ORIGINAL REPORT
Dermatologists’ Attitudes toward Ultrasound-guided One-step Excision for Cutaneous Melanoma: A Survey of Clinical Practice and Perceived Barriers
Alanood ALMERAISEL1*, Youssef MOURTADA1, Audrey BISSON-PATOUE2, Chrystelle QUEIROS2, Alice FAYAD3, Nina SIGG3, Adeline PERRINAUD4 and Laurent MACHET1,5*![]()
1Dermatology Department, Centre Hospitalier Régional Universitaire, Tours, France, 2Plastic and Facial Surgery Department, Centre Hospitalier Régional Universitaire, Tours, France, 3Dermatology Department, Centre Hospitalier Universitaire, Angers, France, 4Private Dermatology Practice, 6 rue Thérèse et René Planiol, 37540 Saint-Cyr-sur-Loire, France, and 5UMR INSERM U1253, Université de Tours, Tours, France
Corr: Alanood Almeraisel, Department of Dermatology, Centre Hospitalier Régional Universitaire, Tours, France and Laurent Machet, Department of Dermatology, Centre Hospitalier Régional Universitaire, Tours, France. *Emails: alanood.almeraisel@gmail.com; machet@univ-tours.fr
Key words: cutaneous melanoma; one-step surgery; ultrasound imaging; Breslow thickness; wide local excision; patient preference; dermatology.
Citation: Acta Derm Venereol 2026; 106: adv-2026-0494. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0494.
Copyright: © The Authors 2026. Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 13, 2026. Accepted after revision: Jun 2, 2026.
Published: Jun 22, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
The study consisted of an anonymous survey of physicians and did not involve patient data. According to national regulations, formal ethics committee approval was not required.
Wide local excision of primary cutaneous melanoma is usually performed in 2 stages: diagnostic excision followed by definitive surgery with margins based on histopathological Breslow thickness. High-frequency ultrasound may enable reasonably accurate preoperative thickness estimation and may allow a single-stage approach. However, its adoption in routine practice remains limited. This study evaluated dermatologists’ acceptance of ultrasound-guided 1-step melanoma surgery and explored barriers to its implementation. An electronic survey including 9 clinical vignettes with dermoscopy images and preoperative ultrasound measurements was sent to dermatologists in the Loire Valley, France. Participants selected preferred management strategies, rated ultrasound utility and patient preference on Likert scales, and provided open-ended responses about perceived obstacles. Fifty-three dermatologists completed the questionnaire (57% response rate). One-step surgery was selected in 28% of scenarios, increasing to 47% when diagnosis was confirmed by biopsy and decreasing to 24.5% without histopathological confirmation (p<0.0001). Most respondents acknowledged ultrasound’s usefulness for thickness estimation (median Likert score 3 [IQR 3–4]) and believed patients would prefer a single procedure (median 4 [IQR 3–5]). Major barriers included limited access to high-resolution ultrasound (n=18), concerns regarding overtreatment (n=14) and medico-legal risk in the absence of histopathological confirmation (n=9). Dermatologists remain cautious about 1-step melanoma surgery, primarily due to diagnostic uncertainty and resource limitations.
SIGNIFICANCE
This study looks at how dermatologists feel about removing a skin tumour in one procedure using ultrasound to measure its thickness before surgery. Doing it in one step could save time, reduce stress and make care easier for patients. By understanding dermatologists’ perspectives and the challenges they face, we can help make this approach more widely used, improving treatment efficiency and patient experience.
Melanoma accounts for the highest number of deaths among skin cancers. Current guidelines recommend a 2-step approach: an initial diagnostic excision with narrow margins of 1–3 mm is performed, followed by a wider local excision after confirming the melanoma diagnosis and measuring the Breslow thickness through histopathological examination. According to the French Society of Dermatology (1), recommended surgical margins for wide local excision are 5 mm for melanoma in situ, 1–2 cm for invasive melanoma with Breslow thickness >1 mm or melanoma in situ located on the face, and 2 cm for melanoma with Breslow thickness >2 mm. Updated European guidelines published in 2024 are relatively similar: 5 mm margins for melanoma in situ, 1 cm for tumours with thickness ≤2 mm and 2 cm margins for thickness >2 mm (2).
Advances in high-frequency ultrasound now allow noninvasive measurement of melanoma thickness before surgery. Many studies, including meta-analyses, have demonstrated a strong correlation between ultrasound measurements and histopathological Breslow thickness (3, 4, 5, 6). This has enabled the development of a 1-step surgical approach in which excision margins are determined based on preoperative ultrasound assessment (7). In addition, qualitative research suggests that patients often prefer a single-stage procedure rather than 2 separate operations (8). However, this strategy has not yet been widely adopted in routine clinical practice.
The aim of this study was to evaluate dermatologists’ perspectives in the French Loire Valley regarding the feasibility and acceptability of performing wide excision of melanoma in a single procedure, based on clinical assessment, occasionally supported by punch biopsy and preoperative ultrasound evaluation. We also sought to identify perceived barriers in order to better understand the factors that may limit its adoption in routine clinical practice.
METHODS
Study design
From March to June 2025, we conducted a survey of dermatologists in the French Loire Valley to investigate their perceptions, potential advantages and risks associated with a 1-step surgical strategy guided by ultrasound measurement of tumour thickness.
A questionnaire was initially developed by 2 dermatologists: a dermatology trainee (AA) and an experienced practitioner in cutaneous ultrasonography and melanoma management (LM). It was then discussed during an audio-recorded meeting lasting 75 min with 4 private dermatologists. Their comments were taken into account, and a final version of the questionnaire was validated during a staff meeting. The questionnaire consisted of 9 short clinical cases showing pigmented cutaneous lesions, including dermoscopy pictures and the maximum depth of the lesion measured with high-resolution ultrasound (annex 1). Two probes operating at 20 and 50 MHz were used (Dermcup 2020, Atys Médical, Soucieu-en-Jarrest, France). The pictures were collected from patients participating in previous studies in our centre (7, 8).
Dermatologists were asked to choose among 5 or 6 management options for each vignette. These included clinical surveillance, partial incisional biopsy, diagnostic excision without predetermined wide margins (i.e. narrow excision intended for histopathological diagnosis), delayed diagnostic excision, followed by wider excision according to histopathological Breslow thickness, immediate 1-step wide excision or delayed 1-step wide excision guided by the maximal thickness measured using ultrasound. Participants were also invited to answer 4 questions using a 5-point Likert scale evaluating their perception of ultrasound in initial management of primary cutaneous melanoma. Finally, respondents were invited to express in plain language the foreseen difficulties of the 1-step approach using 2 open questions.
What are the main obstacles you see to performing wide excision surgery without prior histopathological confirmation?
What obstacles do you see in offering the patient the choice between a classic 2-stage surgery or an “innovative” 1-step wide excision with margins guided by ultrasound thickness?
The questionnaire, clinical vignettes, and detailed response categories are provided in the Supplementary Material.
Setting and participants
Dermatologists belonging to the Fédération Française de Formation Continue et d’Evaluation en Dermatologie-Vénéréologie (French Federation for Continuing Medical Education) and working in the Loire Valley at Tours (ADERMCO, 50 dermatologists) and Angers (AIDA, 43 dermatologists) received an email inviting them to complete an online questionnaire. A reminder was sent 3 months later. The survey targeted all dermatologists registered in the 2 regional dermatology networks in the Loire Valley.
Data analysis
Descriptive analyses of participant characteristics and questionnaire responses were performed using Microsoft Excel (Microsoft Corp, Redmond, WA, USA). Categorical variables were summarized as frequencies and percentages, while continuous variables were reported as medians with interquartile ranges (IQR). Comparisons between groups were performed using contingency tables and Fisher’s exact test when appropriate. Statistical significance was defined as p<0.05. Responses to open-ended questions were categorized thematically and summarized according to the frequency of recurring themes.
RESULTS
Among the 93 dermatologists invited to participate, 53 completed the questionnaire (34 after the initial solicitation and 19 after a reminder was sent), yielding a response rate of 57%. Participants’ median age was 40 years (IQR 32–51), and the median time taken to complete the survey was 11.3 min (IQR 8.4–15.2). Most respondents were female (87%), and the majority reported working in private practice (75%), followed by hospital-based practice (34%) and mixed practices (9%). Most dermatologists (n=48, 91%) indicated that they perform surgery, while 9% (n=5) indicated that they do not perform surgery. Participant demographics are summarized in Table I.
Table I. Participant demographics
| Characteristic | Value, n (%) |
|---|---|
| Total respondents | 53 (57%) |
| Median age [IQR] | 40.0 years [32.0–51.0] |
| Median completion time [IQR] | 11.3 min [8.4–15.2] |
| Sex (Female) | 46 (87%) |
| Sex (Male) | 7 (13%) |
| Practice type (Private) | 40 (75%) |
| Practice type (Hospital) | 18 (34%) |
| Practice type (Mixed) | 5 (9%) |
| Performs surgery (Yes) | 48 (91%) |
| Performs surgery (No) | 5 (9%) |
Vignettes
The nine clinical vignettes presented 9 melanocytic lesions, each exhibiting varying levels of suspicion for melanoma as observed through clinical and dermoscopy images. The maximum depth was assessed through the use of ultrasound technology. Overall, a 1-step surgical approach was chosen in 28% of the 9 clinical situations. One-step surgery was selected in only 10% of responses for the 2 lesions considered less suggestive of malignancy (vignette D and H, including one benign lesion), in contrast to 34% for the 7 other lesions that were deemed more suspicious (p<0.0001). The benign lesion (vignette H) was observed in a patient who had a prior history of melanoma, as noted in the synopsis. The majority of participants recommended diagnostic excision without margins (n=44/53), while 5 opted for a 3-month follow-up, and 4 selected a 1-step wide excision with a 1 cm margin. Two lesions, one situated on the sole (vignette B) and the other on the back (vignette F), were previously assessed through punch biopsy, which confirmed a diagnosis of melanoma. In one instance, the Breslow thickness was also documented on pathology report. In these 2 instances (B and F), 47% of participants opted for 1-step surgery, whereas only 24.5% made the same choice in the 7 other cases lacking histopathology (p<0.0001). The responses to clinical vignettes across simplified management categories are summarized in Table SI.
Five-point Likert scale questionnaire
The 5-point Likert-scale questions (1=strongly disagree, 5=strongly agree) provided further insights into perceptions of ultrasound.
When asked whether cutaneous ultrasound is easily accessible to all patients with melanoma, the median score was 2 [IQR 1–3], indicating limited perceived accessibility (Fig. 1).
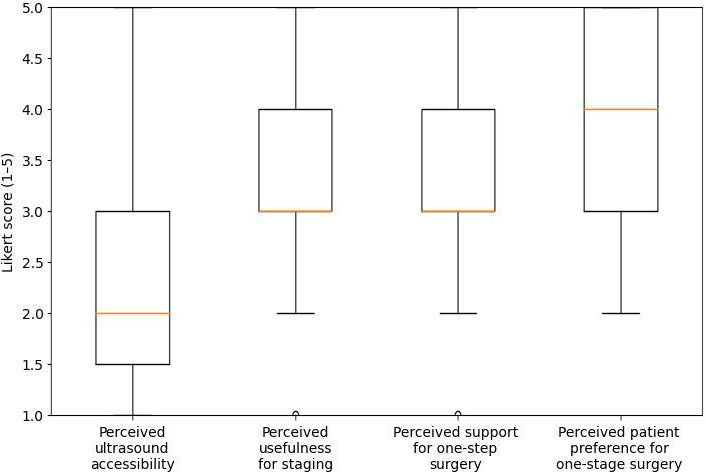
Fig. 1. Distribution of dermatologists’ perceptions regarding accessibility and usefulness of ultrasound and perceived patient preference for 1-step melanoma surgery. Boxes represent the interquartile range, centre lines the median, and whiskers represent the range. Responses were recorded on a 5-point Likert scale.
For the statement “Performing a skin ultrasound is very useful for determining the depth of melanoma”, the median score was 3 [IQR 3–4], suggesting moderate confidence in its utility (Fig. 1).
When asked whether preoperative ultrasound measurement of Breslow thickness helps proceed to 1-step wide excision, the median score was 3 [IQR 3–4], reflecting cautious acceptance of the principle (Fig. 1).
Finally, for the statement “Most patients with cutaneous melanoma prefer to undergo a single surgical procedure rather than two”, dermatologists reported a median score of 4 [IQR 3–5], indicating that most respondents believed patients would prefer a 1-step surgical approach (Fig. 1).
Open-ended question
Participants identified several obstacles to performing wide excision without prior histopathology. The most frequently reported concerns were overtreatment of benign lesions and potential patient dissatisfaction (n=14), excessively wide margins due to overestimation of Breslow thickness (n=12), and the technical difficulty of performing large excisions in an outpatient setting without sufficient time or assistance (n=11). Additional obstacles included medico-legal concerns related to the absence of histopathological proof (n=9), anatomical restrictions in cosmetically or functionally sensitive areas (n=8), and the benefit of a 2-step procedure to allow patients time to process their diagnosis before definitive excision (n=5). Less frequently cited barriers were sentinel lymph node biopsy difficulties (n=4), diagnostic uncertainty (n=4), concerns about ultrasound reliability (n=3), and postoperative complications in office-based practice (n=2). These findings are summarized in Table II.
Table II. Obstacles to 1-step wide excision without histopathology
| Obstacle (wide excision without histopathology) | n |
|---|---|
| Overtreatment of benign lesions / patient dissatisfaction | 14 |
| Excessively wide margins if ultrasound overestimates Breslow | 12 |
| Large excisions difficult in office (time/assistance) | 11 |
| Medico-legal risk (no histopathology before wide excision) | 9 |
| Anatomically difficult sites (face, palms, soles) | 8 |
| A 2-step pathway preferred to allow patient acceptance | 5 |
| Sentinel lymph node issues | 4 |
| Diagnostic uncertainty | 4 |
| Reliability of ultrasound thickness | 3 |
| Postoperative complications in office practice | 2 |
With respect to ultrasound-guided wide excision, the most frequently cited limitation was the restricted availability of high-resolution ultrasound outside hospital settings (n=18). Other barriers included doubts regarding the accuracy of Breslow thickness measurement (n=7), the belief that histopathological confirmation is required before excision (n=6), anatomical difficulties (n=6), the risk of overly wide excisions (n=6) and a lack of available operators for 1-step procedures (n=5). Less commonly reported issues included logistical constraints in private practice (n=3), sentinel node management (n=3) and concerns about deviation from established guidelines (n=2). These barriers are summarized in Table III.
Table III. Obstacles to ultrasound-guided surgery
| Obstacle (ultrasound-guided surgery) | n |
|---|---|
| Limited access to high-resolution ultrasound | 18 |
| Reliability of ultrasound Breslow measurement | 7 |
| Belief that histopathology is needed before wide excision | 6 |
| Anatomical difficulties | 6 |
| Risk of excessive excision | 6 |
| Lack of available operator for 1-step pathway | 5 |
| Office setting logistics | 3 |
| Sentinel node logistics | 3 |
| Outside recommendations/guidelines | 2 |
Unstructured remarks corroborated these findings. Participants predominantly highlighted challenges in obtaining ultrasound services outside of academic institutions (n=14), but several indicated a desire to enhance the incorporation of ultrasonography into clinical practice (n=12). Supplementary comments emphasized the necessity for operator training and expertise (n=5), the opportunity to enhance care via a 1-step process (n=5) and apprehensions over scarring or overtreatment (n=5). A limited number of participants also identified difficulties with sentinel node logistics and emphasized the abruptness of a 1-step method in contrast to the more gradual 2-step process.
DISCUSSION
This study highlights a clear gap between emerging evidence supporting ultrasound-guided 1-step melanoma surgery and its real-world clinical adoption. Although high-frequency ultrasound has demonstrated strong correlation with histopathologic Breslow thickness in multiple studies, including systematic reviews and meta-analyses (5, 6), dermatologists in our survey adopted a cautious approach, favouring the conventional 2-stage pathway in most scenarios.
The presence of histopathologic confirmation strongly influenced decision-making. When melanoma had already been diagnosed by punch biopsy, acceptance of 1-step surgery nearly doubled. This finding underscores the central role of diagnostic certainty in surgical planning and reflects adherence to established recommendations that prioritize histopathological confirmation prior to definitive excision (1, 2). Our results suggest that deviation from this paradigm even when supported by imaging accuracy generates substantial professional reluctance.
Importantly, the reluctance observed was not primarily related to disbelief in ultrasound technology. Participants generally acknowledged its utility for thickness estimation and surgical planning. Instead, the major barriers were structural and medico-legal. Limited access to high-resolution ultrasound outside academic centres was the most frequently cited limitation, reflecting disparities in technological infrastructure. Previous studies have also reported uneven access to advanced imaging tools and emphasized that operator expertise and equipment availability are key determinants of ultrasound accuracy (6, 9, 10). Implementation of ultrasound-guided pathways therefore appears contingent not only on scientific evidence but also on resource distribution and adequate training.
Medico-legal concerns emerged as another prominent theme. Performing wide excision without prior histopathologic proof was perceived as legally vulnerable, particularly in cosmetically sensitive or functionally complex anatomical sites. This finding is consistent with current international recommendations that emphasize histopathologic confirmation and Breslow thickness measurement prior to definitive wide excision (1, 2).
Another recurring concern was the risk of overtreatment, especially if ultrasound were to overestimate Breslow thickness. Although prior prospective studies have demonstrated strong concordance between ultrasound and histopathological measurements (5, 7, 11, 12), dermatologists expressed concern that potential overestimation could lead to unnecessarily wide excisions. While this limitation has been reported to occur only rarely in previous evaluations of the technique (5, 7), even small uncertainties may influence clinical decision-making. Some participants also raised concerns regarding the implications for sentinel lymph node procedures. An important practical consideration concerns the integration of the 1-step surgical approach with sentinel lymph node biopsy (SLNB) pathways. In routine melanoma management, the indication for SLNB is typically determined after histopathological confirmation of melanoma and measurement of Breslow thickness following diagnostic excision (1, 2). In a 1-step strategy performed without prior histopathological confirmation, the indication for SLNB may therefore remain uncertain at the time of surgery. However, estimation of Breslow thickness may help identify situations in which SLNB is unlikely to be indicated, such as very thin melanomas (typically ≤0.8 mm without additional high-risk features, given the low probability of lymph node involvement) or very thick melanomas (e.g. ≥4 mm, where adjuvant systemic therapy may be considered regardless of SLNB status, in accordance with current European guidelines) (2, 13). In other situations, SLNB may need to be performed as a secondary procedure following histopathological analysis of the excised specimen, potentially increasing logistical complexity and patient burden. These uncertainties represent a significant limitation of the 1-step approach and highlight the importance of defining clear clinical pathways before widespread implementation.
Interestingly, dermatologists widely believed that patients would prefer a single-stage procedure. This perception aligns with qualitative research showing that patients value procedural efficiency, reduced waiting time, and psychological reassurance when management can be completed in a single intervention (8). However, clinician caution appeared to outweigh perceived patient preference, highlighting the challenges associated with translating innovative approaches into routine clinical practice.
From an implementation perspective, these findings suggest that broader adoption of ultrasound-guided 1-step melanoma surgery will require more than diagnostic validation. Structured training programmes, improved access to high-frequency ultrasound equip-ment, and clearer integration into clinical guidelines may help facilitate wider acceptance of this strategy.
Limitations
This study has several limitations. First, it was conducted within a single French region, which may limit generalizability to other healthcare systems with different access to high-frequency ultrasound. Second, participation was voluntary, introducing potential selection bias, as dermatologists with greater interest in melanoma management may have been more likely to respond. Third, responses to clinical vignettes may not fully reflect operative decision-making in real-world practice. Another limitation is that the level of familiarity with dermoscopy among respondents was not assessed. Differences in dermoscopic expertise may influence diagnostic confidence and therapeutic decision-making, and future studies should consider including this parameter. Finally, the moderate sample size limited the power for extensive subgroup analyses.
Despite these limitations, the inclusion of detailed clinical vignettes incorporating dermoscopic and ultrasound data strengthens the relevance of the findings to real-world clinical practice and provides insight into decision-making processes.
Conclusion
Together, our findings indicate that dermatologists acknowledge the potential advantages of 1-step melanoma surgery guided by ultrasound; however, their widespread implementation will necessitate the resolution of technical, infrastructural, and medico-legal obstacles. The potential for expanded clinical implementation may be facilitated by the expansion of training opportunities, the provision of high-resolution equipment, and the development of standardized guide-lines that align with European recommendations (2).
ACKNOWLEDGEMENTS
The authors thank the dermatologists belonging to ADERMCO and AIDA who completed the questionnaire.
REFERENCES
- Guillot B, Dalac S, Denis MG, Dupuy A, Emile JF, De La Fouchardiere A, et al. French updated recommendations in Stage I to III melanoma treatment and management. J Eur Acad Dermatol Venereol 2017; 31: 594–602. https://doi.org/10.1111/jdv.14064
- Garbe C, Amaral T, Peris K, Hauschild A, Arenberger P, Basset-Seguin N, et al. European consensus-based interdisciplinary guideline for melanoma. Part 2: Treatment - Update 2024. Eur J Cancer 2025; 215: 115153. https://doi.org/10.1016/j.ejca.2024.115153
- Reali UM, Santucci M, Paoli G, Chiarugi C. The use of high resolution ultrasound in preoperative evaluation of cutaneous malignant melanoma thickness. Tumori 1989; 75: 452–455. https://doi.org/10.1177/030089168907500510
- Tacke J, Haagen G, Hornstein OP, Huettinger G, Kiesewetter F, Schell H, et al. Clinical relevance of sonometry-derived tumour thickness in malignant melanoma--A statistical analysis. Br J Dermatol 1995; 132: 209–214. https://doi.org/10.1111/j.1365-2133.1995.tb05015.x
- Machet L, Belot V, Naouri M, Boka M, Mourtada Y, Giraudeau B, et al. Preoperative measurement of thickness of cutaneous melanoma using high-resolution 20 MHz ultrasound imaging: A monocenter prospective study and systematic review of the literature. Ultrasound Med Biol 2009; 35: 1411–1420. https://doi.org/10.1016/j.ultrasmedbio.2009.03.018
- Sellyn GE, Lopez AA, Ghosh S, Topf MC, Chen H, Tkaczyk E, et al. High-frequency ultrasound accuracy in preoperative cutaneous melanoma assessment: A meta-analysis. J Eur Acad Dermatol Venereol 2025; 39: 86–96. https://doi.org/10.1111/jdv.20179
- Chaput L, Laurent E, Pare A, Sallot A, Mourtada Y, Ossant F, et al. One-step surgical removal of cutaneous melanoma with surgical margins based on preoperative ultrasound measurement of the thickness of the melanoma. Eur J Dermatol 2018; 28: 202–208. https://doi.org/10.1684/ejd.2018.3298
- Lim M, Kervarrec T, Mourtada Y, Chaput L, Lebeau JP, Machet L. Exploring patients’ perceptions of one-step surgery for primary cutaneous melanoma: A qualitative study. Acta Derm Venereol 2024; 104: adv40064. https://doi.org/10.2340/actadv.v104.40064
- Wortsman X, Alfageme F, Roustan G, Arias-Santiago S, Martorell A, Catalano O. Ultrasound in dermatology: Why, how, and when? Semin Ultrasound CT MR 2013; 34: 177–195. https://doi.org/10.1053/j.sult.2012.10.001
- Di Stefani A, Chimenti S, Basile D, Soyer HP, Argenziano G, Peris K, et al. Role of ultrasound in preoperative assessment of melanoma. J Eur Acad Dermatol Venereol 2017; 31: 758–763.
- Vilana R, Puig S, Sanchez M, Squarcia M, Lopez A, Castel T, et al. Preoperative assessment of cutaneous melanoma thickness using 10-MHz sonography. AJR Am J Roentgenol 2009; 193: 639–643. https://doi.org/10.2214/AJR.08.1387
- Fernández Canedo I, de Troya Martín M, Fúnez Liébana R, Rivas Ruiz F, Blanco Eguren G, Blázquez Sánchez N. Preoperative 15-MHz ultrasound assessment of tumor thickness in malignant melanoma. Actas Dermosifiliogr 2013; 104: 227–231. https://doi.org/10.1016/j.ad.2012.06.007
- van Akkooi ACJ, Eggermont AMM. Reduction in surgical interventions in melanoma. Eur J Cancer 2025; 220: 115376. https://doi.org/10.1016/j.ejca.2025.115376