ORIGINAL REPORT
Economic and Humanistic Burden in Paediatric Patients with Atopic Dermatitis
Roselie ACHTEN1#, Lisa VAN DER RIJST1#, Marjanne PIENA2, Hedda LAMERS1, Fleur DE BEER1, Marjolein DE BRUIN-WELLER1 and Marlies DE GRAAF1
1Department of Dermatology and Allergology, University Medical Center Utrecht, Utrecht and 2OPEN Health, Evidence & Access, Rotterdam, The Netherlands
#These authors contributed equally.
Data concerning the economic and humanistic burden in patients with paediatric atopic dermatitis (AD) and their families are scarce. This retrospective study investigated these burdens in paediatric patients with AD using maintenance treatment with topical corticosteroids and/or conventional systemic immunosuppressants. Patient-reported outcomes regarding quality of life, AD severity, and parental work-related impairment were completed at inclusion. Data on healthcare resource utilization and medication prescription were collected retrospectively over the previous 12 months. Patients were categorized into mild, moderate or severe AD, based on Eczema Area and Severity Index score and medication use. Costs per patient per year per AD severity category were calculated. A total of 101 patients (median age 11.0 years (interquartile range 7.5–14.0), 47.5% men) were included, of whom 38 had mild AD, 37 moderate AD, and 26 severe AD. Mean ± standard deviation (SD) total costs patient per year for mild, moderate and severe AD were €1,812 ± €1,280, €2,680 ± €3,127, and €5,861 ± €3,993, respectively. Highest total direct and indirect costs were found in patients with severe AD, mainly due to higher healthcare and medication costs. Highest humanistic burden was found in patients with moderate AD. For example, the median (interquartile range) Patient-Oriented Eczema Measure score was significantly higher in these patients compared with mild and severe AD (19.0 (15.0–24.0) vs 12.0 (8.8–15.0) and 17.0 (9.5–22.0), respectively). AD in paediatric patients incurs considerable direct and indirect costs, especially in patients with severe AD. The high humanistic burden in patients with moderate AD underlines the need for effective and safe new treatment options for children with AD.
Key words: atopic dermatitis; economic burden; humanistic burden; health-related quality of life; paediatric.
SIGNIFICANCE
This study investigated the economic and humanistic burden related to atopic dermatitis severity category in paedi-atric patients with atopic dermatitis and their families. In 101 paediatric patients with atopic dermatitis, total costs were calculated over the previous 12 months and patient-reported outcomes were completed. Total costs, including direct and indirect costs, increased with the severity of atopic dermatitis. The highest humanistic burden was found in patients with moderate atopic dermatitis, indicating possible undertreatment in this group. These data show that patients with atopic dermatitis incur a considerable impact of humanistic and economic burden. The results emphasize the need for effective and safe new treatment options for children with atopic dermatitis.
Citation: Acta Derm Venereol 2023; 103: adv00881. DOI https://doi.org/10.2340/actadv.v103.4842.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Dec 14, 2022; Published: Mar 8, 2023
Corr: Marlies de Graaf, Department of Dermatology and Allergology, University Medical Center Utrecht, Heidelberglaan 100, NL-3584 CX Utrecht, The Netherlands. E-mail: M.deGraaf-10@umcutrecht.nl
Competing interests and funding: MdB-W is a consultant, advisory board member, and/or speaker for AbbVie, Almirall, Aslan, Arena, Eli Lilly, Galderma, Janssen, Leo Pharma, Pfizer, Regeneron, and Sanofi-Genzyme. MdG is a consultant, advisory board member, and/or speaker for AbbVie, Eli Lilly, Leo Pharma, Novartis, Pfizer, Regeneron, and Sanofi-Genzyme.
The other authors have no conflicts of interest to declare
INTRODUCTION
Atopic dermatitis (AD) is a chronic inflammatory, itchy skin disease, characterized by exacerbations and remissions. The physician-diagnosed 1-year prevalence of paediatric AD in Europe varies between 1.8% and 17.0% (1, 2). Most patients with paediatric AD have mild AD, which can be well-controlled with intermittent use of low-potency topical corticosteroids and emollients. Approximately 33% of paediatric patients with AD have moderate-to-severe AD, which requires more challenging treatment, including continuous use of more potent topical corticosteroids, systemic immunosuppressants, and/or hospitalization (3).
Due to intensive time-consuming therapy, uncontrollable itch, atopic comorbidities, and difficult-to-control disease, AD has a major impact on the quality of life (QoL) of patients and their families. Humanistic burden, often presented as health-related quality of life (HRQoL) or patient burden, reflects the impact of disease on the QoL of patients, activities of daily living (ADL), caregiver health and caregiver QoL, and is assessed in health economic studies (3–5). Multiple studies have demonstrated that the QoL of paediatric patients and their caregivers reduces as the severity of AD increases (5–7).
Next to the humanistic burden, AD causes an economic burden in terms of direct and indirect costs related to AD (8, 9). Several studies in different countries have shown that the economic burden increases with AD severity (5, 8, 10, 11). A study including 5 countries worldwide showed that costs varied between USD71 (the Netherlands) and USD2.559 (Germany) per patient per year (PPY), depending on the population studied and expenses included (12). Both the economic and humanistic burden of AD in paediatric patients are often underestimated (13).
Limited data are available on the economic and humanistic burden per AD severity category in paediatric patients with AD and their families. More information on the economic and humanistic burden is needed in order to understand the association between the impact on QoL and costs PPY in paediatric patients with AD. This current study includes patients treated with maintenance treatment with topical corticosteroids and/or conventional systemic immunosuppressants. AD treatment is changing and new systemic therapies are becoming available; this study provides context regarding the value of new treatment options.
The aim of this study was to investigate the economic burden, including direct and indirect costs, and the humanistic burden, including patient-reported outcome measures, in children with mild, moderate, and severe AD and their families in a daily practice setting. Based on previous literature, it is hypothesized that the economic and humanistic burden will increase with severity of AD (14–16).
METHODS
Study design and patient population
This retrospective cohort study included patients with AD from 4 to 17 years old between November 2018 and November 2021. All eligible patients were diagnosed with AD by a dermatologist or paediatrician at least 1 year prior to inclusion (17). All patients were treated at the Department of Dermatology and Allergology of Wilhelmina Children’s Hospital, University Medical Center Utrecht (UMCU), in the Netherlands. The study was approved by the local medical research ethics committee Utrecht as a non-interventional study (METC 18-725) and was performed according to the Declaration of Helsinki. All patients and/or caregivers gave written informed consent.
Patients were categorized into mild, moderate, and severe AD based on the Eczema Area and Severity Index (EASI) score at inclusion, which was stratified as following: EASI 0–5.9 (mild AD), EASI 6–22 (moderate AD) and EASI 23–72 (severe AD) (18). Patients who were treated with systemic immunosuppressants (cyclosporine A, methotrexate and/or prednisolone) at inclusion or in the previous year were classified as patients with severe AD, regardless of their EASI score at inclusion. Electronic patient files were reviewed by a dermatologist (MdG) to determine severity categories from patients with missing EASI scores and from patients hospitalized for AD in the previous year. Paediatric patients treated with new systemic therapies (e.g. biologics and Janus kinase (JAK)-inhibitors) and patients and parents who were unable to complete Dutch questionnaires were excluded.
Data collection
Depending on the patients’ age at inclusion, questionnaires regarding AD, atopic comorbidities, and the economic and humanistic burden of AD were completed by patients and/or their caregivers. Data regarding healthcare resource use were collected retrospectively over a 12-month period. Information about the treatment for AD and atopic comorbidities (asthma, allergic rhinitis, and food allergy) was obtained by analysing electronic medical records from the hospital, pharmacists, the general practitioner (GP), and other healthcare institutions.
Economic burden of disease
Resource utilization. Healthcare resource utilization was categorized into outpatient visits including telephone consultations per healthcare provider and hospitalization. A distinction was made between tertiary and secondary care. Total medication use included systemic immunosuppressants, topical treatment, treatment for atopic comorbidities, and other AD-related treatments (e.g. antibiotics and antihistamines). Furthermore, both self-care products and bandage material/anti-bacterial clothing were taken into account. Diagnostic and laboratory tests were included per patient. Google Maps (Mountain View, CA: Google LLC) was used to determine the geographical distance between the patients’ residence and the UMCU. Lastly, absenteeism of employed caregivers was evaluated by the caregivers’ reported missed hours of work due to their child’s AD.
Costs. The Dutch Costing Manual (DCM) for Economic Evaluations in Health Care, published by the Dutch National Health Care Institute, was used to determine the costs related to AD and atopic comorbidities (19). The DCM describes reference prices from 2014, which were adjusted for inflation until 2021 using the Consumer Price Index constructed by Statistics Netherlands (20). Costs were calculated PPY. All expenses made 1 year prior to inclusion were categorized into direct and indirect costs (Table SI). Direct costs were defined as costs directly related to AD or atopic comorbidities, including healthcare costs (outpatient visits, hospitalization and diagnostic and laboratory tests), medication costs, transportation costs, and estimated out-of-pocket costs. Medication prices (including 9% medication tax) were obtained from the online drugs registry from the Dutch National Health Care Institute (21). Diagnostic and laboratory costs included a laboratory fee, the fee charged for dispensing medication. Indirect costs, defined as costs due to absenteeism of employed caregivers because of their child with AD, were calculated using the human capital method (22).
Humanistic burden of disease
Validated questionnaires were used to examine the patientreported severity of AD, as this could affect QoL, and the impact on QoL of daily and social activities of patients and their families (23–30). These questionnaires were qualified to represent the different dimensions of health (physical and psychosocial), defined as the humanistic burden. The visual analogue scale (VAS), a numerical rating scale from absent (score 0) to severe (score 10), was used to measure pain and itch in the previous 7 days. The Patient-Oriented Eczema Measure (POEM) questionnaire (0–2=clear or almost clear AD, 3–7=mild AD, ≥8=moderate AD, and ≥17=severe AD) was used to evaluate severity of AD during the previous week (23, 24). The EuroQoL 5 Dimensions Youth (EQ-5D-Y) was completed to measure health-related QoL, defined by “problems” or “no problems” (25). The impact of AD on QoL of patients and their families was measured with the Children’s Dermatology Life Quality Index (CDLQI) (2–6=small effect, 7–12=moderate effect, and ≥13=large effect) and the Dermatitis Family Impact (DFI) (6–10=low impact, ≥11=moderate impact and >20=high impact). Although anxiety is often reported as a comorbidity in AD, anxiety can additionally affect humanistic burden. Therefore, the paediatric anxiety short-form of the Patient-Reported Outcomes Measurement Information System (PROMIS) was used to report anxiety experienced in the previous 7 days for paediatric patients aged ≥8 years (28, 29). The reported outcomes were rescaled into T-scores using the PROMIS scoring table (T-scores >50 indicated more anxiety compared with the mean population) (31).
Caregivers’ work impairment and impairment in daily activities regarding the previous 7 days were measured by using the Work Productivity and Activity Impairment (WPAI) questionnaire for caregivers of AD (30). Higher outcomes of the WPAI indicated greater impairment and less work productivity.
Statistical analysis
Patients were categorized into mild, moderate or severe AD, based on EASI score and/or use of systemic immunosuppressive drugs. The χ2 test and the Fisher’s exact test were used to assess differences between categorical variables. Normally distributed data were expressed as means and standard deviations (SD). Non-normally distributed data were expressed in medians and interquartile ranges (IQR). Costs by AD severity were compared using Kruskal–Wallis H-test. The Pearson’s χ2 test and Mann–Whitney U tests were used to compare differences within the severity groups. p-values were corrected for multiple testing by use of the Benjamini-Hochberg method, which controls false discovery rate (FDR) (32). For all analyses, a FDR adjusted p-value of <0.05 was considered statistically significant. Data analyses were conducted using IBM SPSS Statistics, Version 26 (Armonk, NY: IBM Corp) (33). Figures were created using Prism (GraphPad Prism version 9.3.0 for Windows, GraphPad Software, San Diego, CA, USA).
RESULTS
Patient characteristics
A total of 101 patients (median (IQR) age 11.0 years (7.5–14.0), 47.5% men) were included: 38 with mild AD, 37 with moderate AD, and 26 with severe AD. Median (IQR) age of AD onset was 0 years (0.0–1.0). The highest EASI scores were found in patients with moderate AD (11.0 (IQR 7.6–15.2)) followed by patients with severe AD (7.7 (IQR 3.4–16.5)), and mild AD (3.1 (IQR 1.7–3.9)). Among the total cohort, 11.9% (n=12) patients were hospitalized for AD in the previous year and 25.7% (n=26) patients were treated with systemic immunosuppressants for AD in the previous year. All other patient characteristics are shown in Table I.
| Total cohort (n=101) | Mild AD(n=38) | Moderate AD (n=37) | Severe AD(n=26) | |
| Male, n (%) | 48 (47.5) | 19 (50.0) | 17 (45.9) | 12 (46.2) |
| Age, years, median (IQR) | 11.0 (7.5–14.0) | 9.0 (5.0–14.0) | 11.0 (9.0–14.0) | 14.0 (10.5–15.3) |
| Age onset AD, years, median (IQR) | 0.0 (0.0–1.0) | 0.0 (0.0–0.0) | 0.0 (0.0–2.0) | 0.0 (0.0–1.0) |
| Hospitalized for AD in the previous year, n (%) | 12 (11.9) | 0.0 (0.0) | 4 (10.8) | 8 (30.8) |
| Systemic immunosuppressants as treatment for AD in the previous yeara, n (%) | 26 (25.7) | 0.0 (0.0) | 0.0 (0.0) | 26 (100.0) |
| Cyclosporine A, n (%) | 26 (25.7) | 0.0 (0.0) | 0.0 (0.0) | 26 (100.0) |
| Methotrexate, n (%) | 3 (3.0) | 0.0 (0.0) | 0.0 (0.0) | 3 (11.5) |
| Prednisolone, n (%) | 6 (5.9) | 0.0 (0.0) | 0.0 (0.0) | 6 (23.1) |
| Mycophenolate mofetil, n (%) | 1 (1.0) | 0.0 (0.0) | 0.0 (0.0) | 1 (3.8) |
| Dexamethasone, n (%) | 1 (1.0) | 0.0 (0.0) | 0.0 (0.0) | 1 (3.8) |
| Atopic diseases | ||||
| Asthma, n (%) | 42 (41.6) | 14 (36.8) | 16 (43.2) | 12 (46.2) |
| Allergic rhinitis, n (%) | 63 (62.4) | 21 (55.3) | 24 (64.9) | 18 (69.2) |
| Food allergy, n (%) | 51 (50.5) | 19 (50.0) | 18 (48.6) | 14 (53.8) |
| EASI, median (IQR) | 5.7 (3.0–11.3) | 3.1 (1.7–3.9) | 11.0 (7.6–15.2) | 7.7 (3.4–16.5) |
| Missing, n (%) | 9 (8.9) | 2 (5.3) | 3 (8.1) | 4 (15.4) |
| IGA, median (IQR) | 2.0 (2.0–3.0) | 2.0 (1.5–2.0) | 3.0 (2.0–3.0) | 2.0 (2.0–3.2) |
| Missing, n (%) | 14 (13.9) | 5 (13.2) | 4 (10.5) | 5 (19.2) |
| aSome patients were treated with multiple systemic immunosuppressants for atopic dermatitis (AD). | ||||
| IQR: interquartile range; SD: standard deviation; EASI: Eczema Area and Severity Index; IGA: Investigator’s Global Assessment. | ||||
Economic burden of disease
Mean total costs, including direct and indirect costs, were €3,145 (SD ± €3,265), shown in Table II and Fig. 1. Mean ± SD total costs PPY were €1,812 ± €1,280 for mild AD, €2,680 ± €3,127 for moderate AD, and €5,861 ± €3,993 for severe AD (p<0.001). Patients with severe AD most frequently visited the outpatient clinic, and were more often hospitalized in the previous 12 months compared with patients with mild or moderate AD. This resulted in significantly higher healthcare utilization costs in patients with severe AD, compared with patients with mild or moderate AD (p<0.001). Indirect costs were highest in patients with moderate AD (€696 ± 2,272), compared with mild (€300 ± 847) and severe AD (€601 ± 929). No significant differences were found within these 3 groups.
| Total cohort (n=101)Mean ± SD | Mild AD (n=38)Mean ± SD | Moderate AD (n=37)Mean ± SD | Severe AD (n=26)Mean ± SD | p-value* | Adjusted p-value | |
| Total direct costs | 2,680 ± 2,744 | 1,512 ± 854 | 1,984 ± 2,093 | 5,377 ± 3,518 | < 0.001 | < 0.001 |
| Total healthcare costs | 1,567 ± 2,129 | 725 ± 368 | 1,308 ± 1,859 | 3,167 ± 3,018 | < 0.001 | < 0.001 |
| Total medication costs | 709 ± 738 | 393 ± 394 | 385 ± 287 | 1,632 ± 799 | < 0.001 | < 0.001 |
| Emollients therapy | 110 ± 142 | 111 ± 151 | 78 ± 87 | 156 ± 179 | 0.113 | 0.147 |
| Topical corticosteroids | 119 ± 117 | 98 ± 132 | 105 ± 88 | 169 ± 118 | 0.002 | 0.004 |
| Topical immunomodulators | 20 ± 53 | 21 ± 41 | 10 ± 22 | 33 ± 89 | 0.353 | 0.382 |
| Systemic immunosuppressants | 240 ± 524 | 0 ± 0 | 0 ± 0 | 930 ± 657 | < 0.001 | < 0.001 |
| Other medication | 74 ± 158 | 58 ± 134 | 80 ± 205 | 91 ± 112 | 0.004 | 0.007 |
| Diagnostic (incl. laboratory) costs | 63 ± 125 | 47 ± 85 | 47 ± 103 | 108 ± 183 | 0.002 | 0.004 |
| Transportation costs | 126 ± 112 | 95 ± 73 | 114 ± 102 | 189 ± 147 | 0.008 | 0.012 |
| Out-of-pocket costs | 215 ± 423 | 252 ± 548 | 130 ± 155 | 281 ± 467 | 0.853 | 0.853 |
| Total indirect costs | ||||||
| Absenteeism caregivers | 521 ± 1545 | 300 ± 847 | 696 ± 2272 | 601 ± 929 | 0.286 | 0.338 |
| Total costs | 3,145 ± 3,265 | 1,812 ± 1,280 | 2,680 ± 3,127 | 5,861 ± 3,993 | < 0.001 | < 0.001 |
| AD: atopic dermatitis; SD: standard deviation. All data is presented in Euro (€). | ||||||
| *p-value <0.05 was considered significant. p-values were adjusted for multiple testing using the Benjamini-Hochberg method, controlling the false discovery rate (FDR) (32). | ||||||
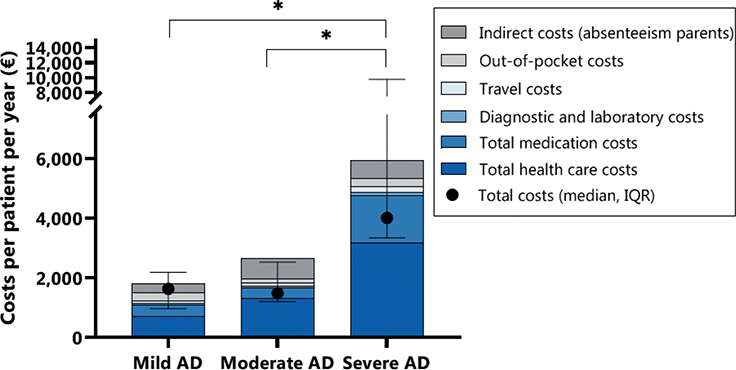
Fig. 1. Mean total direct and indirect costs per cost category and per atopic dermatitis (AD) severity category. Data of costs per patient per year were skewed, median and interquartile (IQR) range are shown.
Humanistic burden of disease
Among all included patients, the median POEM score was 15.0 (IQR 10.0–20.0) and the median VAS itch was 6.0 (IQR 3.0–8.0) (Fig. 2, Table III, Table SII). A significantly higher POEM score was reported in patients with moderate AD, compared with patients with mild AD and severe AD (p < 0.001). Subsequently, a higher VAS itch was found in patients with moderate AD compared with patients with mild and severe AD (p=0.003). Median CDLQI scores were comparable within patients with moderate AD and those with severe AD, and were significantly higher compared with patients with mild AD (p = 0.003). Since only a few patients were aged 16 or 17 years, limited patients completed the DLQI (n = 15) and no statistically significant differences within the severity categories could be analysed. PROMIS T-scores were comparable between all severity groups. School absenteeism, expressed in median days per year, was highest in patients with severe AD (9.0 days (IQR 3.0–20.0)), followed by patients with moderate and mild AD (4.0 days (IQR 1.0–8.8) and 1.0 day (IQR 0.0–3.0), respectively, p = <0.001).
| Total cohort (n=101) | Mild AD (n=38) | Moderate AD (n=37) | Severe AD (n=26) | p-value* | Adjusted p-value | |
| POEM, median (IQR)a | 15.0 (10.0–20.0) | 12.0 (8.8–15.0) | 19.0 (15.0–24.0) | 17.0 (9.5–22.0) | <0.001 | <0.001 |
| Missing, n (%) | 2 (2.0) | 0 (0.0) | 0 (0.0) | 2 (7.7) | ||
| VAS itch, median (IQR)b | 6.0 (3.0–8.0) | 5.0 (2.0–7.0) | 8.0 (5.0–8.0) | 5.0 (3.0–8.3) | 0.001 | 0.003 |
| VAS pain, median (IQR)b | 3.0 (1.0–5.0) | 2.0 (0.0–3.3) | 3.0 (0.5–6.5) | 4.0 (2.0–5.0) | 0.014 | 0.037 |
| CDLQI, median (IQR)b | 8.0 (4.0–12.0) | 5.0 (3.0–8.0) | 9.0 (7.0–12.0) | 9.5 (4.0–15.8) | 0.001 | 0.003 |
| Completed by parents, n (%) | 86 (85.1) | 35 (92.1) | 31 (83.8) | 20 (76.9) | ||
| DLQI, median (IQR)c | 6.0 (2.0–13.0) | 2.0 (1.0–n/a) | 12.5 (4.8–14.8) | 8.0 (3.3–13.8) | 0.142 | 0.214 |
| Completed by patients, n (%) | 15 (14.9) | 3 (7.9) | 6 (16.2) | 6 (23.1) | ||
| DFI, median (IQR)d | 5.0 (2.3–9.0) | 3.5 (2.0–8.0) | 6.0 (3.0–10.0) | 6.0 (1.0–13.0) | 0.110 | 0.214 |
| Missing, n (%) | 1 (1.0) | 0 (0.0) | 0 (0.0) | 1 (3.8) | ||
| EQ-5D-Y**, n (%)a | ||||||
| Mobility | 0.794 | 0.822 | ||||
| Problems | 11 (10.9) | 5 (13.2) | 3 (8.1) | 3 (11.5) | ||
| No Problems | 88 (87.1) | 33 (86.8) | 33 (89.2) | 22 (84.6) | ||
| Self-care | 0.822 | 0.822 | ||||
| Problems | 27 (26.7) | 10 (26.3) | 9 (24.3) | 8 (30.8) | ||
| No Problems | 72 (71.3) | 28 (73.7) | 27 (73.0) | 17 (65.4) | ||
| Daily activity | 0.422 | 0.482 | ||||
| Problems | 38 (37.6) | 12 (31.6) | 14 (37.8) | 12 (46.2) | ||
| No Problems | 61 (60.4) | 26 (68.4) | 22 (59.5) | 13 (50.0) | ||
| Pain/discomfort | 0.147 | 0.214 | ||||
| Problems | 60 (59.4) | 19 (50.0) | 26 (70.3) | 15 (57.7) | ||
| No Problems | 39 (38.6) | 19 (50.0) | 10 (27.0) | 10 (38.5) | ||
| Anxiety/depression | 0.100 | 0.214 | ||||
| Problems | 42 (41.6) | 11 (28.9) | 18 (48.6) | 13 (50.0) | ||
| No Problems | 57 (56.4) | 27 (71.1) | 18 (48.6) | 12 (46.2) | ||
| Missing, n (%) | 2 (2.0) | 0 (0.0) | 1 (2.7) | 1 (3.8) | ||
| VAS EQ-5D-Y, median (IQR)a | 80.0 (70.0–90.0) | 82.5 (80.0–91.8) | 75.0 (70.0–90.0) | 65.0 (50.0–79.0) | <0.001 | <0.001 |
| Missing, n (%) | 3 (3.0) | 0 (0.0) | 1 (2.7) | 2 (7.7) | ||
| T-score PROMIS anxiety, median (IQR)e | 54.8 (50.9–62.1) | 53.5 (49.6–58.5) | 56.0 (50.9–63.9) | 56.0 (49.9–63.0) | 0.268 | 0.357 |
| Missing due to age, n (%) | 25 (24.8) | 13 (34.2) | 8 (21.6) | 4 (15.4) | ||
| Missing, n (%) | 4 (4.0) | 2 (2.0) | 0 (0.0) | 2 (7.7) | ||
| Impairment in caregivers’ work, median (IQR)d | 0.0 (0.0–20.0) | 0.0 (0.0–17.5) | 0.0 (0.0–19.2) | 20.0 (0.0–60.0) | 0.126 | 0.214 |
| Missing due to unemployment, n (%) | 14 (13.9) | 5 (13.2) | 6 (16.2) | 3 (11.5) | ||
| Missing, n (%) | 10 (9.9) | 3 (7.9) | 4 (10.8) | 3 (11.5) | ||
| Impairment in caregivers’ daily activities, median (IQR)d | 10.0 (0.0–30.0) | 10.0 (0.0–22.5) | 0.0 (0.0–20.0) | 10.0 (0.0–57.5) | 0.375 | 0.462 |
| Missing, n (%) | 2 (2.0) | 0 (0.0) | 0 (0.0) | 2 (7.7) | ||
| School absenteeism, days per year, median (IQR)d | 3 (0.1–8.8) | 1.0 (0.0–3.0) | 4.0 (1.0–8.8) | 9.0 (3.0–20.0) | <0.001 | <0.001 |
| Missing, n (%) | 5 (5.0) | 1 (2.6) | 1 (2.7) | 3 (11.5) | ||
| aQuestionnaire completed by caregivers of patients aged <16 years and by patients aged ≥16 years. bQuestionnaire completed by caregivers of patients aged <12 years and by patients aged 12–17 years. cQuestionnaire completed in by patients aged 17 years. dQuestionnaire completed by caregivers. eQuestionnaire completed by patients aged ≥8 years. | ||||||
| *p-value <0.05 was considered significant. p-values were adjusted for multiple testing using the Benjamini-Hochberg method, controlling the false discovery rate (FDR) (32). | ||||||
| **EQ-5D-Y, “problems” include “some problems” and “problems” with the concomitant dimension. | ||||||
| IQR: interquartile range; SD: standard deviation; POEM: Patient Oriented Eczema Measure; VAS: visual analogue scale; CDLQI: Children’s Dermatology Life Quality Index; DFI: Dermatitis Family Impact; PROMIS: Patient-Reported Outcomes Measurement Information System. | ||||||

Fig. 2. Results of the patient-reported outcomes. Median and interquartile range (IQR) are shown. Children’s Dermatology Life Quality Index (CDLQI) for patients aged 4–15 years (n=86), Dermatology Life Quality Index (DLQI) for patients aged >16 years (n=15). AD: atopic dermatitis; POEM: Patient Oriented Eczema Measure; VAS: Visual Analogue Scale; DFI: Dermatitis Family Impact. †Statistical test was not applicable due to the low number of patients.
In addition, the median DFI score was slightly higher in families of patients with moderate or severe AD, compared with families of patients with mild AD (p = 0.214). Of the employed caregivers, the caregivers of patients with severe AD reported the highest work impairment in days per year (20.0 days (IQR 0.0–60.0), p = 0.214).
DISCUSSION
This study investigated the economic and humanistic burden associated with mild, moderate, and severe AD in paediatric patients in the Netherlands. The findings indicate that the total costs increase with AD severity, confirming the study hypothesis. Furthermore, the study found that all severity groups experienced impact on QoL due to AD. The highest impact on QoL was found in patients with moderate AD.
The economic burden of paediatric patients with AD, expressed as the mean ± SD total costs PPY, was €3,145 ± 3,265 (equivalent to USD 3,279 ± 3,404, daily exchange rate conversion on 4 July 2022). As disease severity increased, higher expenditures were found in healthcare costs (outpatient visits and hospitalization) followed by medication costs. Patients treated with systemic immunosuppressants were classified as having severe AD, which explains the high medication costs in this group compared with patients with mild or moderate AD. The reported costs are in line with results of studies from Italy (USD 1,540), Germany (USD 2,559), and Singapore (USD 7,943) (8, 10, 12). Consistent with studies from the USA, Italy, Singapore, Australia, and Israel, the costs PPY increased as AD severity increased (5, 8, 10, 11, 34, 35). In line with the current results, a recent study from Israel reported that the highest expenses in paediatric patients with AD were due to frequent healthcare-related visits and higher use of medication (11). Other studies reported different expenses or used different methodology, which complicates the comparison of direct and indirect costs of patients with AD (8, 10, 12). Nevertheless, the trend of these studies is similar to the current study. To compare the economic burden among different countries worldwide, equivalent methodology is necessary, and differences of the various national healthcare systems should be taken into account.
The significant impact on QoL in all severity categories in this paediatric cohort demonstrates the need for improvement in disease management for AD. The highest impact on QoL was seen in patients with moderate AD who also had the highest disease activity, reflected by the highest median EASI score. This implicates that the impact on QoL increases as the disease severity worsens, which is supported by previous studies (5–7). Disease severity and impact on QoL in patients with moderate AD were higher compared with patients with severe AD. This might be explained by the use of systemic immunosuppressants in patients with severe AD, resulting in better controlled disease with lower humanistic burden. This could indicate that patients with moderate AD in this cohort may have been undertreated and may require systemic immunosuppressants. The decision to initiate systemic immunosuppressants is made on an individual basis and is usually considered in severe cases (36, 37). However, physicians’ reluctance to prescribe conventional systemic agents may play a part in this decision, as the side-effect profiles and risks of long-term toxicity are known barriers to prescribing systemic agents, such as cyclosporine A and methotrexate (38). This highlights the unmet need for the development of new, effective, and safe systemic agents for paediatric patients with AD. Recently, new systemic agents have been approved and reimbursed in the Netherlands for the treatment of paediatric patients with moderate-to-severe AD: dupilumab for the treatment of children ≥ 6 years and upadacitinib for adolescents ≥ 12 years of age (14–16). These new therapies and the development of future treatment options may address the unmet need in the treatment of children with AD and improve AD disease management.
The high impact on economic and humanistic burden raises the question of what level of costs is acceptable to achieve well-controlled disease, and thus improvement in QoL of paediatric patients with AD. In the current study, patients with severe AD had significantly higher costs compared with patients with mild and moderate AD, and had a lower humanistic burden compared with patients with moderate AD. To establish an association between the level of costs acceptable for controlled disease, a longer follow-up time of these patients is necessary. In particular, when noting the established impact of uncontrolled disease in childhood and in adulthood due to social impact in childhood and/or academic and work-related impact in adulthood, Zuberbier et al. (39) reported that career progression was hindered by AD in 14% of participating adult patients. Ariens et al. (9) showed that work-absenteeism in adulthood leads to high indirect costs, which play an important role in the total costs and could not be taken into account in this paediatric study. Uncontrolled disease is undesirable, and can lead to avoidable socioeconomic costs of AD in terms of lost productivity and effect on learning capacity in younger patients. Furthermore, Zuberbier et al. (39) suggested that both the individual and socioeconomic costs of AD could be reduced if better treatment options were offered, which again indicates the unmet need for safe and effective treatment for AD.
Study limitations
This study has some limitations. The cross-sectional design may have led to recall bias, possibly over- or under-estimating the impact on economic and humanistic burden. However, most data on the economic burden were collected retrospectively using data from healthcare institutions, reducing the risk of bias. Secondly, the COVID-19 pandemic may have influenced the results, as there were fewer physical consultations and more flexibility in the working hours of caregivers, which may have led to an underestimation of costs. Lastly, as this study was conducted in a tertiary expertise AD centre in the Netherlands, the humanistic and economic impact cannot be generalized for patients with AD in primary or secondary care, and may reflect a higher impact on disease burden and costs.
Conlusion
This study shows that AD in paediatric patients incurs a high economic burden, with considerable direct and indirect costs, which increases as the severity of AD increases. In addition, an impact on humanistic burden was found in all patients, especially in the group of patients with moderate AD. Notably, disease activity and impact on humanistic burden was the highest in this group, which may indicate undertreatment of moderate paediatric AD patients, possibly due to a lack of effective and safe systemic agents. This study highlights the unmet need for new and safe systemic agents for paediatric patients with AD. Further research is needed to evaluate the economic and humanistic burden in paediatric patients with AD in relation to the use of new systemic therapies.
ACKNOWLEDGEMENTS
This investigator-initiated study was sponsored by Sanofi Genzyme. The sponsor was not involved in the collection, analysis, interpretation or publication of the data.
REFERENCES
- Asher MI, Montefort S, Björkstén B, Lai CK, Strachan DP, Weiland SK, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet 2006; 368: 733–743.
- Bylund S, Kobyletzki LB, Svalstedt M, Svensson A. Prevalence and Incidence of Atopic Dermatitis: A Systematic Review. Acta Derm Venereol 2020; 100: adv00160.
- Silverberg JI, Simpson EL. Associations of childhood eczema severity: a US population-based study. Dermatitis 2014; 25: 107–114.
- Filanovsky MG, Pootongkam S, Tamburro JE, Smith MC, Ganocy SJ, Nedorost ST. The financial and emotional impact of atopic dermatitis on children and their families. J Pediatr 2016; 169: 284–290.e5.
- Hebert AA, Stingl G, Ho LK, Lynde C, Cappelleri JC, Tallman AM, et al. Patient impact and economic burden of mild-to-moderate atopic dermatitis. Curr Med Res Opin 2018; 34: 2177–2185.
- Carroll CL, Balkrishnan R, Feldman SR, Fleischer AB, Jr., Manuel JC. The burden of atopic dermatitis: impact on the patient, family, and society. Pediatr Dermatol 2005; 22: 192–199.
- Chiesa Fuxench ZC, Block JK, Boguniewicz M, Boyle J, Fonacier L, Gelfand JM, et al. Atopic dermatitis in america study: a cross-sectional study examining the prevalence and disease burden of atopic dermatitis in the US adult population. J Invest Dermatol 2019; 139: 583–590.
- Olsson M, Bajpai R, Wee LWY, Yew YW, Koh MJA, Thng S, et al. The cost of childhood atopic dermatitis in a multi-ethnic Asian population: a cost-of-illness study. Br J Dermatol 2020; 182: 1245–1252.
- Ariens LFM, van Nimwegen KJM, Shams M, de Bruin DT, van der Schaft J, van Os-Medendorp H, et al. Economic burden of adult patients with moderate to severe atopic dermatitis indicated for systemic treatment. Acta Derm Venereol 2019; 99: 762–768.
- Ricci G, Bendandi B, Pagliara L, Patrizi A, Masi M. Atopic dermatitis in Italian children: evaluation of its economic impact. J Pediatr Health Care 2006; 20: 311–315.
- Weil C, Sugerman PB, Chodick G, Liang H, Wang H, Calimlim BM, et al. Epidemiology and economic burden of atopic dermatitis: real-world retrospective data from a large nationwide Israeli Healthcare Provider Database. Adv Ther 2022; 39: 2502–2514.
- Verboom P, Hakkaart-Van L, Sturkenboom M, De Zeeuw R, Menke H, Rutten F. The cost of atopic dermatitis in the Netherlands: an international comparison. Br J Dermatol 2002; 147: 716–724.
- Mancini AJ, Kaulback K, Chamlin SL. The socioeconomic impact of atopic dermatitis in the United States: a systematic review. Pediatr Dermatol 2008; 25: 1–6.
- Simpson EL, Paller AS, Siegfried EC, Boguniewicz M, Sher L, Gooderham MJ, et al. Efficacy and safety of dupilumab in adolescents with uncontrolled moderate to severe atopic dermatitis: a phase 3 randomized clinical trial. JAMA Dermatol 2020; 156: 44–56.
- Paller AS, Siegfried EC, Thaci D, Wollenberg A, Cork MJ, Arkwright PD, et al. Efficacy and safety of dupilumab with concomitant topical corticosteroids in children 6 to 11 years old with severe atopic dermatitis: a randomized, double-blinded, placebo-controlled phase 3 trial. J Am Acad Dermatol 2020; 83: 1282–1293.
- Reich K, Teixeira HD, de Bruin-Weller M, Bieber T, Soong W, Kabashima K, et al. Safety and efficacy of upadacitinib in combination with topical corticosteroids in adolescents and adults with moderate-to-severe atopic dermatitis (AD Up): results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2021; 397: 2169–2181.
- Hanifin JM, Thurston M, Omoto M, Cherill R, Tofte SJ, Graeber M. The eczema area and severity index (EASI): assessment of reliability in atopic dermatitis. EASI Evaluator Group. Exp Dermatol 2001; 10: 11–18.
- Chopra R, Vakharia PP, Sacotte R, Patel N, Immaneni S, White T, et al. Severity strata for Eczema Area and Severity Index (EASI), modified EASI, Scoring Atopic Dermatitis (SCORAD), objective SCORAD, Atopic Dermatitis Severity Index and body surface area in adolescents and adults with atopic dermatitis. Br J Dermatol 2017; 177: 1316–1321.
- Guideline for conducting economic evaluations in health care (2015). National Health Care Institute, Diemen. Available from: www.zorginstituutnederland.nl.
- Netherlands S. Consumer price index 2018. [accessed Jan 2021] Available from: http://statline.cbs.nl/StatWeb/publication/?VW=T&DM=SLNL&PA=83131ned.
- Medicijnkosten.nl (2017). National Health Care Institute, Diemen. Available from: www.medicijnkosten.nl.
- van den Hout WB. The value of productivity: human-capital versus friction-cost method. Ann Rheum Dis 2010; 69: i89–91.
- Charman CR, Venn AJ, Ravenscroft JC, Williams HC. Translating Patient-Oriented Eczema Measure (POEM) scores into clinical practice by suggesting severity strata derived using anchor-based methods. Br J Dermatol 2013; 169: 1326–1332.
- Charman CR, Venn AJ, Williams HC. The patient-oriented eczema measure: development and initial validation of a new tool for measuring atopic eczema severity from the patients’ perspective. Arch Dermatol 2004; 140: 1513–1519.
- Wille N, Badia X, Bonsel G, Burström K, Cavrini G, Devlin N, et al. Development of the EQ-5D-Y: a child-friendly version of the EQ-5D. Qual Life Res 2010; 19: 875–886.
- Lewis-Jones MS, Finlay AY. The Children’s Dermatology Life Quality Index (CDLQI): initial validation and practical use. Br J Dermatol 1995; 132: 942–949.
- Lawson V, Lewis-Jones MS, Finlay AY, Reid P, Owens RG. The family impact of childhood atopic dermatitis: the Dermatitis Family Impact Questionnaire. Br J Dermatol 1998; 138: 107–113.
- Haverman L, Grootenhuis MA, Raat H, van Rossum MA, van Dulmen-den Broeder E, Hoppenbrouwers K, et al. Dutch-Flemish translation of nine pediatric item banks from the Patient-Reported Outcomes Measurement Information System (PROMIS)®. Qual Life Res 2016; 25: 761–765.
- Terwee CB, Roorda LD, de Vet HC, Dekker J, Westhovens R, van Leeuwen J, et al. Dutch-Flemish translation of 17 item banks from the patient-reported outcomes measurement information system (PROMIS). Qual Life Res 2014; 23: 1733–1741.
- Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics 1993; 4: 353–365.
- Patient-Reported Outcomes Measurement Information System Anxiety, Dynamic Tools to Measure Health Outcomes From the Patient Perspective, 2015: 1-11.
- Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Strat Soc 1995; 57: 289–300.
- IBM Corp. IBM SPSS Statistics for Windows, Version 26.0; IBM Corp.: Armonk, NY, USA, 2019. Available online: https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-26.
- Fivenson D, Arnold RJ, Kaniecki DJ, Cohen JL, Frech F, Finlay AY. The effect of atopic dermatitis on total burden of illness and quality of life on adults and children in a large managed care organization. J Manag Care Pharm 2002; 8: 333–342.
- Su JC, Kemp AS, Varigos GA, Nolan TM. Atopic eczema: its impact on the family and financial cost. Arch Dis Child 1997; 76: 159–162.
- Wollenberg A, Christen-Zach S, Taieb A, Paul C, Thyssen JP, de Bruin-Weller M, et al. ETFAD/EADV Eczema task force 2020 position paper on diagnosis and treatment of atopic dermatitis in adults and children. J Eur Acad Dermatol Venereol 2020; 34: 2717–2744.
- Boguniewicz M, Fonacier L, Guttman-Yassky E, Ong PY, Silverberg J, Farrar JR. Atopic dermatitis yardstick: practical recommendations for an evolving therapeutic landscape. Ann Allergy Asthma Immunol 2018; 120: 10–22.e2.
- Totri CR, Eichenfield LF, Logan K, Proudfoot L, Schmitt J, Lara-Corrales I, et al. Prescribing practices for systemic agents in the treatment of severe pediatric atopic dermatitis in the US and Canada: the PeDRA TREAT survey. J Am Acad Dermatol 2017; 76: 281–285.
- Zuberbier T, Orlow SJ, Paller AS, Taïeb A, Allen R, Hernanz-Hermosa JM, et al. Patient perspectives on the management of atopic dermatitis. J Allergy Clin Immunol 2006; 118: 226–232.