SHORT COMMUNICATION
Mycosis Fungoides with Concurrent Squamous Cell Carcinoma in a Young Patient: A Rare Case
Jianv WANG1![]() , Wei CHEN1, Tingting WANG1* and Lin WANG1*
, Wei CHEN1, Tingting WANG1* and Lin WANG1*
1Department of Dermatovenereology, West China Hospital, Sichuan University, Chengdu 610041, China. *Emails: wangtingting817@126.com; lkzwl@126.com
Citation: Acta Derm Venereol 2026; 106: adv-2025-0062. DOI: https://doi.org/10.2340/actadv.v106.adv-2025-0062.
Copyright: © The Authors 2026. Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Sept 29, 2025. Accepted after revision: Jun 2, 2026.
Published: Jun 24, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
This study was supported by the Sichuan Provincial Administration of Traditional Chinese Medicine (25ZDIZX037).
The data that support the findings of this study are available from the corresponding author upon reasonable request.
The patient in this manuscript had given written informed consent to publication of his case details during hospitalization.
INTRODUCTION
Mycosis fungoides (MF) is the most prevalent form of primary cutaneous T-cell lymphoma (CTCL), typically progressing through patch, plaque and tumour stage. Approximately 20% of patients with advanced-stage disease develop lymph node or visceral involvement (1). Immunological dysregulation, chronic inflammation and impaired skin barrier function in MF may contribute to an elevated risk of secondary malignancies (2). Squamous cell carcinoma (SCC) is a prevalent cutaneous malignancy, often associated with ultraviolet (UV) exposure, chronic inflammation and immunosuppression (3). Although SCC has been reported in MF patients, it is predominantly observed in those who have undergone local chemotherapy ((e.g.) nitrogen mustard), radiotherapy (e.g. total skin electron beam therapy, TSEB) or phototherapy (e.g. PUVA, NB-UVB) (4). These treatments have been associated with DNA damage and an elevated risk of secondary skin malignancies. However, the occurrence of SCC in MF patients without prior exposure to these therapies is exceedingly rare, and the underlying mechanisms remain unclear. Here, we report a case of rapidly progressive SCC in a young patient with MF who had not received radiotherapy, phototherapy or chemotherapy. This case underscores that additional cutaneous malignancies should remain a diagnostic consideration in patients with MF, even in young patients without conventional treatment-related carcinogenic exposures.
CASE REPORT
A 29-year-old male presented with a 10-year history of recurrent pruritic erythematous plaques on the trunk, with progressive worsening and ulceration over the past 4 months. Physical examination revealed an approximately 15 × 15 cm irregular ulcer with an erythematous base and exudate on the left anterior chest, as well as an approximately 8 × 10 cm ulcer on the right upper abdomen characterized by a firm, yellow, hyperkeratotic, exophytic mass (Fig. 1A). Multiple erythematous plaques were also observed on the trunk and extremities. Wound cultures yielded Staphylococcus aureus (S. aureus). Laboratory investigations – including haematologic, biochemical, coagulation, microbiological, and immunological parameters – were within normal limits. Bone marrow aspiration showed active granulopoiesis and erythropoiesis without neoplastic infiltration. PET-CT demonstrated increased metabolic activity in the abdominal lesion and cutaneous thickening of the left chest, with reactive bilateral axillary lymphadenopathy.
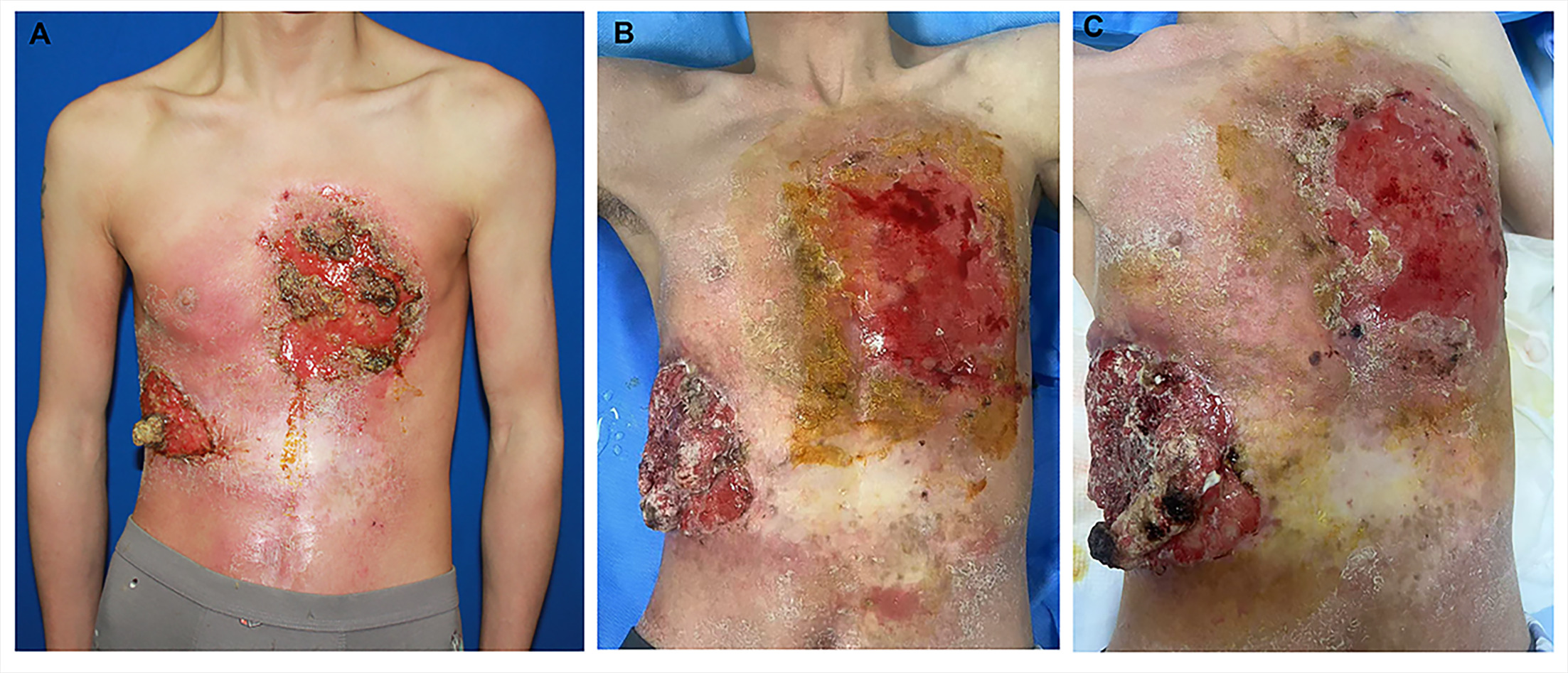
Fig. 1. Clinical presentation and progression of cutaneous lesions. (A) An approximately 15 × 15 cm ulcerated and eroded lesion on the left chest with an erythematous base, irregular borders and white exudate. An approximately 8 × 10 cm ulcerated lesion on the right upper abdomen exhibits a central hyperkeratotic mass. (B, C) Follow-up images at 3 and 4 months post-treatment show progressive enlargement of the abdominal keratotic mass with increased necrosis, as well as marked worsening of the chest ulcer and erosion, consistent with rapid tumour progression.
Histopathological examination of the left chest ulcer revealed epidermal atrophy, hyperkeratosis, basal layer liquefaction, prominent epidermotropism and dense perivascular lymphoplasmacytic infiltration (Fig. S1A). The right chest plaque showed parakeratosis, Pautrier microabscesses and band-like lymphocytic infiltrates (Fig. S1B). Immunohistochemistry of both lesions demonstrated infiltrating lymphocytes positive for CD2, CD3 and CD4, negative for CD7, CD8 and CD20, with a Ki-67 proliferation index of approximately 10% (Fig. S1C). CD5 and CD30 were not expressed in the left ulcer, whereas partial expression of both markers was observed in the right plaque. Clonal T-cell receptor rearrangement was confirmed only in the left lesion. A third biopsy from the right abdominal mass confirmed invasive keratinizing SCC (Fig. S2A, B), while adjacent tissue demonstrated atypical lymphocytes infiltrating within and around the SCC nests (Fig. S2C, D). Inguinal lymph node biopsy revealed dermatopathic lymphadenitis without histological evidence of lymphoma involvement.
Integrating clinical, histopathological, immuno-phenotypic and molecular findings, a final diagnosis of MF (Stage IIB; T3N0M0B0) with concurrent SCC was established. The patient received multimodal treatment, including antibiotics, laser therapy, NB-UVB, chemotherapy (gemcitabine and capecitabine) and radiotherapy. However, the disease progressed, and treatment was discontinued after 4 months due to clinical deterioration and financial constraints (Fig. 1B and C), and the patient subsequently died approximately 2 months later.
DISCUSSION
Although patients with MF have been reported to have an increased risk of cutaneous epithelial malignancies, with one cohort of 202 patients with MF/Sézary syndrome showing a prevalence of 10.5% (5), the published literature suggests heterogeneous clinical contexts. In treatment-associated contexts, Lee et al. identified 4 SCC lesions among 29 patients with MF treated with topical nitrogen mustard (6), whereas South et al. described SCC arising within a previously irradiated MF lesion 17 years after localized radiotherapy (7). Conversely, SCC has also been documented in MF-affected skin without prior carcinogenic exposure: Muradova et al. reported SCC within a long-standing MF patch in a patient with no previous local or systemic therapy (8), and Le et al. described multiple moderately differentiated SCCs in MF-affected skin in a patient without prior carcinogenic treatment (9). Collectively, these reports indicate that SCC in patients with MF can occur in diverse clinical contexts, although reports involving young patients without known carcinogenic exposure remain limited.
In the present case, the patient was only 29 years old, substantially younger than the median age of 55–65 years reported in most previous cases of MF with SCC (8, 10). The SCC developed on the right upper abdomen, a non-sun-exposed site, before the patient had received radiotherapy, systemic chemotherapy, or other potentially carcinogenic therapies. Clinically, the lesion was extensive, with prominent ulceration, erosion, and a rapidly enlarging hyperkeratotic tumour mass that progressed despite multimodal treatment. Although the MF and SCC lesions were anatomically adjacent and atypical lymphocytes were observed around and within SCC nests, direct histological or molecular evidence supporting a causal relationship or shared clonal origin remains unknown.
Previous studies have proposed several mechanisms that may help contextualize the coexistence of MF and SCC. Chronic inflammation may be relevant (11), as MF lesions are characterized by persistent inflammatory infiltration, epidermal barrier disruption and repeated tissue repair, processes that may promote keratinocyte proliferation, oxidative stress, DNA damage and genomic instability (12). Inflammation-associated pathways, including NF-κB and STAT3, have also been implicated in inflammation-related epithelial carcinogenesis (13). Immune dysregulation may represent another relevant factor, as MF is associated with complex local and systemic immune abnormalities that may alter inflammatory responses, immune surveillance and the tumour microenvironment (8). In this context, impaired antitumour surveillance may weaken immune control of dysplastic keratinocytes, providing a plausible link between immune dysregulation and cutaneous carcinogenesis (14). In addition, wound culture from this patient’s lesion was positive for S. aureus. S. aureus colonization or infection is common in patients with MF and has been associated with barrier disruption, inflammation and immune imbalance. Its enterotoxins may affect T-cell activation and influence the cutaneous lymphoma microenvironment through STAT3 activation and immunoregulatory cytokines such as IL-10 (15). In this case, S. aureus infection is best interpreted as a marker of local barrier dysfunction and inflammatory burden, rather than direct evidence of carcinogenesis.
In summary, this report describes a rare case of rapidly progressive SCC in a young patient with MF who had no previous exposure to potentially carcinogenic therapy. Clinicians should remain alert to the possibility of additional cutaneous malignancies in patients with MF, particularly when lesions show rapid growth, ulceration, abnormal proliferation or marked hyperkeratosis. Long-term surveillance remains important regardless of age or treatment history. Further studies are needed to better characterize similar cases of coexisting MF and SCC.
REFERENCES
- Liu X, Jin S, Hu S, Li R, Pan H, Liu Y, et al. Single-cell transcriptomics links malignant T cells to the tumor immune landscape in cutaneous T cell lymphoma. Nat Commun 2022; 13: 1158. https://doi.org/10.1038/s41467-022-28799-3
- Whittaker S. Biological insights into the pathogenesis of cutaneous T-cell lymphomas (CTCL). Semin Oncol 2006; 33: S3–6. https://doi.org/10.1053/j.seminoncol.2005.12.015
- Liu T, Jiang F, Yu LY, Wu YY. Lidocaine represses proliferation and cisplatin resistance in cutaneous squamous cell carcinoma via miR-30c/SIRT1 regulation. Bioengineered 2022; 13: 6359–6370. https://doi.org/10.1080/21655979.2022.2031419
- Abel EA, Sendagorta E, Hoppe RT. Cutaneous malignancies and metastatic squamous cell carcinoma following topical therapies for mycosis fungoides. J Am Acad Dermatol 1986; 14: 1029–1038. https://doi.org/10.1016/s0190-9622(86)70128-x
- Du Vivier A, Vonderheid EC, Van Scott EJ, Urbach F. Mycosis fungoides, nitrogen mustard and skin cancer. Br J Dermatol 1978; 99: 61–63. https://doi.org/10.1111/j.1365-2133.1978.tb01962.x
- Lee LA, Fritz KA, Golitz L, Fritz TJ, Weston WL. Second cutaneous malignancies in patients with mycosis fungoides treated with topical nitrogen mustard. J Am Acad Dermatol 1982; 7: 590–598. https://doi.org/10.1016/s0190-9622(82)70138-0
- South SC, Kluglein KA, Demoret B, Miller R. Cutaneous squamous cell carcinoma arising within a previously irradiated mycosis fungoides lesion. Cureus 2024; 16: e73071. https://doi.org/10.7759/cureus.73071
- Muradova E, Patel N, Chen PL, Seminario-Vidal L. Cutaneous squamous cell carcinoma arising within a mycosis fungoides patch: Case report and review of the literature. JAAD Case Rep 2020; 6: 1288–1290. https://doi.org/10.1016/j.jdcr.2020.09.016
- Le K, Lim A, Samaraweera U, Morrow C, See A. Multiple squamous cell carcinomas in a patient with mycosis fungoides. Australas J Dermatol 2005; 46: 270–273. https://doi.org/10.1111/j.1440-0960.2005.00198.x
- Terada T. Mycosis fungoides in plaque stage with pronounced eosinophilic infiltration, folliculotropism, and concomitant invasive squamous cell carcinoma. Int J Clin Exp Pathol 2013; 6: 749–756.
- Stolearenco V, Namini MRJ, Hasselager SS, Gluud M, Buus TB, Willerslev-Olsen A, et al. Cellular interactions and inflammation in the pathogenesis of cutaneous T-cell lymphoma. Front Cell Dev Biol 2020; 8: 851. https://doi.org/10.3389/fcell.2020.00851
- Kay J, Thadhani E, Samson L, Engelward B. Inflammation-induced DNA damage, mutations and cancer. DNA Repair 2019; 83: 102673. https://doi.org/10.1016/j.dnarep.2019.102673
- Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell 2010; 140: 883–899. https://doi.org/10.1016/j.cell.2010.01.025
- Plasmeijer EI, Sachse MM, Gebhardt C, Geusau A, Bouwes Bavinck JN. Cutaneous squamous cell carcinoma (cSCC) and immunosurveillance - The impact of immunosuppression on frequency of cSCC. J Eur Acad Dermatol Venereol 2019; 33: 33–37. https://doi.org/10.1111/jdv.16025
- Krejsgaard T, Willerslev-Olsen A, Lindahl LM, Bonefeld CM, Koralov SB, Geisler C, et al. Staphylococcal enterotoxins stimulate lymphoma-associated immune dysregulation. Blood 2014; 124: 761–770. https://doi.org/10.1182/blood-2014-01-551184