ORIGINAL REPORT
Happiness Behind the Scenes: Associations between Heuristic Happiness and Related Dimensions in Skin Diseases
Johanna WEIS1#, Hannah WECKER1#, Alexander ARNOLD1,2, Barbara SCHUSTER1, Stefanie ZIEHFREUND1, Linda TIZEK1, Sonja MITTAG1, Tilo BIEDERMANN1 and Alexander ZINK1,3
1Department of Dermatology and Allergy, Technical University of Munich, School of Medicine, Munich, 2Private Practice, Dermatologie Arnold, Augsburg, Germany and 3Division of Dermatology and Venereology, Department of Medicine Solna, Karolinska Institutet, Stockholm, Sweden
#Shared first authorship.
Positive health approaches, such as happiness, are largely unexplored in medicine, including dermatology. Taking into consideration the various happiness measures, the aims of this cross-sectional study were to assess this concept using a 1-item heuristic happiness question and its related dimensions (Satisfaction with Life, Positive and Negative Affect, Quality of Life, and Compound Psychological Capital) in outpatients with different skin diseases between December 2019 and June 2020, and to examine the link between these dimensions. Overall, 414 dermatological patients were included: 67 with psoriasis, 84 atopic eczema, 10 mastocytosis, 19 nummular eczema, 84 malignant melanoma and 150 keratinocyte carcinoma. Comparing the skin diseases, differences were observed for heuristic happiness, Positive Affect, and some domains of Quality of Life and Compound Psychological Capital. Analysing the relationship between heuristic happiness and other happiness measures, the data revealed moderate to strong correlations (r = 0.30–0.46, p< 0.001) and variations in the understanding of happiness between the skin diseases. Overall, the most important facet of happiness was Hope as a domain of Compound Psycho-logical Capital. This study emphasizes the individual definition of heuristic happiness in patients with skin diseases. A 1-item heuristic approach may be a simple and practical method to assess the complexity and individuality of happiness.
Key words: happiness; quality of life; holistic health; skin diseases.
SIGNIFICANCE
Everyone has their own definition of happiness and associates different conditions with it. Consequently, there are multiple measures, including the 1-item heuristic happiness question (“Taking all things together, how happy would you say you are?”). The aims of this study were to assess 6 different happiness measures in patients with skin disease and to investigate the relationship between these measures. Differences in the happiness measures were observed, and the interpretation and associated conditions of happiness varied between different skin diseases. Hence, a 1-item happiness question may be a useful approach to reflect the individual understanding of happiness.
Citation: Acta Derm Venereal 2023; 103: adv5284. DOI: https://doi.org/10.2340/actadv.v103.5284.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Feb 13, 2023; Published: May 30, 2023
Corr: Alexander Zink, Technical University of Munich, School of Medicine, Department of Dermatology and Allergy, Munich, Germany. E-mail: alexander.zink@tum.de
Competing interests and funding: JW received an unrestricted research grant from Novartis Pharma. BS received research grants from Novartis Pharma and started working at Beiersdorf AG after finishing her work on this paper. LT has received speaker honoraria from Janssen-Jilag and received an unrestricted research grant from Novartis Pharma. TB gave advice to or got a honorarium for talks or research grant from the following companies: AbbVie, Alk-Abelló, Celgene-BMS, Lilly Deutschland GmbH, Mylan, Novartis, Phadia-Thermo Fisher, p-95 for Curevac, Sanofi-Genzyme, Regeneron, Viatris. AZ has been an advisor and/or received speaker’s honoraria and/or received grants and/or participated in clinical trials of the following companies: AbbVie, Almirall, Amgen, Beiersdorf Dermo Medical, Bencard Allergie, BMS, Celgene, Eli Lilly, GSK, Janssen Cilag, Leo Pharma, Miltenyi Biotec, Novartis, Pfizer, Sanofi-Aventis, Takeda Pharma, UCB Pharma. HW, SM, AA, and SZ have no conflicts of interest to declare.
INTRODUCTION
Skin diseases are ranked as the 4th leading cause of disability worldwide (1). In Germany, skin diseases are among the most common reasons for seeking medical care (2), which is primarily provided by dermatologists and general practitioners in outpatient settings (3). Different skin diseases vary in their severity and can cause substantial physical, psychological, and social impairments (4–7). Traditionally, most empirical research in dermatology has taken a problem-oriented approach by investigating how psychological stress and disease are related to poor health outcomes, such as wound healing (8) and depression (9). In contrast, positive health concepts, such as happiness, have remained largely unexplored in dermatology, but have been stated as essential to comprehensively understand skin diseases (7).
The health benefits of happiness and well-being have been increasingly emphasized in medical and sociopsychological research (10–12). There is growing evidence that happiness reduces pain in chronic diseases and has the potential to lower the incidence or moderate the severity of various diseases (13, 14). Happy people tend to have better health outcomes through better integrative thinking, creativity, and resilience (15).
In literature, happiness has different meanings (16) and is mainly used to describe positive subjective experiences (17). Subjective well-being (SWB) provides one of the most widely adopted definitions of happiness (18). This model is based on individual satisfaction with life (SWL) (19) and the predominance of positive affect (PA) over negative affect (NA) (18). In this taxonomy, happiness includes both cognitive and affective appraisals of life and is synonymously used with SWB (18). Happiness has also been conceptualized as an evaluation of individual’s quality of life (QoL) (12) and is often used interchangeable with other positive health dimensions, such as optimism (17). Depending on the context, happiness has different definitions (20) and thus highlights the relationship and a certain overlap between happiness and related dimensions (12, 16).
The increasing number of measuring tools for happiness has led to extensive debate about the most appropriate methods among researchers, clinicians, and policymakers (15, 16, 20). Happiness is often included as single-item question in population-based surveys. The European Social Survey (ESS) asks: “Taking all things together, how happy would you say you are?” (21). As this question should be answered quickly and unconsciously, it follows a heuristic approach and is therefore defined as heuristic happiness (7). Additional scales attempt to measure further related dimensions, such as the Satisfaction with Life Scale (SWLS) (22), Scale of Positive and Negative Experience (SPANE) (23), Quality of Life Questionnaire (WHOQOL-BREF) (24), and the scale measuring Compound Psychological Capital (CPC-12) (25). The simplification to a 1-item question supports better comparisons and saves time in medical practice. However, to fully understand heuristic happiness as a concept, one should also study its associated dimensions.
The aim of this study was to assess heuristic happiness and its related dimensions in dermatological outpatients. The second aim was to investigate the relationship between heuristic happiness and other common and validated happiness-related measures for a better understanding of happiness in skin diseases.
MATERIALS AND METHODS
Study design
A cross-sectional study was conducted in a dermatological outpatient practice in Augsburg (Greater Munich area, Southern Germany). Patients affected by psoriasis, atopic eczema (AE), nummular eczema, mastocytosis, malignant melanoma, or keratinocyte carcinoma (KC) were recruited consecutively from December 2019 to June 2020. The inclusion criteria were at least 1 confirmed diagnosis of the aforementioned diseases, age ≥ 18 years, and being able to read and understand German. Patients meeting these criteria were asked to complete the paper-based questionnaire and provided written informed consent prior to study inclusion.
The study was reviewed and approved by the ethics committee of the Medical Faculty at Technical University of Munich (reference 424/17S) and conducted in accordance with the ethics standards of the Declaration of Helsinki.
Measures
Data were collected using structured questionnaires including age, sex, and happiness measures validated in the German language. The treating physician documented the diagnosis.
Heuristic happiness was assessed with the single-item Happiness Thermometer from the ESS (21), which uses an 11-point Likert scale (0–10: extremely unhappy to extremely happy).
SWL was evaluated with SWLS (22), consisting of 5 items rated on a 7-point Likert scale (1–7: strongly disagree to strongly agree). The items were summed to a total score ranging from 5 to 35, with higher scores indicating higher life satisfaction (19).
PA and NA were measured with SPANE (23), which consists of 12 items. Six items relate to the frequency of general and specific PA and 6 to general and specific NA. Each item is scored on a 5-point Likert scale (1–5: very rarely/never to very often/always). Two independent total scores ranging from 6 (= lowest) to 30 (= highest) were built by summing the corresponding 6 items for each PA and NA.
QoL was assessed with WHOQOL-BREF (24), consisting of 26 items with a 5-point Likert scale (1–5: very poor/very dissatisfied/not at all to very good/very satisfied/extremely). Scores were transformed into a continuous scale from 0 to 100, with higher values indicating higher QoL, and divided into 4 different domains: physical health (QoL-Physical), psychological health (QoL-Psychological), social relationships (QoL-Social), and environmental (QoL-Environmental). Scores were then summarized by a total score (QoL-Total).
CPC was evaluated with CPC-12 (25), consisting of 4 domains with each 3 items for hope (CPC-Hope), optimism (CPC-Optimism), resilience (CPC-Resilience), and self-efficacy (CPC-Self-efficacy). All 12 items were surveyed using a 6-point Likert scale (1–6: strongly/totally disagree to strongly agree). For each domain a mean score was calculated separately and all domains were summarized to a total score (CPC-Total).
The internal consistency of the scales was assessed with Cronbach’s alpha. QoL (0.92), SWLS (0.91), and CPC (0.91) had excellent reliability and PA (0.89) and NA (0.87) had good reliability.
Missing values
Data were checked for unclear (e.g. multiple diagnoses, n = 4) and implausible answers (e.g. multiple answers in 1 question, n = 1) and excluded afterwards. Observations with more than 20% missing values in each happiness scale (n = 15) were omitted. For linear regression, further 12 participants had to be excluded because they either did not report their sex (n = 2) or belonged to the small patient group of mastocytosis (n = 10).
Statistical analysis
Only QoL-Total was normally distributed. To test for differences between sexes, a Mann-Whitney U test, a χ2-test for categorical data, and a t-test for QoL-Total were used. To assess the differences between skin diseases, Kruskal-Wallis tests, χ2-tests for categorical variables, and analysis of variance (ANOVA) for QoL-Total were performed. For t-tests and ANOVA, the assumption of equal variances was checked with Levene’s test.
Spearman’s correlations (r) were calculated to examine the relationship between continuous variables. To investigate these associations in more detail, multiple linear regression with heuristic happiness as an outcome variable was conducted. SWL, PA, NA, QoL, CPC domains, skin diseases, sex, and age squared (Fig. S1) were included as predictor variables. To account for differences between sex and skin diseases in the happiness-related scales, interaction terms were included in the full model. A stepwise selection was performed using Akaike information criterion to identify only relevant variables. Model assumptions such as linearity, normality, and homoscedasticity were checked using residual plots. Since all scores tend to examine the same subject, multicollinearity had to be considered. Pearson correlation and variance inflation factor (VIF) were used to assess multicollinearity, with correlation r > 0.7 and/or VIF ≥ 10 being commonly used cut-off values (26, 27). If at least 1 cut-off value was exceeded, 1 of the affected variables had to be removed.
Statistical analyses were performed using R version 4.0.4 (28). Graphical representations of the correlations were created by hand based on the R package “corrplot” (29). The significance level was set to α = 0.05.
RESULTS
Descriptive data
In total, 434 dermatological patients were recruited. After checking for validity, data from 414 patients were analysed: 67 (16.2%) with psoriasis, 84 (20.3%) AE, 10 (2.4%) mastocytosis, 19 (4.6%) nummular eczema, 84 (20.3%) malignant melanoma, and 150 KC (36.2%, Table I). Overall, 218 (52.9%) participants were women and the median age was 47.00 (interquartile range (IQR) 35.00–60.00) years.
Differences in sex and skin diseases affecting happiness scores
Sex differences were observed between the skin diseases (p = 0.017). Heuristic happiness, SWL, NA, CPC-Total, CPC-Hope, CPC-Optimism, and CPC-Resilience were similar for both sexes (0.050 ≤ p ≤ 0.610). Women reported better PA, QoL-Total, all QoL domains, and CPC-Self-efficacy (0.002 ≤ p ≤ 0.032, Table I).
Differences in median age were observed for the different skin diseases (p < 0.001, Table II). Comparing the happiness scales, greater differences were observed for heuristic happiness, PA, QoL-Physical, QoL-Social, CPC-Hope, CPC-Self-efficacy, and in both total scores (0.002 ≤ p ≤ 0.028). The remaining scales were rated more similarly in different dermatological conditions (0.058 ≤ p ≤ 0.386). In general, patients with nummular eczema, mastocytosis, and KC scored lower on most scales than other patients, with KC patients showing higher variability in nearly all happiness scores.
Correlation analysis in dermatological patients
Among all patients, low negative associations were found between age and the different happiness scores (|r| = 0.12–0.23, 0.001 ≤ p ≤ 0.016) with an exception for NA, which showed low positive association (r = 0.12, p = 0.018). Low to strong positive correlations were shown between the different happiness scores among all skin conditions, with exceptions for NA, which demonstrated negative associations (r = 0.14–0.87, 0.001 ≤ p ≤ 0.003). The domains of QoL and CPC correlated highly with their total scores. In general, the data indicated moderate to strong correlations between heuristic happiness and other happiness-related scores (|r| = 0.30–0.46, p < 0.001), with highest correlations with CPC-Hope (r = 0.46) and SWL (r = 0.45) (Fig. 1, Table SI).
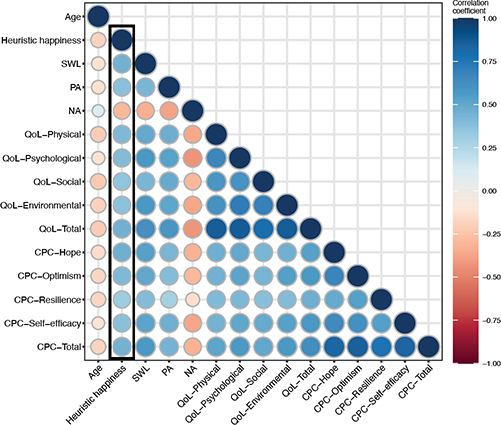
Fig. 1. Spearman’s correlations between heuristic happiness and happiness-related scales in skin diseases. SWL: satisfaction with life; PA: positive affect; NA: negative affect; QoL: quality of life; CPC: Compound Psychological Capital.
Since differences were observed for the skin diseases, correlations between heuristic happiness and related dimensions were calculated separately for each skin disease (Fig. 2, Tables SII–SVII):
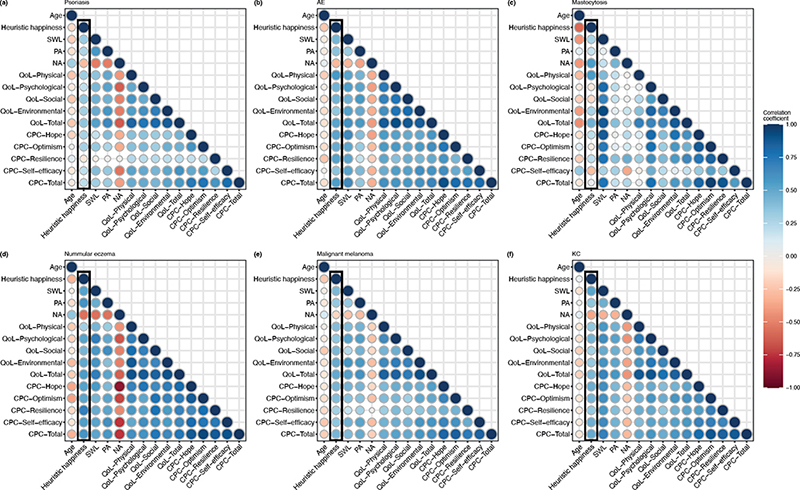
Fig. 2. Spearman’s correlations between heuristic happiness and happiness-related scales in patients with (a) psoriasis, (b) atopic eczema (AE), (c) mastocytosis, (d) nummular eczema, (e) malignant melanoma, and (f) keratinocyte carcinoma (KC). SWL: satisfaction with life; PA: positive affect; NA: negative affect; QoL: quality of life; CPC: Compound Psychological Capital.
Psoriasis. Mild to moderate correlations were observed, with the highest correlation documented for QoL-Social (r = 0.35, p = 0.004) and the lowest for CPC-Resilience (r = –0.10, p = 0.399).
Atopic eczema. Moderate to strong correlations were found. The highest correlations were identified for QoL-Physical (r = 0.57, p < 0.001), CPC-Resilience (r = 0.52, p < 0.001), and CPC-Hope (r = 0.52, p < 0.001) and the lowest for NA (r = –0.30, p = 0.006).
Mastocytosis. Heuristic happiness correlated slightly to strongly with the related dimensions (|r| = 0.04–0.56, 0.096 ≤ p ≤ 0.921), with partly reversed directions compared with other skin diseases.
Nummular eczema. Moderate to strong correlations were observed. The highest correlation was seen for CPC-Resilience (r = 0.70, p < 0.001) and the lowest for QoL-Physical (r = 0.30, p = 0.215).
Malignant melanoma. Heuristic happiness showed low to moderate correlation with the related dimensions. Highest correlations were observed for QoL-Environmental (r = 0.48, p < 0.001) and CPC-Hope (r = 0.43, p < 0.001), while lowest for NA (r = –0.18, p = 0.109) and CPC-Resilience (r = 0.29, p = 0.008).
Keratinocyte carcinoma. Moderate to strong correlations were observed. Highest correlations were shown for SWL (r = 0.51, p < 0.001) and CPC-Hope (r = 0.47, p < 0.001) and the lowest for QoL-Social (r = 0.30, p < 0.001).
Furthermore, this study investigated the correlation between heuristic happiness and happiness-related scores for different age categories. All age categories showed low to stronger correlations (|r| = 0.18–0.52, 0.001 ≤ p ≤ 0.178, Table SVIII).
Regression model of heuristic happiness
To examine the relationship between heuristic happiness and happiness-related scores in more detail, a linear regression model was generated (n = 402). Two scores each had to be removed after stepwise selection (QoL-Social, CPC-Self-efficacy) and checking for multicollinearity (QoL-Environmental, CPC-Optimism). In the final model, CPC-Hope played an important role in heuristic happiness in all patients (Table III). The outcome variable was slightly associated with QoL-Psychological and negatively associated with NA. Differences in effects were found for SWL, PA, QoL-Physical, and CPC-Resilience in different skin diseases as seen in the interaction terms, while PA, QoL-Physical, and CPC-Resilience, showed either a positive or negative effect on heuristic happiness. In particular, CPC-Resilience showed a greater effect in nummular eczema and AE, whereas it was negatively associated with other skin diseases.
DISCUSSION
Studies on the role of happiness, particularly in dermatology, are limited. Comparing happiness scores, differences were observed in each dermatological disease. Overall, the associations between heuristic happiness and its related dimensions demonstrated moderate to strong correlations that differed between skin diseases. The regression indicated that CPC-Hope was important for heuristic happiness in all patients, while QoL-Social and CPC-Self-efficacy played no significant role for patients.
The current study observed sex and age differences between patients, as incidence rates and mortality differ depending on a patient’s age and sex. For example, men are more frequently affected than women by KC (30), and its occurrence is closely associated with advanced age (2). Most happiness scores were approximately the same for both sexes as seen in previous research (31–33). However, some studies report contradictory results (6, 34). Analyses demonstrated negative correlations between age and nearly all happiness scores. These results align with those of other studies reporting lower Psychological Capital, SWL, and QoL among elderly people (31, 32). The relationship between age and happiness is still discussed in the literature (33). Further research is necessary for a more differentiated picture of happiness in relation to age and sex.
The ESS (n = 2,358, mean (age): 49.7 ± 19.1 years, 48.6% women) showed that the happiness of the general German population, who stated being almost extremely happy (mean: 9.1) (21), exceeded that of dermatological patients (mean: 7.3) in the current study. In line with Schuster et al., this study also reported lower levels of heuristic happiness in dermatological patients compared with healthy controls (7).
The higher frequency of PA as opposed to NA in this study is consistent with the definition of SWB as a dimension related to happiness (10, 15). A previous study also identified stronger associations between SWL and optimism than pessimism (22). Different happiness dimensions are linked to several health-promoting behaviours and improved stress management (10, 11, 15). Studies in dermatology have found significant relationships between stress-related factors and the occurrence, severity, and progression of skin diseases (8). People with skin diseases reported lower PA compared with healthy controls (7), emphasizing the importance of positive psychological interventions (7, 9, 11). These methods potentially support both patients and physicians by motivating self-regulation, reducing time needed to understand health conditions, and expediting referrals to psychological specialists (32). Although interventions have been positively evaluated, they still need to be adapted for dermatological practice and integrated into interdisciplinary treatment approaches (11, 32).
Physical activity decreases with age and the presence of disease (13, 32), which may explain why physical health demonstrated the lowest scoring within the 4 domains of QoL in this study. Patients with KC and nummular eczema, the 2 oldest patient groups, showed the lowest scores and correlations with heuristic happiness for QoL-Physical and -Psychological. QoL-Social and -Environmental were not indicated as important in explaining heuristic happiness in most patients due to lower correlations and model exclusion. This finding appears consistent with that of a small sample of healthy university students (16).
Analyses indicated that especially CPC-Hope was important in explaining heuristic happiness in all patients, as CPC-Hope reflects a positive psychological state (25). The aforementioned association between stress and skin disease may be a reason for the lower rating of CPC-Resilience in all patients. Only for patients affected by nummular eczema and AE was resilience of higher importance in explaining heuristic happiness. A review demonstrated that children and adolescents affected by AE are severely impaired by problems such as embarrassment and bullying because of their visible skin lesions (5). Patients burdened in this manner may have formed coping strategies at an early age and consequently view resilience as an important factor for individual happiness. People with nummular eczema tend to have histories of AE (35), hence resilience may play a similar role in their happiness. Several studies have shown that patients with skin diseases have lower self-esteem than controls (36), which is probably attributed to the stigmatization of visible skin lesions (5). Since self-esteem and self-efficacy are closely related (37), this might be reflected in the low importance of self-efficacy in all patients.
Overall, the current study found that dermatological patients diagnosed with nummular eczema, mastocytosis, or KC scored lower in most happiness scores than other patient groups. One reason may be the small sample size for 2 of the 3 groups. In particular, the smallest group, comprising patients affected by mastocytosis, showed the highest intra- and inter-variations in ratings and correlations of happiness scales, e.g. the positive correlation between heuristic happiness and NA. These rather inconsistent ratings complicated comparisons. Some findings, such as the low scoring for QoL-Social, are consistent with previous studies (38). Larger study samples are required for a more in-depth understanding of happiness and, particularly, of happiness in mastocytosis.
Moderate to strong correlations between heuristic happiness and happiness-related scores indicate the theoretical and conceptual intersection of the dimensions. This raises the question of whether an overlap leads to redundancy (12, 16, 17). Simplifying a universal heuristic happiness measurement requires more attention in health research and clinical practice for better comparisons and time-saving (9). One concern regarding 1-item measures is that they do not encompass the detail and breadth that can be achieved with multiple measures (39). Further studies are needed to compare single-item vs multiple-item happiness measures and to develop a measure consisting of only a few items, with international applicability.
Study limitations
Although happiness as a state of mind may be universal, asking about happiness in different cultures and languages may assess different dimensions, consequently leading to biased results (40). Germans frequently associate happiness with unexpected events, which may be attributed to the fact that the German word “Glück” can mean both “happiness’’ and “luck’’. Therefore, these conclusions are valid only in a German language setting. It should also be considered that a different order of happiness-related measures in the questionnaire could have led to different results (17). Another limitation is selection bias, as recruitment occurred in a single outpatient practice. The sample may therefore not be representative. Furthermore, the sample size was very small for skin diseases such as mastocytosis and nummular eczema, which may have led to biased results. Finally, the lack of a population-representative control group inhibits the evaluation of happiness measures in dermatological patients.
Conclusion
This study focused on positive health research to better understand its impact on skin diseases and the interaction between heuristic happiness and related happiness measures. The variations in skin diseases highlight the individual understanding of heuristic happiness, at least in a German context. Physicians should be trained to use positively framed questions to support patients to talk openly. This may lead to a better understanding of patients’ holistic health, focus their attention on a positive perspective, and potentially have a therapeutic effect. Overall, analysing heuristic happiness may present a practical approach to approximating and simplifying a complex concept, such as happiness in both clinical practice and research.
ACKNOWLEDGEMENTS
This work was supported by the Technical University of Munich, School of Medicine, Munich, Germany.
REFERENCES
- Karimkhani C, Dellavalle RP, Coffeng LE, Flohr C, Hay RJ, Langan SM, et al. Global skin disease morbidity and mortality: an update from the Global Burden of Disease Study 2013. JAMA Dermatol 2017; 153: 406–412.
- Tizek L, Schielein MC, Seifert F, Biedermann T, Böhner A, Zink A. Skin diseases are more common than we think: screening results of an unreferred population at the Munich Oktoberfest. J Eur Acad Dermatol Venereol 2019; 33: 1421–1428.
- Augustin M, Girbig G, Kis A, Bechara FG, Hertl M, Hischke S, et al. Inpatient care for skin diseases in Germany: multi-source analysis on the current and future health care needs. J Dtsch Dermatol Ges 2021; 19 Suppl 5: 25–53.
- Schuster B, Peifer C, Ziehfreund S, Tizek L, Biedermann T, Zink A, et al. Happiness and depression in psoriasis: a cross-sectional study in Germany. Qual Life Res 2021.
- Birdi G, Cooke R, Knibb RC. Impact of atopic dermatitis on quality of life in adults: a systematic review and meta-analysis. Int J Dermatol 2020; 59: e75–e91.
- Kowalewska B, Jankowiak B, Niedżwiecka B, Krajewska-Kułak E, Niczyporuk W, Khvorik DF. Relationships between the acceptance of illness, quality of life and satisfaction with life in psoriasis. Postepy Dermatol Alergol 2020; 37: 948–955.
- Schuster B, Ziehfreund S, Albrecht H, Spinner CD, Biedermann T, Peifer C, et al. Happiness in dermatology: a holistic evaluation of the mental burden of skin diseases. J Eur Acad Dermatol Venereol 2020; 34: 1331–1339.
- Graubard R, Perez-Sanchez A, Katta R. Stress and skin: an overview of mind body therapies as a treatment strategy in dermatology. Dermatol Pract Concept 2021; 11: e2021091.
- Guo F, Yu Q, Liu Z, Zhang C, Li P, Xu Y, et al. Evaluation of life quality, anxiety, and depression in patients with skin diseases. Medicine (Baltimore) 2020; 99: e22983.
- Diener E, Pressman SD, Hunter J, Delgadillo-Chase D. If, why, and when subjective well-being influences health, and future needed research. Appl Psychol Health Well Being 2017; 9: 133–167.
- Braunwalder C, Müller R, Glisic M, Fekete C. Are positive psychology interventions efficacious in chronic pain treatment? A systematic review and meta-analysis of randomized controlled trials. Pain Med 2022; 23: 122–136.
- Veenhoven R. Notions of the good life. In: David SA, Boniwell I, Ayers AC, editors. The Oxford handbook of happiness. Oxford: Oxford University Press, 2013.
- Zhang Z, Chen W. A systematic review of the relationship between physical activity and happiness. J Happiness Stud 2019; 20: 1305–1322.
- Kushlev K, Heintzelman SJ, Lutes LD, Wirtz D, Kanippayoor JM, Leitner D, et al. Does happiness improve health? Evidence from a randomized controlled trial. Psychol Sci 2020; 31: 807–821.
- Veenhoven R. Healthy happiness: effects of happiness on physical health and the consequences for preventive health care. J Happiness Stud 2008; 9: 449–469.
- Medvedev ON, Landhuis CE. Exploring constructs of well-being, happiness and quality of life. PeerJ 2018; 6: e4903.
- Carlquist E, Ulleberg P, Delle Fave A, Nafstad HE, Blakar RM. Everyday understandings of happiness, good life, and satisfaction: three different facets of well-being. Applied Research Quality Life 2017; 12: 481–505.
- Diener E, Wirtz D, Tov W, Kim-Prieto C, Choi D, Oishi S, et al. New well-being measures: short scales to assess flourishing and positive and negative feelings. Soc Indic Res 2010; 97: 143–156.
- Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess 1985; 49: 71–75.
- Bekhet AK, Zauszniewski JA, Nakhla WE. Happiness: theoretical and empirical considerations. Nurs Forum 2008; 43: 12–23.
- European Social Survey. ESS Round 9 Source Questionnaire: ESS ERIC Headquarters c/o City University London; 2016. [accessed Jul 11, 2022] Available from: http://www.europeansocialsurvey.org/data/country.html?c=germany.
- Hinz A, Conrad I, Schroeter ML, Glaesmer H, Brähler E, Zenger M, et al. Psychometric properties of the Satisfaction with Life Scale (SWLS), derived from a large German community sample. Qual Life Res 2018; 27: 1661–1670.
- Rahm T, Heise E, Schuldt M. Measuring the frequency of emotions – validation of the Scale of Positive and Negative Experience (SPANE) in Germany. PLoS One 2017; 12: e0171288.
- World Health Organization. WHOQOL-BREF: introduction, administration, scoring and generic version of the assessment. Geneva: World Health Organization, 1996. [accessed Jun 9, 2022] Available from: https://www.who.int/tools/whoqol/whoqol-bref.
- Dudasova L, Prochazka J, Vaculik M, Lorenz T. Measuring psychological capital: Revision of the Compound Psychological Capital Scale (CPC-12). PLoS One 2021; 16: e0247114.
- Dormann CF, Elith J, Bacher S, Buchmann C, Carl G, Carré G, et al. Collinearity: a review of methods to deal with it and a simulation study evaluating their performance. Ecography 2013; 36: 27–46.
- Fox J, Monette G. Generalized collinearity diagnostics. J Am Statist Assoc 1992; 87: 178.
- R Core Team (2021). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria.
- Taiyun Wei and Viliam Simko (2021). R package ’corrplot’: Visualization of a Correlation Matrix (Version 0.92). [Accessed Apr 19, 2022] Available from https://github.com/taiyun/corrplot.
- Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Piñeros M, Znaor A, et al. Cancer statistics for the year 2020: an overview. Int J Cancer 2021 Apr 5 [Online ahead of print].
- Dirzyte A, Perminas A, Biliuniene E. Psychometric properties of Satisfaction with Life Scale (SWLS) and Psychological Capital Questionnaire (PCQ-24) in the Lithuanian population. Int J Environ Res Public Health 2021; 18: 2608.
- Jankowiak B, Sekmistrz S, Kowalewska B, Niczyporuk W, Krajewska-Kułak E. Satisfaction with life in a group of psoriasis patients. Postepy Dermatol Alergol 2013; 30: 85–90.
- Karwetzky C, Michaelsen MM, Werdecker L, Esch T. The U-Curve of Happiness Revisited: Correlations and differences in life satisfaction over the span of life-an empirical evaluation based on data from 1,597 individuals aged 12–94 in Germany. Front Psychol 2022; 13: 837638.
- Joshanloo M, Jovanović V. The relationship between gender and life satisfaction: analysis across demographic groups and global regions. Arch Womens Ment Health 2020; 23: 331–338.
- Jiamton S, Tangjaturonrusamee C, Kulthanan K. Clinical features and aggravating factors in nummular eczema in Thais. Asian Pac J Allergy Immunol 2013; 31: 36–42.
- Brihan I, Ianoși SL, Boda D, Hălmăjan A, Zdrîncă M, Fekete LG. Implications of self-esteem in the quality of life in patients with psoriasis. Exp Ther Med 2020; 20: 202.
- Gardner DG, Pierce JL. Self-esteem and self-efficacy within the organizational context. Group Organiz Manag 1998; 23: 48–70.
- Pulfer S, Ziehfreund S, Gebhard J, Hindelang B, Biedermann T, Brockow K, et al. Health-related quality of life and influencing factors in adults with nonadvanced mastocytosis – a cross-sectional study and qualitative approach. J Allergy Clin Immunol Pract 2021; 9: 3166–3175.e2.
- Jovanović V. The validity of the Satisfaction with Life Scale in adolescents and a comparison with single-item life satisfaction measures: a preliminary study. Qual Life Res 2016; 25: 3173–3180.
- Pflug J. Folk theories of happiness: a cross-cultural comparison of conceptions of happiness in Germany and South Africa. Soc Indic Res 2009; 92: 551–563.