SHORT COMMUNICATION
Possible Association Between Melanoma Arising from Congenital Naevus and Oestrogen or Progesterone Receptor Expression: Clinicopathological Analysis
Chiho SUMITOMO1, Yohei IWATA1*, Yasuhiro SAKAI2, Tetsuya TSUKAMOTO3 and Kazumitsu SUGIURA1
Department of 1Dermatology, 2Joint Research Laboratory of Clinical Medicine, and 3Diagnostic Pathology, Fujita Health University School of Medicine, 1-98 Dengakugakubo, Kutsukake-cho, Toyoake, Aichi 470-1192, Japan. *E-mail: iwayou@fujita-hu.ac.jp
Citation: Acta Derm Venereol 2023; 103: adv00887. DOI: https://doi.org/10.2340/actadv.v103.5206.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Feb 1, 2023; Published: Mar 14, 2023
Competing interests and funding: The authors have no conflicts of interest to declare.
Malignancies such as breast cancer, melanoma, cervical cancer, lymphoma, or acute leukaemia reportedly occur in approximately 0.1% of all pregnancies (1). Of these, melanoma, which has a high metastatic potential, is one of the most common malignancies (accounting for approximately 8% of all malignancies) diagnosed during pregnancy (1). Levels of circulating sex hormones (oestrogen and progesterone) increase during pregnancy, and this increases tumorigenesis, possibly due to mechanisms involved in maternal–foetal immune tolerance (2). The influence of oestrogen on melanoma progression is varied and has been shown to both promote and hinder melanoma growth (2, 3). Thus, the effect of sex hormones on melanoma development remains unclear.
This study performed clinicopathological analysis, using immunostaining of oestrogen receptor (ER) and progesterone receptor (PR), in 42 cases of melanoma.
MATERIALS AND METHODS
To assess the association between sex hormones and melanoma, the expression of ER and PR in melanoma cells was examined. Forty-two skin specimens (from 17 men and 25 women; mean age ± standard deviation, 67 ± 16 years; range 28–91 years), that were diagnosed as melanoma at the Fujita Health University, Toyoake, Japan, between June 2013 and February 2019, were retrieved from the archives, in retrospect, to perform haematoxylin and eosin (H&E), ER- and PR-staining. Immunostaining for ER and PR was performed on paraffin sections using an HX System Discovery Automated Immunostainer (Roche, Basel, Swiss) with a polymer-based detection system, according to the manufacturer’s instructions. The primary antibodies used were rabbit anti-human ERα (1:200; clone SP1; Abcam, Cambridge, UK) and rabbit anti-human PR (1:100; clone 1E2; Roche). Ten high-power fields (magnification, ×400) in the tumour lesion were randomly selected, the staining patterns of ER and PR were assessed according to the Allred score (4), and the samples were categorized in 2 groups: + (positive; Allred score ≥ 3), and – (negative; Allred score < 3). Written informed consent was obtained from all patients and tissue donors according to the Declaration of Helsinki. Informed consent for skin samples was obtained for each collection according to the protocols approved by the Institutional Review Board of Fujita Health University.
RESULTS
The histopathological features of melanoma are summarized in Table SI. According to the Allred score, tumour cells tested positive for ER and PR in 3 female specimens (cases 1–3; mean age, 34 ± 5 years; age range 28–40 years), while those in other specimens tested negative (Fig. 1). ER and PR were found to be expressed in the nuclei of tumour cells in all 3 positive cases. Case 1 and 2 were pregnant. Case 3 had a history of two pregnancies. Notably, in the 3 positive specimens, black macule was present since birth or childhood, and the melanoma developed and spread rapidly during pregnancy or after childbirth. The presence of naevi near the melanoma was histopathologically confirmed in all 3 positive cases (Fig. 2).
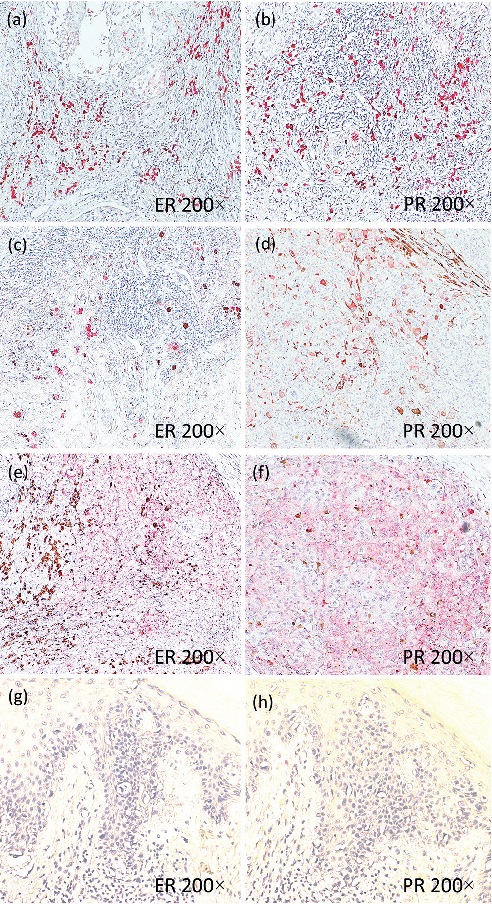
Fig. 1. Tumour cells tested positive for oestrogen receptor and progesterone receptor in cases 1–3. Case 1: tumour cells are positive for (a) oestrogen receptor (ER) and (b) progesterone receptor (PR). Case 2: tumour cells are positive for (c) ER and (d) PR. Case 3: tumour cells are positive for (e) ER and (f) PR. Control (Table SI. Number 38): tumour cells are negative for (g) ER and (h) PR. (a–h 200×).
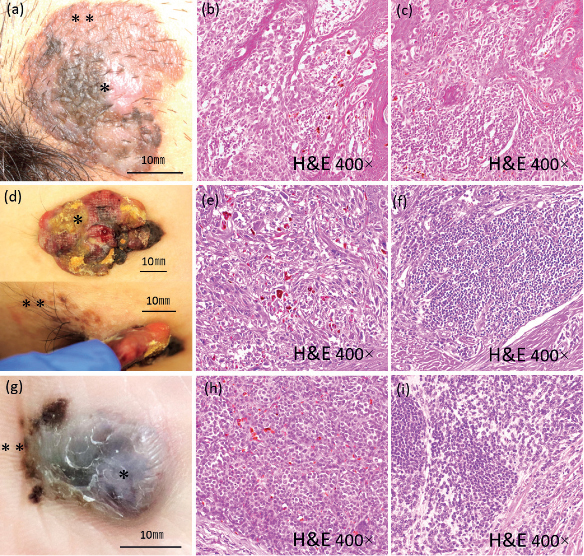
Fig. 2. Clinical images and haematoxylin and eosin staining of cases 1-3. Case 1: (a) Clinical image, 30×30 mm sized multicolored macule in the lower abdomen. (b) H&E staining of tumor cells (*). (c) H&E staining of nevus cells (**). Case 2: (d) Clinical image, 50× 35 mm sized multicolored tumor on her right buttock. (e) H&E staining of tumor cells (*). (f) H&E staining of nevus cells (**). Case 3: (g) Clinical image, 25 × 15 mm sized tumor and black macule on her right heel. (h) H&E staining of tumor cells (*). (i) H&E staining of nevus cells (**). (b,c,e,f,h,i. 400×)
DISCUSSION
The human chorionic gonadotropin and oestrogen that increase during early pregnancy and from early to mid-pregnancy, respectively, tend to suppress apoptosis and promote vascular growth (3). Progesterone suppresses Th1 cells and induces immune tolerance (3). Therefore, the risk of melanoma development, proliferation, and metastasis increase in the early to mid-pregnancy stages (3). In contrast, the secretion of oestrogen, progesterone, corticotrophin-releasing hormone, and prolactin increases during late pregnancy, which may induce the resolution of melanomas due to Th1 induction, apoptosis promotion, and suppression of vascular hyperplasia (3). Sex hormone receptor expression is induced during pregnancy or while using oral contraceptives, which may increase the risk of melanoma development and may be associated with pigment changes in melanoma precursor lesions (5). However, the association between hormone receptor expression and melanoma development is contradictory (6–10). Recent studies investigating G protein-coupled oestrogen receptor (GPER) on cultured melanoma cells have shown that selective GPER activation induced long-term changes that maintained a more differentiated cell state, increased pigment production, decreased proliferative capacity, and decreased expression of the onco-driver and stem cell marker c-Myc (11).
In the current study, 3 patients with pregnancy-related melanoma (cases 1–3) had black macules present from birth or early childhood, and the melanomas developed and rapidly enlarged during pregnancy, after childbirth, or hormonal therapy. The tumour size at resection was ≥ 20 mm in all 3 cases. Pathological findings showed that the melanoma cells were positive for ER and PR; and naevus cells were observed near the melanoma. In contrast, 22 out of 25 women (mean age 68 ± 12 years; range 45–91 years) had no preceding black macules, and the melanoma development was unrelated to pregnancy. The melanoma cells were pathologically negative for ER and PR in these 22 women. These findings indicate that melanoma developed from congenital naevus in the 3 pregnant patients. Furthermore, the study findings also suggest that the expression of ER and PR may be involved in the rapid growth of melanoma and in the development of melanoma from naevi.
In summary, melanoma development from naevi and rapid tumour growth in patients in this study may be related to both immune tolerance induced by sex hormones and receptor expression in melanoma cells. Furthermore, the expression of ER and PR may be involved in the rapid growth and development of melanoma. Therefore, studying ER and PR expression for early diagnosis, may help predict the rapid growth of pregnancy-related melanoma or in melanoma with a history of sex hormone exposure. To date, the distinct effects of sex hormones on melanoma progression remain unclear, and the impact of pregnancy-related hormonal changes on melanoma development and progression remains controversial (12). Nevertheless, careful clinical evaluation of suspicious lesions is essential for the early diagnosis of melanoma during pregnancy.
ACKNOWLEDGEMENTS
The authors would like to thank Yoshihito Tanaka, Kenta Saito, and Tamaki Maeda for their technical assistance.
Written informed consent was obtained from all patients and tissue donors in accordance with the Declaration of Helsinki. Informed consent for skin samples was obtained for each collection in accordance with the protocols approved by the Institutional Review Board of Fujita Health University.
REFERENCES
- Zagouri F, Dimitrakakis C, Marinopoulos P, Tsigginou A, Dimopoulos MA. Cancer in pregnancy: disentangling treatment modalities. ESMO Open 2016; 1: 1–6.
- Still R, Brennecke S. Melanoma in pregnancy. Obstet Med 2017; 10: 107–112.
- Enninga EA, Holtan SG, Creedon DJ, Dronca RS, Nevala WK, Ognjanovic S, et al. Immunomodulatory effects of sex hormones: requirements for pregnancy and relevance in melanoma. Mayo Clin Proc 2014; 89: 520–535.
- Allred DC, Harvey JM, Berardo M, Clark GM. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod Pathol 1998; 11: 155–168.
- Ellis DL, Wheeland RG. Increased nevus estrogen and progesterone ligand binding related to oral contraceptives or pregnancy. J Am Acad Dermatol 1986; 14: 25–31.
- Caldarola G, Battista C, Pellicano R. Melanoma onset after estrogen, thyroid, and growth hormone replacement therapy. Clin Ther 2010; 32: 57–59.
- Dika E, Fanti PA, Vaccari S, Capizzi E, Degiovanni A, Gobbi A, et al. Oestrogen and progesterone receptors in melanoma and nevi: an immunohistochemical study. Eur J Dermatol 2017; 27: 254–259.
- Lyn MD, Robin LT, Frederick CK, Martin CM, Arthur JS. Estrogen and progesterone receptor analysis in pregnancy-associated melanoma: absence of immunohistochemically detectable hormone receptors. Hum Pathol 1994; 25: 36–41.
- Dika E, Patrizi A, Lambertini M, Manuelpillai N, Fiorentino M, Altimari A, et al. Estrogen receptors and melanoma: a review. Cells 2019; 8: 1463.
- Dika E, Lambertini M, Lauriola M, Veronesi G, Ricci C, Tartari F, et al. Female melanoma and estrogen receptors expression: an immunohistochemical pilot study. Melanoma Res 2022; 32: 231–240.
- Natale CA, Li J, Zhang J, Dahal A, Dentchev T, Stanger BZ, et al. Activation of G protein-coupled estrogen receptor signaling inhibits melanoma and improves response to immune checkpoint blockade. Elife 2018; 7: e31770.
- Todd SP, Driscoll MS. Prognosis for women diagnosed with melanoma during, before, or after pregnancy: weighing the evidence. Int J Womens Dermatol 2017; 3: 26–29.