REVIEW ARTICLE
Atopic Dermatitis Across the Lifespan: Understanding, Measuring and Minimizing Cumulative Life Course Impairment
Matthias AUGUSTIN1*, Paolo AMERIO2, Anthony BEWLEY3, Uwe GIELER4, Jan GUTERMUTH5, Alexa B. KIMBALL6, Eric SIMPSON7 and Richard B. WARREN8
1Institute for Health Services Research in Dermatology and Nursing, University of Hamburg-Eppendorf, Hamburg, Germany, 2Clinic of Dermatology, Department of Medicine and Aging Sciences, University G. D’Annunzio, Chieti, Italy, 3Barts Health NHS Trust, Queen Mary University, London, United Kingdom, 4Vitos Clinic, Giessen, Germany, 5Department of Dermatology, Free University Brussels, University Hospital Brussels, SKIN Research Group, Brussels, Belgium, 6Harvard Medical School and Clinical Laboratory for Epidemiology and Applied Research in Skin, Department of Dermatology, Beth Israel Deaconess Medical Center, Boston, MA, United States, 7Oregon Health and Science University, Portland, OR, United States, and 8Dermatology Center, Northern Care Alliance NHS Foundation Trust & Division of Musculoskeletal and Dermatological Sciences, Manchester NIHR Biomedical Research Centre, Manchester Academic Health Science Centre, University of Manchester, Manchester, United Kingdom
Corr: Matthias AUGUSTIN, Institute for Health Services Research in Dermatology and Nursing, University of Hamburg-Eppendorf, Martinistr. 52, DE-20246 Hamburg, Germany. *Email: m.augustin@uke.de
Key words: atopic dermatitis; chronic disease; eczema; patient-reported outcomes; quality of life; symptom burden.
Citation: Acta Derm Venereol 2026; 106: adv-2025-0066. DOI: https://doi.org/10.2340/actadv.v106.adv-2025-0066.
Copyright: 2026 ©Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Oct 1, 2025. Accepted after revision: Mar 17, 2026.
Published: Jun 16, 2026.
Competing interests and funding: Medical writing support, under the direction of the authors, was provided by Ashfield MedComms, an Inizio company, and funded by Sanofi.
Not applicable
Matthias Augustin served as a consultant, lecturer, researcher, and/or received research grants from companies producing atopic dermatitis drugs, including AbbVie, Almirall, Bayer, Beiersdorf, Eli Lilly, Galderma, Incyte, La Roche-Posay, LEO Pharma, Menlo, MSD, Novartis, Pfizer, Regeneron, Sanofi-Genzyme, Trevi, Viatris. Paolo Amerio has received honoraria for speech and advisory boards from: AbbVie, Eli Lilly, Galderma, LEO Pharma, Novartis, Pfizer, Sanofi. He is a PI for interventional studies for AD sponsored by: Amgen, Almirall, Sanofi. Anthony Bewley has had ad hoc consultancy/travel/lecturing fees from: AbbVie, Almirall, Bristol Myers Squibb, Galderma, Janssen, Lilly, LEO-Pharma, Novartis, Pfizer, Sanofi, UCB. Uwe Gieler has received honoraria for speech and advisory boards from: AbbVie, Almirall, Incyte, Janssen, Novartis, Pfizer, Sanofi, UCB. He is the PI of an interventional study for AD sponsored by Beiersdorf AG Germany. Jan Gutermuth has conducted clinical trials and/or has been an advisory board member and/or speaker for: AbbVie, Almirall, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly and Company, Galderma, Genzyme, Janssen, Johnson & Johnson, LEO Pharma, Pfizer, Regeneron, Sanofi, UCB. Alexa Kimball disclosures are consulting: AbbVie, Lilly, Pfizer, Regeneron, Sanofi; board of directors: Almirall. Institution receives grants from: AbbVie, Lilly, Pfizer, Regeneron, Sanofi. Eric Simpson has received speaker and/or consulting fees from: AbbVie, Advances in Cosmetic Medical Dermatology Hawaii LLC, Amgen, AOBiome LLC, Arcutis Biotherapeutics, Arena Pharmaceuticals, Aslan Pharma, Boehringer Ingelheim USA Inc, Boston Consulting Group, Bristol Myers Squibb, Collective Acumen LLC (CA), CorEvitas, Dermira, Eli Lilly, Evelo Biosciences, Evidera, Excerpta Medica, FIDE, Forte Bio RX, Galderma, GlaxoSmithKline, Gilead Sciences Inc, Incyte, Innovaderm Research, Janssen, Johnson & Johnson, Kyowa Kirin Pharmaceutical Development, LEO Pharma, Medscape LLC, Merck, Maui Derm, MJH Holding, MLG Operating, Pfizer, Physicians World LLC, PRImE, Recludix Pharma, Regeneron, Revolutionizing Atopic Dermatitis Inc, Roivant, Sanofi-Genzyme, Trevi Therapeutics, Valeant, Vindico Medical Education, WebMD. Richard Warren has received honoraria for speech and advisory boards from: AbbVie, Almirall, Amgen, Arena, Astellas, Avillion, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, DiCE, Galderma, GSK, Immunocore, Janssen, Lilly, LEO Pharma, Meiji Pharma, Nektar Therapeutics, Novartis, Pfizer, RAPT pharmaceuticalsPharmaceuticals, Sanofi, Sun Pharma, Takeda, UCB, UNION.
Atopic dermatitis (AD) presents a multidimensional burden, often beginning in infancy and accumulating over time. Beyond itch and pain, AD is associated with significant losses of health-related quality of life resulting from sleep disturbance, stigmatization, other atopic diseases and nonatopic comorbidities, among others. These associated conditions affect patients’ physical and mental health, development, social interaction and productivity, resulting in what has been termed cumulative life course impairment (CLCI). To alter the trajectory of AD and improve patient outcomes, it is important to identify people at risk of CLCI, measure it in clinical practice and intervene with appropriate treatment. Although a digital, structured questionnaire for adults exists, a separate instrument to assess CLCI in children and adolescents would benefit our understanding of these issues in a patient population in need. This paper discusses the need for such a questionnaire, with the goal of increasing awareness of the lifelong impact of AD among healthcare professionals, caregivers and patients, potentially improving shared decision-making and facilitating conversations about treatment.
SIGNIFICANCE
Atopic dermatitis influences the course of patients’ lives through its chronic effects on sleep, mental health, development of other conditions such as asthma and social isolation. In this article, we describe cumulative life course impairment (CLCI), the concept that negative, and sometimes irreversible, effects of atopic dermatitis on a patient’s life increase the longer it is not treated appropriately. By measuring this impact and starting treatment early, we may be able to minimize harm. We propose developing a short questionnaire that can assess CLCI in paediatric patients to improve long-term outcomes.
Atopic dermatitis (AD) is a systemic inflammatory disease that creates a multidimensional burden on patients, affecting them throughout the course of their lives. Recognizing and measuring this impact is the first step in minimizing long-term negative outcomes. Life course research recognizes the complex interaction of biological, environmental and societal influences over time that affect health and development, noting the potential for accumulated risk as adverse factors can lead to other adverse factors (1, 2). Often described in the context of skin disease, cumulative life course impairment (CLCI) refers to the summed burden of a chronic condition that shapes an individual’s life course, eventually causing irreversible consequences (3, 4, 5). For example, in addition to its effects on physical health, disease severity can influence mental health and behaviour, including avoidance of social situations because of perceived stigma or embarrassment. One systematic review found an increased risk of patients with psoriasis developing lifelong consequences such as cardiovascular disease, other autoimmune diseases and psychiatric disorders (6). Outside dermatology, a life course approach identified the negative impacts of endometriosis on educational attainment, employment and productivity, social life and personal relationships (7).
Early onset of disease can lead to a greater cumulative impact that can significantly impair an individual’s potential (3). Considering that approximately 85% of first manifestations of AD occur in children (8), AD is likely to influence life course and lead to CLCI (Fig. 1). Indeed, one study found that patients with severe AD in childhood reported significantly delayed social development along with high rates of psychosocial consequences and physical discomfort (9). A correlation has also been observed between impaired health-related quality of life and current disease severity. Early intervention to change disease course is therefore important in minimizing the accrual of disease burden and reducing the CLCI associated with chronic skin diseases (10, 11, 12). In this review, we will focus on how the concept of CLCI may be applied to decision-making in the clinical care of patients with AD to improve outcomes.

Fig. 1. Cumulative life course impairment (CLCI) in patients with atopic dermatitis (AD).
TYPICAL PATIENT JOURNEY WITH AD
Burden of disease across the life course
AD is characterized by recurrent, itchy, painful skin inflammation, often beginning in infancy (8, 13). Eczematous plaques present on the face, trunk and extensor extremities in infants and on flexural surfaces in older patients (8). While some children experience improvement, severity remains the same or worsens in many children after they transition to adolescence (14). Although itch and pain are more well-known components of disease burden (15, 16, 17), overall health effects have been noted on growth, development and social connections. Patient- and caregiver-reported measures have found a negative impact of AD on quality of life in patients as young as age 6 months (13, 15, 16, 17). Greater disease severity also increases costs, both the direct financial burden of health care as well as indirect costs such as loss of productivity both in patients and employed caregivers of paediatric patients (13, 15, 18), for example, through effects on career choice and education (19).
Sleep. AD is associated with impaired sleep quality, and sleep disturbance is among the most reported and problematic symptoms both in childhood and throughout life, affecting patients, caregivers and partners (13, 16, 17, 20). Itch can drive disrupted sleep, but the relationship between sleep and inflammation may be bidirectional (21, 22). Lack of sleep and resultant biological and psychological stress may impair cognition, increase inflammatory biomarkers and lower the itch threshold (22). Sleep disturbance is also likely to influence other aspects of health, including neurocognitive processing, mood and even growth (21, 22). Although AD has not been associated with short stature overall, bone mineral density is decreased in children and adolescents with AD, and an analysis of multiple population-based studies found that a subset of children with severe disease and insufficient sleep are at increased risk of short stature in early adolescence (23, 24).
Attention-deficit/hyperactivity disorder (ADHD). An association between AD and the diagnosis of ADHD is also modified by sleep (25, 26). However, factors other than sleep disturbance are likely to mediate the impact of AD on development as well. The presence of an atopic disease increases the risk of developing ADHD by 30% to 50%, possibly because of hypersensitivity to environmental stimuli, effects of inflammatory cytokines or other pathways (27). ADHD may be misdiagnosed in children with AD as they may lack the ability to sit still due to itch and scratching. Notably, cognitive impairment associated with AD is primarily limited to children with concomitant ADHD or learning disabilities, so these patients are at highest risk (28).
Atopic comorbidities. Multiple atopic conditions are associated with AD, including asthma, rhinitis, eosinophilic oesophagitis and food allergies (29, 30). In one international survey, at least 1 atopic comorbidity was present in 92% of paediatric patients with AD (17). Longitudinal studies have shown that the presence of AD increases the likelihood of developing other atopic diseases, in a relationship referred to as the “atopic march” (31) (Fig. 2). Infants diagnosed with AD have a 2–8 fold higher risk of developing other atopic diseases over the 8 years after diagnosis than children who do not develop AD before age 1 year (32). Additionally, the severity of AD is directly correlated with the severity of the associated atopic comorbidities (33). It has been hypothesized that a dysfunctional skin barrier leads to allergic sensitization, inducing systemic type 2 immunity that predisposes patients to other atopic diseases (31). Together, these conditions contribute to limitations in daily activities and negative effects on quality of life in paediatric patients (34). Avoidance of allergens or triggers from food, sports or other activities can be limiting and decrease life satisfaction (35, 36). Indeed, the presence of multiple allergic diseases at age 4 years is significantly associated with increased risk for internalizing behaviours and anxiety at age 7 years (37).

Fig. 2. Progression of the atopic march.
Depression and anxiety. The burden of AD is high, and the development of other diseases multiplies that burden, so it is unsurprising that depression and anxiety are among the most frequently reported burdens of AD in adolescents and adults (13). Multiple studies have found associations between AD and depression, anxiety and suicidal ideation (38, 39, 40, 41). Notably, there is an age-dependent pattern for psychological comorbidities. One study in children aged 2–17 years found that while emotional and behavioural difficulties peaked during early adolescence, depression, worry and prevalence of multiple psychological comorbidities increased throughout adolescence (41). A longitudinal cohort study evaluating mental health outcomes in patients with AD aged 4–18 years found increased risk of internalizing behaviours as early as age 4 years and remaining similar across ages, while symptoms of depression increased from 6% at age 10 years (earliest age evaluated) to 22% at age 18 years (39).
Stigmatization and social isolation. Stigmatization and social isolation associated with AD are likely to play a role in these negative outcomes and affect development over time. According to one survey, children aged 6–11 years with AD were more frequently bullied compared with a control group (20% vs 9%) (42). Another survey found that 52% of children aged 12–15 years with AD had been the target of AD-related bullying (16). This age group was also most likely to report that they felt embarrassed because of AD, that AD interfered with relationships with friends or classmates, and that they self-isolated because of AD (16). Absenteeism (being absent from school or work because of the disease) and presenteeism (e.g., difficulty remaining focused and concentrated at school or while doing homework) resulted in 37.8 days of study impairment per student aged 6–11 years over the previous 12 months (42). Similarly, in students overall, 17.1 days of absenteeism and 19.5 days of presenteeism per student per year were reported (16). Again, absenteeism was more pronounced in the 12–15 year-old group.
In adults, social isolation may be evident because people with AD are less likely to be living with a partner and have higher rates of separation and divorce than are those without AD. (43).
Nonatopic comorbidities. An increased risk of nonatopic comorbidities, such as infections, autoimmune conditions, lymphoid/haematologic malignancies, ocular disorders, metabolic syndrome and obesity, has also been identified in paediatric and adult patients with AD (29, 30). In a study comparing children with AD with a non-AD reference cohort, having AD increased the likelihood of developing infections and neurological, immunological/inflammatory, endocrine/metabolic and ocular disorders over a mean follow-up of 5.7 person-years (44). The factors predisposing patients to nonatopic conditions are being investigated; for example, skin barrier defects, suppression of cutaneous innate immunity by type 2 inflammation, Staphylococcus aureus colonization and cutaneous dysbiosis contribute to increased infections in patients with AD (45). Importantly, each of these comorbidities has its own burden that is likely to worsen over time, supporting the need to treat early to avoid a cumulative burden.
Work productivity. Although developmental concerns no longer exist in adults, impacts on quality of life and health can persist and accumulate, affecting productivity. As found in paediatric patients, sleep disturbance remains a mediator of impaired overall health. AD in adults is associated with fatigue, daytime sleepiness and insomnia. However, adults with AD are more likely to report fair/poor rather than good/very good/excellent overall health, even without fatigue or sleep disturbances (46). Associations between AD and poorer health outcomes, such as higher numbers of missed workdays, days in bed and doctor visits, are only partially explained by fatigue and/or sleep disturbance (46). Depression and anxiety are also observed in a majority of adults with moderate-to-severe AD and are associated with work-related impairment and decreased health-related quality of life, leading to substantial direct and indirect costs (47). For example, one survey estimated AD-related absenteeism to be 10.9 days/year and presenteeism to be 13.1 days/year, with 67.8% of respondents having had negative professional implications in the previous year because of AD (16). Another study quantified the mean indirect costs of an incapacity to work at €589 /year (48).
Older adult health concerns. Additional health concerns may also develop in adults with AD that are not present in childhood. AD of any severity has been associated with an increased risk of type 2 diabetes, dyslipidaemia, cerebrovascular accident and deep vein thrombosis in adults (49). Another study found that adult patients newly diagnosed with AD were at a significantly increased risk of subsequently developing cardiovascular diseases, including angina pectoris, myocardial infarction, ischaemic stroke and haemorrhagic stroke within a mean follow-up period of 5 years (50). However, other large European claims database studies found no increased levels of obesity, cardiovascular risk or type 2 diabetes (51, 52).
Overall, the many components of disease burden need to be identified in practice and translated to patient needs and treatment goals. Patients with AD have been shown to have a particularly broad spectrum of treatment needs, ranging from itch relief and skin clearance to improvements in emotions, social relationships and participation, everyday life, treatment facilitation and overall disease control (53).
Potential for early intervention and disease control to minimize risk of CLCI
Because AD typically starts in early childhood and early onset is a risk factor for disease persistence and the development of AD comorbidities, the combined burden over time is likely to cause CLCI (54). Treating patients with AD early and with the most effective available therapies can impede this trajectory of increasing impairment, meet patients’ needs and avoid accumulation of risk factors and possible comorbid conditions. In effect, treatment should “flatten the curve” of accumulating CLCI over time (Fig. 3).

Fig. 3. Potential impact of early intervention on disease outcomes.
Ideally, early intervention would minimize CLCI by controlling or stopping the underlying disease. The concept of disease modification has been introduced in other chronic inflammatory diseases, such as rheumatoid arthritis and Crohn’s disease, where earlier intervention has resulted in higher remission rates (55), and has been hypothesized in other skin diseases, such as psoriasis (56). Like these diseases, moderate-to-severe AD is believed to be systemic and, recently, disease modification in AD has been discussed as a novel treatment outcome (57). It is hypothesized that epidermal barrier dysfunction allows the penetration of allergens that increase sensitivity and lead to inflammation, including the generation of type 2 helper T cells, production of allergen-specific immunoglobulin E (IgE), which can lead to food allergy and asthma, and release of cytokines and chemokines that affect other organs involved in atopic disorders (57). Therefore, influencing the natural course of AD through treatment is likely to affect overall health. Definitions of disease modification vary, referring to attenuation of disease progression, full regression or prevention of the development or progression of comorbidities (55, 57). For AD, early intervention may lead to remission, reduced disease severity and/or reduced risk of comorbidities. Some early intervention trials targeting the skin barrier to prevent the atopic march have found that proactive use of topical steroids in patients with AD reduced later incidence of food allergy or aeroallergen IgE sensitization (55).
However, patients receiving topical treatment alone, especially those with severe AD, report low effectiveness and overall satisfaction (58, 59). In a multinational study, 27.6% of adult patients and 12.9% of adolescents reported inadequately controlled disease (60). Systemic treatment options may be underused (61) and even patients on systemic corticosteroids and older nonsteroidal systemic immunosuppressants, such as cyclosporine, can experience treatment failure (62). Newer systemic agents may be better suited to influence AD disease course and reduce the development of comorbidities and CLCI. For example, one cohort study of paediatric patients with AD found that treatment with dupilumab, a human monoclonal antibody that inhibits interleukin (IL)-4 and IL-13 signalling, resulted in a significantly lower incidence of asthma and allergic rhinitis after 3 years than treatment with conventional systemic therapies. The greatest reductions occurred in the youngest age group (63). Similarly, a cohort study in adults found that dupilumab treatment was associated with statistically significant improvements on all patient-reported outcomes, including disease control, flares, skin symptoms and treatment satisfaction (64). Importantly, patients also reported improved sleep and health-related quality of life and reduced work and activity impairment, suggesting the positive impact of treatment on multiple aspects of life.
UNMET NEED FOR TOOLS TO ASSESS CLCI IN CLINICAL PRACTICE
To minimize CLCI, the impact of AD on patients’ life courses needs to be assessed to identify when intervention is needed. Incorporation of CLCI measurement in routine clinical practice may advance understanding of the long-term impact of untreated or undertreated AD and help identify the type and timing of interventions that would best reduce CLCI. To do so, it is necessary to develop tools to evaluate both existing CLCI and patients at risk, and to assess the predictive value of CLCI for disease outcomes.
Criteria and characteristics for CLCI tools
The only available CLCI instruments for chronic skin diseases, including AD, are 2 questionnaires (Fig. 4) that have recently been developed for adults that focus on quality of life, psychosocial impacts and comorbidities. The DermCLCI-r is a retrospective tool for assessing CLCI and the DermCLCI-p is a predictive tool that assesses current CLCI status and future risk (65). Patients are asked to rate how burdensome they find various disease-related problems, such as feeling stressed by their disease or negative financial impacts. While the DermCLCI-r asks respondents to rate each item since the onset of the first symptoms of the disease and to state whether each problem is ongoing or has been life changing, the DermCLCI-p asks for rating of the past 2 weeks. The print version of these tools has been validated, but the electronic version has not. It may be used in clinical practice using electronic documentation. More education about the CLCI concept is likely to accelerate their adoption.

Fig. 4. Existing CLCI questionnaires for skin diseases.
One study using these questionnaires determined that CLCI-p has good internal consistency with the Patient-Oriented Eczema Measure (POEM) and the Dermatology Life Quality Index (DLQI), and both tools had excellent reliability, with Cronbach’s alpha scores of >0.96 (66).
Importantly, these available measures have not been adapted for use in paediatric patients. An ideal CLCI measure would be a digital, brief, structured questionnaire that is validated to address age-specific considerations. Both predictive and retrospective measures would be valuable, but predictive ones are needed more in practice for measures to avoid CLCI. A new CLCI tool is likely to have broader clinical adoption if it is in a familiar format that integrates into electronic health records and augments existing scoring systems with CLCI-specific questions. For example, established metrics like the DLQI (67), Eczema Area and Severity Index (EASI) (68), or POEM (69) may be used as foundational elements that are combined with items that capture cumulative life impacts. Actionable outputs, such as a treat-to-target approach if defined thresholds for CLCI and severity measures are crossed, would help with usability.
Given that important life events change over time, independent tools for paediatric and adult patients are needed. Questions related to educational or social impairment could provide valuable information about paediatric patients, while indicators of employment or relationship stability may be more relevant for adult patients. Family impact metrics and proxy instruments would also be important for paediatric patients because young children cannot fully articulate their experiences and parents and caregivers often have secondary burdens, including sleep disruption, additional caregiving tasks and emotional distress (42).
The different components affecting CLCI can interact to make an individual vulnerable to life course impairment (3, 6). While disease severity, chronic course, early onset and comorbidities are among the more easily assessed factors that place patients at risk, clinicians also need to recognize and evaluate more complex factors, such as each patient’s perception of stigmatization, level of social support, personality traits, coping strategies and behaviours that affect health (70). Validated screening tools to measure anxiety and depression, health-related quality of life, social support and coping behaviours have been developed and can be used as a starting point (70).
Notably, the impact of CLCI on patient outcomes is intertwined with cultural and societal expectations, and personal definitions of success or impairment can vary significantly. These differences require sensitivity to each patient’s life context. Rather than imposing standard outcomes, a CLCI measure should be framed in a positive, patient-centred way to accommodate individual life paths, personal aspirations and potential, reducing stigma and fostering engagement with quality-of-life improvement strategies. Therefore, language that could be perceived as negative or limiting should be avoided. For example, a question on the degree of physical limitations would be reworded to ask about the degree of physical capabilities.
Ideally, this tool would help with shared decision-making by empowering the patient and facilitating treatment conversations. The most useful information may be collected if patients can complete the measure at home, which would streamline clinical workflows and provide more accurate responses, as patients have more time to reflect when outside the clinical setting. Given that both patients and providers are often hesitant to escalate treatment, even when warranted (71), the measure could show everyone involved when a patient may face significant risks if more effective therapy is not initiated, helping to overcome reluctance and leading to better outcomes.
Next steps for integrating CLCI metrics into clinical practice
Once a CLCI assessment tool has been developed, additional steps will be needed prior to implementation (Fig. 5). The critical first steps for integrating CLCI metrics are for healthcare professionals to appreciate the concept of CLCI and understand that they can intervene to minimize it.
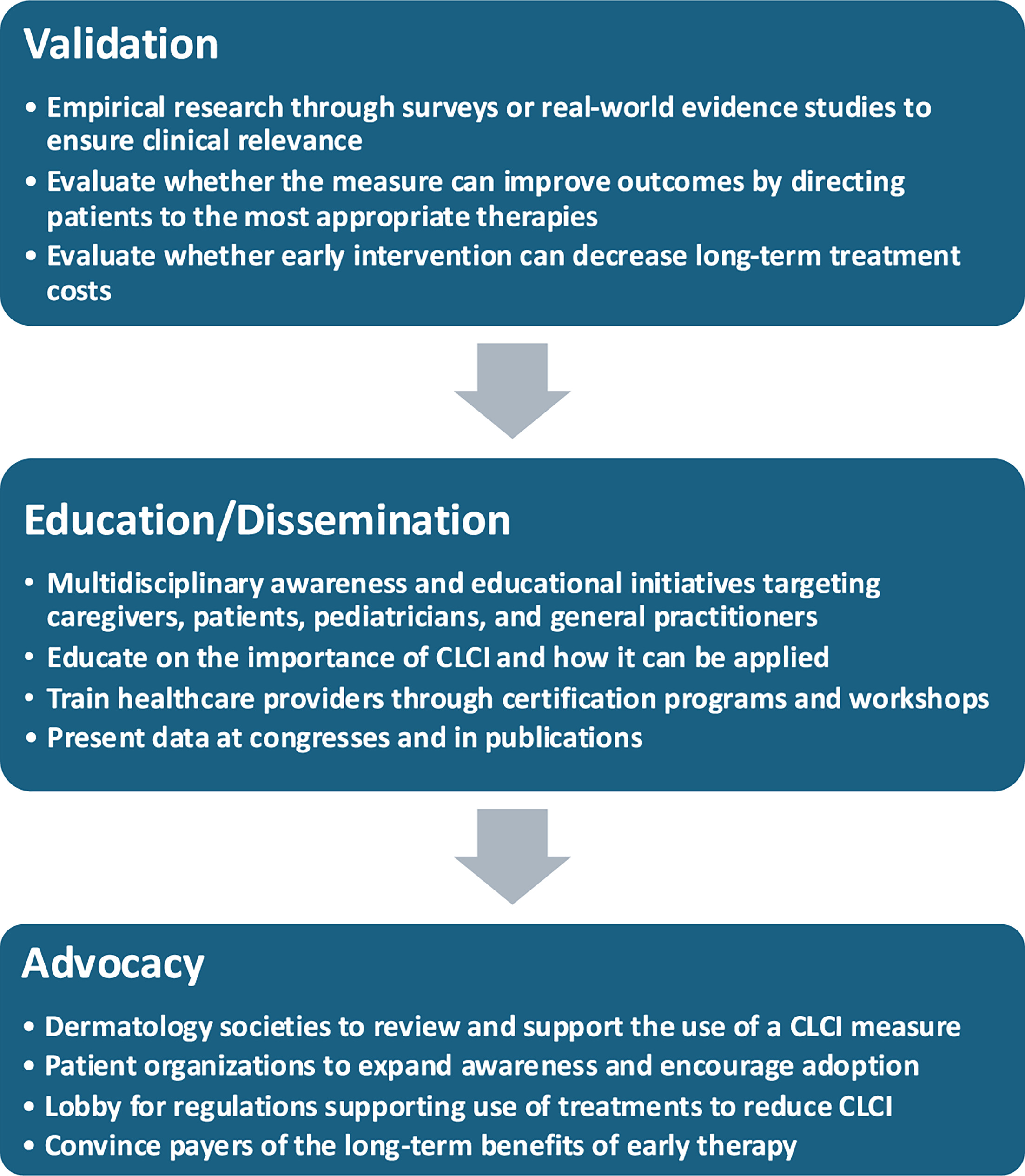
Fig. 5. Implementing cumulative life course impairment (CLCI) metrics in clinical practice.
Empirical research will be needed to validate the tool’s relevance and positive impact on outcomes. The development framework will be based on the current evidence for child developmental research in AD and follow the COSMIN criteria (COnsensus-based Standards for the selection of health Measurement INstruments). Validation will require a multinational, multilanguage development and validation study. Multiple specialties and professions will be included, and patient and parent involvement will be a special focus.
Additionally, robust training resources will be needed to support dermatologists and other practitioners in applying CLCI as part of routine care. Moreover, methods to facilitate the implementation of these tools are needed to minimize their impact on outpatient visits (e.g., length of visit, reducing patient-doctor interactions). Public awareness initiatives to introduce the concept of CLCI in an accessible way could also increase recognition and empower patients to understand and address their own life course impacts. Finally, advocacy by dermatologic societies and patient organizations could be instrumental in expanding awareness and encouraging further adoption.
CONCLUSION
The concept of CLCI is particularly relevant to patients with AD, who are often diagnosed in infancy or childhood and have symptoms and comorbidities that affect overall health, growth and development. Routine assessment of CLCI would help to identify opportunities when intervention could minimize or prevent impairment. Development of a validated CLCI measure for paediatric and adult patients, and collaboration between dermatologists, paediatricians, primary care providers, patients and advocacy groups is needed to improve awareness of CLCI, lessen the overall negative impacts of AD and increase the quality of life and well-being of patients and the people important to them.
REFERENCES
- Darnton-Hill I, Nishida C, James WPT. A life course approach to diet, nutrition and the prevention of chronic diseases. Public Health Nutr 2004; 7: 101–121. https://doi.org/10.1079/phn2003584
- Hanson HA, Leiser CL, Bandoli G, Pollock BH, Karagas MR, Armstrong D, et al. Charting the life course: emerging opportunities to advance scientific approaches using life course research. J Clin Transl Sci 2020; 5: e9. https://doi.org/10.1017/cts.2020.492
- Kimball AB, Gieler U, Linder D, Sampogna F, Warren RB, Augustin M. Psoriasis: is the impairment to a patient’s life cumulative? J Eur Acad Dermatol Venereol 2010; 24: 989–1004. https://doi.org/10.1111/j.1468-3083.2010.03705.x
- Linder MD, Piaserico S, Augustin M, Fortina AB, Cohen AD, Gieler U, et al. Psoriasis - the life course approach. Acta Derm Venereol 2016; 96: 102–108. https://doi.org/10.2340/00015555-2430
- Doroudian Tehrani M, Gibson RS, Snyder CL, Porter ML, Kimball AB. Cumulative life course impairment: evidence for hidradenitis suppurativa. J Eur Acad Dermatol Venereol 2025; 39: 1395–1409. https://doi.org/10.1111/jdv.20607
- von Stülpnagel CC, Augustin M, Düpmann L, da Silva N, Sommer R. Mapping risk factors for cumulative life course impairment in patients with chronic skin diseases – a systematic review. J Eur Acad Dermatol Venereol 2021; 35: 2166–2184. https://doi.org/10.1111/jdv.17348
- Missmer SA, Tu FF, Agarwal SK, Chapron C, Soliman AM, Chiuve S, et al. Impact of endometriosis on life-course potential: a narrative review. Int J Gen Med 2021; 14: 9–25. https://doi.org/10.2147/IJGM.S261139
- Silverberg NB, Durán-McKinster C. Special considerations for therapy of pediatric atopic dermatitis. Dermatol Clin 2017; 35: 351–363. https://doi.org/10.1016/j.det.2017.02.008
- Brenninkmeijer EEA, Legierse CM, Sillevis Smitt JH, Last BF, Grootenhuis MA, Bos JD. The course of life of patients with childhood atopic dermatitis. Pediatr Dermatol 2009; 26: 14–22. https://doi.org/10.1111/j.1525-1470.2008.00745.x
- Arancio LMH, D’Amico D, Dastoli S, Fiorella CS, Manfredini M, Moretta G, et al. Early intervention and cumulative life course impairment in psoriasis: a review. Clin Exp Dermatol 2024; 49: 1525–1531. https://doi.org/10.1093/ced/llae282
- Felix PAO, Sampaio AL, Silva BL, Viana ALP. Early intervention in psoriasis: Where do we go from here? Front Med 2022; 9: 1027347. https://doi.org/10.3389/fmed.2022.1027347
- Romiti R, Magalhães RF, Duarte GV. Cumulative life course impairment in patients with dermatological diseases, with a focus on psoriasis. An Bras Dermatol 2024; 99: 269–276. https://doi.org/10.1016/j.abd.2023.08.006
- Fasseeh AN, Elezbawy B, Korra N, Tannira M, Dalle H, Aderian S, et al. Burden of atopic dermatitis in adults and adolescents: a systematic literature review. Dermatol Ther (Heidelb) 2022; 12: 2653–2668. https://doi.org/10.1007/s13555-022-00819-6
- Hon KL, Tsang YCK, Poon TCW, Pong NH, Kwan M, Lau S, et al. Predicting eczema severity beyond childhood. World J Pediatr 2016; 12: 44–48. https://doi.org/10.1007/s12519-015-0064-9
- Achten R, Van der Rijst L, Piena M, Lamers H, De Beer F, De Bruin-Weller M, et al. Economic and humanistic burden in paediatric patients with atopic dermatitis. Acta Derm Venereol 2023; 103: adv00881. https://doi.org/10.2340/actadv.v103.4842
- Stingeni L, Belloni Fortina A, Baiardini I, Hansel K, Moretti D, Cipriani F. Atopic dermatitis and patient perspectives: insights of bullying at school and career discrimination at work. J Asthma Allergy 2021; 14: 919–928. https://doi.org/10.2147/JAA.S317009
- Weidinger S, Simpson EL, Silverberg JI, Barbarot S, Eckert L, Mina-Osorio P, et al. Burden of atopic dermatitis in paediatric patients: an international cross-sectional study. Br J Dermatol 2024; 190: 846–857. https://doi.org/10.1093/bjd/ljad449
- Augustin M, Misery L, von Kobyletzski L, Mealing S, Redding M, Chuang CC, et al. Systematic literature review assessing the overall costs and societal impacts of moderate‐to‐severe atopic dermatitis in Europe. J Eur Acad Dermatol Venereol 2022; 36: 2316–2324. https://doi.org/10.1111/jdv.18481
- Chung J, Simpson EL. The socioeconomics of atopic dermatitis. Ann Allergy Asthma Immunol 2019; 122: 360–366. https://doi.org/10.1016/j.anai.2018.12.017
- Ramirez FD, Chen S, Langan SM, Prather AA, McCulloch CE, Kidd SA, et al. Association of atopic dermatitis with sleep quality in children. JAMA Pediatr 2019; 173: e190025. https://doi.org/10.1001/jamapediatrics.2019.0025
- Chang YS, Chiang BL. Sleep disorders and atopic dermatitis: A 2-way street? J Allergy Clin Immunol 2018; 142: 1033–1040. https://doi.org/10.1016/j.jaci.2018.08.005
- Cameron S, Donnelly A, Broderick C, Arichi T, Bartsch U, Dazzan P, et al. Mind and skin: exploring the links between inflammation, sleep disturbance and neurocognitive function in patients with atopic dermatitis. Allergy 2024; 79: 26–36. https://doi.org/10.1111/all.15818
- Silverberg JI, Paller AS. Association between eczema and stature in 9 US population-based studies. JAMA Dermatol 2015; 151: 401–409. https://doi.org/10.1001/jamadermatol.2014.3432
- Wu D, Wu XD, Zhou X, Huang W, Luo C, Liu Y. Bone mineral density, osteopenia, osteoporosis, and fracture risk in patients with atopic dermatitis: a systematic review and meta-analysis. Ann Transl Med 2021; 9: 40. https://doi.org/10.21037/atm-20-4708
- Romanos M, Gerlach M, Warnke A, Schmitt J. Association of attention-deficit/hyperactivity disorder and atopic eczema modified by sleep disturbance in a large population-based sample. J Epidemiol Community Health 2010; 64: 269–273. https://doi.org/10.1136/jech.2009.093534
- Yaghmaie P, Koudelka CW, Simpson EL. Mental health comorbidity in patients with atopic dermatitis. J Allergy Clin Immunol 2013; 131: 428–433. https://doi.org/10.1016/j.jaci.2012.10.041
- Schans J van der, Çiçek R, de Vries TW, Hak E, Hoekstra PJ. Association of atopic diseases and attention-deficit/hyperactivity disorder: a systematic review and meta-analyses. Neurosci Biobehav Rev 2017; 74: 139–148. https://doi.org/10.1016/j.neubiorev.2017.01.011
- Ma EZ, Chang HR, Radtke S, Wan J. Symptoms of cognitive impairment among children with atopic dermatitis. JAMA Dermatol 2024; 160: 447–452. https://doi.org/10.1001/jamadermatol.2024.0015
- Huang AH, Roh YS, Sutaria N, Choi J, Williams KA, Canner JK, et al. Real-world comorbidities of atopic dermatitis in the pediatric ambulatory population in the United States. J Am Acad Dermatol 2021; 85: 893–900. https://doi.org/10.1016/j.jaad.2021.03.016
- Thyssen JP, Halling AS, Schmid-Grendelmeier P, Guttman-Yassky E, Silverberg JI. Comorbidities of atopic dermatitis-what does the evidence say? J Allergy Clin Immunol 2023; 151: 1155–1162. https://doi.org/10.1016/j.jaci.2022.12.002
- Bantz SK, Zhu Z, Zheng T. The atopic march: progression from atopic dermatitis to allergic rhinitis and asthma. J Clin Cell Immunol 2014; 5: 202. https://doi.org/10.4172/2155-9899.1000202
- Choi UE, Deng J, Parthasarathy V, Liao V, D’Amiano A, Taylor M, et al. Risk factors and temporal associations of progression of the atopic march in children with early-onset atopic dermatitis. J Am Acad Dermatol 2025; 92: 732–740. https://doi.org/10.1016/j.jaad.2024.10.107
- Silverberg JI, Simpson EL. Association between severe eczema in children and multiple comorbid conditions and increased healthcare utilization. Pediatr Allergy Immunol 2013; 24: 476–486. https://doi.org/10.1111/pai.12095
- Dierick BJH, van der Molen T, Flokstra-de Blok BMJ, Muraro A, Postma MJ, Kocks JWH, et al. Burden and socioeconomics of asthma, allergic rhinitis, atopic dermatitis and food allergy. Expert Rev Pharmacoecon Outcomes Res 2020; 20: 437–453. https://doi.org/10.1080/14737167.2020.1819793
- Haanpää L, Af Ursin P, Nermes M, Kaljonen A, Isolauri E. Association of allergic diseases with children’s life satisfaction: population-based study in Finland. BMJ Open 2018; 8: e019281. https://doi.org/10.1136/bmjopen-2017-019281
- Valero-Moreno S, Torres-Llanos R, Pérez-Marín M. Impact of childhood food allergy on quality of life: a systematic review. Appl Sci 2024; 14: 10989. https://doi.org/10.3390/app142310989
- Nanda MK, LeMasters GK, Levin L, Rothenberg ME, Assa’ad AH, Newman N, et al. Allergic diseases and internalizing behaviors in early childhood. Pediatrics 2016; 137: e20151922. https://doi.org/10.1542/peds.2015-1922
- Rønnstad ATM, Halling-Overgaard AS, Hamann CR, Skov L, Egeberg A, Thyssen JP. Association of atopic dermatitis with depression, anxiety, and suicidal ideation in children and adults: a systematic review and meta-analysis. J Am Acad Dermatol 2018; 79: 448–456. https://doi.org/10.1016/j.jaad.2018.03.017
- Kern C, Wan J, LeWinn KZ, Ramirez FD, Lee Y, McCulloch CE, et al. Association of atopic dermatitis and mental health outcomes across childhood: a longitudinal cohort study. JAMA Dermatol 2021; 157: 1200–1208. https://doi.org/10.1001/jamadermatol.2021.2657
- Johnson JK, Loiselle A, Chatrath S, Smith Begolka W. Patient and caregiver perspectives on the relationship between atopic dermatitis symptoms and mental health. Dermatitis 2024; 35: 386–391. https://doi.org/10.1089/derm.2023.0365
- Hou A, Silverberg JI. Predictors and age-dependent pattern of psychologic problems in childhood atopic dermatitis. Pediatr Dermatol 2021; 38: 606–612. https://doi.org/10.1111/pde.14588
- Neri I, Galli E, Baiardini I, Picozza M, Rossi AB, Matruglio P, et al. Implications of atopic dermatitis on the quality of life of 6–11-year-old children and caregivers (PEDI-BURDEN). J Asthma Allergy 2023; 16: 383–396. https://doi.org/10.2147/JAA.S404350
- Hua T, Silverberg JI. Atopic dermatitis in US adults: epidemiology, association with marital status, and atopy. Ann Allergy Asthma Immunol 2018; 121: 622–624. https://doi.org/10.1016/j.anai.2018.07.019
- von Kobyletzki L, Henrohn D, Ballardini N, Neary MP, Ortsäter G, Rieem Dun A, et al. Comorbidities in childhood atopic dermatitis: a population‐based study. J Eur Acad Dermatol Venereol 2024; 38: 354–364. https://doi.org/10.1111/jdv.19569
- Wang V, Boguniewicz J, Boguniewicz M, Ong PY. The infectious complications of atopic dermatitis. Ann Allergy Asthma Immunol 2021; 126: 3–12. https://doi.org/10.1016/j.anai.2020.08.002
- Silverberg JI, Garg NK, Paller AS, Fishbein AB, Zee PC. Sleep disturbances in adults with eczema are associated with impaired overall health: a US population-based study. J Invest Dermatol 2015; 135: 56–66. https://doi.org/10.1038/jid.2014.325
- Girolomoni G, Luger T, Nosbaum A, Gruben D, Romero W, Llamado LJ, et al. The economic and psychosocial comorbidity burden among adults with moderate-to-severe atopic dermatitis in Europe: analysis of a cross-sectional survey. Dermatol Ther 2021; 11: 117–130. https://doi.org/10.1007/s13555-020-00459-8
- Mohr N, Augustin M, Zeervi L, Bieber T, Werfel T, Wollenberg A, et al. Determinants of costs and benefits in atopic dermatitis routine care in Germany. J Eur Acad Dermatol Venereol 2022; 36: 1450–1455. https://doi.org/10.1111/jdv.18169
- Wan J, Fuxench ZCC, Wang S, Syed MN, Shin DB, Abuabara K, et al. Incidence of cardiovascular disease and venous thromboembolism in patients with atopic dermatitis. J Allergy Clin Immunol Pract 2023; 11: 3123–3132. https://doi.org/10.1016/j.jaip.2023.08.007
- Lee SW, Kim H, Byun Y, Baek YS, Choi CU, Kim JH, et al. Incidence of cardiovascular disease after atopic dermatitis development: a nationwide, population-based study. Allergy Asthma Immunol Res 2023; 15: 231–245. https://doi.org/10.4168/aair.2023.15.2.231
- Augustin M, Radtke MA, Glaeske G, Reich K, Christophers E, Schaefer I, et al. Epidemiology and comorbidity in children with psoriasis and atopic eczema. Dermatology 2015; 231: 35–40. https://doi.org/10.1159/000381913
- Ascott A, Mansfield KE, Schonmann Y, Mulick A, Abuabara K, Roberts A, et al. Atopic eczema and obesity: a population-based study. Br J Dermatol 2021; 184: 871–879. https://doi.org/10.1111/bjd.19597
- Augustin M, Langenbruch A, Blome C, Gutknecht M, Werfel T, Ständer S, et al. Characterizing treatment‐related patient needs in atopic eczema: insights for personalized goal orientation. Acad Dermatol Venereol 2020; 34: 142–152. https://doi.org/10.1111/jdv.15919
- Irvine AD, Mina-Osorio P. Disease trajectories in childhood atopic dermatitis: an update and practitioner’s guide. Br J Dermatol 2019; 181: 895–906. https://doi.org/10.1111/bjd.17766
- Jacobson ME, Seshadri RS, Morimoto R, Grinich E, Haag C, Nguyen K, et al. Early intervention and disease modification in atopic dermatitis-the current state of the field and barriers to progress. J Eur Acad Dermatol Venereol 2024; 38: 665–672. https://doi.org/10.1111/jdv.19699
- Ranzinger D, Eyerich K. Disease modification in psoriasis: future prospects for long-term remission. Am J Clin Dermatol 2025; 26: 477–486. https://doi.org/10.1007/s40257-025-00949-5
- Bieber T. Disease modification in inflammatory skin disorders: opportunities and challenges. Nat Rev Drug Discov 2023; 22: 662–680. https://doi.org/10.1038/s41573-023-00735-0
- Bacci ED, Correll JR, Pierce EJ, Atwater AR, Dawson Z, Begolka WS, et al. Burden of adult atopic dermatitis and unmet needs with existing therapies. J Dermatolog Treat 2023; 34: 2202288. https://doi.org/10.1080/09546634.2023.2202288
- Paller AS, Guttman-Yassky E, Schuttelaar MLA, Irvine AD, Baselga E, Kataoka Y, et al. Disease characteristics, comorbidities, treatment patterns and quality of life impact in children <12 years old with atopic dermatitis: interim results from the PEDISTAD Real-World Registry. J Am Acad Dermatol 2022; 87: 1104–1108. https://doi.org/10.1016/j.jaad.2022.01.018
- Eyerich K, Gooderham MJ, Silvestre JF, Shumack SP, Mendes-Bastos P, Aoki V, et al. Real-world clinical, psychosocial and economic burden of atopic dermatitis: results from a multicountry study. J Eur Acad Dermatol Venereol 2024; 38: 340–353. https://doi.org/10.1111/jdv.19500
- Kleyn CE, Barbarot S, Reed C, Losi S, von Arx LB, Robert C, et al. Burden of moderate to severe atopic dermatitis in adults from France, Italy, and the UK: patient-reported outcomes and treatment patterns. Dermatol Ther 2022; 12: 1947–1965. https://doi.org/10.1007/s13555-022-00777-z
- Calzavara-Pinton P, Čelakovská J, Lapeere H, Holzer G, Al-Ahmad M, Chu CY, et al. Baseline demographics, comorbidities, treatment patterns and burden of atopic dermatitis in adults and adolescents from the GLOBOSTAD long-term observational study. Adv Ther 2023; 40: 5366–5382. https://doi.org/10.1007/s12325-023-02644-5
- Lin TL, Fan YH, Fan KS, Juan CK, Chen YJ, Wu CY. Reduced atopic march risk in pediatric atopic dermatitis patients prescribed dupilumab versus conventional immunomodulatory therapy: a population-based cohort study. J Am Acad Dermatol 2024; 91: 466–473. https://doi.org/10.1016/j.jaad.2024.05.029
- Strober B, Mallya UG, Yang M, Ganguli S, Gadkari A, Wang J, et al. Treatment outcomes associated with dupilumab use in patients with atopic dermatitis: 1-year results from the RELIEVE-AD study. JAMA Dermatol 2022; 158: 142–150. https://doi.org/10.1001/jamadermatol.2021.4778
- Braren-von Stülpnagel CC, Augustin M, Westphal L, Sommer R. Development of measurement tools to assess cumulative life course impairment in patients with chronic skin diseases. J Eur Acad Dermatol Venereol 2023; 37: 1626–1633. https://doi.org/10.1111/jdv.18977
- Ho MJ, Sultana R, Choo K, Lee HY. Cumulative life course impairment in moderate-to-severe atopic dermatitis: a cross-sectional study in Singapore. Dermatology 2025; 241: 425–436. https://doi.org/10.1159/000548368
- Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol 1994; 19: 210–216. https://doi.org/10.1111/j.1365-2230.1994.tb01167.x
- Hanifin JM, Baghoomian W, Grinich E, Leshem YA, Jacobson M, Simpson EL. The Eczema Area and Severity Index—a practical guide. Dermatitis 2022; 33: 187–192. https://doi.org/10.1097/DER.0000000000000895
- Charman CR, Venn AJ, Williams HC. The patient-oriented eczema measure: development and initial validation of a new tool for measuring atopic eczema severity from the patients’ perspective. Arch Dermatol 2004; 140: 1513–1519. https://doi.org/10.1001/archderm.140.12.1513
- Augustin M. Cumulative life course impairment: identifying patients at risk. Curr Probl Dermatol 2013; 44: 74–81. https://doi.org/10.1159/000350555
- Heratizadeh A, Mempel M, von Kiedrowski R, Hagl S, Mosch T, Fritz B, et al. Checklist identification of candidates for systemic therapy in adult patients with atopic dermatitis in Germany: a multicentre study. J Eur Acad Dermatol Venereol 2024; 38: 157–166. https://doi.org/10.1111/jdv.19465