SHORT COMMUNICATION
Actinic Folliculitis (Formerly Acne Aestivalis and Mallora Acne): A Report of 18 Patients and Review of the Literature
Mario MANISCALCO1, Laura MANISCALCO1, Italo Francesco AROMOLO2![]() , Gianluca NAZZARO2
, Gianluca NAZZARO2![]() and Stefano VERALDI3*
and Stefano VERALDI3*![]()
1Studiodermomaniscalco, Sciacca, Italy, 2Department of Pathophysiology and Transplantation, Università degli Studi, IRCCS Foundation, Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy, and 3Dermatological Centre in Milan, Milan, Italy. *Email: stefano.veraldi@dcim.it
Citation: Acta Derm Venereol 2026; 106: adv-2026-0423. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0423.
Copyright: 2026 ©Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 15, 2026. Accepted after revision: Jun 29, 2026.
Published: Jul 9, 2026.
Competing interests and funding: The authors have no conflicts of interest to declare.
Anonymized data will be shared upon reasonable request from any qualified investigator for purposes of replicating procedures and results.
In accordance with the guidelines of our institutions ethics committee, and given the nature of the study, formal approval was not required.
In 1972, Hjorth et al. (1) coined the term acne aestivalis/Mallorca acne to describe an acneiform eruption that occurred in a group of 40 patients, 37 of them were females, aged 20–40 years, with a negative medical history of acne. The eruption appeared 15–30 days after sun exposure, without the use of sunscreens. It was characterized by papules, with rare comedones and pustules, located on the face, neck, shoulders, upper trunk and upper limbs. Histopathological picture was characterized by follicular keratosis. The arms eruption lasted 3–6 months.
The name of acne aestivalis was subsequently used by other authors (2, 3, 4, 5, 6, 7). The term solar acne or acne solaris was also suggested (8). It was hypothesized that acne aestivalis was, simply, acne aggravated by sunlight (9). In 1985, Nieboer suggested the name of actinic superficial folliculitis (10). The latter was used by other authors (11, 12, 13), although the name actinic folliculitis and recurrent photosensitive pustular eruption were also suggested (14, 15, 16, 17, 18, 19).
Review of the literature revealed that, on the basis of clinical presentations and histopathological pictures, all these 3 entities, acne aestivalis/Mallorca acne, actinic superficial folliculitis and actinic folliculitis, are the same disease. As the term of acne aestivalis/Mallorca acne is rather old, we agree to name this entity actinic folliculitis (AF).
We present 18 patients with AF: to our knowledge, this is one of the largest caselists reported so far.
CASE REPORTS
From 1987 to 2025, we observed 18 Caucasian patients, 5 males and 13 females, with an age ranging from 19 to 37 years (mean age: 22.3 years) with AF. Four patients (2 males and 2 females) were affected by acne. According to medical history, latency time from sun exposure to the appearance of the first skin lesions ranged from 12 to 72 h. Patients’ characteristics are reported in Table I. In all patients the eruption was characterized by roundish, erythematous papules and pustules, of a few millimetres in diameter, located on the face (Fig. 1a, b and c), neck (Fig. 1b), shoulders (Fig. 2a and b), chest (Fig. 2b) and upper portion of the back. In addition, the upper limbs were involved in 2 patients (Fig. 2c). Nine patients complained of mild itching. In 12 patients, AF was recurrent. Laboratory tests were carried out in all patients: in 4 of them, mild leukocytosis and increase in erythrocyte sedimentation rate were detected. In 4 patients, bacteriological examinations of pustular lesions were negative for aerobic and anaerobic bacteria. In 8 patients, patch tests and photopatch tests with the SIDAPA baseline series (Società Italiana di Dermatologia Allergologica, Professionale e Ambientale) were negative. Three patients were subjected to biopsy. Histopathological examination was superimposable in all patients: it showed foci of necrosis in the upper dermis and a perivascular and perifollicular infiltrate consisting of neutrophils, lymphocytes and histiocytes. Ten patients were treated with the fixed combination 0.1% adapalene/2.5% benzoyl peroxide gel, 4 patients with 0.005% retinaldehyde cream and 4 patients with 0.05% tretinoin cream. In all patients, complete remission was observed within 4 months (Table I).
Table I. Actinic Folliculitis: patients’ characteristics in our case series
| N. | Gender | Age, years | Time to onset, hours | Time to remission | Recurrences | Therapy |
|---|---|---|---|---|---|---|
| 1 | F | 19 | 18–36 | 3 weeks | Yes | Adapalene/benzoyl peroxide gel |
| 2 | M | 22 | 24 | 3 weeks | Yes | Adapalene/benzoyl peroxide gel |
| 3 | F | 25 | 18 | 4 weeks | No | Adapalene/benzoyl peroxide gel |
| 4 | F | 23 | 24 | 4 months | Yes | Retinaldehyde cream |
| 5 | F | 17 | 12–24 | 4 weeks | Yes | Adapalene/benzoyl peroxide gel |
| 6 | M | 23 | 32 | 3 weeks | No | Adapalene/benzoyl peroxide gel |
| 7 | M | 26 | 24 | 2 months | No | Retinaldehyde cream |
| 8 | F | 19 | 18–36 | 4 weeks | Yes | Adapalene/benzoyl peroxide gel |
| 9 | M | 20 | 24–72 | 2 months | No | Retinaldehyde cream |
| 10 | M | 21 | 12–18 | 4 weeks | Yes | Adapalene/benzoyl peroxide gel |
| 11 | F | 24 | 24 | 2 months | No | Retinaldehyde cream |
| 12 | F | 27 | 24 | 3 weeks | Yes | Adapalene/benzoyl peroxide gel |
| 13 | F | 20 | 18–24 | 3 weeks | No | Tretinoin cream |
| 14 | F | 19 | 12–18 | 3 weeks | Yes | Tretinoin cream |
| 15 | F | 37 | 36 | 3 weeks | Yes | Adapalene/benzoyl peroxide gel |
| 16 | F | 21 | 24 | 4 weeks | Yes | Adapalene/benzoyl peroxide gel |
| 17 | F | 18 | 36 | 3 weeks | Yes | Tretinoin cream |
| 18 | F | 21 | 24 | 3 weeks | Yes | Tretinoin cream |
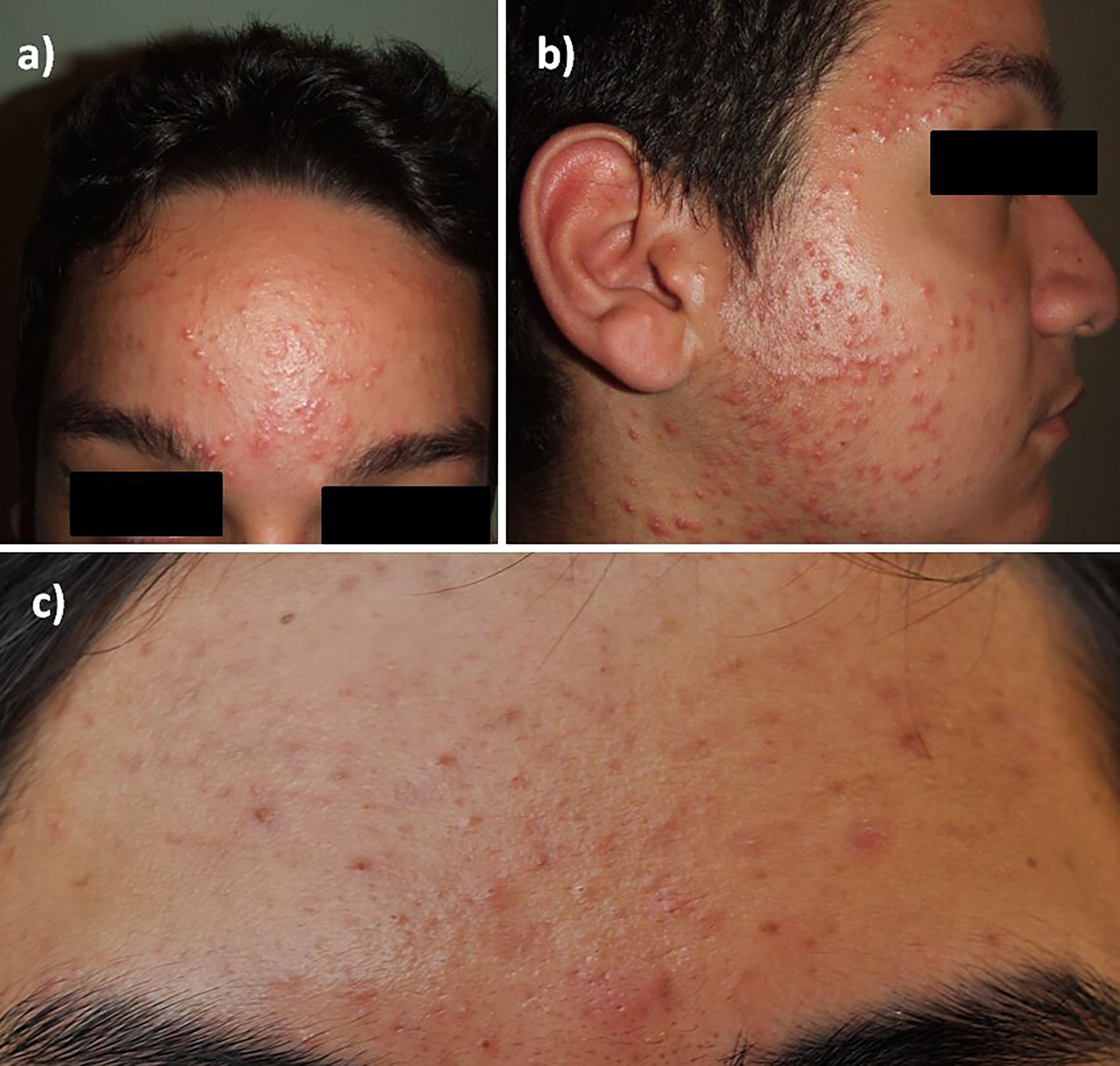
Fig. 1. Different patients with actinic folliculitis: Erythematous papules on the forehead (A,C); Erythematous papules on the temple, cheek and neck (B).
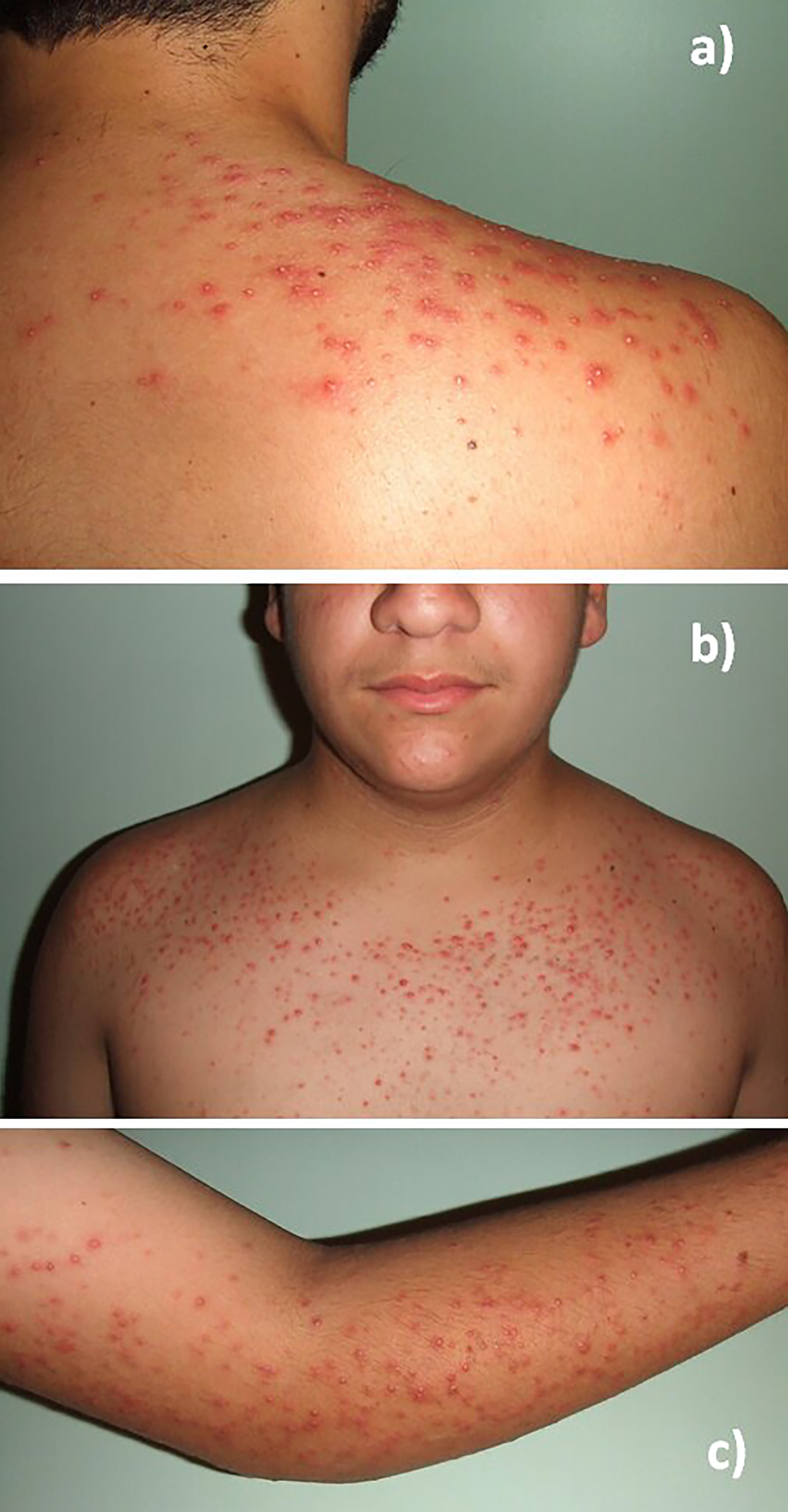
Fig. 2. Different patients with actinic folliculitis: Erythematous papules and pustules on the shoulder (A); Erythematous papules on the shoulders and chest (B); Erythematous papules and pustules on the upper limb (C).
DISCUSSION
AF mainly occurs in adult females (2, 4, 10, 14, 15, 16, 17, 18), although some males were observed (4, 10, 11, 12, 13, 14). Seborrhea (4) and the use of oily sunscreens that cause obstruction of the follicles (8) were suggested as possible predisposing factors; although, in the caselist by Hjorth et al. (1), sunscreens were not used. In addition, we cannot exclude the role of hot-humid weather, hyperhidrosis and sweating.
Latency time from the sunlight exposure to the appearance of the first skin lesions is extremely changeable: from 15 min to 3 weeks (18), to 4–6 h (16), 4–24 h (17), 6–24 h (15), 24–36 h (10, 12, 13), 48–72 h (11), up to 15–30 days (1). As previously mentioned, in our group of patients, time to onset ranged from 12 to 72 h.
AF is characterized by follicular, erythematous papules (1, 2, 4, 5, 8, 9, 14, 15, 17, 18) and pustules (1, 5, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18), with rare comedones (1, 5, 9), located on the face (1, 3, 5, 9, 15, 16, 17, 18), neck (1, 3, 4, 5, 10, 11, 18), shoulders (1, 3, 5, 8, 10, 11, 12, 13, 14), chest (3, 4, 5, 8, 12, 13, 17, 18), upper portion of the back (3, 4, 10, 11, 12, 13, 18) and upper arms (1, 3, 4, 5, 8, 10, 11, 14, 17, 18). Rare locations are breasts (10), buttocks (3), thighs (18) and legs (3). The lesions are sometimes accompanied by itching (8, 18). Based on this clinical picture, AF was considered similar to steroid acne (2, 5) or a clinical variant of polymorphous light eruption (5). A recently reported clinical entity, which was named acute and recurrent pustulosis, differs from AF for several reasons: it occurs almost exclusively in young women; sun exposure is not always the trigger; it is characterized almost exclusively by pustules; time to resolution is very short; treatment is unnecessary; it is almost always recurrent (20). Several drugs were used for the treatment of AF, such as benzoyl peroxide (4, 5), tretinoin (2, 4, 5), adapalene (17), topical corticosteroids (8) and isotretinoin (15, 17). Remission occurs at very variable times: from 3 days (15), to 5–7 days (11, 13), to 7–10 days (10, 17), to 3 months (14), to 3–6 months (1, 4). Recurrences are rather common (13, 17): some authors suggested, in patients with recurrent AF, a prophylaxis with UVA (5) or UVB (5), either alone (5) or in combination (5) or narrow-band-UVB (18) or PUVA (5). In summary: a) AF is an acneiform eruption induced by the exposure to sunlight; b) Caucasian, adult females are more frequently involved; c) latency time is extremely variable, from a few hours to weeks; d) erythematous papules and pustules, located on the face, neck, shoulders, chest, upper portion of the back and upper arms are the most frequently observed lesions; e) several drugs are effective, although remission occurs from a few days to some months; f) recurrences are rather common and g) prophylaxis with phototherapy is helpful.
REFERENCES
- Hjorth N, Sjolin KE, Sylvest B, Thomsen K. Acne aestivalis--Mallorca acne. Acta Derm Venereol 1972; 52: 61–63.
- Mills OH Jr, Kligman AM. Acne aestivalis. Arch Dermatol 1975; 111: 891–892.
- Sjølin KE. Acne aestivalis. A histopathological study. Acta Derm Venereol Suppl 1979; 59: 171–176.
- Petruzzellis V, Scardigno A, Velon A. Contributo alla conoscenza dell’acne aestivalis. G Ital Dermatol Venereol 1986; 121: 55–60.
- Plewig G, Jansen T. Acneiform dermatoses. Dermatology 1998; 196: 102–107. https://doi.org/10.1159/000017841
- Jansen T. Was hat sie sich in Nordafrika gefangen? MMW - Fortschritte Der Medizin 2015; 157: 5–5. https://doi.org/10.1007/s15006-015-2788-9
- Rippke F, Wendt G, Bohnsack K, Dörschner A, Stäb F, Hölzle E, et al. Results of photoprovocation and field studies on the efficacy of a novel topically applied antioxidant in polymorphous light eruption. J Dermatolog Treat 2001; 12: 3–8. https://doi.org/10.1080/095466301750163491
- Padilha-Gonçalves A, Alvimar Ferreira J. Solar acne. Med Cutan Ibero Lat Am 1977; 5: 271–274.
- Allen HB, LoPresti PJ. Acne vulgaris aggravated by sunlight. Cutis 1980; 26: 254–256.
- Nieboer C. Actinic superficial folliculitis; a new entity? Br J Dermatol 1985; 112: 603–606. https://doi.org/10.1111/j.1365-2133.1985.tb15271.x
- Labandeira J, Suarez-Campos A, Toribio J. Actinic superficial folliculitis. Br J Dermatol 1998; 138: 1070–1074. https://doi.org/10.1046/j.1365-2133.1998.02283.x
- Jaeger C, Hartschuh W, Jappe U. Actinic superficial folliculitis. J Eur Acad Dermatol Venereol 2003; 17: 562–565. https://doi.org/10.1046/j.1468-3083.2003.00816.x
- LaBerge L, Glassman S, Kanigsberg N. Actinic superficial folliculitis in a 29-year-old man. J Cutan Med Surg 2012; 16: 191–193. https://doi.org/10.1177/120347541201600310
- Verbov J. Actinic folliculitis. Br J Dermatol 1985; 113: 630–631. https://doi.org/10.1111/j.1365-2133.1985.tb02392.x
- Norris PG, Hawk JL. Actinic folliculitis--response to isotretinoin. Clin Exp Dermatol 1989; 14: 69–71. https://doi.org/10.1111/j.1365-2230.1989.tb00889.x
- Veysey EC, George S. Actinic folliculitis. Clin Exp Dermatol 2005; 30: 659–661. https://doi.org/10.1111/j.1365-2230.2005.01899.x
- Rahman S, Powell J, Al-Ismail D. First reported cases of actinic folliculitis treated successfully with topical retinoid. Clin Exp Dermatol 2020; 45: 716–718. https://doi.org/10.1111/ced.14179
- Butt S, Dawe R, Blair R, Ibbotson S. A new approach to actinic folliculitis: prophylactic narrowband ultraviolet B phototherapy. Clin Exp Dermatol 2021; 46: 675–679. https://doi.org/10.1111/ced.14518
- Brokamp G, Chung CG. Recurrent photosensitive pustular eruption in a young woman. JAMA Dermatol 2022; 158: 204–205. https://doi.org/10.1001/jamadermatol.2021.5383
- Porter AP, James WD. Acute and recurrent pustulosis: consolidating uncommon cases of follicular pustulosis induced by UV light and other triggers. Int J Womens Dermatol 2023; 9: e100. https://doi.org/10.1097/JW9.0000000000000100