ORIGINAL REPORT
Therapeutic Effect of Dupilumab on Systemic and Vascular Inflammation in Adults with Severe Atopic Dermatitis: Feasibility Study Using 18F-Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography
Gi-Wook LEE1#, Keunyoung KIM2,3#, Seong-Jang KIM2, Kihyuk SHIN1, Hoonsoo KIM1,3, Hyun-Chang KO1, Moon-Bum KIM1,3 and Byungsoo KIM1,3
1Department of Dermatology, School of Medicine, Pusan National University, Busan, Korea, 2Department of Nuclear Medicine, and 3Biomedical Research Institute, Pusan National University Hospital, Busan, Korea
#These authors contributed equally to this study and should be considered as co-first authors.
Atopic dermatitis (AD) is an inflammatory skin disease associated with increased systemic and vascular inflammation. Although dupilumab has been proven to be effective against severe AD, imaging studies analysing its inflammation-reducing effect have rarely been reported. The aim of this study was to evaluate the effect of dupilumab on systemic and vascular inflammation in adult patients with severe AD, using 18F-fluorodeoxyglucose positron emission tomography-computed tomography (18F-FDG PET/CT). A total of 33 adult patients with severe AD and 25 healthy controls underwent 18F-FDG PET/CT at baseline. Patients on dupilumab treatment underwent 18F-FDG PET/CT again after achieving a 75% reduction from baseline on the Eczema Area and Severity Index (EASI-75). Patients with AD exhibited increased 18F-FDG uptake values in the liver, spleen, pancreas, and carotid artery compared with healthy controls. However, compared with baseline, there was no statistically significant difference in 18F-FDG uptake in major organs and arteries after achieving EASI-75 with dupilumab treatment. In conclusion, while dupilumab treatment resulted in a significant clinical improvement and reduced serum inflammatory markers in adult patients with severe AD, no changes in systemic and vascular inflammation were observed on 18F-FDG PET/CT imaging.
Key words: atopic dermatitis; cardiovascular disease; comorbidity; dupilumab; inflammation; PET/CT: positron emission tomography-computed tomography.
SIGNIFICANCE
Dupilumab is an effective treatment for atopic dermatitis; however, data on its systemic effects are limited. Patients with atopic dermatitis have increased vascular inflammation according to clinical severity. However, this study found that the changes in systemic and vascular inflammation after dupilumab treatment were not significant. Special attention is required to determine whether atopic dermatitis treatment not only improves skin symptoms, but also improves systemic and vascular inflammation.
Citation: Acta Derm Venereol 2023; 103: adv5320. DOI https://doi.org/10.2340/actadv.v103.5320.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Apr 6, 2023; Published: May 22, 2023
Corr: Byungsoo Kim, Department of Dermatology, School of Medicine, Pusan National University, 179 Gudeok-ro, Seo-gu 49241, Busan, Korea. E-mail: dockbs@pusan.ac.kr
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Atopic dermatitis (AD) is a common chronic inflammatory disease that is associated with numerous comorbidities, including cardiovascular and systemic diseases (1–3). Notably, analysis of the 2002–2012 Nationwide Inpatient Sample of adults in the USA found that AD was associated with increased odds (odds ratio [95% confidence interval] 1.18 [1.14–1.22]) of vascular, cardiovascular, and cerebrovascular diseases (4). Recent data have explained this association using the concept of inflammatory skin march, which occurs when a vast range of proinflammatory cytokines and chemokines from the lesional skin enter the circulatory system and cause systemic inflammation and other comorbidities (3). Although standard systemic inflammation markers, such as high-sensitivity C-reactive protein (hsCRP) and erythrocyte sedimentation rate (ESR) can reflect systemic inflammation in AD, novel assessment modalities providing regional inflammation in vivo are still required to understand the association between AD, systemic inflammation and comorbidities. 18F-fluorodeoxyglucose positron emission tomography-computed tomography (18F-FDG PET/CT) is a validated functional imaging modality for the diagnosis and management of malignancies,, which can also be used to successfully evaluate benign inflammatory diseases with high sensitivity (5, 6). Because enhanced glycolytic activity is a hallmark of activated inflammatory cells, combined PET and CT imaging provides visualization of accumulation of acute and chronic inflammatory cells resulting from primary atherosclerosis or secondary to systemic inflammatory diseases (7, 8). Thus, 18F-FDG PET/CT is used as a measurement tool to evaluate inflammatory activity, including vascular, visceral, and whole-body inflammation in vivo (6). These trials have been attempted in several previous studies in the field of psoriasis (8–10). 18F-FDG PET/CT was used to evaluate systemic and vascular inflammation in patients with psoriasis; in addition, an improvement in inflammation after treatment was also confirmed by 18F-FDG PET/CT. Although increased vascular inflammation in AD was confirmed in a recent study using PET/magnetic resonance imaging (MRI), the data are still limited (11). Furthermore, the improvement in inflammation after treatment has not yet been evaluated. The aim of the current study was therefore to assess systemic and vascular inflammation using 18F-FDG PET/CT in patients with severe AD and to evaluate whether dupilumab, an interleukin (IL)-4 receptor α-antagonist that modulates the signalling of IL-4 and IL-13 pathways, could have a positive effect on reducing inflammation in these patients.
MATERIALS AND METHODS
Study population
This study included patients aged 18–70 years who were diagnosed with AD according to the Hanifin and Rajka diagnostic criteria and had had AD for over 3 years (12). Diagnostic confirmation and severity assessment were performed by 2 experienced dermatologists. Patients were eligible if they were candidates for dupilumab therapy with Eczema Area and Severity Index (EASI) > 23, who did not respond to topical therapy or oral cyclosporine or methotrexate therapy for at least 3 months (13). The exclusion criteria included factors that could increase systemic or vascular inflammation, such as a history of malignant tumours within the past 5 years, uncontrolled diabetes mellitus and hypertension, uncontrolled dyslipidaemia, major surgery within 3 months, and active infection within the preceding 72 h. Twenty-five healthy controls without any history of systemic and/or cutaneous inflammatory disease underwent the same protocol at baseline. The study protocol was approved by the Pusan National University Hospital Institutional Review Board and all patients provided informed consent (IRB number 2001-022-087).
Study design
After initial screening, 33 patients with AD and 25 healthy controls underwent 18F-FDG PET/CT imaging and laboratory testing (complete blood count, total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), ESR, and CRP). Of the 33 patients with AD included in this study, 25 patients treated with dupilumab underwent 18F-FDG PET/CT and laboratory testing again after achieving a 75% reduction from baseline on EASI (EASI-75). The levels of inflammation in large organs, including the liver, spleen, and pancreas, and major arteries, including the carotid artery, thoracic aorta, and abdominal aorta, in patients with AD were compared with those in healthy controls. Moreover, the current study determined the relationship between the severity of inflammation with sex, obesity, and clinical severity of AD in the AD group. Finally, the study evaluated the changes in arterial and visceral inflammation after EASI-75 was achieved with dupilumab.
Imaging studies
PET/CT protocol. All patients fasted and rested for at least 6 h before undergoing 18F-FDG PET/CT imaging, since serum glucose levels needed to be below 120 mg/dL before 18F-FDG administration. A dose of 370 MBq (10 mCi) 18F-FDG was injected intravenously 60 min prior to PET/CT scanning. The patients were scanned from vertex to toe using a Gemini TF 18F-FDG PET/CT scanner (Gemini TF, Philips, Milpitas, CA, USA). The emission scan time per bed position was 3 min, and 6 bed positions were used. PET data were obtained using a high-resolution whole-body scanner with an axial field of view of 21.6 cm. The mean axial resolution varied between 2 mm full width at half maximum at the centre and 2.4 mm at 28 cm. The mean total PET/CT examination time was 20 min. Attenuation correction was performed in all patients with iterative reconstruction. PET/CT images were analysed in 3 different planes: transverse, coronal, and sagittal.
Standard uptake values measurement
The 18F-FDG PET/CT datasets were reviewed retrospectively by 2 experienced nuclear medicine specialists. 18F-FDG uptake was quantified by drawing a region of interest around the liver, spleen, pancreas, and each part of the artery on every slice of the co-registered 18F-FDG PET/CT image. To evaluate systemic inflammation, the maximum standard uptake values (SUV) of the liver, spleen, pancreas, and vascular inflammation, and those in the carotid artery, thoracic aorta, and abdominal aorta were examined by the circular region of interest (ROI) placed on the axial plane, where the most intense uptake was visualized for each organ. Using the CT images for co-registration, the areas of interest were identified on the PET images.
Statistical analysis
The AD and healthy groups were compared using 2-sided t-tests for normally distributed continuous variables and the Mann–Whitney U tests for non-parametric variables. To assess the changes within each group, a paired t-test was performed. Two-tailed probability values were reported, and statistical significance was assumed when the p - value was < 0.05. Descriptive data were presented as the mean ± standard deviation (SD) for continuous parametric variables.
RESULTS
Patients’ characteristics
The demographics and clinical characteristics of the study participants are shown in Table I. The basic demographic profiles did not differ significantly between the patients with AD and healthy controls, except for higher age in the healthy control group. Patients with AD were observed to have a mean EASI of 31.7. Among the patients with AD, 33 were treated with topical calcineurin inhibitors, 32 with topical corticosteroids, 31 with cyclosporine, and 9 with methotrexate.
Comparisons of 18F-fluorodeoxyglucose uptake between atopic dermatitis and healthy control groups
Baseline 18F-FDG PET/CT imaging revealed greater increases in the 18F-FDG uptake in the liver, spleen, pancreas, and carotid artery in the AD group than in healthy controls. There was no significant difference in the thoracic and abdominal aorta between the patients with AD and healthy controls (Fig. 1).
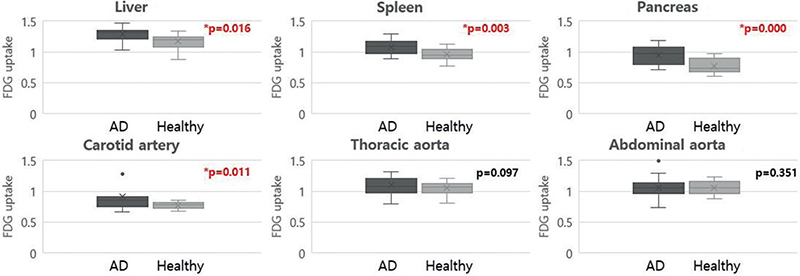
Fig. 1. Comparison of 18F-fluorodeoxyglucose (18F-FDG) uptake between atopic dermatitis (AD) (n = 33) and healthy controls (n = 25) using positron emission tomography-computed tomography (PET/CT) imaging. The y-axis represents the standard uptake value of 18F-FDG. Bars indicate the mean ± standard deviation values. *Statistically significant (p < 0.05).
Comparisons of 18F-fluorodeoxyglucose uptake among patients with atopic dermatitis
Among the patients with AD, there was no significant difference in the 18F-FDG uptake in the major organs and all parts of the aorta, according to sex and body mass index (BMI) at baseline (Fig. 2). However, a positive correlation was found between the baseline EASI score and 18F-FDG uptake in the carotid artery and abdominal aorta (p < 0.05) (Fig. 3).
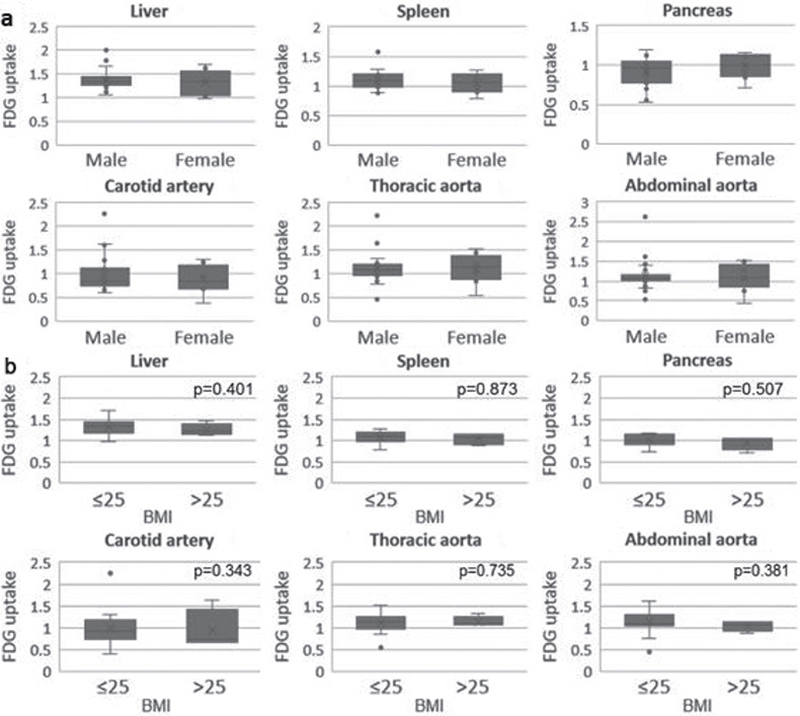
Fig. 2. Comparison of 18F-fluorodeoxyglucose (18F-FDG) uptake in positron emission tomography-computed tomography (PET/CT) imaging by (a) sex and (b) body mass index (BMI) among patients with atopic dermatitis (AD). 18F-FDG uptake level showed no significant difference in the major organs and all parts of the arteries according to sex and BMI. *Statistically significant (p < 0.05).
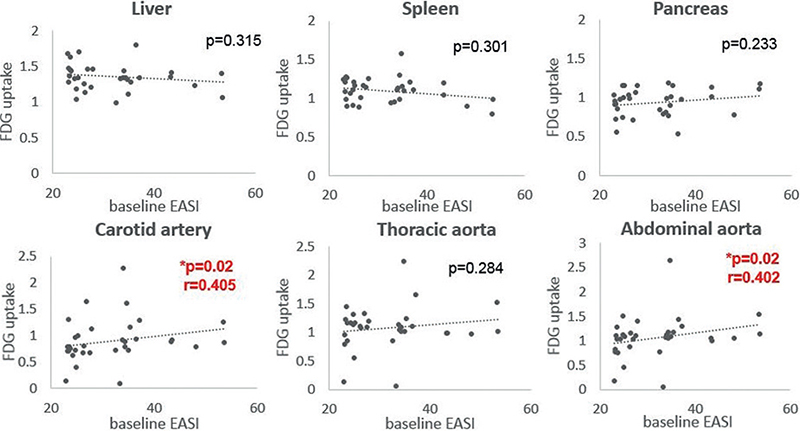
Fig. 3. Correlation between the baseline Eczema Area and Severity Index (EASI) and 18F-fluorodeoxyglucose (18F-FDG) uptake in positron emission tomography-computed tomography (PET/CT) imaging in patients with atopic dermatitis (AD). Baseline EASI score correlates with 18F-FDG uptake in the carotid artery and abdominal aorta.
Comparisons of 18F-fluorodeoxyglucose uptake before and after dupilumab treatment
After EASI-75 was achieved with dupilumab treatment for a mean period of 18.9 weeks, the mean EASI score was reduced from 31.7 to 5.75; an improvement of 81.9%. The levels of inflammatory markers (ESR and hsCRP) also decreased significantly after dupilumab treatment (Table II). However, there was no significant difference in 18F-FDG uptake in major organs and all parts of the aorta after dupilumab treatment (Fig. 4).
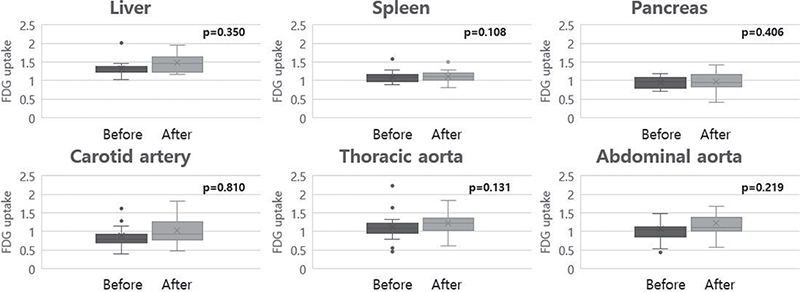
Fig. 4. Comparison of 18F-fluorodeoxyglucose (18F-FDG) uptake in positron emission tomography-computed tomography (PET/CT) imaging before and after dupilumab treatment. No significant differences in 18F-FDG uptake in major organs and all parts of the arteries after dupilumab treatment.
DISCUSSION
Through its association with various systemic comorbidities, several studies have been conducted to prove that AD is a systemic disease (14, 15). Beyond molecular analysis, the current study focused on assessing the increase in systemic and vascular inflammation in patients with AD through imaging modalities. The study also evaluated whether systemic and vascular inflammation were modifiable through treatment.
The results showed that patients with AD had increased inflammation in the liver, spleen, pancreas, and carotid artery compared with healthy controls. It is known that future cardiovascular disease (CVD) events can be predicted from increased 18F-FDG uptake of the arteries; thus, the current findings imply that adult patients with severe AD have a higher CVD risk than healthy individuals (9, 11, 16). Furthermore, the current study showed a positive correlation between baseline EASI scores and 18F-FDG uptake in the carotid artery and abdominal aorta, which suggests that severe skin inflammation may accompany vascular inflammation in AD. This result is in accordance with a previous report that showed higher vascular inflammatory activity for severe AD than for moderate AD and healthy control groups using 18F-FDG PET/MRI (11). However, there was no significant association between 18F-FDG uptake and sex and BMI. It is assumed that the relatively young age of the study participants and their demographic characteristics with less metabolic syndrome may have influenced these results.
The current study also analysed whether a significant reduction in AD severity with dupilumab treatment could modulate these values. A total of 18.9 weeks of dupilumab therapy (mean 10 injections) decreased the clinical severity of AD by a mean of 81.9%. In addition to clinical improvement, there was a significant decrease in ESR and hsCRP levels after dupilumab treatment. However, no significant changes in systemic or vascular inflammation were detected on 18F-FDG PET/CT imaging. Thus, it was assumed that the following factors could contributed to the discrepancies between the result of this study with those of our previous study on psoriasis (10). Firstly, dupilumab treatment may be less effective in reducing vascular inflammation because the Th2 pathway is still controversial in the pathogenesis of atherosclerosis; in addition, evidence on whether reducing vascular inflammation could lower the risk of CVD is lacking (17–19). Although Villani et al. (15) showed dysregulation of atherosclerosis-related genes after dupilumab treatments in patients with AD, they did not reveal an improvement in vascular inflammation after treatment with 18F-FDG PET/CT. Secondly, an overall lower uptake of 18F-FDG by major organs and vessels in patients with AD compared with in patients with psoriasis may have influenced the results. These differences can be explained by the fact that patients with AD are relatively young and have fewer comorbidities (e.g. hyperlipidaemia, obesity, diabetes, and ischaemic heart disease) (20).
Numerous studies suggest that serum markers, such as ESR, hsCRP, and leukocyte count, could be independent predictors of future cardiovascular events in both healthy individuals and in patients with several CVDs (21, 22). In the current study, baseline serum hsCRP levels in the AD group were significantly higher than those in the healthy control group. In addition, this level decreased after treatment with dupilumab. These changes in inflammatory serum markers suggest that dupilumab may be effective in preventing cardiovascular complications in patients with severe adult AD.
However, PET/CT did not show the same results as serum inflammatory markers for dupilumab treatment, which may be evaluated as showing limitations in PET/CT sensitivity. The current study has some limitations. First, the study did not compare patients with AD with age- and sex-matched healthy controls, which might have influenced the differences in 18F-FDG uptake in major organs between patients with AD and healthy controls. Secondly, previous use of cyclosporine or methotrexate might have influenced the results of 18F-FDG uptake. The difference according to the duration of drug use was not reflected in the study. Thirdly, the small sample size may have decreased the statistical power of the current results. Fourthly, assessment of atopic comorbidities, such as asthma or allergic rhinitis, was not considered. As these diseases often coexist with AD and are associated with Th2-driven inflammation, this may have influenced the outcome. Finally, since the current study did not report on systemic or cardiovascular events in patients in the long-term follow-up, it is not clear whether the increase in inflammation detected through imaging modalities has a meaningful clinical effect. In conclusion, special attention is required to determine whether AD treatment not only improves skin symptoms, but also improves systemic and vascular inflammation.
ACKNOWLEDGEMENTS
This study was supported by the Biomedical Research Institute Grant (202000030001), Pusan National University Hospital, Busan, Korea.
The study protocol was approved by the Pusan National University Hospital Institutional Review Board and all patients provided informed consent (IRB number 2001-022-087).
REFERENCES
- Silverberg JI. Comorbidities and the impact of atopic dermatitis. Ann Allergy Asthma Immunol 2019; 123: 144–151.
- Brunner PM, Silverberg JI, Guttman-Yassky E, Paller AS, Kabashima K, Amagai M, et al., Councilors of the International Eczema Council. increasing comorbidities suggest that atopic dermatitis is a systemic disorder. J Invest Dermatol 2017; 137: 18–25.
- Furue M, Kadono T. “Inflammatory skin march” in atopic dermatitis and psoriasis. Inflamm Res 2017; 66: 833–842.
- Kwa MC, Silverberg JI. Association between inflammatory skin disease, cardiovascular and cerebrovascular comorbidities in US adults: analysis of Nationwide Inpatient Sample data. Am J Clin Dermatol 2017; 18: 813–823.
- Vaidyanathan S, Patel CN, Scarsbrook AF, Chowdhury FU. FDG PET/CT in infection and inflammation – current and emerging clinical applications. Clin Radiol 2015; 70: 787–800.
- Kim SJ, Park MY, Pak K, Han J, Kim GW, Kim HS, et al. Improvement of depressive symptoms in patients with moderate-to-severe psoriasis treated with ustekinumab: an open label trial validated using beck depression inventory, Hamilton depression rating scale measures and 18fluorodeoxyglucose (FDG) positron emission tomography (PET). J Dermatolog Treat 2018; 29: 761–768.
- Lawal I, Sathekge M. F-18 FDG PET/CT imaging of cardiac and vascular inflammation and infection. Br Med Bull 2016; 120: 55–74.
- Youn SW, Kang SY, Kim SA, Park GY, Lee WW. Subclinical systemic and vascular inflammation detected by (18) F-fluorodeoxyglucose positron emission tomography/computed tomography in patients with mild psoriasis. J Dermatol 2015; 42: 559–566.
- Mehta NN, Yu Y, Saboury B, Foroughi N, Krishnamoorthy P, Raper A, et al. Systemic and vascular inflammation in patients with moderate to severe psoriasis as measured by [18F]-fluorodeoxyglucose positron emission tomography-computed tomography (FDG-PET/CT): a pilot study. Arch Dermatol 2011; 147: 1031–1039.
- Kim BS, Lee WK, Pak K, Han J, Kim GW, Kim HS, et al. Ustekinumab treatment is associated with decreased systemic and vascular inflammation in patients with moderate-to-severe psoriasis: feasibility study using 18F-fluorodeoxyglucose PET/CT. J Am Acad Dermatol 2019; 80: 1322–1331.
- Ungar B, Pavel AB, Robson PM, Kaufman A, Pruzan A, Brunner P, et al. A preliminary 18F-FDG-PET/MRI study shows increased vascular inflammation in moderate-to-severe atopic dermatitis. J Allergy Clin Immunol Pract 2020; 8: 3500–3506.
- Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol 1980; Suppl 92: 44–47.
- Lee H, Kim BR, Kim KH, Lee DH, Na JI. One-year effectiveness and safety of dupilumab treatment for moderate-to-severe atopic dermatitis in Korean patients: a real-world retrospective analysis. Allergy Asthma Immunol Res 2022; 14: 117–122.
- Guttman-Yassky E, Bissonnette R, Ungar B, Suárez-Fariñas M, Ardeleanu M, Esaki H, et al. Dupilumab progressively improves systemic and cutaneous abnormalities in patients with atopic dermatitis. J Allergy Clin Immunol 2019; 143: 155–172.
- Villani AP, Pavel AB, Wu J, Fernandes M, Maari C, Saint-Cyr Proulx E, et al. Vascular inflammation in moderate-to-severe atopic dermatitis is associated with enhanced Th2 response. Allergy 2021; 76: 3107–3121.
- Rominger A, Saam T, Wolpers S, Cyran CC, Schmidt M, Foerster S, et al. 18F-FDG PET/CT identifies patients at risk for future vascular events in an otherwise asymptomatic cohort with neoplastic disease. J Nucl Med 2009; 50: 1611–1620.
- Elnabawi YA, Dey AK, Goyal A, Groenendyk JW, Chung JH, Belur AD, et al. Coronary artery plaque characteristics and treatment with biologic therapy in severe psoriasis: results from a prospective observational study. Cardiovasc Res 2019; 115: 721–728.
- Kim JD, Lee SH, Seo EH, Woo SY, Kim SH, Chung SM, et al. Role of Th1 and Th17 cells in the development and complexity of coronary artery disease: comparison analysis by the methods of flow cytometry and SYNTAX score. Coron Artery Dis 2015; 26: 604–611.
- Taleb S. Inflammation in atherosclerosis. Arch Cardiovasc Dis 2016; 109: 708–715.
- Radtke MA, Schäfer I, Glaeske G, Jacobi A, Augustin M. Prevalence and comorbidities in adults with psoriasis compared to atopic eczema. J Eur Acad Dermatol Venereol 2017; 31: 151–157.
- Madjid M, Awan I, Willerson JT, Casscells SW. Leukocyte count and coronary heart disease: implications for risk assessment. J Am Coll Cardiol 2004; 44: 1945–1956.
- Vekaria AS, Brunner PM, Aleisa AI, Bonomo L, Lebwohl MG, Israel A, et al. Moderate-to-severe atopic dermatitis patients show increases in serum C-reactive protein levels, correlating with skin disease activity. F1000Res 2017; 6: 1712.