SHORT COMMUNICATION
Dermoscopic Structures Predictive of Response to Photodynamic Therapy in Basal Cell Carcinoma
Alba NAVARRO-BIELSA1,2, Paulina CERRO-MUÑOZ1, Manuel ALMENARA-BLASCO1,2, Tamara GRACIA-CAZAÑA1,2 and Yolanda GILABERTE1,2
1Department of Dermatology, Miguel Servet University Hospital, Paseo Isabel la Católica 1-3, ES-50009 and 2IIS Aragón, Zaragoza, Spain. E-mail: albanavarrobielsa@hotmail.com
Citation: Acta Derm Venereol 2023; 103: adv00892. DOI https://doi.org/10.2340/actadv.v103.4838.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Feb 14, 2023; Published: Mar 20, 2023
INTRODUCTION
The most common type of non-melanoma skin cancer is basal cell carcinoma (BCC), with incidence rates in Europe and the USA increasing from 519 to 1,019 (between 1998–2010) and from 606 to 1,488 (between 1986–2006) (1). Rates are predicted to continue to increase until at least 2040, owing to an aging population with historical exposure to ultraviolet (UV) light (2).
Photodynamic therapy (PDT) is recommended for treatment of primary superficial and thin low-risk nodular BCC. PDT is considered most appropriate for nodular lesions where surgical excision is contraindicated or in cases in which patients, based on past treatment history, comorbidities, and/or cosmetic considerations, are willing to accept a higher risk of recurrence (3).
However, dermatologists are often faced with doubts as to the effectiveness of PDT in a given BCC, and whether a lesion has been completely eradicated by the end of the treatment or whether residual disease persists. Dermoscopy, a non-invasive diagnostic technique, can aid the selection of patients who can benefit most from PDT, and can be used during follow-up to detect recurrences.
Clinical, histological, and immunohistochemical biomarkers that help predict the response of BCC to PDT have been described to date. However, only one study has evaluated the use of dermoscopy to assess patients’ response to non-ablative therapies for the treatment of superficial BCC (4). The aim of the current study was to identify dermoscopic signs of BCC (superficial and nodular) predictive of the response to PDT.
MATERIALS AND METHODS
A prospective study of patients with biopsy-diagnosed BCC treated with photodynamic therapy–methyl aminolevulinate (PDT-MAL) at Miguel Servet University Hospital in Zaragoza, Spain, between 2019 and 2021 was performed.
After tumour curettage patients were treated with 16% MAL. After 3 h of light-impenetrable occlusion the area was illuminated with a red-light-emitting diode device, diode device Aktilite CL128 (Galderma Nordic AB, Uppsala, Sweden) with a fluence of 37 J cm2 (8 min of ilumination at 10 cm of distance), repeating the session after 1 week. Clinicians were blinded to clinical status in order to avoid classification bias, and dermoscopic evaluations were always performed by the same clinician taking dermoscopic photographs. The presence of dermoscopic signs associated with BCC (blue ovoid nests, globules, specks of brown and grey pigment, leaf-like structures, spoke wheel areas, concentric structures, arborizing telangiectasias, linear and short telangiectasias, multiple erosions, ulceration, reddish-white areas, and bright white structures) (5) was recorded in each case, as well as the response to PDT, evaluated by clinical and dermoscopic signs, performing a biopsy in doubtful cases, with a minimum follow-up period of 9 months. Non-responders were treated with surgery.
RESULTS
A total of 29 patients with a histological diagnosis of BCC (10 nodular and 19 superficial) were included in the study. The only dermoscopic pattern that was significantly associated with lack of response to PDT and/or recurrence, regardless of histological type, was the presence of spoke wheel areas (p = 0.043). Values approaching significance were obtained for other signs related to the presence of pigment, such as leaf-like structures, and concentric structures (p = 0.063 in both cases). Blue globules, spoke wheel areas, and concentric structures were significantly associated with recurrence (p = 0.022, p = 0.000, and p = 0.004, respectively). No such associations were observed for the remaining variables studied (Fig. 1 and Table I).
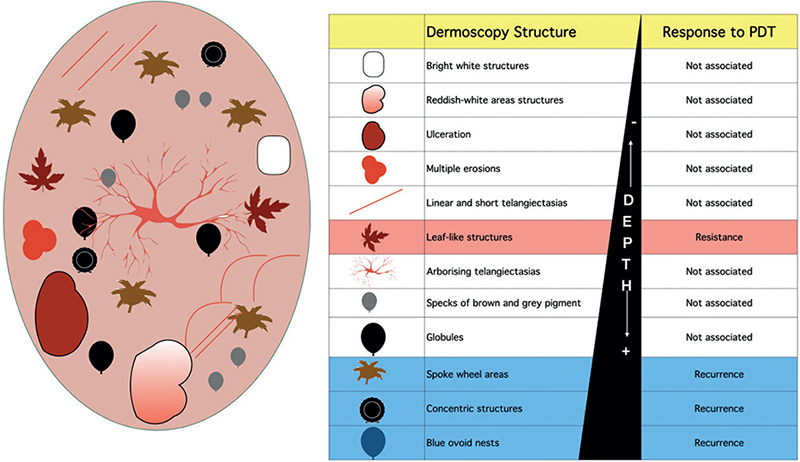
Fig. 1. Dermoscopic structures associated with basal cell carcinoma (BCC) and the response to photodynamic therapy (PDT).
DISCUSSION
In their study, Apalla et al. (4) highlighted the utility of dermoscopy as an adjuvant tool for naked-eye clinical examination to evaluate treatment outcome and monitoring of superficial BCCs after non-ablative therapy. The authors assessed residual disease-associated dermoscopic criteria proposed to predict the presence of residual/recurrent disease in all cases studied, and found that 21% of the lesions studied had been clinically miscategorised as achieving a complete response. In addition to these dermoscopic criteria, the current study describes new prognostic patterns, which should be evaluated before opting for non-ablative therapies, such as PDT.
This study found that superficial pigmented structures in BCCs located at the dermal-epidermal junction and superficial papillary dermis, such as spoke wheels, concentric structures, and leaf-like structures, were associated with a lack of response to PDT. This may be explained by the limited passage of light through these structures. Deeper pigment structures, such as globules, which are more characteristic of nodular BCCs, have been associated with greater recurrence.
Dermoscopy could help identify structures typical of pigmented BCCs and improve the response to PDT of BCCs with pigmented structures prior to curettage or debulking (6), thus achieving greater efficacy.
Certain dermoscopic features of BCCs may be predictive of the response to PDT, thereby enabling optimal selection of clinical treatment and aiding follow-up.
REFERENCES
- Cameron MC, Lee E, Hibler BP, Barker CA, Mori S, Cordova M, et al. Basal cell carcinoma: Epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol 2019; 80: 303–317.
- Diffey BL, Langtry JA. Skin cancer incidence and the ageing population. Br J Dermatol 2005; 153: 679–680.
- Peris K, Fargnoli MC, Garbe C, Kaufmann R, Bastholt L, Seguin NB, et al.; European Dermatology Forum (EDF), the European Association of Dermato-Oncology (EADO) and the European Organization for Research and Treatment of Cancer (EORTC). Diagnosis and treatment of basal cell carcinoma: European consensus-based interdisciplinary guidelines. Eur J Cancer 2019; 118: 10–34.
- Apalla Z, Lallas A, Tzellos T, Sidiropoulos T, Lefaki I, Trakatelli M, et al. Applicability of dermoscopy for evaluation of patients’ response to nonablative therapies for the treatment of superficial basal cell carcinoma. Br J Dermatol 2014; 170: 809–815.
- Álvarez-Salafranca M, Ara M, Zaballos P. Dermoscopy in basal cell carcinoma: an updated review. Actas Dermosifiliogr (Engl Ed) 2021; 112: 330–338.
- Gracia-Cazaña T, González S, Juarranz A, Gilaberte Y. Methyl aminolevulinate photodynamic therapy combined with curettage debulking for pigmented basal cell carcinoma. Photodermatol Photoimmunol Photomed 2017; 33: 228–232.