosed skin cancers (1). Although its metastatic potential is low, BCC is locally invasive and can cause significant morbidity if not adequately excised (2).
In the diagnostic work-up of suspected BCC, a punch or shave biopsy is typically performed to establish histopathological confirmation. Upon verification of the diagnosis, margin-controlled (micrographic) surgery is commonly employed in high-risk tumours in critical anatomical sites like the face to achieve complete tumour clearance while minimizing removal of uninvolved tissue (3).
The current gold standard for diagnosis and margin control is the histopathological evaluation of formalin-fixed, paraffin-embedded tissue. However, this process is time-consuming and resource-intensive, thereby limiting intraoperative decision-making. To enable intraoperative assessment of tumour-free margins, Mohs micrographic surgery was developed. In Mohs micrographic surgery, cryoconserved (frozen) tissue sections are prepared and examined intraoperatively, allowing evaluation of the entire peripheral and deep margins of the excised specimen. If residual tumour is detected, the procedure is performed in a stepwise manner with additional excision stages until tumour-free margins are achieved. This technique combines complete margin control with maximal preservation of healthy tissue (4).
In recent years, ex vivo confocal laser scanning microscopy (EVCM) has emerged as a promising imaging modality that enables real-time microscopic visualization of freshly excised tissue without the need for cryoconservation or conventional staining. This technique therefore has the potential to facilitate intraoperative margin assessment more rapidly and with fewer resources. EVCM provides optical sections of skin structures at a resolution comparable to that of traditional histopathology, allowing for the identification of characteristic BCC features such as tumour nests, peripheral palisading and stromal clefting (5, 6, 7). Several studies have investigated the sensitivity and specificity of EVCM for both the diagnosis and margin assessment of BCC.
The aim of this systematic review and meta-analysis was to synthesize data from existing studies on the diagnostic accuracy of EVCM for the diagnosis of BCC in tissue specimens and for margin assessment in micrographic surgery, to better define its clinical applicability.
MATERIALS AND METHODS
Protocol registration and reporting standards
This systematic review and meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) of Diagnostic Test Accuracy Studies guidelines (8). The study protocol was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the ID CRD42024601458.
Search strategy and study selection
A systematic literature search was conducted in MEDLINE and Embase (via Ovid) on 1 November 2024 to identify studies evaluating the diagnostic accuracy of EVCM in the diagnosis and/or margin assessment of BCC. The complete search string is provided in Table SI. In addition to the database search, the reference lists of eligible studies were reviewed, and experts in the field were contacted to identify potentially relevant studies.
Studies were eligible for inclusion if they
investigated the diagnostic accuracy of EVCM for the diagnosis of BCC in tissue specimens and/or margin control in micrographic surgery
reported a 2×2 contingency table or provided sufficient information to reconstruct one and
used formalin-fixed paraffin-embedded or cryocon-served histology as the reference standard.
Studies were excluded if the EVCM evaluation was performed exclusively by artificial intelligence or automated image analysis without human expert validation.
No restrictions regarding publication year were applied. Conference abstracts, case reports, review articles and opinions were excluded. In addition, studies that included fewer than 10 cases of BCC were excluded.
Data extraction
Two reviewers (S.L. and L.M.) independently extracted data from the included studies using a predefined data extraction form. Extracted variables included study design; patient and lesion characteristics; specimen preparation method (punch, shave, bread loaf excision, or micrographic excision using Mohs procedure (9, 10), randstrip method = “Tuebinger Torte” (11), muffin technique (11) or other); EVCM device type; EVCM acquisition time; and the number of true positives, false positives, false negatives and true negatives.
All extracted data were cross-checked for accuracy and consistency between the reviewers. In cases of ambiguous or inconsistent information, the corresponding authors of the original publications were contacted for clarification. Disagreements between reviewers were resolved through discussion, and if necessary, arbitration by a third reviewer (B.K.).
Data synthesis and statistical analysis
All statistical analyses were performed using R version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria). Analyses were conducted by one author (B.K.), who holds an M.Sc. in Biostatistics, using the meta (12) and mada R packages (13).
Continuous variables such as mean age of included patients and mean EVCM acquisition time were pooled using random-effects meta-analysis models for continuous outcomes. Pooled proportions of histological subtypes (nodular, sclerodermiform, superficial/multifocal and others) and tumor localizations (head/neck, trunk, extremities and other sites) were estimated using random-effects models for proportions.
Bivariate random-effects models following the Reitsma et al. framework (14) were applied to pool sensitivity and specificity estimates of EVCM with formalin-fixed paraffin-embedded or cryoconserved histology as the reference standard. Analyses were conducted separately for diagnostic detection of BCC in punch, shave and broad leaf excision specimens, and for margin assessment in micrographic excisions.
To explore heterogeneity in diagnostic accuracy across different micrographic surgery techniques, subgroup analyses using meta-regression models were applied to assess differences in the diagnostic performance of EVCM between the following methods: Mohs micrographic surgery (9, 10), the randstrip method (“Tübinger Torte”) (11) and the muffin technique (11).
A robustness analysis/sensitivity analysis was performed to assess the stability of the results and to determine whether the diagnostic performance estimates were consistent across different EVCM device generations. This analysis compared earlier- vs newer-generation EVCM devices for both BCC diagnosis in tissue specimens and margin assessment using meta-regression models to evaluate potential differences in accuracy between device generations.
An alpha level of 0.05 was considered statistically significant for all analyses.
Risk of bias assessment
The risk of bias and applicability concerns for each included study were evaluated using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool (15). Two reviewers (S.L. and L.M.) independently assessed four domains: patient selection, index test, reference standard and flow and timing. For each domain, risk of bias was rated “low”, “high” or “unclear”, applicability concerns were considered for the first three domains. Discrepancies were resolved by consensus, with a third reviewer consulted (B.K.) if agreement could not be reached.
Potential publication bias was assessed visually using funnel plots of diagnostic odds ratios from studies evaluating the diagnostic accuracy of EVCM for BCC diagnosis in tissue specimens and for margin assessment. Funnel plot asymmetry was formally tested using the Harbord regression test (16).
Certainty of evidence assessment
The certainty of the evidence for each pooled diagnostic accuracy measure was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework for diagnostic tests (17). The certainty of evidence for a pooled effect estimate was downgraded when substantial heterogeneity was present among the included effect estimates, when the pooled estimate showed wide confidence intervals, when several studies with a high risk of bias in the 5 domains were included in the analysis, or when publication bias was detected.
RESULTS
Study selection
The electronic database search yielded 880 records, which were screened by title and abstract. Of these, 155 full-text articles were assessed for eligibility. Ultimately, 16 studies met the inclusion criteria and were included in the quantitative synthesis (5, 7, 11, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30). The study selection process is summarized in the PRISMA flow diagram (Fig. 1).
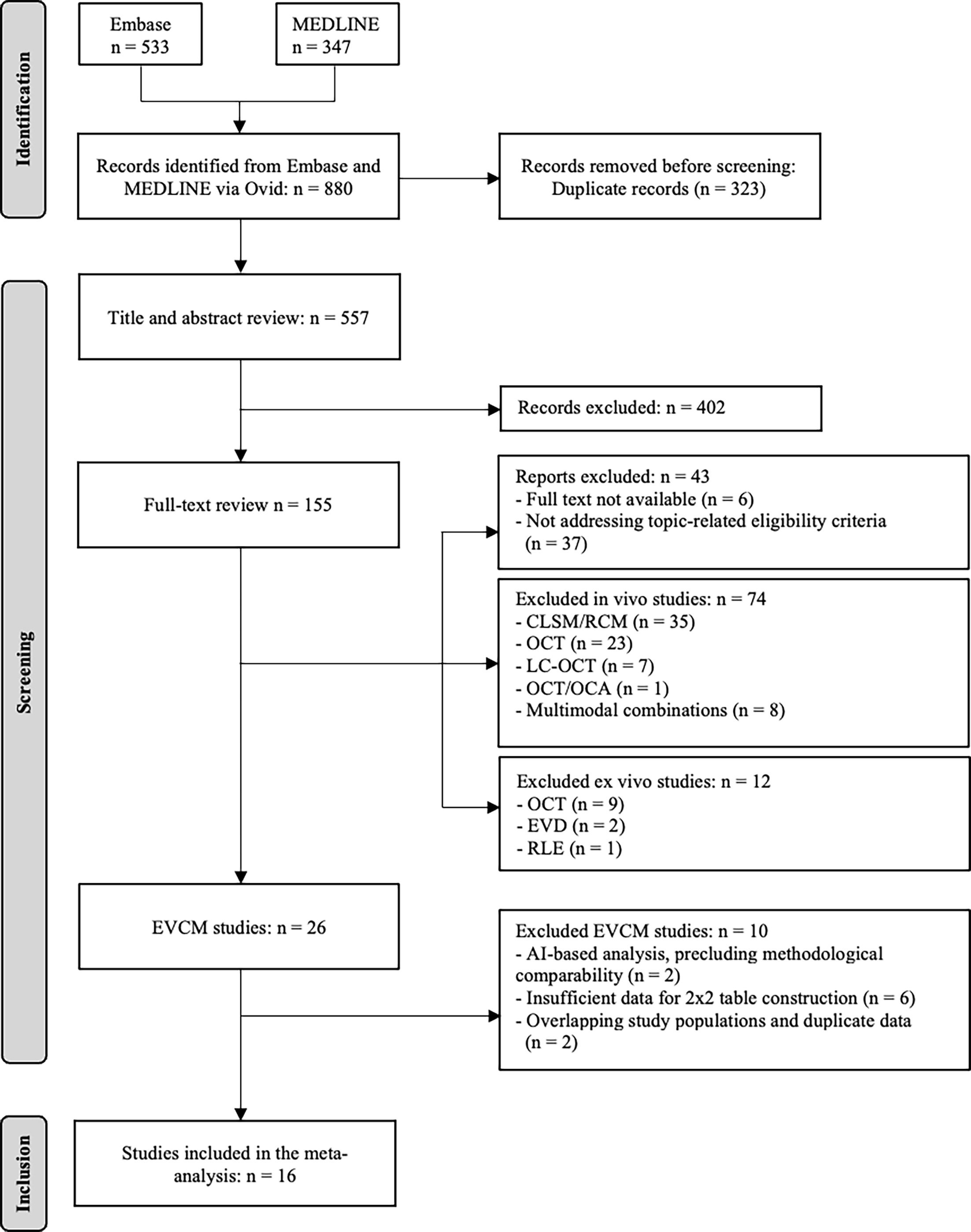
Fig. 1. Screening of References. PRISMA flow diagram summarizing the study selection process structured into 3 phases: identification, screening and inclusion. Screening the reference lists of included studies and contacting experts in the field did not reveal additional eligible studies. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; CLSM: confocal laser scanning microscopy; RCM: reflectance confocal microscopy; OCT: optical coherence tomography; LC-OCT: line-field optical coherence tomography; OCA: optical coherence angiography; EVD: ex vivo dermoscopy; RLE: Rapid Lump examination.
Study characteristics
The 16 included studies comprised a total of 1,387 specimens. The majority of specimens were excised from the head and neck region (91.8%; 95% CI [confidence interval]: 76.0–97.5). Nodular BCC was the most common histopathological subtype (45.3%; 95% CI: 33.8–57.3), followed by sclerodermiform/micronodular BCC (30.1%; 95% CI: 17.8–45.9), superficial BCC (10.8%; 95% CI: 6.6–17.2) and other forms. Overall, 15.9% of specimens were free of BCC (95% CI: 7.1–31.9). The mean age of included patients was 73.2 years (95% CI: 71.5–74.9), and 41.6% (95% CI: 36.3–47.0) were female.
Twelve studies utilized the VivaScope® 2500 microscope (Lucid Inc., Rochester, USA), one study used the VivaScope® 2000, one study applied a strip-mosaicing confocal microscope based on VivaScope® technology, one study employed the Histolog® Scanner V1(SamanTree Medical SA, Awans, Belgium) and one used the Histolog® Scanner V2. The pooled mean EVCM acquisition time was 7.0 min (95% CI: 5.3–9.4).
Diagnostic accuracy for BCC diagnosis in tissue specimens
Seven studies reported the diagnostic accuracy for EVCM in BCC diagnosis using punch, shave or bread-loaf excision specimens. Forest plots of individual study sensitivities and specificities are presented in Figs. S1 and S2, respectively. The pooled sensitivity was 91.4% (95% CI: 85.9–94.9), and the pooled specificity was 91.1% (95% CI: 79.2–94.5). Between-study heterogeneity was low (I²=5.2%). The summary receiver operating characteristic (SROC) curve is shown in Fig. 2.

Fig. 2. Summary receiver operating characteristic (SROC) curve for the diagnostic accuracy of ex vivo confocal microscopy (EVCM) in the diagnosis of basal cell carcinoma (BCC) in tissue specimens. The solid line represents the SROC curve, illustrating the trade-off between sensitivity and the false-positive rate across the included studies, with each triangle representing an individual study estimate. The solid oval indicates the 95% confidence region around the summary estimate (large triangle). The false-positive rate is mathematically equivalent to 1 – specificity.
Given the low heterogeneity, relatively narrow confidence intervals, absence of major concerns regarding risk of bias in most studies included in this analysis (Table SII and Fig. S3) and the lack of evidence for publication bias (Fig. S4), the certainty of evidence for diagnostic detection was rated as high according to the GRADE framework.
Diagnostic accuracy for margin assessment in micrographic surgery
Twelve studies investigated the diagnostic accuracy of EVCM for margin assessment of BCC in the context of micrographic surgery. Forest plots of sensitivities and specificities are shown in Figs S5 and S6. The pooled sensitivity for margin assessment was 79.5% (95% CI: 65.0–89.0), and the pooled specificity was 92.2% (95% CI: 85.5–95.9), with moderate heterogeneity (I²=13.8%). The SROC curve is shown in Fig. 3.
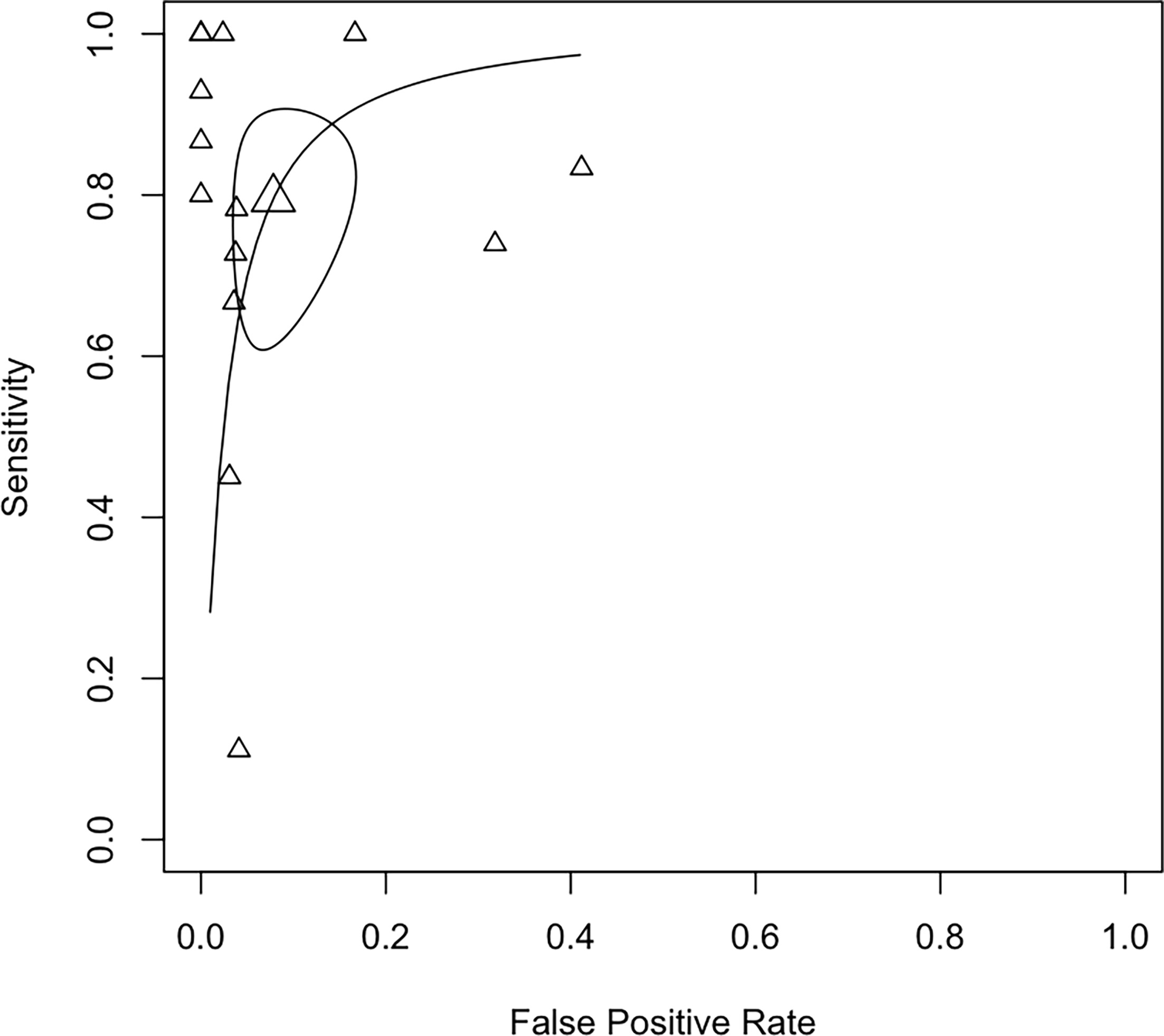
Fig. 3. Summary receiver operating characteristic (SROC) curve for the diagnostic accuracy of ex vivo confocal microscopy (EVCM) in the margin assessment in micrographic surgery of basal cell carcinoma (BCC). The solid line represents the SROC curve, illustrating the trade-off between sensitivity and the false positive rate across the included studies, with each triangle representing an individual study estimate. The solid oval indicates the 95% confidence region around the summary estimate (large triangle). The false-positive rate is mathematically equivalent to 1 – specificity.
Given the moderate heterogeneity, acceptably narrow confidence intervals, absence of major concerns regarding risk of bias in most studies included in this analysis (Table SII and Fig. S3), and the lack of evidence for publication bias (Fig. S7), the certainty of evidence for margin assessment was rated as high according to the GRADE framework.
Subgroup analysis by micrographic surgery technique
Subgroup analyses were conducted to explore heterogeneity across micrographic surgery techniques for margin assessment. When the Mohs micrographic surgery procedure was used, the pooled sensitivity was 87.6% (95% CI: 44.9–98.4) and the pooled specificity was 93.8% (95% CI: 85.5–97.4; I²=26.4). For the margin-strip technique (“Tübinger Torte”), the pooled sensitivity was 67.9% (95% CI: 52.1–80.5) and the pooled specificity was 93.3% (95% CI: 79.4–98.1; I²=37.1). For the muffin technique, the pooled sensitivity was 76.1% (95% CI: 34.1–95.1) and the pooled specificity was 85.6% (95% CI: 25.0–99.1; I²=0). The SROC curves for these subgroups are presented in Fig. 4. No statistically significant differences in sensitivity or specificity were observed between excision techniques (p>0.05).
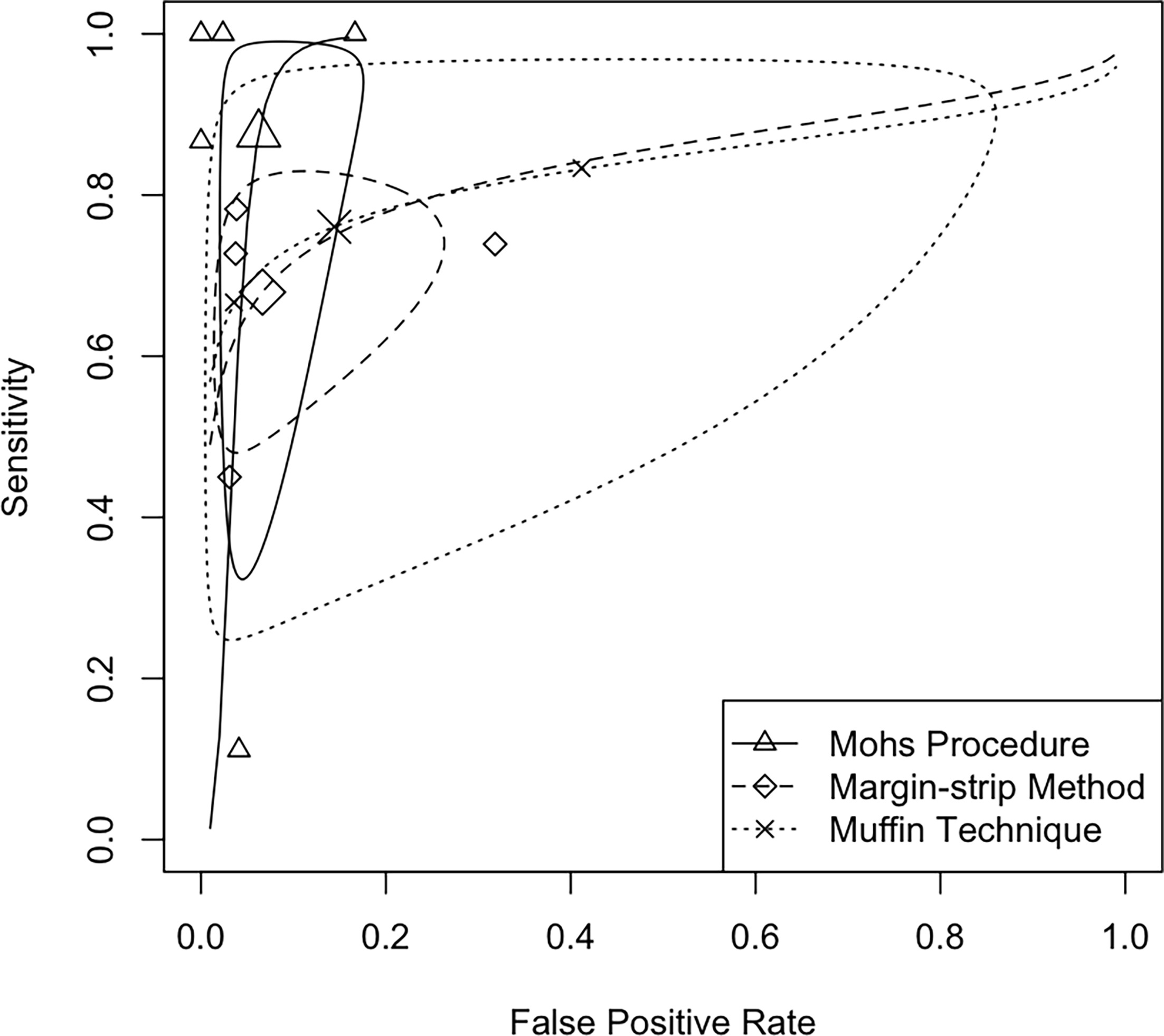
Fig. 4. Summary receiver operating characteristic (SROC) curve for the diagnostic accuracy of ex vivo confocal microscopy (EVCM) in the margin assessment in micrographic surgery of basal cecll carcinoma (BCC), subgrouped by excision technique. The solid, dashed and dotted lines represent the SROC curves, illustrating the trade-off between sensitivity and the false-positive rate across the included studies. Each triangle, diamond and cross represents an individual study estimate corresponding to a specific excision technique. The solid, dashed and dotted ovals indicate the 95% confidence regions around the respective summary estimates (large triangle, diamond or cross). The false positive rate is mathematically equivalent to 1 – specificity.
The GRADE certainty of evidence was downgraded to moderate for the Mohs and margin-strip subgroups and to low for the muffin technique due to wide confidence intervals.
Robustness analysis
A sensitivity analysis was performed to compare diagnostic performance between EVCM devices of earlier and newer generations. For BCC diagnosis in tissue specimens, newer-generation devices (VivaScope® 2500 and Histolog® Scanner V2) demonstrated a significantly higher pooled sensitivity of 93.9% (95% CI: 90.6–96.1) compared with older-generation devices (VivaScope® 2000 and Histolog® Scanner V1), which showed a sensitivity of 83.0% (95% CI: 73.7–89.5; p=0.002). The pooled specificity did not differ significantly between generations (newer: 90.0%, 95% CI: 71.4–97.0; older: 93.7%, 95% CI: 80.6–98.2).
For margin assessment, the pooled sensitivity with newer-generation devices was 80.0% (95% CI: 64.2–89.9), compared to 77.8% (95% CI: 22.7–97.7) for older-generation devices. This difference was not statistically significant. Similarly, pooled specificity did not differ significantly between device generations (newer: 92.4%, 95% CI: 82.7–96.8; older: 93.2%, 95% CI: 79.9–97.9).
Summary of key findings
The key findings are summarized in Table I.
Table I. Summary of diagnostic accuracy measures of EVCM for BCC
| Outcome | pooled sensitivity, % (95% ci) | Pooled specificity, % (95% CI) | I², % | GRADE certainty of evidence |
|---|---|---|---|---|
| BCC diagnosis in tissue specimens | 91.4 (85.9–94.9) | 91.1 (79.2–94.5) | 5.2 | High |
| Margin assessment in micrographic surgery | 79.5 (65.0–89.0) | 92.2 (85.5–95.9) | 13.8 | High |
| Mohs procedure | 87.6 (44.9–98.4) | 93.8 (85.5–97.4) | 26.4 | Moderate |
| Margin-strip method (“Tübinger Torte”) | 67.9 (52.1–80.5) | 93.3 (79.4–98.1) | 37.1 | Moderate |
| Muffin technique | 76.1 (34.1–95.1) | 85.6 (25.0–99.1) | 0.0 | Low |
|
BCC: basal cell carcinoma; CI: confidence interval; EVCM: ex vivo confocal microscopy; GRADE: Grading of Recommendations Assessment, Development, and Evaluation framework. |
||||
DISCUSSION
Conventional histopathological examination of resected tissue is the reference standard for diagnosis and margin control of BCC (31). To extend diagnostic capabilities and develop more time-efficient intraoperative tools, EVCM has emerged as a promising approach to accelerate and streamline surgical workflows (5, 6, 7). In this context, we conducted a systematic review and meta-analysis aiming to estimate the diagnostic accuracy of EVCM for BCC diagnosis in tissue specimens and margin assessment in micrographic surgery.
Our results are based on 16 studies encompassing a total of 1,387 excised specimens. Seven studies evaluated the diagnostic accuracy for BCC diagnosis in tissue specimens and 12 studies assessed margin control. EVCM correctly diagnosed the presence or absence of BCC in approximately 9 out of 10 tissue specimens. In contrast, diagnostic accuracy for margin assessment was lower. EVCM detected tumour-free margins in around 9 out of 10 cases during micrographic surgery, whereas tumour involvement of the excision margin was detected in approximately 8 out of 10 cases. No statistically significant differences in sensitivity or specificity were observed between micrographic surgery techniques; however, the certainty of the evidence was reduced due to wide confidence intervals. When comparing EVCM device generations, sensitivity for BCC diagnosis in tissue specimens was significantly higher with newer-generation devices than with earlier models, while specificity remained comparable. No significant differences were observed for margin assessment.
Comparison with relevant literature
Given the current state of research, most existing review articles on EVCM in this field are qualitative in nature, focusing on technical aspects, characteristic imaging features and the discussion of its potential role as an intraoperative pathology tool (32, 33, 34). Ge, Cherian and Dang presented an abstract of a systematic review and meta-analysis on the diagnostic accuracy of EVCM for margin assessment of BCC at the Australasian College of Dermatologists 55th Annual Scientific Meeting in 2023 (35) however, no corresponding journal publication of this work could be identified in MEDLINE or Embase.
Most available evidence summarizing the use of confocal laser scanning microscopy in dermatologic surgery focuses on in vivo applications (36, 37). Lupu et al. (36) conducted a comprehensive systematic review and meta-analysis on the diagnostic accuracy of in vivo confocal laser scanning microscopy for BCC, reporting pooled sensitivity and specificity estimates of 92% and 93%, respectively. These values are comparable to the pooled sensitivity and specificity derived from the ex vivo data included in our systematic review and meta-analysis, although heterogeneity was substantially higher in the in vivo studies.
Clinical implications
For the diagnosis of BCC in skin tissue specimens such as punch or shave samples, EVCM demonstrates high sensitivity and specificity, correctly identifying the presence or absence of tumour in approximately 9 out of 10 cases. This high level of diagnostic accuracy suggests that EVCM could selectively replace conventional histology in certain scenarios where rapid diagnosis is desired to enable prompt surgical intervention.
For margin assessment, EVCM demonstrates high specificity but moderate sensitivity, with tumour involvement correctly identified in approximately 8 out of 10 cases. Consequently, tumour extension at the surgical margin may be missed in around 2 out of 10 cases. This level of uncertainty does not yet support the use of EVCM as a stand-alone method for intraoperative margin control. Therefore, conventional histology should be considered as a subsequent step, at least after the final excision stage in stepwise micrographic surgery, to ensure detection and appropriate management of any tumour extensions missed by EVCM.
Strengths and limitations
To our knowledge, this systematic review and meta-analysis represents the first comprehensive quantitative synthesis of the diagnostic accuracy of EVCM for both BCC diagnosis in tissue specimens and margin assessment in micrographic surgery. The study was conducted according to established methodological standards for diagnostic test accuracy reviews, including prospective protocol registration in PROSPERO, adherence to PRISMA guidelines and use of the QUADAS-2 and GRADE frameworks to assess risk of bias and certainty of evidence. The application of bivariate random-effects models allowed joint pooling of sensitivity and specificity while accounting for their interdependence. In addition, subgroup and robustness analyses provided insight into potential sources of heterogeneity, including different micrographic surgery techniques and EVCM device generations, thereby strengthening the interpretability and clinical relevance of the findings.
Several limitations should also be acknowledged. First, subgroup estimates for individual micrographic surgery techniques were based on a limited number of studies, resulting in wide confidence intervals and reduced certainty of evidence. Second, most included studies were single-centre investigations conducted under experimental or semi-controlled conditions, which may limit generalizability to routine clinical practice. Third, institutional clustering may represent a potential source of bias, as several included studies originated from research within our institution. Fourth, the literature search was limited to 2 databases rather than 3 or more, which may have reduced the comprehensiveness of study identification.
Future research
Future research should focus on improving the diagnostic accuracy of EVCM for margin assessment, as current performance does not yet support its use as a stand-alone method for intraoperative margin control.
In addition, future studies should explore integrated diagnostic workflows, including the potential role of in vivo confocal laser scanning microscopy (IVCM) in identifying lesions that are particularly suitable for EVCM (38), not only for detection but also for subtype classification and assessment of tumour extent. Such preselection may increase pretest probability, potentially further enhance diagnostic accuracy of EVCM and enable nonsurgical treatment of superficial or flat nodular BCC.
The integration of artificial intelligence is expected to become increasingly relevant for advancements in imaging technology and image interpretation, for example by enhancing consistency and reducing dependency on reader expertise (39).
Conclusion
EVCM demonstrates high sensitivity and specificity for the diagnosis of BCC in punch and shave biopsies and may selectively replace conventional histology in scenarios where rapid diagnosis is desired to enable prompt surgical intervention.
For margin assessment, EVCM shows high specificity but moderate sensitivity. Therefore, conventional histology should currently still be considered as a subsequent step, at least after the final excision stage in stepwise micrographic surgery.
ACKNOWLEDGEMENTS
This work was supported by the Munich Clinician Scientist Program (MCSP) of the Ludwig Maximilian University (LMU), grant number CS 067. The funders had no role in the study design, data collection, analysis, or interpretation of the data, nor in the writing of the report or the decision to submit the article for publication. The researchers were independent of the funders.
REFERENCES
- Lomas A, Leonardi-Bee J, Bath-Hextall F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br J Dermatol 2012; 166: 1069–1080. https://doi.org/10.1111/j.1365-2133.2012.10830.x
- Tang S, Thompson S, Smee R. Metastatic basal cell carcinoma: case series and review of the literature. Australas J Dermatol 2017; 58: e40–e43. https://doi.org/10.1111/ajd.12459
- Basset-Seguin N, Herms F. Update in the management of basal cell carcinoma. Acta Derm Venereol 2020; 100: adv00140. https://doi.org/10.2340/00015555-3495
- Brown AC, Brindley L, Hunt WTN, Earp EM, Veitch D, Mortimer NJ, et al. A review of the evidence for Mohs micrographic surgery. Part 2: basal cell carcinoma. Clin Exp Dermatol 2022; 47: 1794–1804. https://doi.org/10.1111/ced.15266
- Vladimirova G, Ruini C, Kapp F, Kendziora B, Ergün EZ, Bağcı IS, et al. Ex vivo confocal laser scanning microscopy: a diagnostic technique for easy real-time evaluation of benign and malignant skin tumours. J Biophotonics 2022; 15: e202100372. https://doi.org/10.1002/jbio.202100372
- Ruini C, Schuh S, Gust C, Kendziora B, Frommherz L, French LE, et al. Line-field optical coherence tomography: in vivo diagnosis of basal cell carcinoma subtypes compared with histopathology. Clin Exp Dermatol 2021; 46: 1471–1481. https://doi.org/10.1111/ced.14762
- Ruini C, Vladimirova G, Kendziora B, Salzer S, Ergun E, Sattler E, et al. Ex-vivo fluorescence confocal microscopy with digital staining for characterizing basal cell carcinoma on frozen sections: a comparison with histology. J Biophotonics 2021; 14: e202100094. https://doi.org/10.1002/jbio.202100094
- McInnes MDF, Moher D, Thombs BD, McGrath TA, Bossuyt PM, Clifford T, et al. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: The PRISMA-DTA Statement. JAMA 2018; 319: 388–396. https://doi.org/10.1001/jama.2017.19163
- Connolly SM, Baker DR, Coldiron BM, Fazio MJ, Storrs PA, Vidimos AT, et al. AAD/ACMS/ASDSA/ASMS 2012 appropriate use criteria for mohs micrographic surgery: a report of the American Academy of Dermatology, American College of Mohs Surgery, American Society for Dermatologic Surgery Association, and the American Society for Mohs Surgery. J Am Acad Dermatol 2012; 67: 531–550. https://doi.org/10.1016/j.jaad.2012.06.009
- Bittner GC, Cerci FB, Kubo EM, Tolkachjov SN. Mohs micrographic surgery: a review of indications, technique, outcomes, and considerations. An Bras Dermatol 2021; 96: 263–277. https://doi.org/10.1016/j.abd.2020.10.004
- Ziefle S, Schüle D, Breuninger H, Schippert W, Moehrle M. Confocal laser scanning microscopy vs 3-dimensional histologic imaging in basal cell carcinoma. Arch Dermatol 2010; 146: 843–847. https://doi.org/10.1001/archdermatol.2010.191
- meta SG. meta: An R package for meta-analysis. 2007; 7: 40–45.
- Doebler P. Meta-analysis of diagnostic accuracy with mada. R Packages. Preprinted posted online 2015.
- Reitsma JB, Glas AS, Rutjes AWS, Scholten RJPM, Bossuyt PM, Zwinderman AH. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J Clin Epidemiol 2005; 58: 982–990. https://doi.org/10.1016/j.jclinepi.2005.02.022
- Whiting PF, Rutjes AWS, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 2011; 155: 529–536. https://doi.org/10.7326/0003-4819-155-8-201110180-00009
- Harbord RM, Egger M, Sterne JAC. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat Med 2006; 25: 3443–3457. https://doi.org/10.1002/sim.2380
- Prasad M. Introduction to the GRADE tool for rating certainty in evidence and recommendations. Clin Epidemiol Glob Health 2024; 25: 101484. https://doi.org/10.1016/j.cegh.2023.101484
- Bennàssar A, Vilata A, Puig S, Malvehy J. Ex vivo fluorescence confocal microscopy for fast evaluation of tumour margins during Mohs surgery. Br J Dermatol 2014; 170: 360–365. https://doi.org/10.1111/bjd.12671
- Bergeret B, Masset F, Bekoy YD, Roger P, Habib F, Ovtchinnikoff B, et al. Diagnostic accuracy of digital staining ex vivo confocal microscopy for diagnosing and subtyping basal cell carcinoma in fresh pretherapeutic punch biopsies: a monocentric prospective study. Dermatology (Basel) 2022: 1–7. https://doi.org/10.1159/000524349
- Espinasse M, Cinotti E, Grivet D, Labeille B, Prade V, Douchet C, et al. “En face” ex vivo reflectance confocal microscopy to help the surgery of basal cell carcinoma of the eyelid. Clin Exp Ophthalmol 2017; 45: 442–447. https://doi.org/10.1111/ceo.12904
- Gellrich FF, Laske J, Steininger J, Eberl N, Meier F, Beissert S, et al. Ex vivo confocal microscopy speeds up surgical margin control of re-excised skin tumors and greatly shortens in-hospital stay. Cancers (Basel) 2024; 16: 3209. https://doi.org/10.3390/cancers16183209
- Grizzetti L, Kuonen F. Ex vivo confocal microscopy for surgical margin assessment: a histology-compared study on 109 specimens. Skin Health Dis 2022; 2: e91. https://doi.org/10.1002/ski2.91
- Grupp M, Illes M, Mentzel J, Simon JC, Paasch U, Grunewald S. Routine application of ex vivo confocal laser scanning microscopy with digital staining for examination of surgical margins in basal cell carcinomas. J Dtsch Dermatol Ges 2021; 19: 685–692. https://doi.org/10.1111/ddg.14374
- Hartmann D, Krammer S, Bachmann MR, Mathemeier L, Ruzicka T, von Braunmühl T. Simple 3-criteria-based ex vivo confocal diagnosis of basal cell carcinoma. J Biophotonics 2018; 11: e201800062. https://doi.org/10.1002/jbio.201800062
- Karen JK, Gareau DS, Dusza SW, Tudisco M, Rajadhyaksha M, Nehal KS. Detection of basal cell carcinomas in Mohs excisions with fluorescence confocal mosaicing microscopy. Br J Dermatol 2009; 160: 1242–1250. https://doi.org/10.1111/j.1365-2133.2009.09141.x
- Larson B, Abeytunge S, Seltzer E, Rajadhyaksha M, Nehal K. Detection of skin cancer margins in Mohs excisions with high-speed strip mosaicing confocal microscopy: a feasibility study. Br J Dermatol 2013; 169: 922–926. https://doi.org/10.1111/bjd.12444
- Longo C, Pampena R, Bombonato C, Gardini S, Piana S, Mirra M, et al. Diagnostic accuracy of ex vivo fluorescence confocal microscopy in Mohs surgery of basal cell carcinomas: a prospective study on 753 margins. Br J Dermatol 2019; 180: 1473–1480. https://doi.org/10.1111/bjd.17507
- Messner L, Deußing M, Maurer M, Buttgereit L, Stärr L, French LE, et al. Ex vivo confocal laser scanning microscopy in rare skin diseases. Cancers (Basel) 2024; 16: 1713. https://doi.org/10.3390/cancers16091713
- Mu EW, Lewin JM, Stevenson ML, Meehan SA, Carucci JA, Gareau DS. Use of digitally stained multimodal confocal mosaic images to screen for nonmelanoma skin cancer. JAMA Dermatol 2016; 152: 1335–1341. https://doi.org/10.1001/jamadermatol.2016.2997
- Peters N, Schubert M, Metzler G, Geppert JP, Moehrle M. Diagnostic accuracy of a new ex vivo confocal laser scanning microscope compared to H&E-stained paraffin slides for micrographic surgery of basal cell carcinoma. J Eur Acad Dermatol Venereol 2019; 33: 298–304. https://doi.org/10.1111/jdv.15243
- Peris K, Fargnoli MC, Kaufmann R, Arenberger P, Bastholt L, Seguin NB, et al. European consensus-based interdisciplinary guideline for diagnosis and treatment of basal cell carcinoma-update 2023. Eur J Cancer 2023; 192: 113254. https://doi.org/10.1016/j.ejca.2023.113254
- Longo C, Ragazzi M, Rajadhyaksha M, Nehal K, Bennassar A, Pellacani G, et al. In vivo and ex vivo confocal microscopy for dermatologic and mohs surgeons. Dermatol Clin 2016; 34: 497–504. https://doi.org/10.1016/j.det.2016.05.012
- Malvehy J, Pérez-Anker J, Toll A, Pigem R, Garcia A, Alos LL, et al. Ex vivo confocal microscopy: revolution in fast pathology in dermatology. Br J Dermatol 2020; 183: 1011–1025. https://doi.org/10.1111/bjd.19017
- Ragazzi M, Longo C, Piana S. Ex Vivo (Fluorescence) confocal microscopy in surgical pathology: state of the art. Adv Anat Pathol 2016; 23: 159–169. https://doi.org/10.1097/PAP.0000000000000114
- Mohs. Aust J Dermatology 2023; 64: 97–100. https://doi.org/10.1111/ajd.14046
- Kadouch DJ, Schram ME, Leeflang MM, Limpens J, Spuls PI, de Rie MA. In vivo confocal microscopy of basal cell carcinoma: a systematic review of diagnostic accuracy. J Eur Acad Dermatol Venereol 2015; 29: 1890–1897. https://doi.org/10.1111/jdv.13224
- Lupu M, Popa IM, Voiculescu VM, Caruntu A, Caruntu C. A systematic review and meta-analysis of the accuracy of in vivoreflectance confocal microscopy for the diagnosis of primary basal cell carcinoma. J Clin Med 2019; 8: 8. https://doi.org/10.3390/jcm8091462
- Perino F, Suarez R, Perez-Anker J, Carrera C, Rezze GG, Primiero CA, et al. Concordance of in vivo reflectance confocal microscopy and horizontal-sectioning histology in skin tumours. J Eur Acad Dermatol Venereol 2024; 38: 124–135. https://doi.org/10.1111/jdv.19491
- Sendín-Martín M, Lara-Caro M, Harris U, Moronta M, Rossi A, Lee E, et al. Classification of basal cell carcinoma in ex vivo confocal microscopy images from freshly excised tissues using a deep learning algorithm. J Invest Dermatol 2022; 142: 1291–1299. https://doi.org/10.1016/j.jid.2021.09.029