QUIZ SECTION
A Congenital Subcutaneous Tumour of the Scalp in a Child: A Quiz
Haruka MUKAI1, Yuto YAMAMURA1*![]() , Kazuyasu FUJII1, Shunya USUI1 and Atsushi OTSUKA1
, Kazuyasu FUJII1, Shunya USUI1 and Atsushi OTSUKA1
1Department of Dermatology, Kindai University Hospital, Osaka, Japan. *Email: 220196@med.kindai.ac.jp
Citation: Acta Derm Venereol 2026; 106: adv-2026-0401. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0401.
Copyright: 2026 ©Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Accepted after revision:
Published: Jul 1, 2026.
Competing interests and funding:
A 12-year-old girl presented to our department with a subcutaneous mass on the occipital scalp. She had no remarkable past medical history or family history. According to her family, the lesion had been noticed since birth and had gradually increased in size without associated symptoms. On physical examination, a well-circumscribed, elastic-soft subcutaneous mass measuring approximately 4 cm in diameter was observed on the occipital region (Fig. 1A). The lesion was freely movable over both the overlying skin and the underlying skull. There were no signs of inflammation, including erythema, spontaneous pain or tenderness.
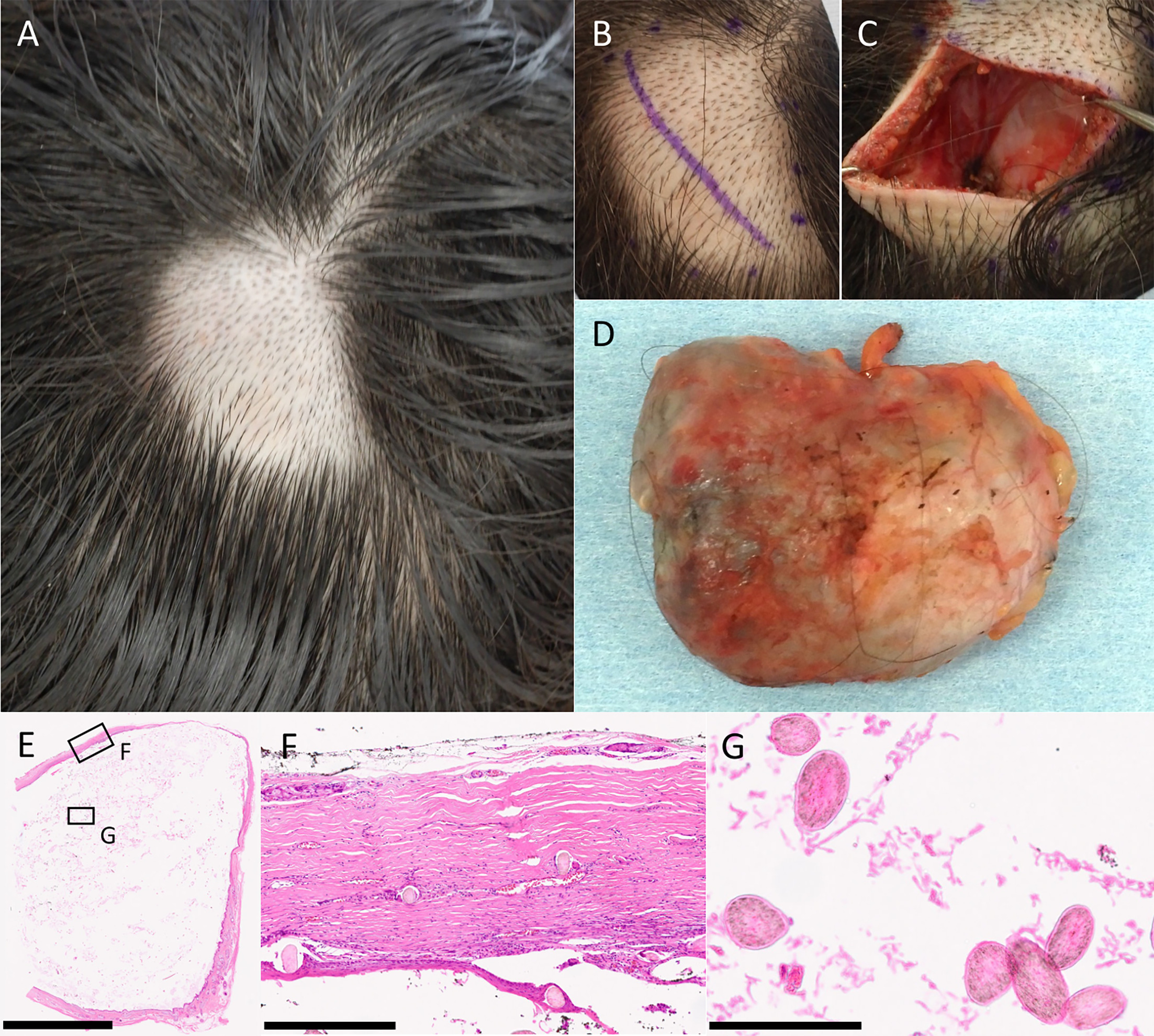
Fig. 1. Clinical and histopathological findings. (A) Subcutaneous tumour measuring approximately 4 cm in maximum diameter on the occipital scalp, freely movable over the overlying skin and underlying tissues. (B) Surgical excision via a direct skin incision; the tumour was well encapsulated. (C) the tumour base extended to the level of the galea aponeurotica. (D) Gross appearance of the excised specimen measuring approximately 4 cm in maximum diameter, well encapsulated without adhesion to surrounding tissues. (E) Low-power view (hematoxylin and eosin stain) showing a well-circumscribed intradermal cyst containing keratinous material and hairs. (F) High-power view demonstrating a cyst wall composed of stratified squamous epithelium with a well-formed granular layer. The rounded structures in the cyst wall were interpreted as cross-sections of vellus hair shafts, and no mature adnexal structures, such as sebaceous glands, eccrine glands or well-developed hair follicles, were identified. (G) Laminated keratinous material and numerous vellus hairs within the cyst lumen. Scale bars: 10 mm (E), 500 µm (F), 250 µm (G).
Based on the clinical findings, the lesion was considered a benign subcutaneous tumour, and complete surgical excision was performed under general anaesthesia (Fig. 1B). Intraoperatively, the tumour was well encapsulated and located above the galea aponeurotica. No adhesion to or invasion of the surrounding tissues was observed (Fig. 1C and D). The postoperative course was uneventful, and no complications or recurrence have been noted to date.
The excised specimen was subsequently subjected to histopathological examination, which was essential for establishing the correct diagnosis.
What is your diagnosis?
1: Epidermal cyst.
2: Dermoid cyst.
3: Vellus hair cyst.
4: Pilar cyst (trichilemmal cyst).
See next page for answer.
ANSWERS TO QUIZ
A Congenital Subcutaneous Tumour of the Scalp in a Child: A Quiz
Diagnosis: Vellus hair cyst.
Vellus hair cyst (VHC) is a benign follicular cystic disorder characterized by the presence of laminated vellus hairs within the cyst lumen (1). Clinically, VHC most commonly develops after puberty and typically presents as multiple papules or nodules on the trunk, extremities or face, a presentation often referred to as eruptive VHC. The majority of reported cases fall into this eruptive, multifocal category. Histopathologically, VHC is characterized by a cyst wall composed of stratified squamous epithelium with a well-formed granular layer and a lumen filled with laminated keratinous material and numerous vellus hairs. In contrast, solitary VHC is extremely rare, with only a very limited number of cases reported to date.
In paediatric patients, subcutaneous tumours arising on the scalp encompass a broad differential diagnosis, including pilar (trichilemmal) cysts, dermoid cysts and epidermal cysts (2, 3). Pilar cysts are benign tumours that preferentially occur on the scalp and are derived from the outer root sheath of the hair follicle. Histologically, they are characterized by trichilemmal keratinization and the absence of a granular layer, which clearly distinguishes them from VHC (2). Epidermal cysts are common benign subcutaneous lesions that may also occur on the scalp in children. Histopathologically, they are lined by stratified squamous epithelium and contain laminated keratin; however, they lack cutaneous adnexal structures such as hair follicles or sebaceous glands, allowing differentiation from VHC (3). Dermoid cysts represent congenital lesions that may occur on the head in paediatric patients. Although hair shafts may be present within the cyst lumen, dermoid cysts are characterized by the presence of multiple adnexal structures, including hair follicles, sebaceous glands and sweat glands, within the cyst wall (3). The absence of such adnexal structures in VHC allows clear histopathological distinction. Conversely, recent reports have described cases diagnosed as vellus hair cysts despite atypical histological findings, such as the presence of vellus hairs within the cyst wall, highlighting that some degree of diagnostic ambiguity may exist in rare presentations (4).
In the present case, all of the abovementioned benign subcutaneous tumours were considered in the clinical differential diagnosis. However, VHC is not generally recognized as a congenital subcutaneous tumour of the scalp, making preoperative clinical diagnosis particularly challenging. VHC most commonly affects the trunk, extremities and face (1), and to the best of our knowledge, no clearly documented cases of VHC arising on the scalp have been reported. Although congenital onset of VHC has been sporadically described, such cases are exceedingly rare (5). Furthermore, when limited to solitary VHC, there have been no previous reports of lesions presenting either congenitally or on the scalp. From this perspective, the present case represents an exceptionally rare clinical presentation.
The final diagnosis was established based on histopathological examination of the excised specimen. The key diagnostic features were a well-circumscribed dermal cyst lined by stratified squamous epithelium with a granular layer and numerous laminated vellus hairs within the cyst lumen (1). Although rounded structures were observed in the cyst wall on high-power examination, these were interpreted as cross-sections of vellus hair shafts rather than adnexal structures. No mature adnexal structures, such as sebaceous glands, eccrine glands or well-developed hair follicles, were identified in the cyst wall.
In conclusion, the present case represents an extremely rare form of VHC with a solitary, congenital presentation on the scalp. This report highlights the importance of including solitary VHC in the histopathological differential diagnosis of congenital subcutaneous tumours of the scalp in paediatric patients.
REFERENCES
- Torchia D, Vega J, Schachner LA. Eruptive vellus hair cysts: a systematic review. Am J Clin Dermatol 2012; 13: 19–28. https://doi.org/10.2165/11589050-000000000-00000
- Ramaswamy AS, Manjunatha HK, Sunilkumar B, Arunkumar SP. Morphological spectrum of pilar cysts. N Am J Med Sci 2013; 5: 124–128. https://doi.org/10.4103/1947-2714.107532
- Prior A, Anania P, Pacetti M, Secci F, Ravegnani M, Pavanello M, et al. Dermoid and epidermoid cysts of scalp: case series of 234 consecutive patients. World Neurosurg 2018; 120: 119–124. https://doi.org/10.1016/j.wneu.2018.08.197
- Ghosh Moulic A, Deshmukh P, Gaurkar SS. A facial solitary vellus hair cyst: a rare entity. Cureus 2024; 16: e54159. https://doi.org/10.7759/cureus.54159
- Piepkorn MW, Clark L, Lombardi DL. A kindred with congenital vellus hair cysts. J Am Acad Dermatol 1981; 5: 661–665. https://doi.org/10.1016/s0190-9622(81)70127-0