ORIGINAL REPORT
A Cross-sectional Study on Quality of Life in EB: Validation of the Italian QOLEB and Assessment in Italian Patients
Giovanna ZAMBRUNO1![]() , Tonia SAMELA2
, Tonia SAMELA2![]() , Andrea DIOCIAIUTI1
, Andrea DIOCIAIUTI1![]() , Gudrun SALAMON3
, Gudrun SALAMON3![]() , Sophie STROBL3,4
, Sophie STROBL3,4![]() , Cinzia PILO5, Damiano ABENI2
, Cinzia PILO5, Damiano ABENI2![]() , Renata LINERTOVÁ6
, Renata LINERTOVÁ6![]() , Dedee F. MURRELL7
, Dedee F. MURRELL7![]() , May EL HACHEM1*
, May EL HACHEM1*![]() and the BUR-EB Study Group
and the BUR-EB Study Group
1Dermatology Unit and Genodermatosis Research Unit, Translational Pediatrics and Clinical Genetics Research Division, Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy, 2Laboratory of Clinical Epidemiology, IDI-IRCCS, Rome, Italy, 3HEALTH Lab, Competence Center for Medical and Health Psychology, Faculty of Psychology, Sigmund Freud University Vienna, Vienna, Austria, 4Department of Dermatology, Medical Centre, Faculty of Medicine, University of Freiburg, Freiburg, Germany, 5DEBRA Italy ETS, Milan, Italy, 6Servicio de Evaluación del Servicio Canario de la Salud (SESCS), Instituto de Investigación Sanitaria de Canarias (IISC), Santa Cruz de Tenerife, Spain, and 7Department of Dermatology, St George Hospital, Sydney and Faculty of Medicine, University of NSW, Sydney, Australia
Corr: May El Hachem, Dermatology Unit, Bambino Gesù Children’s Hospital, Piazza Sant’Onofrio 4, 00165, Rome, Italy. *Email: may.elhachem@opbg.net
Key words: Epidermolysis bullosa; health-related quality of life; pain; patient-reported outcome measure; symptom burden; female.
Citation: Acta Derm Venereol 2026; 106: adv-2026-0543. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0543.
Copyright: © The Authors 2026. Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 27, 2026. Accepted after revision: May 28, 2026.
Published: Jun 29, 2026.
Competing interests and funding: The project BUR-EB has received funding from the European Union’s Horizon 2020 research and innovation programme under the EJP RD COFUND-EJP Nº 825575. This work was also supported in part by the Italian Ministry of Health with “Current Research funds”.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
For Italy, the research was approved by the Institutional Ethical Committee of Bambino Gesù Children’s Hospital (OPBG) (protocol number 3107/2023).
M.E.H. is member of the advisory board of Chiesi Global Rare Diseases, and consultant for Krystal Biotech. G.Z. has acted as invited speaker for Chiesi Global Rare Diseases. D.F.M. is creator of QOLEB.
Inherited epidermolysis bullosa comprises a heterogeneous group of skin fragility diseases, presenting with a range of manifestations and complications that profoundly affect quality of life (QoL). A disease-specific instrument, Quality of Life in EB (QOLEB), has been developed to assess the impact of epidermolysis bullosa signs and symptoms on QoL. The aim of this cross-sectional study, conducted as part of a European project – BUR-EB, was to test the psychometric properties of the Italian version of the QOLEB and to assess QoL in Italian epidermolysis bullosa patients. Demographic, clinical, and QOLEB data of 56 Italian patients aged ≥11 years participating in the BUR-EB online survey were analysed. Principal component analysis showed excellent internal consistency of Italian QOLEB, and high convergent validity with the generic questionnaire EQ-5D. About 40% of patients reported severe to very severe disease burden, and a strong correlation was observed between disease severity and QOLEB scores. Independent variables associated with worse QoL were pain, chronic wounds, wheelchair use and patient organization membership. Our study confirms the good psychometric properties of the Italian QOLEB. In addition to depicting the major impact of epidermolysis bullosa on QoL, it identifies pain, chronic wounds and functional disability as major targets for therapeutic interventions.
SIGNIFICANCE
Epidermolysis bullosa is a rare inherited disease characterized by lifelong skin blistering. Affected individuals can develop multiple complications that impact on quality of life. This study aimed to validate the Italian version of an epidermolysis bullosa-specific quality of life questionnaire and to evaluate quality of life of people affected by epidermolysis bullosa in Italy. Data were obtained from a European online survey. In addition to confirming the validity of the Italian pidermolysis bullosa-specific quality of life questionnaire, findings show high impact of epidermolysis bullosa and strong correlation between clinical severity and worse quality of life, with a major influence of pain, chronic wounds, wheelchair use and patient organization membership.
INTRODUCTION
Inherited epidermolysis bullosa (EB) comprises a heterogeneous group of rare mucocutaneous blistering disorders due to defective epithelial adhesion (1, 2). Four major types are distinguished based on the level of blister formation: EB simplex (EBS), junctional EB (JEB), dystrophic EB (DEB) and Kindler EB (KEB) (1, 2). Each type can present with a spectrum of clinical manifestations; in particular, EBS, JEB and DEB are classified as localized or generalized major subtypes. Disease complications include chronic wounds, recurrent infections, hand and foot deformities, joint contractures, oesophageal strictures, anaemia, malnutrition, failure to thrive and growth delay, and aggressive squamous cell carcinomas (SCC) (2). In addition, almost all patients experience both acute and chronic pain, often of considerable severity, and frequently report itching (2, 3).
Despite the recent approval of the first topical drug and gene therapies for EB wounds (4), no systemic curative treatment is yet available. In addition, EB manifestations can alter the physical appearance and affect the self-perception of patients. Overall, disease manifestations, care, and direct and indirect healthcare costs strongly impact patient quality of life (QoL) (2).
While validated specialty-specific instruments for assessing the QoL of dermatology patients are available, the development of disease-specific questionnaires remains highly valuable (5, 6). These tools, which focus on a single disease or a group of related conditions, are designed to capture specific disease signs and symptoms and their impact on QoL, thereby aiding in the evaluation of therapeutic interventions (7). Disease-specific measurement instruments are valuable in chronic and complex diseases, like EB (8).
The “Quality of Life in Epidermolysis Bullosa” (QOLEB) questionnaire (9) has been the most widely used disease-specific tool to assess QoL in EB (8, 10). Over time, QOLEB validated translations in several languages have been developed (11, 12, 13, 14, 15, 16, 17, 18). An Italian version has been recently pilot-tested (19). The goal of the present study is to test the psychometric properties of the Italian version of the QOLEB and to assess QoL in Italian EB patients.
MATERIALS AND METHODS
Setting, study design and sample
This is a cross-sectional study conducted as part of the BUR-EB (Changes in the Socio-economic Burden of Epidermolysis Bullosa in Europe) project, aimed to quantify health-related QoL and socio-economic impact of EB on patients and families in Europe (20). The study, developed in collaboration with patients’ associations (DEBRA International and national DEBRAs), was administered as an online survey across 7 European countries. In addition, printed questionnaires were available in reference centres. For Italy, the research was approved by the Institutional Ethical Committee of Bambino Gesù Children’s Hospital (OPBG). The survey was translated and culturally adapted in Italian. It was advertised via social media, national patients’ association, reference centres and directly to patients attending OPBG Rare Skin Disease centre. The survey was accessible between May and November 2024. Due to the rarity of EB, no formal sample size calculation was performed. The study sample was determined by the number of patients available and willing to participate, aiming to include as many participants as possible, a well-established approach in rare disease research (21).
Participants were eligible for the study if they had a confirmed diagnosis of EB, independently of age. Adult participants provided consent via an online form, minors aged ≥4 years provided informed assent.
Data collection
Self-reported data collection comprised socio-demographic and clinical information, including EB type/subtype and presence/absence of 15 EB signs and symptoms (Tables I and SI). For the present study, a clinical severity score was calculated by summing one point for the presence of each EB symptom.
Table I. Sociodemographic characteristics, epidermolysis bullosa (EB) major type and subtype of Italian EB survey respondents
| Variable | Number | Percentage | |
|---|---|---|---|
| Sex | |||
| Male | 20 | 35.7 | |
| Female | 36 | 64.3 | |
| Age | |||
| 11–18 years | 17 | 30.4 | |
| 18–30 years | 14 | 25.0 | |
| >31 years | 25 | 44.6 | |
| Distance (km)a | |||
| <100 | 29 | 51.8 | |
| 101–200 | 8 | 14.3 | |
| >200 | 19 | 33.9 | |
| Educationb | |||
| Primary | 1 | 2.6 | |
| High school | 22 | 56.4 | |
| University | 16 | 41.0 | |
| Marital statusb | |||
| Single | 24 | 61.5 | |
| Married/cohabiting | 14 | 35.9 | |
| Other | 1 | 2.6 | |
| Family history | |||
| No | 47 | 83.9 | |
| Yes | 9 | 16.1 | |
| Caregiver | |||
| No | 19 | 33.9 | |
| Yes | 37 | 66.1 | |
| Caregiver type | |||
| Parent | 31 | 83.8 | |
| Other family member | 4 | 10.8 | |
| Professional | 2 | 5.4 | |
| Patients” association member | |||
| No | 34 | 60.7 | |
| Yes | 22 | 39.3 | |
| EB type | |||
| EB simplex | 13 | 23.2 | |
| Junctional EB | 9 | 16.1 | |
| Dystrophic EB | 31 | 55.4 | |
| Kindler EB | 3 | 5.3 | |
| EB subtypec | |||
| Localized | 13 | 27.7 | |
| Generalized | 34 | 72.3 | |
|
aDistance between reference centre and patient home; breferred to the adult EB individuals; ctotal varies due to 9 missing values. |
|||
The survey comprised standardized health-related generic (i.e. EQ-5D-5L for adults, EQ-5D-Y for minors), and disease-specific (QOLEB for patients≥11 years old) assessment tools.
The online survey data have been downloaded and processed by the BUR-EB coordinating centre which provided the participant centres their set of national data. Data curation was performed by the Austrian study team. Only datasets with complete sociodemographic and clinical data and QOLEB were included.
QOLEB and EQ-5D questionnaires
In its original form, the QOLEB is a self-reported assessment tool conceived for all EB types, composed of 17 items, each scored on a 4-point Likert scale (9). The total score ranges from 0 to 51 and can be further interpreted using clinical bands to classify the disease impact (22). In addition, it can be subdivided into 2 broad subscales: a “Functioning subscale” evaluating physical impact and an “Emotions subscale” that addresses the psychological impact (9). The original QOLEB is validated for patients ≥11 years old (9).
In addition, the general health-related QoL of adult and minor respondents was assessed by the EQ-5D-5L and EQ-5D-Y, respectively, that evaluate 5 health dimensions (23). The combination of the responses under each dimension describes a person’s health state, called EQ-5D profile. A scoring system which uses country-specific value sets, based on representative samples of the general public, converts profile data to a single number – called health utility or EQ-5D value, that lies on a scale between 1, full health, and 0, a state as bad as being dead.
Study phases
To adapt and validate the original QOLEB scale in its Italian version, we used Beaton’s guidelines (24). The evaluation of the psychometric properties of QOLEB is one of the goals of the present study.
Statistical analysis
All variables have been analysed in terms of frequencies and percentages, and means, standard deviations (SD), medians and minimum-maximum values. Cronbach α coefficients were calculated to measure internal consistency (25). The adequacy of the dataset for principal component analysis (PCA) was first assessed using Bartlett Test of Sphericity and the Kaiser–Meyer–Olkin (KMO) measure. A PCA with Varimax rotation was then conducted to identify the underlying factor structure. A scree plot was subsequently generated to better determine the optimal number of components to extract. The instrument’s sensitivity was assessed by analysing floor and ceiling effects (26). Finally, convergent validity was evaluated by calculating Spearman ρ between the total QOLEB and its subscales and the EQ-5D value, determined using the validated value sets available for the Italian and Spanish population (27, 28); values of ρ were defined as high (≥0.7), high–moderate (0.61 to 0.69), moderate (0.4 to 0.6), moderate–weak (0.31 to 0.39) or weak (≤0.3) (29).
Then, for each level of the variables of interest, mean (SD) and median (minimum–maximum) values of the QOLEB were computed. Differences were tested using the Mann–Whitney U test for 2 groups, and the Kruskal–Wallis 1-way analysis of variance (ANOVA) for 3 or more groups. Such differences were also tested pairwise, for each combination of age-group and EB type.
To allow for a meaningful comparison, the scores of the 2 QOLEB subscales were normalized to 100, and the interaction of such scores with the EB subtype (i.e. localized vs generalized) was explored. The correlation between the disease severity score and patient-reported outcomes was studied using Spearman’s correlation coefficient.
To assess the possible independent role of each factor of interest, while controlling for potential confounders, 3 separate multiple linear regression models – for the total score, the Functioning, and the Emotions subscales of the QOLEB – were produced. A backward stepwise selection was used to reach the final regression models: for all 3 outcomes, we started with the same model including all potential predictor variables (as observed in univariate analysis) and iteratively removed the least significant predictor at each step, using the classical stringent criteria of 0.050 for inclusion and 0.100 for removal. All statistical analyses have been performed with the Statistical Package for the Social Sciences (SPSS), version 28.0.0.
RESULTS
Study population
Tables I and SI summarize the sociodemographic and clinical data of 56 Italian EB patients, aged≥11 years. Seventeen patients (30.4%) were minors, 14 (25.0%) were aged between 18 and 30 years, and the remaining 25 (44.6%) were aged ≥31. Most respondents were females (N=36, 64.3%, female/male ratio=1.8). The majority of respondents (N=37, 66.1%) had a caregiver, mainly a parent (N=31, 83.8%). As to the EB type, more than half of the respondents (N=31, 55.4%) were affected with DEB, 9 (16.1%) with JEB, 13 (23.2%) with EBS and 3 (5.3%) with KEB. In addition, 34 (72.3%) had generalized EB. Twenty-two respondents (39.3%) were members of a patients’ association. Interestingly about half of patients with DEB and JEB (54.8% and 44.4%, respectively) were members, compared to only 1 of 13 patients with EBS (7.7%). In addition to blisters and crusts, the most common clinical characteristics reported by participants were atrophic scars (N=37, 66.1%), itch (N=40, 71.4%) and pain (N=35, 62.5%) (Table SI). About half of the patients reported mucosal involvement (N=30, 53.6%) and functional disability (N=29, 51.8%). Less frequent but severe disease manifestations included chronic wounds (N=24, 42.9%), joint deformities (N=19, 33.9%), tooth loss (N=19, 33.9%), malnutrition (N=20, 35.7%), need for oesophageal dilation and gastrostomy tube use (N=20, 35.7%, N=6, 10.7%, respectively) and SCC development (N=10, 17.9%). Wheelchair use was reported by 11 patients (19.6%).
QOLEB psychometric properties
Initial analysis confirmed the dataset suitability for PCA. Bartlett Test of Sphericity was significant (p<0.001), indicating that the items were sufficiently correlated for factor analysis, and KMO measure was 0.84, which is above the recommended threshold of 0.60. The overall internal consistency of the initial 17 items was excellent, with a Cronbach α of 0.93. A PCA with Varimax rotation was conducted to identify the underlying factor structure. The scree plot showed a sharp drop in eigenvalues after the second factor, suggesting a 2-component solution (Fig. S1). This 2-component structure was extracted using an eigenvalue greater than one as the criterion. The 2 components collectively explained 61.55% of the total variance. A total variance >60% indicates that the 2 components are a robust representation of the underlying relationships between the questionnaire items. The Varimax rotation, chosen for its ability to simplify the factor structure and allow for direct comparison with the original study, confirmed a 2-component model. After rotation, the first component explained 31.92% of the variance, and the second 29.63%. The 2 identified components were (i) the Emotions subscale, including items related to feelings, emotions and psychological well-being, and (ii) the Functioning subscale that encompasses items concerning functioning and daily activities. Both subscales showed excellent internal consistency, with a Cronbach’s alpha of 0.91 and 0.90, respectively.
In our analysis, the items QOLEB-3 (physical pain), QOLEB-9 (ability to move outside home), QOLEB-10 (family relationships) and QOLEB-15 (financial burden) showed significant cross-loadings, meaning that they were related to both components, Functioning and Emotions (Table SII). It was decided to maintain these items in the Functioning subscale for content-related reasons and to ensure comparability with the original questionnaire, facilitating cross-cultural comparisons with previously validated national QOLEB versions, which have adhered to the original structure (11, 12, 13, 14, 15, 16, 17, 18).
Spearman ρ showed high convergent validity between the total QOLEB score and the generic EQ-5D both for adults and minors (ρ=-0.761 and -0.885, respectively). The QOLEB Functioning and Emotions subscales revealed a high-moderate to high correlation with the EQ-5D for the child version (ρ=−0.919; -0.680), and a moderate-weak to high for the adult one (ρ=−0.832; −0.387), respectively.
Sensitivity analysis revealed potential floor and ceiling effects (Table SIII). A significant floor effect was observed for the majority of the items, most notably for QOLEB-12 (need for home modifications, 67.9%), QOLEB-4 (ability to write, 60.7%) and QOLEB-2 (ability to bath/shower, 55.4%), indicating that a substantial portion of this sample reported no impact in these areas. Conversely, a ceiling effect was identified for QOLEB-2 (25.0%) and QOLEB-7 (involvement in sports, 19.6%), suggesting that these activities represent major challenges for a significant subgroup of patients.
Assessment of QoL
In our study population, the mean total score of the QOLEB was 17.5±10.8, with mean score for Functioning subscale of 12.0±8.1, and for Emotions subscale of 5.5±3.8. According to QOLEB banding criteria (22), 16 (28.6%) patients reported a very mild to mild disease impact on QoL (score between 0 and 9), 18 (32.1%) a moderate impact (score between 10 and 19), and 22 (39.3%) scored >20 points indicating a severe to very severe disease burden (Table II). As to the EB type, 16 out of 31 (51.6%) DEB cases reported a severe to very severe disease impact, while only 1 EBS (7.7%) reported a severe impact on QoL. Overall, statistically significant differences were observed in the total QOLEB and Functioning, but not Emotions, subscale scores according to different EB major types (Table III). In particular, looking at pairwise comparisons, significantly higher scores were observed for total QOLEB and Functioning subscale for DEB versus EBS (p=0.001 and 0.002, respectively) and for JEB vs EBS (p=0.025 and 0.036, respectively).
Table II. Quality of life in epidermolysis bullosa (QOLEB) total score: banding by EB type and subtype
| Very mild N (%) |
Mild N (%) |
Moderate N (%) |
Severe N (%) |
Very severe N (%) |
Total N (%) |
|
|---|---|---|---|---|---|---|
| EB simplex | 2 (15.4) | 6 (46.1) | 4 (30.8) | 1 (7.7) | 0 (0) | 13 (23.2) |
| Junctional EB | 0 (0) | 2 (22.3) | 3 (33.3) | 3 (33.3) | 1 (11.1) | 9 (16.1) |
| Dystrophic EB | 0 (0) | 5 (16.1) | 10 (32.3) | 10 (32.3) | 6 (19.3) | 31 (55.3) |
| Kindler EB | 0 (0) | 1 (33.3) | 1 (33.3) | 1 (33.3) | 0 (0) | 3 (5.4) |
| Total | 2 (3.6) | 14 (25) | 18 (32.1) | 15 (26.8) | 7 (12.5) | 56 (100%) |
| Localized EB | 1 (7.7) | 4 (30.8) | 6 (46.1) | 2 (15.4) | 0 (0) | 13 (27.7) |
| Generalized EB | 1 (2.9) | 8 (23.5) | 10 (29.4) | 9 (26.5) | 6 (17.7) | 34 (72.3) |
| Totala | 2 (4.5) | 12 (25.5) | 16 (34.0) | 11 (23.4) | 6 (12.8) | 47 (100%) |
|
QOLEB total score and impact on QoL: very mild= 0-4, mild= 5-9, moderate= 10-19, severe= 20-34, very severe= 35-51 (24). aTotal varies due to missing values. |
||||||
Table III. Associations between Quality of Life in Epidermolysis Bullosa (QOLEB) scores (total, Functioning and Emotions subscales) and clinicodemographic variables
| Total QOLEB score | QOLEB Functioning score | QOLEB Emotions score | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Level | N | % | Mean (SD) | Median(min–max) | p-value | Mean (SD) | Median(min–max) | p-value | Mean (SD) | Median(min–max) | p-value |
| Overall | 56 | 100.0 | 17.5 (10.8) | 16.0 (0–43) | 12.0 (8.1) | 10.0 (0–31) | 5.5 (3.8) | 5.0 (0–14) | ||||
| Sex | Males | 20 | 35.7 | 14.9 (9.9) | 11.0 (6-42) | 0.138 | 10,8 (7.6) | 8.0 (4–31) | 0.504 | 4.0 (3.6) | 3.0 (0–14) | 0.007 |
| Females | 36 | 64.3 | 19.0 (11.1) | 19.0 (0–43) | 12.7 (8.4) | 12.5 (0–30) | 6.4 (3.6) | 5.5 (0–13) | ||||
| Age (years) | 11–17 | 17 | 30.3 | 14.1 (12.0) | 9.0 (0–43) | 0.039 | 8.9 (8.9) | 5.0 (0–30) | 0.009 | 5.2 (3.6) | 4.0 (0–13) | 0.815 |
| 18–30 | 14 | 25.0 | 22.6 (10.6) | 23.0 (7–31) | 16.5 (7.4) | 15.5 (5–31) | 6.1 (4.6) | 5.0 (0–14) | ||||
| ≥31 | 25 | 44.7 | 17.1 (9.3) | 17.0 (0–38) | 11.6 (7.1) | 12.0 (0–29) | 5.5 (3.5) | 5.0 (0–13) | ||||
| EB type | Simplex | 13 | 23.2 | 9.7 (6.9) | 8.0 (0–25) | 0.009 | 6.2 (4.8) | 5.0 (0–15) | 0.009 | 3.5 (2.7) | 4.0 (0–10) | 0.182 |
| Junctional | 9 | 16.1 | 19.0 (9.7) | 18.0 (7–38) | 12.4 (7.8) | 12.0 (5–29) | 6.6 (3.1) | 7.0 (2–10) | ||||
| Dystrophic | 31 | 55.4 | 20.9 (11.1) | 21.0 (6-43) | 14.8 (8.2) | 14.0 (4–31) | 6.1 (4.2) | 5.0 (0–14) | ||||
| Kindler | 3 | 5.3 | 12.7 (8.0) | 12.0 (5–21) | 7.0 (5.0) | 7.0 (2–12) | 5.7 (3.1) | 5.0 (3–9) | ||||
| EB subtype | Localized | 13 | 27.7 | 12.2 (7.4) | 11.0 (0–26) | 0.091 | 7.1 (4.6) | 5.0 (0–15) | 0.022 | 5.1 (3.1) | 4.0 (0–12) | 0.981 |
| Generalized | 34 | 72.3 | 18.8 (11.6) | 17.5 (0–43) | 13.3 (8.6) | 12.5 (0–31) | 5.6 (4.0) | 4.5 (0–14) | ||||
| Patients’ association member | No | 34 | 60.7 | 12.3 (7.4) | 11.0 (0–36) | <0.001 | 7.6 (4.8) | 7.0 (0–23) | <0.001 | 4.6 (3.3) | 4.0 (0–13) | 0.026 |
| Yes | 22 | 39.3 | 25.7 (10.2) | 26.0 (8-43) | 18.8 (7.5) | 20.0 (5–31) | 6.9 (4.1) | 5.5 (0–14) | ||||
| Pain | No | 21 | 37.5 | 10.9 (7.4) | 9.0 (0–27) | <0.001 | 7.2 (6.3) | 5.0 (0–23) | <0.001 | 3.7 (2.2) | 4.0 (0–9) | 0.009 |
| Yes | 35 | 62.5 | 21.5 (10.6) | 21.0 (5-43) | 14.9 (7.7) | 13.0 (4–31) | 6.6 (4.1) | 5.0 (0–14) | ||||
| Itch | No | 16 | 28.6 | 10.7 (8.1) | 9.5 (0–37) | 0.001 | 6.7 (6.1) | 5.0 (0–26) | <0.001 | 4.0 (2.4) | 4.0 (0–11) | 0.048 |
| Yes | 40 | 71.4 | 20.3 (10.6) | 21.0 (0–43) | 14.2 (7.9) | 13.0 (0–31) | 6.2 (4.0) | 5.0 (0–14) | ||||
| Chronic wounds | No | 32 | 57.1 | 13.4 (8.4) | 10.5 (0–36) | <0.001 | 8.8 (6.5) | 6.5 (0–23) | <0.001 | 4.6 (3.3) | 4.0 (0–13) | 0.025 |
| Yes | 24 | 42.9 | 23.0 (11.3) | 21.5 (5-43) | 16.2 (8.2) | 15.0 (5–31) | 6.8 (4.1) | 5.5 (0–14) | ||||
| Mucosal involvement | No | 26 | 46.4 | 13.2 (9.4) | 11.0 (0–42) | 0.004 | 8.2 (6.8) | 6.0 (0–31) | <0.001 | 5.1 (3.3) | 4.0 (0–12) | 0.346 |
| Yes | 30 | 53.6 | 29.3 (10.6) | 21.0 (5-43) | 15.4 (7.7) | 13.5 (4–30) | 5.9 (4.1) | 5.0 (0–14) | ||||
| Malnutrition | No | 36 | 64.3 | 13.6 (8.6) | 11.0 (0–38) | <0.001 | 8.4 (6.1) | 6.5 (0–29) | <0.001 | 5.2 (3.4) | 4.0 (0–13) | 0.335 |
| Yes | 20 | 35.7 | 24.7 (10.7) | 25.5 (5-43) | 18.6 (7.3) | 20.5 (5–31) | 6.2 (4.4) | 5.0 (0–14) | ||||
| Joint deformities | No | 37 | 66.1 | 13.8 (8.5) | 11.0 (0–36) | <0.001 | 8.5 (5.7) | 7.0 (0–23) | <0.001 | 5.3 (3.4) | 4.0 (0–13) | 0.519 |
| Yes | 19 | 33.9 | 24.8 (11.2) | 25.0 (5-43) | 18.8 (7.9) | 21.0 (4–31) | 6.1 (4.4) | 5.0 (0–14) | ||||
| Functional disability | No | 27 | 48.2 | 11.7 (6.1) | 10.0 (0–26) | <0.001 | 6.7 (3.5) | 6.0 (0–14) | <0.001 | 5.0 (3.1) | 4.0 (0–12) | 0.310 |
| Yes | 29 | 51.8 | 23.0 (11.4) | 23.0 (0–43) | 17.0 (8.0) | 18.0 (0–31) | 6.0 (4.3) | 5.0 (0–14) | ||||
| Tooth loss | No | 37 | 66.1 | 15.1 (9.9) | 11.0 (0–43) | 0.017 | 9.9 (7.1) | 8.0 (0–30) | 0.010 | 5.2 (3.7) | 4.0 (0–13) | 0.188 |
| Yes | 19 | 33.9 | 22.4 (11.0) | 23.0 (5-42) | 16.2 (8.5) | 18.0 (3–31) | 6.2 (3.8) | 5.0 (0–14) | ||||
| Wheelchair use | No | 45 | 80.4 | 15.0 (8.7) | 11.0 (0–36) | 0.003 | 9.8 (6.1) | 8.0 (0–23) | <0.001 | 5.3 (3.7) | 5.0 (0–14) | 0.299 |
| Yes | 11 | 19.6 | 27.8 (12.6) | 27.0 (5-43) | 21.3 (8.9) | 23.0 (5–31) | 6.5 (4.1) | 6.0 (0–13) | ||||
| Gastrostomy | No | 50 | 89.3 | 16.4 (10.0) | 13.0 (0–42) | 0.057 | 11.2 (7.6) | 9.5 (0–31) | <0.001 | 5.3 (3.6) | 4.5 (0–14) | 0.519 |
| Yes | 6 | 10.7 | 26.8 (13.1) | 28.0 (5–43 | 19.2 (9.0) | 22.5 5–30) | 7.7 (5.0) | 7.5 (0–13) | ||||
| Esophageal dilatation | No | 36 | 64.3 | 16.1 (10.0) | 13.0 (0–38) | 0.205 | 10.5 (7.7) | 7.5 (0–29) | 0.060 | 5.6 (3.4) | 5.0 (0–13) | 0.850 |
| Yes | 20 | 35.7 | 20.1 (11.9) | 18.0 (5-43) | 14.7 (8.4) | 13.0 (4–31) | 5.4 (4.5) | 5.0 (0–14) | ||||
|
N, number; P-values <0.05 are in bold. |
||||||||||||
As to EB subtype, 15 out of 34 (44.2%) generalized forms reported a severe to very severe QoL alteration, while only 2 out of 13 (15.4%) localized EB had severe burden (Table II). Overall, patients with localized EB reported a less severe impact on QOLEB Functioning score compared to those with generalized EB (mean 7.1±4.6 vs 13.3±8.6, p=0.022) (Table III). The normalized mean scores of the 2 subscales were plotted against the EB subtypes, revealing an effect modification of the latter variable: the Functioning mean scores increased dramatically from localized to generalized EB (p=0.019), while the Emotions mean scores, that in localized EB are higher than the Functioning scores, were similar in localized and generalized disease (p=0.699) (Fig. 1).
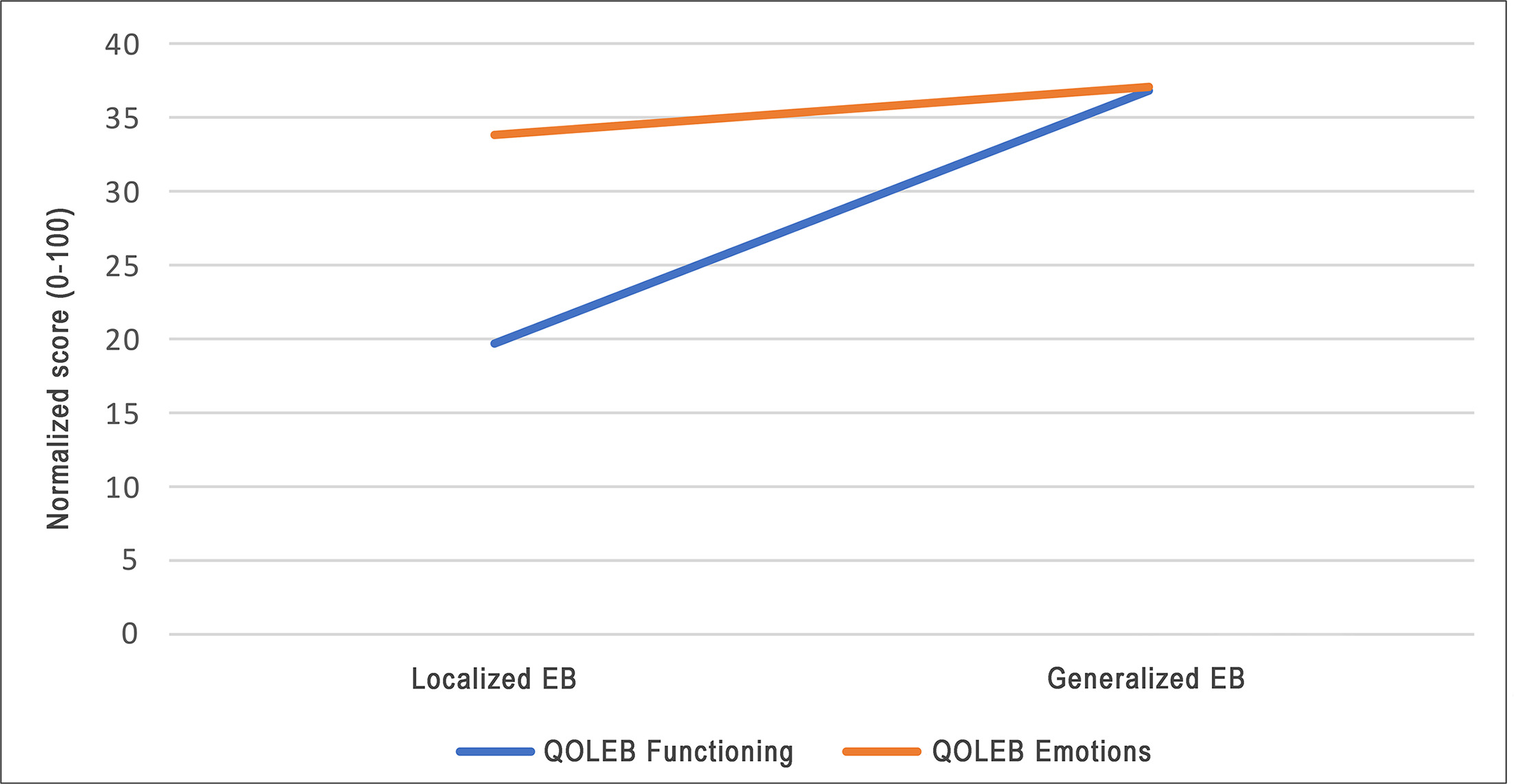
Fig. 1. Normalized scores for the Functioning and Emotions scales of the Quality of Life in Epidermolysis Bullosa (QOLEB) questionnaire, showing mean values by severity level of disease, i.e., localized vs generalized EB.
Most patients complained about difficulties in practicing sports (N=50, 89.3%) and moving around outside their home (N=41, 71.4%) as well as some degree of physical pain (N=49, 87.5%) (Table SIII). In addition, 47 patients (83.9%) reported a family financial impact. As to Emotions, the vast majority of patients reported feelings of frustration (N=45, 80.3%), worry or anxiety (N=44, 78.5%), embarrassment (N=42, 74.9%), and being uncomfortable in social life and with friends (N=39, 69.6 %; N=36, 64.3%, respectively). Finally, 34 patients (60.8%) reported some level of depression.
The total QOLEB score was not different between males and females (p=0.138), but the Emotions subscale score was significantly higher for females (mean 6.4 vs 4.0, p=0.007). Moreover, significant differences in total QOLEB and Functioning scores were observed according to age group. In particular, looking at pairwise comparisons, significantly higher scores were seen for total QOLEB and Functioning subscale for respondents aged between 18 and 30 vs those aged<18 (p=0.021 and 0.006, respectively). Finally, membership of a patients’ association was strongly associated with worse QoL as shown by total QOLEB (mean 25.7±10.2 vs 12.3±7.4, p<0.001) and Functioning (mean 18.8±7.5 versus 7.6±4.8, p<0.001) scores (Table III).
As to disease symptoms and manifestations, the linear correlation between the total disease severity score and the total QOLEB was strong (ρ 0.647), and highly significant (p<0.001). The correlation with the Functioning subscale score resulted even stronger (ρ 0.751, p<0.001), while that with the Emotions subscale was weak (ρ=0.252) and did not reach statistical significance (p=0.061) (Fig. 2). Table III reports the statistically significant associations between presence of single EB manifestations and symptoms and the QOLEB total and subscale scores. In particular, pain and pruritus were significantly associated with worse QoL, as attested by higher total QOLEB and both subscale scores. In a similar way, higher QOLEB total, Functioning and Emotions scores were observed in the presence of chronic wounds. The following disease manifestations were significantly associated with worse QOLEB total and Functioning scores: mucosal involvement, malnutrition, joint deformities, functional disability, tooth loss and wheelchair use. Finally, a greater Functioning impairment was seen in the six patients with gastrostomy compared to those without.

Fig. 2. Scatterplots showing the relationship between Quality of Life in Epidermolysis Bullosa – QOLEB - scores [i.e., total (a), Functioning subscale (b), and Emotions subscale (c)] and the clinical severity score [number of signs and symptoms (range 0–15) reported by patients].
Multivariate linear regression analysis confirmed the association of higher QOLEB total scores with presence of pain, chronic wounds, wheelchair use, and membership of a patients’ association as independent factors (Table IV). As to the Functioning subscale, higher scores were observed in the presence of functional disability, wheelchair use, and patients’ association membership. Finally, the Emotions subscale score was higher in females, and in patients presenting chronic wounds.
Table IV. Multivariate linear regression models for the Quality of Life in Epidermolysis Bullosa (QOLEB) total and subscale scores
| Total QOLEB | QOLEB Functioning score | QOLEB Emotions score | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | Beta coeff. | 95% C.I. | p-value | Beta coeff. | 95% C.I. | p-value | Beta coeff. | 95% C.I. | p-value |
| Females vs males | – | – | – | – | – | – | 2.6 | 0.6–4.6 | 0.013 |
| Pain yes vs no | 5.0 | 0.2–9.7 | 0.041 | 2.9 | -0.1–6.0 | 0.058 | – | – | – |
| Chronic wounds yes vs no | 6.0 | 1.3–10.6 | 0.014 | 2.9 | -0.04–5.9 | 0.053 | 2.8 | 0.8–4.8 | 0.007 |
| Functional disability yes vs no | – | – | – | 3.7 | 0.3–7.0 | 0.033 | – | – | – |
| Wheelchair use yes vs no | 7.5 | 0.9–14.1 | 0.026 | 6.0 | 1.7–10.3 | 0.007 | – | – | – |
| Member of patient association yes vs no | 7.7 | 2.5–12.9 | 0.005 | 5.7 | 2.4–9.0 | 0.001 | 1.9 | −0.2–3.9 | 0.076 |
|
P-values <0.05 in bold. C.I.:confidence interval; Coeff.:coefficient. |
|||||||||
DISCUSSION
The present study validated the Italian version of the QOLEB, and employed this tool to assess the disease impact on QoL of Italian individuals with all EB types. Interestingly, the majority of respondents were female, mirroring the German and Spanish QOLEB data (16, 18) as well as data from other surveys on EB patients (30, 31). This finding is consistent with the gender participation bias (32). Among the 37 respondents with a caregiver, only 2 had a professional one. This likely reflects the tendency among Italian EB families to aid themselves, but possibly also deficiencies in the Italian home healthcare system. Greater resources for professional caregivers might help to reduce the family disease burden.
The PCA showed an excellent internal consistency of the QOLEB items, similar to values obtained in the validation of the original questionnaire and its other national versions (9, 11, 12, 14, 15, 16, 17, 18). Varimax rotation confirmed the validity of the original 2-component structure in Italian EB respondents. Convergent validity was found to be excellent for the total QOLEB score and both subscales in the paediatric sample. Similar results were observed in adults, except for the Emotions subscale, which demonstrated a moderate–weak correlation.
Floor effects were seen for many items, a finding consistent with results reported during the QOLEB validation in other countries (12, 16). Rather than indicating a lack of validity, the presence of these effects reflects the high clinical heterogeneity of EB and the broad range of disease severity within our sample. Such observations are common in tools designed for rare diseases. Consequently, while items with a significant floor effect may be less sensitive to change in milder cases, they remain highly informative for assessing the symptom burden in individuals with more severe phenotypes.
QOLEB results confirmed the major disease impact on QoL with 39% of patients reporting severe to very severe effects. However, total QoL score varied widely (0 to 43), in line with the huge phenotypic EB spectrum. The mean value was 17.5, similar to the results obtained in the Spanish and Romanian patients (14, 16), but higher than those observed in Dutch EB individuals (12), and lower than in the German-speaking ones (18). Such differences may be due to the EB type and subtype distribution among respondents. Similar to findings in the Spanish and German-speaking EB patients (16, 18), women showed a tendency to have a worse QoL than men, with significant differences in the Emotions subscale score. Indeed, female sex was confirmed as an independent variable associated with higher scores on the Emotions subscale in multivariate linear regression analysis. The significantly worse QoL in young adults (18–30 years) as compared to patients between 11 and 18 years might be related to disease progression over time implying increased complications, functional damage and difficulties in social integration. Interestingly, survey participants who were members of a patients’ association were predominantly affected with the most severe EB subtypes, DEB and JEB, and reported markedly poorer QoL, particularly in the Functioning domain, even after multivariate linear regression analysis. This association likely reflects a “selection bias” (33), where individuals with more burdensome symptoms or complex psychosocial needs are more motivated to seek support and join such organizations, that serve as a crucial touchpoint for the most fragile patients. These data highlight the need for integrated clinical and social support strategies tailored to those with the highest disease burden. Among major EB types, the worst QoL was observed in DEB individuals, in particular for the Functioning subscale, in line with previous literature (12, 14, 16, 34). Significant differences between DEB and EBS and between JEB and EBS for total QOLEB and Functioning subscale scores are also observed in Dutch and Spanish populations (12, 16). These findings highlight the sensitivity of the QOLEB instrument in capturing specific disease aspects thus differentiating the various EB types.
We found that EB survey participants showed a strong correlation between the total disease severity score and the QOLEB total and Functioning scores, while the correlation with the Emotions subscale was scarce and not statistically significant. In line with these results, the normalized values of the Functioning scale were markedly lower in respondents with localized EB as compared with generalized disease, while the Emotions subscale scores were similar in the 2 groups. These findings indicate that the emotional life of patients is markedly affected independently from the level of clinical severity, in line with results in the German sample of the BUR-EB study, and in other chronic dermatological conditions (35, 36).
Pain and itch were reported by most individuals and strongly associated with worse QoL, measured by total QOLEB and both subscales, in all EB types (2, 3, 30, 31, 34, 37). Chronic wounds are the only clinical manifestation associated with a significant impact not only on total QOLEB and Functioning scores, but also on Emotions score, and staying as an independent variable for total QOLEB and Emotions subscale in multivariate regression analysis. The burden of chronic wounds is a major determinant of disease impact, due to pain and itch, risk for infections and SCC development, need for time-consuming and painful dressings, and also aesthetic damage (2, 3, 30, 38). Indeed, the presently approved therapies for EB are all meant to treat wounds (4). Moreover, malnutrition, mucosal involvement, tooth loss, joint deformities and functional disability, as well as wheelchair use, were significantly associated with higher scores for total QOLEB and the Functioning subscale. Wheelchair use was confirmed as an independent variable associated with higher total QOLEB and Functioning scores in multivariate linear regression analysis, reflecting the greater functional impairment in patients requiring this device.
Limitations
The present study has several limitations. The major one is represented by the relatively small sample that in a phenotypically heterogeneous disease may not completely reflect the overall EB population. In fact, while all EB types were represented, external validity is not easily verifiable and caution should be adopted when generalizing these results. In addition, our sample size (N=56) is below the conventional psychometric standard often recommended for the validation of self-report questionnaires, typically a 10 : 1 subjects-to-item ratio (39). However, achieving such numbers in rare diseases is challenging. Indeed, our sample size is consistent with, or even superior to, previous validation studies of QOLEB in different languages (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 16, 17, 18). A further limitation concerns the survey dissemination strategy through DEBRA Italy and reference centres and recruitment modality based on voluntary participation, which may have led to a self-selected over-representation of more severe EB forms, even within the specific clinical types. The considerable length of the questionnaire, as well as the online survey modality, may have also affected the composition of the study sample. However, paper questionnaires were available in reference centres for in-person completion.
Conclusion
Our study confirms the good psychometric properties of the Italian QOLEB, in line with previous studies in other populations (9, 11, 12, 13, 14, 15, 16, 17, 18). The Italian QOLEB allowed to document the overall major impact of EB on QoL, also highlighting gender differences in the emotional life, with a greater burden for women. It indicated pain, chronic wounds and functional disability as the main targets for therapeutic interventions to improve QoL of EB patients.
ACKNOWLEDGEMENTS
G.Z., T.S., A.D., D.A., M.E.H. are members of the European Reference Network for Rare Skin Diseases (ERN-Skin). The authors are grateful to DEBRA International and DEBRA Italia ETS for their support in designing the questionnaire, recruiting patients, and contributing to data collection. The authors also thank all participants, both patients and caregivers, for their time and commitment to the survey. Special thanks are extended to Rosa Caprioli, Lena Arnal-Artiaga and Vanessa Canosa-Acosta (Servicios Avanzados de Opinión, S.L.) for editing the questionnaires, and to Gabriele Bacile (OPBG) for figure preparation. The licenselicence for the Italian QOLEB belongs to the Australasian Blistering Diseases Foundation. BUR-EB Study Group (co-authors of this paper not listed): Olivia Mullins, DEBRA International, Austria. Ritu Jain, DEBRA International, Vienna, Austria. Georgi Iskrov, Bulgarian Association of Promotion of Education and Science (BAPES), Institute for Rare Diseases, Bulgaria; Medical University of Pleven, Bulgaria. Kostadin Dimitrov, Bulgarian Association of Promotion of Education and Science (BAPES), Institute for Rare Diseases, Bulgaria; Medical University of Pleven, Bulgaria. Georgi Stefanov, Bulgarian Association of Promotion of Education and Science (BAPES), Institute for Rare Diseases, Bulgaria; Medical University of Pleven, Bulgaria. Ivelina Yordanova, Bulgarian Association of Promotion of Education and Science (BAPES), Institute for Rare Diseases, Bulgaria; Medical University of Plovdiv, Bulgaria. Elena Eneva, Association Epidermolysis Bullosa Bulgaria (ABE Bulgaria), Bulgaria. Rumen Stefanov, Bulgarian Association of Promotion of Education and Science (BAPES), Institute for Rare Diseases, Bulgaria; Medical University of Plovdiv, Bulgaria. Christine Bodemer, Necker Enfants Malades Hospital (NEMH), Paris, France. Catherine Champseix, Necker Enfants Malades Hospital (NEMH), Paris, France. Hélène Dufresne, Necker Enfants Malades Hospital (NEMH), Paris, France. Smail HadjRabia, Necker Enfants Malades Hospital (NEMH), Paris, France. Cristina Has, Universitätsklinikum Freiburg (UKF), Germany. Vinzenz Hübl, Universitätsklinikum Freiburg (UKF), Germany. Márta Péntek, Health Economics Research Center (HECON), University Research and Innovation Center, Obuda University, Hungary. László Gulácsi, Health Economics Research Center (HECON), University Research and Innovation Center, Obuda University, Hungary. Zsombor Zrubka, Health Economics Research Center (HECON), University Research and Innovation Center, Obuda University, Hungary. Áron Hölgyesi, Health Economics Research Center (HECON), University Research and Innovation Center, Obuda University, Hungary. Márta Medvecz, Department of Dermatology, Venereology and Dermatooncology, Semmelweis University, Hungary. Lidia García-Pérez, Fundación Canaria Instituto de Investigación Sanitaria (FIISC), Spain. Alezandra Torres-Castaño, Fundación Canaria Instituto de Investigación Sanitaria (FIISC), Spain. Ana Toledo-Chávarri, Fundación Canaria Instituto de Investigación Sanitaria (FIISC), Spain. Aránzazu Hernández-Yumar, Fundación Canaria Instituto de Investigación Sanitaria (FIISC), Spain. Carmen Guirado-Fuentes, Fundación Canaria Instituto de Investigación Sanitaria (FIISC), Spain. Cristina Valcárcel-Nazco, Fundación Canaria Instituto de Investigación Sanitaria (FIISC), Spain. Yolanda Ramallo-Fariña, Fundación Canaria Instituto de Investigación Sanitaria (FIISC), Spain. Verónica Alonso-Ferreira, Instituto de Investigación de enfermedades Raras (IIER), Instituto de Salud Carlos III, Spain. Juan Benito-Lozano, Instituto de Investigación de enfermedades Raras (IIER), Instituto de Salud Carlos III, Spain. Mario Gómez-Martínez, Instituto de Investigación de enfermedades Raras (IIER), Instituto de Salud Carlos III, Spain. Ana Villaverde-Hueso, Instituto de Investigación de enfermedades Raras (IIER), Instituto de Salud Carlos III, Spain.
Greta Arias-Merino, Instituto de Investigación de enfermedades Raras (IIER), Instituto de Salud Carlos III, Spain
REFERENCES
- Has C, Bauer JW, Bodemer C, Bolling MC, Bruckner-Tuderman L, Diem A, et al. Consensus reclassification of inherited epidermolysis bullosa and other disorders with skin fragility. Br J Dermatol 2020; 183: 614–627. https://doi.org/10.1111/bjd.18921
- Bardhan A, Bruckner-Tuderman L, Chapple ILC, Fine JD, Harper N, Has C, et al. Epidermolysis bullosa. Nat Rev Dis Primers 2020; 6: 78. https://doi.org/10.1038/s41572-020-0210-0
- Has C, El Hachem M, Bučková H, Fischer P, Friedová M, Greco C, et al. Practical management of epidermolysis bullosa: Consensus clinical position statement from the European Reference Network for Rare Skin Diseases. J Eur Acad Dermatol Venereol 2021; 35: 2349–2360. https://doi.org/10.1111/jdv.17629
- Lucky AW, Pope E, Crawford S. Dystrophic epidermolysis bullosa. 2006 (updated 2025). In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews®. Seattle (WA): University of Washington, Seattle; 1993 (updated 2026).
- Chernyshov PV. The evolution of quality of life assessment and use in dermatology. Dermatology 2019; 235: 167–174. https://doi.org/10.1159/000496923
- Finlay AY, Salek MS, Abeni D, Tomás-Aragonés L, van Cranenburgh OD, Evers AWM, et al. Why quality of life measurement is important in dermatology clinical practice: An expert-based opinion statement by the EADV Task Force on Quality of Life. J Eur Acad Dermatol Venereol 2017; 31: 424–431. https://doi.org/10.1111/jdv.13985
- Snyder AM, Chen SC, Chren MM, Ferris LK, Edwards LD, Swerlick RA, et al. Patient-reported outcome measures and their clinical applications in dermatology. Am J Clin Dermatol 2023; 24: 499–511. https://doi.org/10.1007/s40257-023-00758-8
- Chernyshov PV, Finlay AY, Tomas‐Aragones L, Poot F, Murrell DF, Pustisek N, et al. Quality‐of‐life measurement in epidermolysis bullosa. Position statement of the European Academy of Dermatology and Venereology Task Force on quality of life and patient‐oriented outcomes and external experts. Int J Dermatology 2025; 64: 1546–1557. https://doi.org/10.1111/ijd.17668
- Frew JW, Martin LK, Nijsten T, Murrell DF. Quality of life evaluation in epidermolysis bullosa (EB) through the development of the QOLEB questionnaire: An EB-specific quality of life instrument. Br J Dermatol 2009; 161: 1323–1330. https://doi.org/10.1111/j.1365-2133.2009.09347.x
- Arias-Merino G, Benito-Lozano J, Gómez-Martinez M, Villaverde-Hueso A, Linertová R, Alonso-Ferreira V. Health-related quality-of-life evaluation in epidermolysis bullosa: A scoping review. Br J Dermatol 2025; 193: 856–864. https://doi.org/10.1093/bjd/ljaf274
- Frew JW, Cepeda Valdes R, Fortuna G, Murrell DF, Salas Alanis J. Measuring quality of life in epidermolysis bullosa in Mexico: Cross-cultural validation of the Hispanic version of the Quality of Life in Epidermolysis Bullosa questionnaire. J Am Acad Dermatol 2013; 69: 652–653. https://doi.org/10.1016/j.jaad.2013.04.053
- Yuen WY, Frew JW, Veerman K, van den Heuvel ER, Murrell DF, Jonkman MF. Health-related quality of life in epidermolysis bullosa: Validation of the Dutch QOLEB questionnaire and assessment in the Dutch population. Acta Derm Venereol 2014; 94: 442–447. https://doi.org/10.2340/00015555-1758
- Cestari T, Prati C, Menegon DB, Prado Oliveira ZN, Machado MCR, Dumet J, et al. Translation, cross-cultural adaptation and validation of the Quality of Life Evaluation in Epidermolysis Bullosa instrument in Brazilian Portuguese. Int J Dermatol 2016; 55: e94–9. https://doi.org/10.1111/ijd.12819
- Dănescu S, Sălăvăstru C, Sendrea A, Tiplica S, Baican A, Ungureanu L, et al. Correlation between disease severity and quality of life in patients with epidermolysis bullosa. J Eur Acad Dermatol Venereol 2019; 33: e217–e219. https://doi.org/10.1111/jdv.15371
- Yazdanshenas A, Naderi E, Moravvej H, Heidari K, Faghankhani M, Vahidnezhad H, et al. The quality of life in epidermolysis bullosa (EB-QoL) questionnaire: Translation, cultural adaptation, and validation into the Farsi language. Int J Womens Dermatol 2020; 6: 301–305. https://doi.org/10.1016/j.ijwd.2020.05.012
- Villar Hernández AR, Molero Alonso F, Aguado Marín ÁJ, Posada de la Paz M. Transcultural Validation of a Spanish Version of the Quality of Life in Epidermolysis Bullosa Questionnaire. Int J Environ Res Public Health 2022; 19: 7059. https://doi.org/10.3390/ijerph19127059
- Bishnoi A, Manjunath S, Kishore K, De D, Handa S, Murrell DF, et al. Hindi translation and validation of quality of life score in Indian patients with epidermolysis bullosa; and its correlation with the clinical severity assessment scores: A cross-sectional study. Indian J Dermatol Venereol Leprol 2022; 88: 177–183. https://doi.org/10.25259/IJDVL_31_20
- Salamon G, Strobl S, Field-Werners U, Welponer T, Murrell DF, Diem A. Translation, cultural adaptation and validation of the German Quality of Life in Epidermolysis Bullosa (QOLEB) questionnaire. J Health Psychol 2025; 30: 1476–1490. https://doi.org/10.1177/13591053231221369
- El Hachem M, Diociaiuti A, Zambruno G, Samela T, Ferretti F, Carnevale C, et al. “Quality of Life in Epidermolysis Bullosa” and “Epidermolysis Bullosa Burden of Disease”: Italian translation, cultural adaptation, and pilot testing of two disease-specific questionnaires. Ital J Pediatr 2024; 50: 76. https://doi.org/10.1186/s13052-024-01657-2
- Arias-Merino G, Benito-Lozano J, Linertová R, Alonso-Ferreira V, on behalf the BUR-EB Study Group. Health-related quality-of-life evaluation in epidermolysis bullosa: A scoping review protocol. Syst Rev 2025; 14: 159. https://doi.org/10.1186/s13643-025-02918-9
- Geroldinger M, Verbeeck J, Hooker AC, Thiel KE, Molenberghs G, Nyberg J, et al. Statistical recommendations for count, binary, and ordinal data in rare disease cross-over trials. Orphanet J Rare Dis 2023; 18: 391. https://doi.org/10.1186/s13023-023-02990-1
- Frew J, Murrell DF. Improving clinical applications of quality of life scores in epidermolysis bullosa: Defining clinically significant outcomes in the QOLEB questionnaire. Mucosa 2019; 2: 68–75. https://doi.org/10.33204/mucosa.598339
- Devlin N, Parkin D, Janssen B. Methods for Analysing and Reporting EQ-5D Data. 1st edn. Cham: Springer; 2020.
- Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J Clin Epidemiol 1993; 46: 1417–1432. https://doi.org/10.1016/0895-4356(93)90142-n
- Karakaya SPY, Alparslan ZN. Sample size in reliability studies: A practical guide based on Cronbach’s alpha. PBS 2022; 12: 150. https://doi.org/10.5455/PBS.20220127074618
- Terwee CB, Bot SDM, de Boer MR, van der Windt DAWM, Knol DL, Dekker J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol 2007; 60: 34–42. https://doi.org/10.1016/j.jclinepi.2006.03.012
- Finch AP, Meregaglia M, Ciani O, Roudijk B, Jommi C. An EQ-5D-5L value set for Italy using videoconferencing interviews and feasibility of a new mode of administration. Soc Sci Med 2022; 292: 114519. https://doi.org/10.1016/j.socscimed.2021.114519
- Pérez-Sousa MÁ, Olivares PR, Ramírez-Vélez R, Gusi N. Comparison of the psychometric properties of the EQ-5D-3L-Y and EQ-5D-5L-Y instruments in Spanish children and adolescents. Value Health 2021; 24: 1799–1806. https://doi.org/10.1016/j.jval.2021.07.006
- Hancock KJ, Glass N, Anthony CA, Hettrich CM, Albright J, Amendola A, et al. Performance of PROMIS for healthy patients undergoing meniscal surgery. J Bone Joint Surg Am 2017; 99: 954–958. https://doi.org/10.2106/JBJS.16.00848
- Bruckner AL, Losow M, Wisk J, Patel N, Reha A, Lagast H, et al. The challenges of living with and managing epidermolysis bullosa: Insights from patients and caregivers. Orphanet J Rare Dis 2020; 15: 1. https://doi.org/10.1186/s13023-019-1279-y
- So JY, Fulchand S, Wong CY, Li S, Nazaroff J, Gorell ES, et al. A global, cross-sectional survey of patient-reported outcomes, disease burden, and quality of life in epidermolysis bullosa simplex. Orphanet J Rare Dis 2022; 17: 270. https://doi.org/10.1186/s13023-022-02433-3
- Slauson‐Blevins K, Johnson KM. Doing gender, doing surveys? Women’s gatekeeping and men’s non‐participation in multi‐actor reproductive surveys. Sociol Inq 2016; 86: 427–449. https://doi.org/10.1111/soin.12122
- Lu H, Cole SR, Howe CJ, Westreich D. Toward a clearer definition of selection bias when estimating causal effects. Epidemiology (Sunnyvale) 2022; 33: 699–706. https://doi.org/10.1097/EDE.0000000000001516
- Tang JY, Marinkovich MP, Lucas E, Gorell E, Chiou A, Lu Y, et al. A systematic literature review of the disease burden in patients with recessive dystrophic epidermolysis bullosa. Orphanet J Rare Dis 2021; 16: 175. https://doi.org/10.1186/s13023-021-01811-7
- Hübl V, Strobl S, Salamon G, Has C, Group BS. The puzzling effect of disease severity on quality of life in epidermolysis bullosa. J Eur Acad Dermatol Venereol 2025. https://doi.org/10.1111/jdv.70191
- Samela T, Raimondi G, Pintori G, Pupa MB, Cordella G, Antinone V, et al. Clinically mild hidradenitis suppurativa: Mild for whom? Br J Dermatol 2024; 191: 1026–1027. https://doi.org/10.1093/bjd/ljae310
- Jeffs E, Pillay EI, Ledwaba-Chapman L, Bisquera A, Robertson SJ, McGrath JA, et al. Pain in recessive dystrophic epidermolysis bullosa (RDEB): Findings of the Prospective Epidermolysis Bullosa Longitudinal Evaluation Study (PEBLES). Orphanet J Rare Dis 2024; 19: 375. https://doi.org/10.1186/s13023-024-03349-w
- Eng VA, Solis DC, Gorell ES, Choi S, Nazaroff J, Li S, et al. Patient-reported outcomes and quality of life in recessive dystrophic epidermolysis bullosa: A global cross-sectional survey. J Am Acad Dermatol 2021; 85: 1161–1167. https://doi.org/10.1016/j.jaad.2020.03.028
- Zhao Y, Summers R, Gathara D, English M. Conducting cross-cultural, multi-lingual or multi-country scale development and validation in health care research: A 10-step framework based on a scoping review. J Glob Health 2024; 14: 04151. https://doi.org/10.7189/jogh.14.04151