REVIEW ARTICLE
The Role of RCM and LC-OCT in Genodermatoses Associated with Skin Cancer: A Narrative Review
Francesco PISCAZZI1,2![]() , Cristina CARRERA3,4
, Cristina CARRERA3,4![]() , Josep RIERA-MONROIG3
, Josep RIERA-MONROIG3![]() , Susana PUIG3,4
, Susana PUIG3,4![]() , Josep MALVEHY3,4
, Josep MALVEHY3,4![]() , Javiera ANKER3,4
, Javiera ANKER3,4![]() and Marco ARDIGÒ1,2*
and Marco ARDIGÒ1,2*![]()
1Department of Biomedical Sciences, Humanitas University, Pieve Emanuele (MI), Italy, 2Dermatology Unit, IRCCS Humanitas Research Hospital, Rozzano (MI), Italy, 3Department of Dermatology, Hospital Clínic de Barcelona, Barcelona University, Barcelona, Spain, and 4Melanoma Unit, Dermatology Department, Hospital Clínic de Barcelona, IDIBAPS, Barcelona, Spain
Corr: Marco Ardigò, Dermatology Unit, IRCCS Humanitas Research Hospital, Via Alessandro Manzoni, 56, 20089 Rozzano MI, Italy. *Email: marco.ardigo@hunimed.eu
Key words: dermoscopy; microscopy; confocal; skin diseases; skin neoplasms; tomography; optical coherence; diagnosis.
Citation: Acta Derm Venereol 2026; 106: adv-2026-0385. DOI: https://doi.org/10.2340/actadv.v106.adv-2026-0385.
Copyright: 2026 ©Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jan 27, 2026. Accepted after revision: Jun 24, 2026.
Published: Jul 9, 2026.
Competing interests and funding: The data that support the findings of this study are available from the corresponding author upon reasonable request.
This study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Trial registration is not applicable for this review article.
DAMAE provide resources to perform research studies at the Dermatology Department at Hospital Clínic Barcelona.
Patients with genodermatoses, such as nevoid basal cell carcinoma syndrome, recessive dystrophic epidermolysis bullosa, familial atypical multiple mole and melanoma syndrome, xeroderma pigmentosum and ichthyosis with confetti, face a high risk of skin malignancies. While dermoscopy significantly improves diagnostic accuracy compared to clinical examination, its specificity remains limited when evaluating ambiguous lesions in these complex patients. This narrative review examines the role of reflectance confocal microscopy and line-field confocal optical coherence tomography in high-risk populations. By enabling the in vivo visualization of histologic-like features at cellular resolution, these noninvasive imaging technologies overcome the limitations of dermoscopy. The analysis of illustrative cases demonstrates that integrating these tools enhances both sensitivity and specificity, allowing for a precise differentiation between true malignancies and benign mimics. While reflectance confocal microscopy remains the standard for melanocytic criteria, line-field confocal optical coherence tomography complements it by overcoming depth limitations. Consequently, the use of combined noninvasive imaging supports a more conservative management strategy, potentially reducing the number of unnecessary excisions while ensuring the timely detection of skin cancer in patients with rare genetic syndromes.
SIGNIFICANCE
Genodermatosis associated with skin cancers is rare and often unrecognized. Patients affected by these syndromes face a high risk of skin cancer, often leading to frequent surgical removals of suspicious lesions, scarring and anxiety. This review highlights how reflectance confocal microscopy and line-field confocal optical coherence tomography can visualize in vivo skin structures at a cellular level overcoming dermoscopy limitations. By accurately distinguishing between true tumours and harmless mimics, these tools allow dermatologists to reduce unnecessary biopsies and surgeries. This approach significantly improves patient quality of life by minimizing physical scarring and emotional burden while ensuring early and accurate cancer detection.
INTRODUCTION
Although most skin cancers like basal cell carcinomas (BCCs), cutaneous squamous cell carcinomas (cSCCs) and melanomas are predominantly sporadic in origin, several hereditary syndromes are known to dramatically increase their incidence (1). These genetic syndromes predisposing to cutaneous malignancies are rare and frequently go unrecognized, resulting in delayed diagnoses and a substantial clinical and psychological burden on affected individuals (2). Among these, nevoid basal cell carcinoma syndrome (NBCCS, also known as Gorlin–Goltz syndrome) is the most representative for BCCs development (3) while Epidermolysis Bullosa (EB) (4) and its most severe subtype recessive dystrophic epidermolysis bullosa (RDEB), is a syndrome where cSCC is a major cause of cancer-related death (5). Conversely, syndromes primarily associated with melanoma include familial atypical multiple mole and melanoma (FAMMM) (6), Xeroderma Pigmentosum (XP) and Ichthyosis with confetti (IWC) with mutation in keratin 10 (KRT10). XP, in particular, is associated with a 2,000-fold increase in melanoma and up to a 10,000-fold increase in basal and squamous cell carcinomas, though mortality is most frequently related to melanoma (7).
Early prevention and strict dermatological surveillance become integral components of these patients' lives. However, this intensified surveillance inevitably uncovers numerous ambiguous lesions. Consequently, driven by the underlying genetic risk, a significant number of these are subjected to strict digital dermoscopy monitoring or excision, fueling a cycle of increasing patient anxiety and scarring (8).
Much of this cumulative morbidity could be mitigated, and the management of these lesions optimized, by increasing the sensitivity and specificity of diagnostic workflows through noninvasive advanced diagnostic tools. While these patients greatly bene-fit from dermoscopy and digital follow-up, the management of individuals with a high lesions burden and multiple benign mimickers may remain challenging, particularly outside highly specialized referral centres. In these settings, diagnostic performance may be influenced not only by the available imaging technique, but also by operator expertise and by the volume of complex cases routinely evaluated. In contrast, secondary-to-tertiary referral centres equipped with advanced noninvasive diagnostic tools, such as Reflectance Confocal Microscopy (RCM) and Line-Field Confocal Optical Coherence Tomography (LC-OCT), can offer a more refined approach. RCM enables in vivo visualization of epidermal and superficial dermal microarchitecture at almost histologic resolution and LC-OCT has emerged as a complementary image technique providing both vertical and horizontal optical sections with greater depth but with lower lateral resolution compared to RCM (9, 10). In this setting, dermoscopy serves as a screening tool, while advanced imaging acts as a second-level guide to better manage individual lesions. However, evidence specifically addressing their role in genodermatoses remains limited. This narrative review with illustrative cases aims to demonstrate the value of integrating RCM and LC-OCT in the management of patients with high-risk conditions such as genodermatoses, by supporting the evaluation of suspicious lesions and improving the distinction between true skin cancers and benign mimickers.
MATERIALS AND METHODS
This study was designed as a narrative review complemented by a case series. We performed a retrospective search within the databases of 2 tertiary referral centres (located in Italy and Spain) specializing in skin cancer and rare genetic skin disorders. From these datasets, we identified 5 pivotal cases representing distinct genodermatoses associated with an increased risk of cutaneous malignancies: NBCCS, RDEB, FAMMM, XP and IWC. For each selected patient, clinically relevant lesions were evaluated following a standardized noninvasive diagnostic workflow. Initial assessment involved clinical inspection and dermoscopy. Lesions displaying atypical features or those deemed equivocal on dermoscopy underwent second-level high-resolution imaging using either RCM or LC-OCT. The choice of the specific imaging modality was determined by lesion morphology (e.g., presence of hyperkeratosis, depth of the target structure) and anatomical location. Biopsy or surgical excision was reserved for cases in which clinical, dermoscopic or RCM/LC-OCT findings raised a suspicion of malignancy, or when noninvasive evaluation remained inconclusive. RCM and LC-OCT examinations were performed using device-integrated mapping systems to improve spatial correlation between clinical, dermoscopic and microscopic findings. RCM images were acquired with the VivaScope 1500 system. When needed, confocal mosaics, known as VivaBlocks, were generated by assembling multiple adjacent horizontal fields acquired at the same depth, while VivaStacks allowed sequential evaluation of the same area at different depths (11). For LC-OCT, the integrated dermoscopic mapping interface was used to create a lesion mosaic by stitching together adjacent dermoscopic fields acquired during probe movement. When available, the AI-based mapping tool was used as adjunctive support for lesion assessment. This software analyses LC-OCT acquisitions and provides a BCC probability output, which can be displayed on the dermoscopic mosaic as a colour-coded heat map. In this interface, yellow areas indicate regions with a higher algorithm-estimated probability of BCC, whereas blue areas indicate regions with a lower probability (12). This mapping allows the operator to visually correlate the AI output with the corresponding area within the dermoscopic mosaic and to identify the precise regions in which LC-OCT features considered suspicious by the algorithm are located. However, the AI-based heat map was not used as an independent diagnostic tool. Final interpretation and management decisions were based on the combined clinical, dermoscopic, RCM and LC-OCT evaluation performed by experienced operators. Concurrent with the case analysis, a review of the current literature was conducted to synthesize the genetic background, clinical presentation and specific diagnostic challenges associated with each of the 5 syndromes.
GENODERMATOSES ASSOCIATED WITH SKIN CANCERS
Nevoid basal cell carcinoma syndrome
NBCCS is typically caused by germline mutations in PTCH1 or in a minority of cases SUFU. PTCH1 a key tumour suppressor gene within the Hedgehog signalling pathway, and its estimated incidence ranges between 1 in 57,000 and 1 in 256,000 individuals (3). Patients with NBCCS frequently develop multiple superficial BCCs. Dermoscopic features of nonpigmented superficial BCCs, such as a pink-to-rose background and short linear vessels, may overlap with those of inflam-matory or other benign lesions and may therefore be insufficient for confident diagnosis in selected equivocal cases (13). In this context, LC-OCT provides rapid, high-resolution visualization of morphological criteria associated with BCC and its main subtypes, including superficial, nodular and infiltrative forms (Fig. 1A). Importantly, LC-OCT does not autonomously classify BCC subtypes; subtype assessment remains operator-dependent and relies on the interpretation of specific morphological features. Nevertheless, recent prospective evidence has shown that LC-OCT improves diagnostic performance for both BCC detection and subtype discrimination compared with dermoscopy alone, while AI-based tools available in some modern devices may provide additional support by estimating the probability of BCC (14). Beyond tumour detection, LC-OCT can also identify nontumoural features that are characteristic of NBCCS, such as palmar pits, thereby contributing to an early diagnosis of this rare genodermatosis (Fig. 1B). According to the diagnostic criteria for NBCCS, the diagnosis can be established in the presence of: one major criterion plus genetic confirmation, 2 major criteria or 1 major criterion combined with 2 minor criteria (15). In a young patient, LC-OCT alone can perform the diagnosis of NBCCS by identifying 2 major features, BCCs and palmar/plantar pits, even in the absence of genetic testing or in cases where a de novo mutation is suspected in the first affected family member. Moreover, by enabling efficient assessment of multiple lesions in a single session, LC-OCT fulfils a dual function. The former is diagnostic, as the integrated artificial intelligence (AI) provides a BCC prediction score that helps even less experienced users reach a reliable assessment, assisting in distinguishing BCCs from benign mimickers such as nonspecific erythematous areas (16). The latter is predictive for nonsurgical treatments, since LC-OCT enables identification of features that align with superficial, nodular and infiltrative BCCs and is also able to find histological markers like multiple aggregated yellow-white globules associated with high-risk BCCs (17).
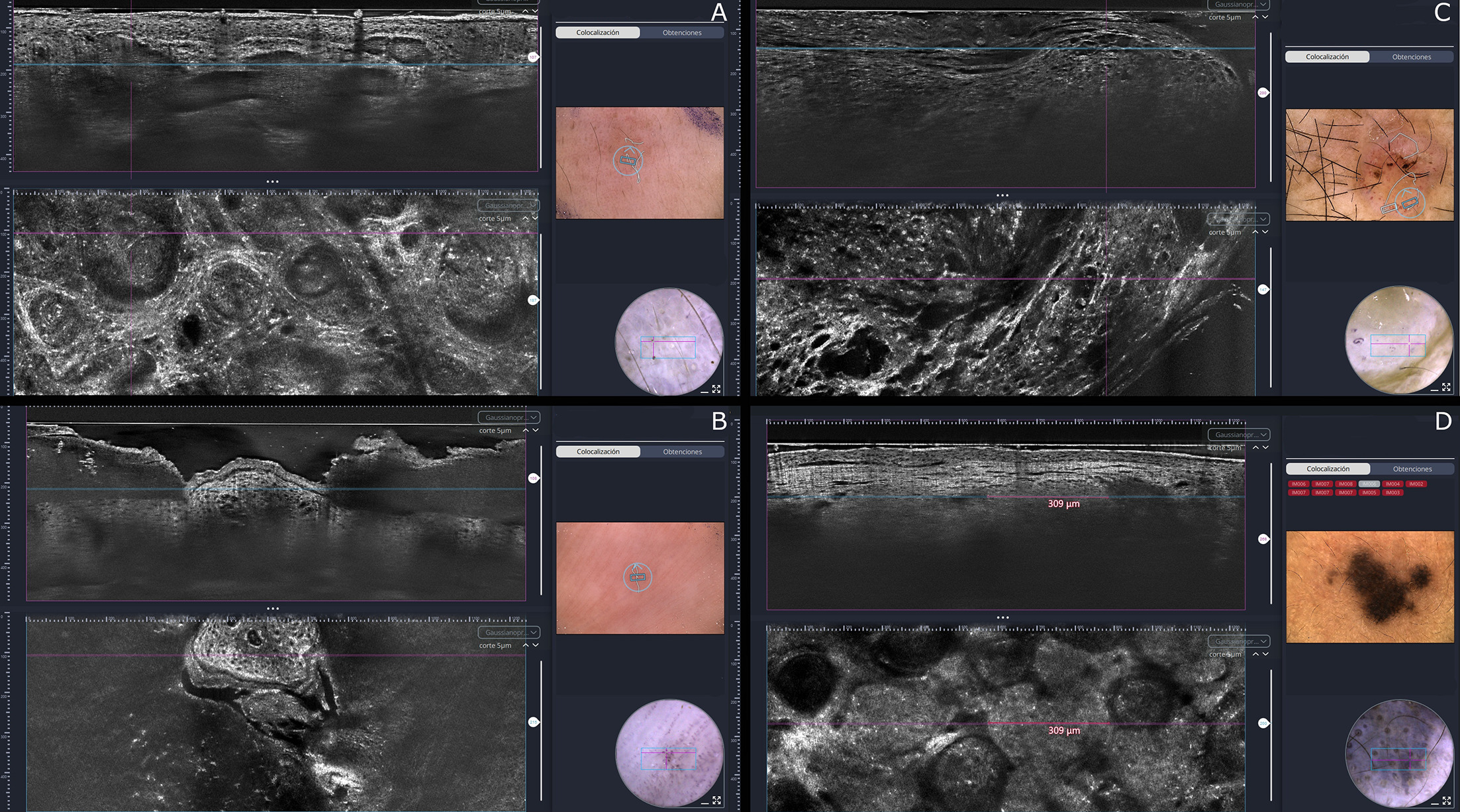
Fig. 1. Line-Field Confocal Optical Coherence Tomography (LC-OCT) images of patients with nevoid basal cell carcinoma syndrome (A, B) and recessive dystrophic epidermolysis bullosa syndrome (C, D). Infiltrative basal cell carcinoma: in the vertical view of LC-OCT images, basaloid tumour islands with a characteristic millefeuille pattern infiltrate the dermis and compress the surrounding hyperreflective collagen; in the horizontal view, these islands appear as ovoid structures containing bright hyperreflective particles (A). Palmar pits: the vertical view shows focal loss of the stratum corneum on the palmar surface, while the horizontal view highlights exposure of the stratum spinosum, confirming the absence of the stratum corneum (B). Squamous cell carcinoma: the vertical view demonstrates marked hyperkeratosis and keratinocytes with variably sized hyporeflective nuclei; in the horizontal view, the normal epidermal honeycomb pattern is completely lost and replaced by dysplastic keratinocytes (C). Epidermolysis bullosa (EB) nevi: dermoscopy reveals a blue–black melanocytic lesion with adjacent satellitosis, consistent with EB nevi. In the vertical LC-OCT view, the epidermis appears preserved, with underlying hyperreflective collagen due to compression and fibrosis, surrounded by hyperreflective ovoid structures corresponding to melanocytic nests. In the horizontal LC-OCT view, the nests appear as ovoid structures of uniform size (≈309 μm), filled with cells showing homogeneous reflectance and morphology (D).
Recessive dystrophic epidermolysis bullosa
EB comprises a group of inherited conditions marked by extreme skin fragility, which makes the skin highly susceptible to mechanical injury (4). Clinical severity largely correlates with the quality and the amount of type VII collagen expressed in the papillary dermis, reflecting the mode of inheritance: dominant dystrophic EB usually presents with a milder phenotype, while RDEB is associated with a much more severe disease course (5). RDEB is also associated with a markedly increased risk of developing aggressive cSCCs, making early detection essential for improving prognosis (18). LC-OCT may support the triage of clinically or dermoscopically equivocal keratinocyte lesions by allowing real-time visualization of epidermal architecture, keratinocyte atypia and, when technically visible, the dermoepidermal junction. In other high-risk populations, such as organ transplant recipients, LC-OCT-based triage models have identified severe dysplasia, broad strands and keratin pearls as high-yield criteria for SCC assessment, suggesting that similar image-markers may be useful to guide clinical decision-making in complex patients with a high tumour burden (19). However, SCC diagnosis and risk stratification with LC-OCT remain challenging, particularly in hyperkeratotic or crusted lesions, where visualization of the dermoepidermal junction may be impaired. Recent evidence in hyperkeratotic actinic keratoses suggests that short preimaging hydration protocols may improve dermoepidermal junction visibility and support more reliable lesion assessment, although this approach has not yet been validated in RDEB or in suspected SCC arising in EB skin (20, 21). Therefore, LC-OCT should be considered an adjunctive triage tool, while biopsy remains mandatory whenever invasive SCC is suspected or noninvasive findings are inconclusive (Fig. 1C). Patients with RDEB may also develop EB nevi, which tend to be large, eruptive, and often irregularly pigmented, with frequent small satellite lesions. EB nevi usually arise at sites of prior blistering or erosions. Repeated basement-membrane disruption prevents melanocytes from re-establishing their position at the dermoepidermal junction (22), causing them instead to localize within the dermis. Their dermal placement accounts for the characteristic grey-blue pigmentation observed (Fig. 1D). While RCM is constrained by its limited penetration depth, LC-OCT offers complementary vertical and horizontal views that extend deeper into the dermis, making it particularly useful for assessing EB nevi. The presence of dense, well-defined nests composed of monomorphic cells is more indicative of a nevus, whereas prominent pagetoid spread and the presence of clefts are features more suggestive of melanoma (23). This provides valuable information for distinguishing between malignant melanocytic lesions and reactive pigmentation changes.
Familial atypical multiple mole and melanoma syndrome
Families with the FAMMM syndrome are characterized by the presence of multiple atypical nevi and a personal/family history of melanoma, due to germline mutations in the cyclin-dependent kinase inhibitor 2A (CDKN2A) gene (6). Cumulative risk estimates indicate that carriers of germline CDKN2A mutations have about a 14% probability of developing melanoma by age 50 (24). Although digital dermoscopy follow-up allows for the detection of subtle changes over time, it is crucial to recognize that not all dermoscopic evolution indicates malignancy. Patients with multiple atypical nevi often exhibit benign dynamic changes; consequently, a low threshold for excising any changing lesion results in the excessive removal of dysplastic nevi rather than improved melanoma detection (25). RCM has shown promising results in reducing the number of unnecessary biopsies by improving the differentiation between benign melanocytic nevi and early melanomas visualizing key diagnostic features (Fig. 2A and B) such as pagetoid spread, atypical cells at the dermoepidermal junction and irregular nests of melanoma cells, thereby increasing diagnostic accuracy and supporting timely melanoma detection (26). LC-OCT can also detect the same microscopic melanoma features of RCM (Fig. 2C) but further studies are needed to assess the accuracy. For these patients a follow-up with digital dermoscopy followed by an RCM analysis of the lesions that show changes in dermoscopy is suggested to reduce the number of unnecessary biopsies increasing their quality of life (27).
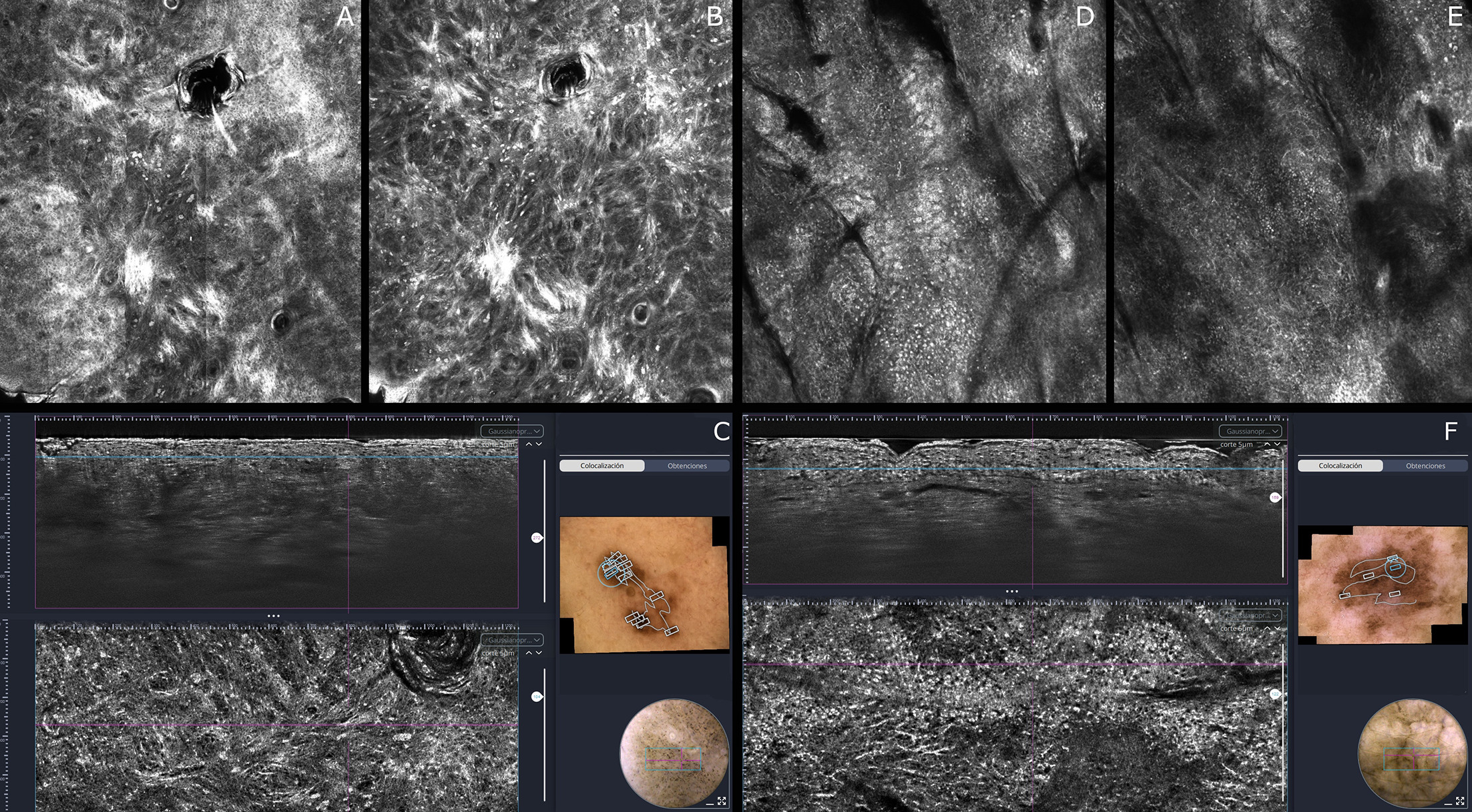
Fig. 2. Reflectance confocal microscopy (RCM) and Line-Field Confocal optical coherence tomography (LC-OCT) features of high-risk melanocytic lesions in familial atypical multiple mole and melanoma (FAMMM) syndrome and xeroderma pigmentosum. RCM and LC-OCT images in a patient with FAMMM syndrome showing scattered round pagetoid melanocytic cells within the epidermis (A), round atypical melanocytes and hyperreflective linear nests at the dermoepidermal junction (DEJ) (B), as well as loss of DEJ definition in the vertical view with round-to-dendritic hyperreflective cells corresponding to pagetoid melanocytes in the horizontal view (C). RCM and LC-OCT images in a patient with xeroderma pigmentosum demonstrate a cobblestone pattern with dendritic pagetoid cells in the epidermis (D), hyperreflective dendritic cells in the suprabasal layer (E) and multiple pagetoid dendritic hyperreflective cells more clearly visualized in the horizontal view (F).
Xeroderma pigmentosum (XP)
XP is a rare, autosomal recessive disorder caused by nucleotide excision repair (NER) defect leading to extreme sensitivity to UV radiation and widespread photodamage. Lesion monitoring in these individuals is particularly challenging for several reasons. First, they are at risk of developing a wide range of skin tumours like nonmelanoma and melanoma skin cancers, each with distinct clinical and dermoscopic features. Second, their severely photodamaged skin can obscure or mimic tumour-specific patterns under dermoscopy, and the high likelihood of multiple concurrent lesions can result in overlapping features that further complicate diagnosis (28). In patients with XP, melanomas often arise in areas resembling solar lentigines, making them difficult to distinguish using dermoscopy alone (29). While digital dermoscopy is valuable for monitoring the evolution of these lesions, RCM is particularly effective for the immediate detection of such superficial melanomas (Fig. 2D and E). Although LC-OCT can visualize epidermal features similar to those seen in RCM (Fig. 2F), its performance is limited by inferior lateral resolution (1.1 um vs. 0.5um). Given that the relevant first melanoma-associated changes are predominantly epidermal, the superior resolution of RCM makes it the preferred first-line modality over LC-OCT. For nonmelanocytic tumours such as BCC and cSCC, LC-OCT enables a faster and broader evaluation, particularly useful in severely photodamaged areas where clinical and dermoscopic assessment is limited.
Ichthyosis with confetti (IWC)
IWC, also known as ichthyosis variegata or congenital reticular ichthyosiform erythroderma, is an exceptionally rare autosomal dominant ichthyosis caused by pathogenic variants in keratin (KRT) 1 or KRT10, which are crucial for epidermal stability (30). The term “confetti” derives from the appearance of numerous small, pale patches of normal skin that emerge during childhood on a background of erythematous, scaly skin, resembling confetti scattered across a surface (31). IWC is usually not associated with the development of multiple melanomas, but some evidence suggests that mutations in KRT10 appear to be linked to the mutation itself, which introduces coding errors and genomic instability (32). IWC patients with KRT10 mutations have been associated with multiples melanomas in 2 case reports (33, 34). In patients with ichthyoses, marked hyperkeratosis significantly restricts the penetration depth of RCM, often preventing the visualization of key diagnostic structures needed to distinguish melanomas from nevi. To overcome this depth limitation, LC-OCT was employed to assess a suspicious papule in a young female patient with a significant history of melanoma (>7 lesions, ranging from in situ to pT3b). LC-OCT revealed an atypical wave pattern, atypical melanocytes at the DEJ and scattered pagetoid cells within the epidermis (Fig. 3A). The lesion was misclassified by the algorithm as BCC with a 99% probability, most likely due to its atypical wave pattern mimicking collagen compression by basaloid tumour islands (Fig. 3B). It is important to note that multiple flat black/blue lesions were distributed across the patient’s skin in which LC-OCT evaluation revealed atypical dendritic, spindle-shaped and round hyperreflective cells within these lesions, raising suspicion for an atypical melanocytic proliferation, including possible melanoma in situ (Fig. 4). Due to the high number of diffuse lesions and the patient’s impaired wound-healing capacity, both complete surgical excision and radiotherapy were deemed unfeasible. Consequently, a conservative management strategy was adopted, relying on strict surveillance via digital dermoscopy. If dermoscopic changes are detected, LC-OCT and clinical assessment are utilized to identify deeper dermal involvement, with biopsy or excision reserved only for lesions demonstrating clear progression. Additionally, a therapeutic trial with imiquimod was attempted but failed to show clinical improvement.
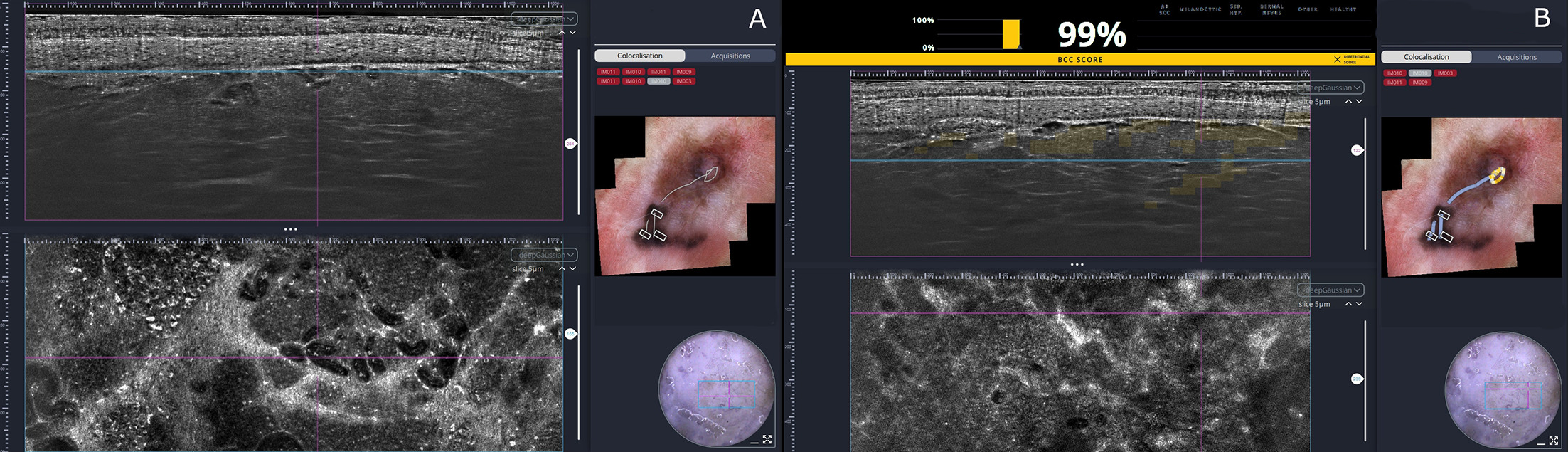
Fig. 3. Line-Field Confocal Optical Coherence Tomography (LC-OCT) features of melanoma in a patient with Ichthyosis with confetti (IWC) and multiple melanoma. LC-OCT images of a melanoma on the right tibial region in a patient with multiple melanomas and IWC. The vertical view shows marked hyperkeratosis related to IWC and a dermal nodule displaying an atypical wave pattern. The horizontal view reveals atypical melanocytes at the dermoepidermal junction and vessels with increased vascularity (A). Histopathologic examination subsequently confirmed a diagnosis of pT1a melanoma with a Breslow thickness of 0.7 mm. The AI algorithm incorrectly classified the lesion as a basal cell carcinoma, likely due to the misinterpretation of hyperreflective collagen bundles compressed around tumour nests. Such misclassifications may occur in rare patient populations not represented in the algorithm’s training dataset (B).
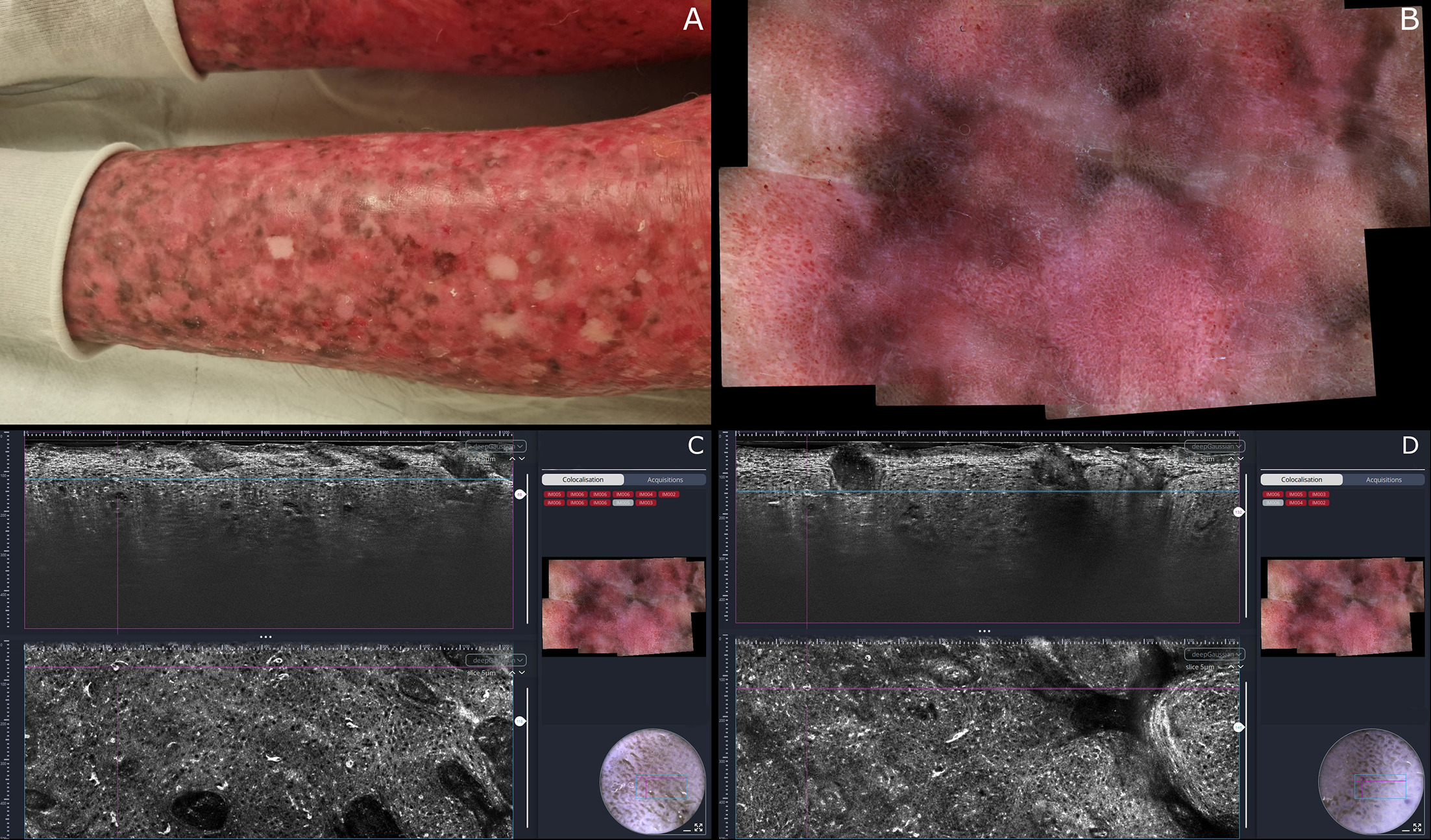
Fig. 4. Pigmented lesions in Ichthyosis with confetti (IWC): Clinical, dermoscopic and Line-Field Confocal Optical Coherence Tomography (LC-OCT) correlation. Clinical image showing the typical ‘confetti-like’ hypopigmented macules on the left lower leg (A). Dermoscopy of atypical flat pigmented macules, characterized by grey–blue structureless areas interspersed with erythematous skin (B). LC-OCT reveals atypical dendritic, spindle-shaped and round hyperreflective cells within the stratum spinosum, consistent with an atypical melanocytic lesion without evidence of dermal involvement (C–D).
DISCUSSION
For many years, dermoscopy was the only noninvasive tool largely available for evaluating suspicious lesions. Although it improves diagnostic accuracy compared with naked-eye examination, it still presents significant limitations (35). Dermoscopy is particularly effective for diagnosing pigmented BCCs which present with leaf-like structures and blue ovoid nests and nodular nonpigmented BCC, where classic arborizing vessels are clearly visible. However, superficial nonpigmented BCCs represent a significant diagnostic challenge, as they often present only with a non-specific pink background (36). RCM overcomes this limitation by visualizing basaloid islands, a pathognomonic feature of BCC. These islands are easily identified as bright (hyperreflective) structures in pigmented BCC, whereas in nonpigmented cases, they appear as dark (hyporeflective) islands contrasted against hyperreflective compressed collagen. Similarly, LC-OCT reveals the specific 'millefeuille' pattern associated with BCC. Additionally, the system’s AI support offers a real-time probability score, providing a useful second opinion for the operator (37). A recent multicentric study demonstrated that dermoscopy alone achieves a sensitivity of 93.2% but a specificity of only 51.7% in the diagnosis of BCC. The addition of RCM increased sensitivity to 97.8% and raised specificity to 86.8%, dramatically reducing false positives and unnecessary biopsies (38). Similarly, LC-OCT has been shown to increase specificity for BCC diagnosis from 37% with dermoscopy alone to 90% while maintaining comparable sensitivity (14). Dermoscopic diagnosis of cSCC relies on well-established criteria, including specific vascular patterns (such as dotted, glomerular or polymorphic vessels) and the presence of hyperkeratosis visualized as a white scale. Although hyperkeratosis is itself a valuable diagnostic clue, it often acts as a significant confounding factor. In dermoscopy, it visually obscures the underlying vascular and structural features essential for a confident differential diagnosis (39). Similarly, in noninvasive imaging, marked hyperkeratosis or crusting may attenuate the optical signal of both RCM and LC-OCT, making deeper structures less visible and thereby reducing diagnostic performance. To partially address this limitation, these tools can be applied at the lesion periphery, where the keratin layer may be thinner, or after careful removal of the hyperkeratotic crust when clinically appropriate. Recent evidence in hyperkeratotic actinic keratoses suggests that short preimaging preparation protocols, such as tap-water occlusion or salicylic acid ointment, may improve DEJ visibility (20). These noninvasive tools allow direct visualization of cellular dysplasia and epidermal architectural disarray; in suspected invasive cSCC, more specific LC-OCT features include dermal tumour strands or nests of atypical keratinocytes (19), whereas keratinizing pearls may be observed as an additional feature, particularly in more differentiated lesions (17). However, the recognition of these structures depends on adequate visualization of the dermoepidermal junction and superficial dermis, which may be limited in hyperkeratotic lesions. Visualization of the DEJ is clinically relevant for 2 reasons: first, in AKs, it may support PRO-score assessment, a prognostic marker proposed to be associated with the risk of progression to cSCC; second, in suspected invasive cases, it may help evaluate DEJ disruption and possible dermal invasion (40). Regarding melanoma, numerous dermoscopic algorithms are widely validated for distinguishing benign from malignant lesions. A major drawback, however, is that classic signs with high specificity (including blue-black colour and ulceration) are generally hallmarks of thick, invasive melanomas rather than early-stage lesions. In patients with genodermatoses, where maximizing life expectancy relies on detecting malignancy at the in situ or thin invasive stage, the clinical priority shifts to differentiating early melanomas from dysplastic nevi, which often share overlapping features (41). To address this challenge, specific RCM scoring systems have been developed, most notably the 2-step algorithm. This method classifies lesions by assessing "nevus criteria" like typical basal cells and edged papillae along with "melanoma criteria" like roundish pagetoid cells and atypical nucleated cells and DEJ. Notably, when at least one of the key nevus criteria is absent, the algorithm achieves a sensitivity of 100% and a specificity of 57% for melanoma detection (42). Similarly, recent LC-OCT research has identified quantitative and structural markers for malignancy: specifically, the presence of more than 10 pagetoid cells per 3D stack and clefting within melanocytic nests have been shown to significantly correlate with melanoma rather than nevi (23, 43). In terms of clinical management, a pivotal multicentric trial involving over 3,000 patients demonstrated that adding RCM to standard dermoscopy reduced the number of unnecessary excisions of suspicious melanocytic lesions by 43.3% (27). Although this study was conducted on a general population rather than a specific genodermatosis cohort, the implications are highly relevant. Given that LC-OCT roughly visualizes the same critical diagnostic features as RCM with the added benefit of vertical depth information, a comparable reduction in surgical morbidity is anticipated, although prospective studies quantifying this specific impact are yet to be published. Beyond their diagnostic role, RCM and LC-OCT should be considered as tools that may support the longitudinal management of complex high-risk patients rather than merely as techniques intended to replace biopsy. In patients with genodermatoses, as in other high-risk populations such as organ transplant recipients (19), the clinical challenge is not limited to the recognition of a single malignant lesion, but also includes the repeated evaluation of multiple equivocal lesions over time. In this context, the integration of noninvasive imaging in specialized referral centres may help guide lesion selection for biopsy or excision, reduce unnecessary procedures and support a more individualized surveillance strategy in patients with a high tumour burden. In conclusion, the integration of RCM and LC-OCT represents a paradigm shift in the management of genodermatoses, enabling a transition from reactive surgery to proactive, conservative surveillance. Although RCM remains the guideline-recommended gold standard for melanocytic lesions, LC-OCT proves indispensable for evaluating keratinocyte carcinomas and deeper dermal structures, particularly in hyperkeratotic conditions where RCM penetration is compromised. Although challenges regarding operator dependence and the need for AI validation in rare cohorts persist, these noninvasive tools significantly enhance diagnostic confidence and reduce procedural morbidity. Future multicentric studies are now required to standardize their application and confirm their long-term cost-effectiveness in these high-risk population.
ACKNOWLEDGEMENTS
The publication fee for this work was covered by the Italian Ministry of Health’s 'Ricerca Corrente' funding to the IRCCS Humanitas Research Hospital
REFERENCES
- Juan HY, Zhou AE, Hoegler KM, Khachemoune A. Overview of familial syndromes with increased skin malignancies. Arch Dermatol Res 2023; 315: 707–727. https://doi.org/10.1007/s00403-022-02447-8
- Schierbeck J, Vestergaard T, Bygum A. Skin cancer associated genodermatoses: a literature review. Acta Derm Venereol 2019; 99: 360–369. https://doi.org/10.2340/00015555-3123
- Smith MJ, Beetz C, Williams SG, Bhaskar SS, O’Sullivan J, Anderson B, et al. Germline mutations in SUFU cause Gorlin syndrome-associated childhood medulloblastoma and redefine the risk associated with PTCH1 mutations. J Clin Oncol 2014; 32: 4155–4161. https://doi.org/10.1200/JCO.2014.58.2569
- Has C, Bauer JW, Bodemer C, Bolling MC, Bruckner-Tuderman L, Diem A, et al. Consensus reclassification of inherited epidermolysis bullosa and other disorders with skin fragility. Br J Dermatol 2020; 183: 614–627. https://doi.org/10.1111/bjd.18921
- Christiano AM, Fine JD, Uitto J. Genetic basis of dominantly inherited transient bullous dermolysis of the newborn: a splice site mutation in the type VII collagen gene. J Invest Dermatol 1997; 109: 811–814. https://doi.org/10.1111/1523-1747.ep12341013
- Soura E, Eliades PJ, Shannon K, Stratigos AJ, Tsao H. Hereditary melanoma: update on syndromes and management: genetics of familial atypical multiple mole melanoma syndrome. J Am Acad Dermatol 2016; 74: 395–407. https://doi.org/10.1016/j.jaad.2015.08.038
- Black JO. Xeroderma pigmentosum. Head Neck Pathol 2016; 10: 139–144. https://doi.org/10.1007/s12105-016-0707-8
- Rossi M, Pellegrini C, Cardelli L, Ciciarelli V, Di Nardo L, Fargnoli MC. Familial melanoma: diagnostic and management implications. Dermatol Pract Concept 2019; 9: 10–16. https://doi.org/10.5826/dpc.0901a03
- Piscazzi F, Ardigò M, Suppa M, Malvehy J, Puig S, Perez-Anker J. Applying RCM-based criteria to LC-OCT for classifying mucosal melanoses: a proof-of-concept study. Dermatol Pract Concept 2026; 16: 6544. https://doi.org/10.5826/dpc.1602a6544
- Valenti M, Piscazzi F, Franceschini C, Ferrari A, Frascione P, Ardigò M. Characterizing pigmented mucosal lesions: new insights from reflectance confocal microscopy. J Eur Acad Dermatol Venereol 2025; 39: e638–e641. https://doi.org/10.1111/jdv.20656
- Ahlgrimm-Siess V, Laimer M, Rabinovitz HS, Oliviero M, Hofmann-Wellenhof R, Marghoob AA, et al. Confocal microscopy in skin cancer. Curr Dermatol Rep 2018; 7: 105–118. https://doi.org/10.1007/s13671-018-0218-9
- Mozaffari M, Tavernier C, Ogien J, Godet P, Fünfer K, Wirsching H, et al. Co-localized dermoscopy and LC-OCT for AI-assisted margin assessment of basal cell carcinoma: development of a “BCC-One-Stop-Shop” workflow. Diagnostics 2026; 16: 750. https://doi.org/10.3390/diagnostics16050750
- Wojtowicz I, Żychowska M. Dermoscopy of basal cell carcinoma part 1: dermoscopic findings and diagnostic accuracy—a systematic literature review. Cancers 2025; 17: 493. https://doi.org/10.3390/cancers17030493
- Orte Cano C, Sanak D, Lenoir C, Diet G, Fontaine M, Boussingault L, et al. Diagnostic performance of line-field confocal optical coherence tomography for basal cell carcinoma: a prospective study. Cancers 2026; 18: 153. https://doi.org/10.3390/cancers18010153
- Verkouteren BJA, Cosgun B, Reinders MGHC, Kessler PAWK, Vermeulen RJ, Klaassens M, et al. A guideline for the clinical management of basal cell naevus syndrome (Gorlin-Goltz syndrome). Br J Dermatol 2022; 186: 215–226. https://doi.org/10.1111/bjd.20700
- Federico S, Cassalia F, Mazza M, Del Fiore P, Ferrera N, Malvehy J, et al. Advancements in diagnosis of neoplastic and inflammatory skin diseases: old and emerging approaches. Diagnostics 2025; 15: 2100. https://doi.org/10.3390/diagnostics15162100
- Piscazzi F, Ardigò M, Carrera C, Suppa M, Cinotti E, Perrot JL, et al. Line-field confocal optical coherence tomography in diagnosing keratinizing pearls, multiple aggregated yellow–white globules and milia-like cysts in squamous cell carcinomas, basal cell carcinomas and seborrhoeic keratoses. Clin Exp Dermatol 2025; 51: 107–109. https://doi.org/10.1093/ced/llaf346
- Rodeck U, Uitto J. Recessive dystrophic epidermolysis bullosa-associated squamous-cell carcinoma: an enigmatic entity with complex pathogenesis. J Invest Dermatol 2007; 127: 2295–2296. https://doi.org/10.1038/sj.jid.5700939
- Jacobsen K, Ortner VK, Wiegell SR, Philipsen PA, Haedersdal M. Skin lesion triage in organ transplant recipients using line‐field confocal optical coherence tomography: a retrospective classification study. J Deutsche Derma Gesell 2026. https://doi.org/10.1111/ddg.15974
- Jacobsen K, Haedersdal M. Line-field confocal optical coherence tomography assessment of dermal-epidermal junction in actinic keratosis and skin cancer. Int J Dermatol 2026. https://doi.org/10.1111/ijd.70415
- Michelini S, Scribani Rossi P, Gemma G, Persechino F, Vespasiani G, Conforti C, et al. Assessing the dermal epidermal junction of hyperkeratotic actinic keratoses via line-field confocal optical coherence tomography. Int J Dermatol 2026. https://doi.org/10.1111/ijd.70328
- Gallardo F, Toll A, Malvehy J, Mascaró-Galy JM, Lloreta J, Barranco C, et al. Large atypical melanocytic nevi in recessive dystrophic epidermolysis bullosa: clinicopathological, ultrastructural, and dermoscopic study. Pediatr Dermatol 2005; 22: 338–343. https://doi.org/10.1111/j.1525-1470.2005.22412.x
- Pérez-Anker J, Soglia S, Puig S, García A, Albero R, Alejo B, et al. Melanocytic clefting is associated with melanoma on LC-OCT. J Eur Acad Dermatol Venereol 2025; 39: 1923–1933. https://doi.org/10.1111/jdv.20761
- Begg CB, Orlow I, Hummer AJ, Armstrong BK, Kricker A, Marrett LD, et al. Lifetime risk of melanoma in CDKN2A mutation carriers in a population-based sample. J Natl Cancer Inst 2005; 97: 1507–1515. https://doi.org/10.1093/jnci/dji312
- Woltsche N, Schwab C, Deinlein T, Hofmann-Wellenhof R, Zalaudek I. Dermoscopy in the era of dermato-oncology: from bed to bench side and retour. Expert Rev Anticancer Ther 2016; 16: 531–541. https://doi.org/10.1586/14737140.2016.1168700
- Dinnes J, Deeks JJ, Saleh D, Chuchu N, Bayliss SE, Patel L, et al. Reflectance confocal microscopy for diagnosing cutaneous melanoma in adults. Cochrane Database Syst Rev 2018; 12: CD013190. https://doi.org/10.1002/14651858.CD013190
- Pellacani G, Farnetani F, Ciardo S, Chester J, Kaleci S, Mazzoni L, et al. Effect of reflectance confocal microscopy for suspect lesions on diagnostic accuracy in melanoma: a randomized clinical trial. JAMA Dermatol 2022; 158: 754–761. https://doi.org/10.1001/jamadermatol.2022.1570
- Malvehy J, Puig S, Marti-Laborda RM. Dermoscopy of skin lesions in two patients with xeroderma pigmentosum. Br J Dermatol 2005; 152: 271–278. https://doi.org/10.1111/j.1365-2133.2004.06332.x
- Stern JB, Peck GL, Haupt HM, Hollingsworth HC, Beckerman T. Malignant melanoma in xeroderma pigmentosum: search for a precursor lesion. J Am Acad Dermatol 1993; 28: 591–594. https://doi.org/10.1016/0190-9622(93)70079-9
- Choate KA, Lu Y, Zhou J, Choi M, Elias PM, Farhi A, et al. Mitotic recombination in patients with ichthyosis causes reversion of dominant mutations in KRT10. Science 2010; 330: 94–97. https://doi.org/10.1126/science.1192280
- Lim YH, Qiu J, Saraceni C, Burrall BA, Choate KA. Genetic reversion via mitotic recombination in ichthyosis with confetti due to a KRT10 polyalanine frameshift mutation. J Invest Dermatol 2016; 136: 1725–1728. https://doi.org/10.1016/j.jid.2016.04.023
- Spoerri I, Brena M, De Mesmaeker J, Schlipf N, Fischer J, Tadini G, et al. The phenotypic and genotypic spectra of ichthyosis with confetti plus novel genetic variation in the 3’ end of KRT10: from disease to a syndrome. JAMA Dermatol 2015; 151: 64–69. https://doi.org/10.1001/jamadermatol.2014.2526
- Ito Y, Takeichi T, Nakagawa K, Tanahashi K, Muro Y, Ogi T, et al. Case of ichthyosis with confetti caused by KRT10 mutation, complicated with multiple malignant melanomas. J Dermatol 2022; 49: e228–e229. https://doi.org/10.1111/1346-8138.16348
- Aromolo IF, Moltrasio C, Cozzaglio L, Colavito D, Leon A, Cavalli R, et al. Multiple melanomas in ichthyosis with confetti: one more piece of evidence. Australas J Dermatol 2023; 64: 576–578. https://doi.org/10.1111/ajd.14143
- Wu X, Marchetti MA, Marghoob AA. Dermoscopy: not just for dermatologists. Melanoma Manag 2015; 2: 63–73. https://doi.org/10.2217/mmt.14.32
- Reiter O, Mimouni I, Gdalevich M, Marghoob AA, Levi A, Hodak E, et al. The diagnostic accuracy of dermoscopy for basal cell carcinoma: a systematic review and meta-analysis. J Am Acad Dermatol 2019; 80: 1380–1388. https://doi.org/10.1016/j.jaad.2018.12.026
- Boussingault L, Lenoir C, Stefani AD, Cappilli S, Fontaine M, Diet G, et al. Line-field confocal optical coherence tomography of basal cell carcinoma: systematic correlation with histopathology. Diagnostics 2025; 15: 3059. https://doi.org/10.3390/diagnostics15233059
- Longo C, Guida S, Mirra M, Pampena R, Ciardo S, Bassoli S, et al. Dermatoscopy and reflectance confocal microscopy for basal cell carcinoma diagnosis and diagnosis prediction score: a prospective and multicenter study on 1005 lesions. J Am Acad Dermatol 2024; 90: 994–1001. https://doi.org/10.1016/j.jaad.2024.01.035
- Zalaudek I, Giacomel J, Schmid K, Bondino S, Rosendahl C, Cavicchini S, et al. Dermatoscopy of facial actinic keratosis, intraepidermal carcinoma, and invasive squamous cell carcinoma: a progression model. J Am Acad Dermatol 2012; 66: 589–597. https://doi.org/10.1016/j.jaad.2011.02.011
- Thamm JR, Daxenberger F, Viel T, Gust C, Eijkenboom Q, French LE, et al. Artificial intelligence‐based PRO score assessment in actinic keratoses from LC‐OCT imaging using Convolutional Neural Networks. J Deutsche Derma Gesell 2023; 21: 1359–1366. https://doi.org/10.1111/ddg.15194
- Thomas L, Puig S. Dermoscopy, digital dermoscopy and other diagnostic tools in the early detection of melanoma and follow-up of high-risk skin cancer patients. Acta Derm Venereol 2017; Suppl 218: 14–21. https://doi.org/10.2340/00015555-2719
- Segura S, Puig S, Carrera C, Palou J, Malvehy J. Development of a two-step method for the diagnosis of melanoma by reflectance confocal microscopy. J Am Acad Dermatol 2009; 61: 216–229. https://doi.org/10.1016/j.jaad.2009.02.014
- Perez-Anker J, Soglia S, Lenoir C, Albero R, Alos L, García A, et al. Criteria for melanocytic lesions in LC-OCT. J Eur Acad Dermatol Venereol 2024; 38: 2005–2016. https://doi.org/10.1111/jdv.20079