ORIGINAL ARTICLE
Severe Scabies: A French Multi-centre Study Involving 95 Patients with Crusted and Profuse Disease and Review of the Literature
Charbel SKAYEM1#, Majda ASKOUR1,2#, Charlotte GARY1,3#, François HEMERY4, Emmanuel MAHÉ5, Frédéric CAUX6, Nicolas DUPIN7, Patricia SENET8, Alix GREDER BELAN9, Brigitte HILLION10, Cécile MENI11, Philippe SAIAG12, Guillaume BELLAUD13, Alexandre BLEIBTREU14, Sylvie LARIVEN14, Diane BOLLENS15, Vincent DESCAMPS16, Jean-Michel MOLINA17, Olivier BOUCHAUD18, Daniel VITTECOQ19, Giao DO-PHAM20, Françoise FOULET3,21, Françoise BOTTEREL3,21, Olivier CHOSIDOW1,3§ and Charlotte BERNIGAUD1,3§
Dermatology Departments: 1Assistance Publique des Hôpitaux de Paris (AP-HP), Hôpital Henri-Mondor, Créteil, France, 2Centre Hospitalier Universitaire IBN SINA, Rabat, Morocco, 5Centre Hospitalier Victor Dupouy, Argenteuil, 6APHP, Hôpital Avicenne, Bobigny, 7APHP, Hôpital Cochin, Pavillon Tarnier, Paris, 8APHP, Hôpital Tenon, Sorbonne Université, Paris, 10Centre Hospitalier Marne la Vallée, Jossigny, 11APHP, Hôpital Necker-Enfants malades, Paris, 12APHP, Hôpital Ambroise Paré, Boulogne-Billancourt and 16APHP, Hôpital Bichat Claude Bernard, 3Research Group Dynamic, EA7380, Faculté de Santé de Créteil, Ecole Nationale Vétérinaire d’Alfort, USC ANSES, Université Paris-Est Créteil, Créteil, 4Service d’Information Médicale, DSIGHM, APHP, Hôpital Henri-Mondor, Créteil, 9Service de Médecine Interne et Unité de Maladies Infectieuses et Tropicales, Centre Hospitalier de Versailles, Hôpital Mignot, Le Chesnay, Infectious Diseases Departments: 13APHP, Hôpital Tenon, Hôpitaux Universitaires Paris-Est, 14APHP, Hôpital Bichat Claude Bernard, 15APHP, Hôpital Saint-Antoine, 17APHP, Hôpital Saint-Louis, Paris, 18APHP, Hôpital Avicenne, Bobigny and 19APHP, CHU Bicêtre, Le Kremlin Bicêtre, 20Service de Médecine Interne, Centre Hospitalier Intercommunal de Créteil, Créteil, and 21Parasitology and Mycology, Department of Microbiology, UPEC, APHP, Hôpital Henri-Mondor, Créteil, France
#These authors contributed equally to the manuscript and should be considered as first authors. §These authors contributed equally to the manuscript.
The aim of this multi-centre French retrospective study was to identify severe, i.e. crusted and profuse, scabies patients. Records were retrieved from 22 Dermatology or Infectious Diseases departments in the Ile-de-France from January 2009 to January 2015 to characterize epidemiology, demography, diagnosis, contributing factors, treatment features, and outcomes in severe scabies. A total of 95 inpatients (57 crusted and 38 profuse) were included. A higher number of cases was observed among elderly patients (>75 years), mostly living in institutions. Thirteen patients (13.6%) reported a history of previously treated scabies. Sixty-three patients (66.3%) had been seen by a previous practitioner for the current episode (up to 8 previous visits). Initial misdiagnosis (e.g. eczema, prurigo, drug-related eruptions, psoriasis) was documented in 41 patients (43.1%). Fifty-eight patients (61%) had already received 1 or more previous treatments for their current episode. Forty percent received corticosteroids or acitretin for an initial diagnosis of eczema or psoriasis. Median time from the onset of symptoms to the diagnosis of severe scabies was 3 months (range 0.3–22). Itch was present in all patients at diagnosis. Most patients (n=84, 88.4%) had comorbidities. Diagnostic and therapeutic approaches varied. Complications occurred in 11.5% of cases. To date, there is no consensus for diagnosis and treatment, and future standardization of is required for optimal management.
Key words: scabies; Sarcoptes scabiei; parasitic; crusted scabies; pruritus; ivermectin; permethrin.
SIGNIFICANCE
Only a few case series regarding severe scabies have been published, with none from Europe. This multicentric retrospective study on 95 patients in the Ile-de-France characterized the epidemiology, demography, diagnosis, contributing factors, treatments, and outcomes of patients with scabies. Most patients were elderly, vulnerable, had comorbidities, and lived in institutions. Cases were commonly misdiagnosed. Unexpectedly, all patients reported pruritus. Time to diagnosis was long, and complications were not rare, with 3.1% mortality. These results highlight the importance of educating general physicians, specialists, and the general public on these entities and developing standardized treatments to control spreading of this highly contagious disease.
Citation: Acta Derm Venereol 2023; 103: adv00878. DOI: https://doi.org/10.2340/actadv.v103.5351.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Feb 1, 2023; Published: Mar 2, 2023
Corr: Olivier Chosidow, Department of Dermatology, Hôpital Henri-Mondor, 51, av du Maréchal-de-Lattre-de-Tassigny, FR-94010 Créteil Cedex, France. E-mail: olivier.chosidow@aphp.fr
Competing interests and funding: CB acts as unpaid scientific advisor for Medicines Development for Global Health. OC received fees for an advisory board meeting, he is the PI of phase 2 moxidectin RCT supported by Medicines Development for Global Health. No other competing interests were declared.
INTRODUCTION
Scabies is a contagious parasitic skin disease caused by Sarcoptes scabiei var homini (1–3). It is now regarded as being of sufficient public-health importance because of more frequent outbreaks and a recognition of the longer term health impacts and downstream effects of scabies infestations. Scabies was added to the World Health Organization (WHO) list of neglected tropical diseases in 2017 (4). Severe forms of scabies include crusted and profuse scabies (2). Although there is no prevalence data on severe scabies, there are rare, yet very easily transmissible, forms, with the number of infesting mites reaching several millions (5, 6). Limited case series exist in the literature, and optimal diagnosis and treatment are still missing (7–11). There are no recent data on the characteristics of crusted scabies in Europe. A multicentric retrospective cohort study was conducted on 95 patients with severe scabies in the Ile-de-France (constituting Paris and its area, a north-east region of France).
METHODS
Study setting and period
All Dermatology and Infectious Diseases departments in Ile-de-France, were solicited. To identify cases of severe scabies, the study searched all inpatients recorded over a 6 years-period (1 January 2009 to 1 January 2015) with the diagnosis of “scabies’’ in the national hospital discharge database (Programme de Médicalisation des Systèmes d’Information; PMSI) using the International Classification of Diseases, 10th Revision (“B86” code). Then, 3 authors (MA, CG, CB) retrospectively reviewed medical records, and only crusted and profuse scabies were included.
Study population, inclusion and exclusion diagnosis criteria
Crusted or profuse scabies were considered as “severe scabies”. Scabies diagnosis was performed at 2 different levels: (i) confirmed diagnosis; or (ii) suspected clinical diagnosis. A confirmed diagnosis was a compatible clinical presentation (see below) associated with at least 1 positive investigation (skin scraping, dermoscopic, or histological). Cases without paraclinical confirmation were discussed for inclusion with study investigators expert in the disease (MA, CG, CB) after reviewing the records and the images. Common scabies cases, doubtful cases, or cases where the records were uninterpretable or insufficient were excluded.
For the clinical presentation, the patient’s body was divided into 9 parts. Scabies was considered profuse when skin lesions extended to the whole body or there was a diffuse eruption involving the trunk, the back, the face, or the scalp. If ≥ 1 hyperkeratotic lesion(s) were reported, crusted scabies was diagnosed. A positive paraclinical examination was a skin scraping demonstrating Sarcoptes scabiei mites, eggs or faecal pellets on microscopy, a dermoscopic examination showing the delta sign, or a skin biopsy with mites, eggs or faecal pellets visible in the stratum corneum.
Data collection
Collected data included demographic information, such as sex, age, residence, comorbidities, clinical information including presence/absence of pruritus, morphology and location of skin lesions, and month of admission. Diagnostic characteristics included time to diagnosis and supporting diagnostic investigations; treatment and outcomes were also recorded.
Statistical analyses
Continuous variables were expressed as medians and categorical variables as numbers (percentage) and extreme values. Statistical analyses were performed using SAS v9.0 (SAS Institute Inc., Cary, NC, USA) software (Version 9.0).
Ethics statement
This is a retrospective non-interventional study. According to the Public Health French Law (art L 1121-1-1, art L 1121-1-2), approval from Institutional Review Board was not required. All participants were informed about the use of their medical data in the study, according to local French regulations.
RESULTS
A total of 95 patients were included during the study period (Fig. 1). Severe scabies was more frequent during winter periods (Fig. S1), with 2 spikes noted in October and December.

Fig. 1. Study flow chart. ID: infectious diseases.
Demographic characteristics and clinical findings
Of the 95 included patients, 57 (60%) had crusted and 38 (40%) had profuse scabies. characteristics of the patients are shown in Table I. The distribution by age group showed a higher number of patients over 75 years old (n = 30, 31.5%) (Fig. 2). Fourteen (14.7%) of them lived in institutions, and 16 (16.8%) were homeless.

Fig. 2. Age repartition of the study population.
Thirteen patients (13.6%) reported a history of previously treated scabies (6 confirmed cases (6.3%), and 7 suspicious cases (7.3%)). A case of scabies in close contacts was identified in 35 patients (36.8%), with a confirmed diagnosis in 10 patients (10.5%) and a suspicious diagnosis in 25 (26.3%) (Table I). Sixty-three patients (66.3%) had been seen by a general practitioner or a specialist for the current episode, at least once, with an extreme of up to 8 previous visits. Initial misdiagnosis was documented in 41 patients (43.1%) (Table I). An eczema flare-up was the most frequently reported initial diagnosis in 19 patients. Other misdiagnoses included prurigo, drug-related eruptions, psoriasis, and pediculosis. Fifty-eight patients (61%) had already received 1 or more treatments before their hospitalization. 40% received corticosteroids, of which 28% were topical, and 1 patient received acitretin for an initial diagnosis of psoriasis. The median time from onset of symptoms to the diagnosis of severe scabies was 3 months, (3 weeks to 22 months). Paraclinical confirmation was performed in 81% of cases, with skin scraping being the most commonly performed test (Table I).
Pruritus was present in all patients at diagnosis and was diffuse in 95% of cases. Burrows were detected in 40% of patients with crusted scabies and in 43% of patients with profuse scabies. Papules, nodules, and vesicles were found in 76%, 10%, and 40% of patients with crusted scabies, respectively. They were found in 84%, 22%, and 57% of patients with profuse scabies, respectively. The distribution of hyperkeratotic lesions in patients with crusted scabies is shown in Fig. 3. Hands were the most commonly affected part (66%). Half of all patients (49.5%) had hypereosinophilia > 500/mm3 (Table I).
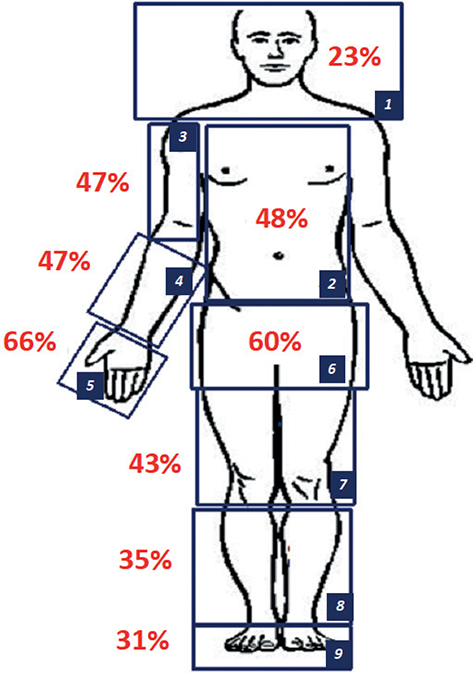
Fig. 3. Distribution of hyperkeratosis in patients with crusted scabies. 1: head: neck: and shoulders; 2: trunk; 3: axilla: arms: and elbows; 4: forearms and wrists; 5: hands; 6: pubis: genitals: and buttocks; 7: thigh and knees; 8: legs and ankles; 9: feet.
Most patients (n = 84, 88.4%) had comorbidities. Sixty patients (63.1%) received immunosuppressive drugs, such as anticancer chemotherapies, azathioprine, mycophenolate mofetil, methotrexate, or rituximab. Corticosteroids were the most common (n = 53, 55.7%), especially topical corticosteroids (n = 40, 42.1%). Other comorbidities were also commonly associated with severe scabies: 30 patients (31.5%) had neurological disorders, 23 (24.2%) had a history of chronic alcoholism, 13 (13.6%) had diabetes, 12 (12.6%) had an underlying skin disease, 11 (11.5%) had psychiatric conditions, and 7 (7.4%) had chronic liver disease.
Therapeutic management, disease course and mortality
A total of 87 patients (91.6%) received a combination of systemic treatment (oral ivermectin 200 µg/kg/dose) and topical treatment (Table I). The others were treated with oral ivermectin only (n = 6, 6.3%) or a topical treatment (n = 2, 2.1%). Benzyl benzoate 10% combined with monosulfiram was the most prescribed topical treatment (n = 63, 66.3%), followed by 10% benzyl benzoate alone (n = 17, 17.9%). The median number of topical applications was 3 [range 1–19], with 1 application per day. In 45 cases (47.4%), ivermectin was prescribed orally in 2 doses of 200 µg/kg/dose; 31 patients (32.6%) received 3 doses, and 4 patients (4.2%) received 4 doses. The interval between ivermectin doses also varied from 7 days in 45 patients (47.4%), to 15 days in 19 patients (20%). Tolerance of topical treatments was variable, with 22 patients (23.2%) requiring topical corticosteroids applications for eczematization or irritation of their skin. Treatment of contact cases and environmental decontamination were reported in 58.9%.
Median hospitalization duration was 12 days [1–46]. Eleven patients (11.5%) had a complication related to their scabies episode. The most common was secondary infection, mostly bacterial skin infection in 8 patients (8.4%), involving Staphylococcus aureus in most cases. Other infections involved Streptococcus pyogenes (e.g. Erysipelas, sepsis) and Escherichia coli (e.g. sepsis). Four patients with confirmed crusted scabies developed bullous diseases, 3 of which were bullous pemphigoid, and 2 patients developed vasculitis. Three patients with crusted scabies died during their hospitalization (mortality rate of 3.1%) (Table I). The cause of death of the first was acute renal failure and hyperkalaemia; the second had severe hypoglycaemia with loss of consciousness; the third was bedridden and died from E.coli and Staphylococcus aureus sepsis.
DISCUSSION
This multi-centric regional retrospective study with 95 patients is among the largest case series of severe scabies. Only 5 series are found in the literature (5–9). The current study confirms the long delay in the diagnosis of severe scabies, lasting up to several months, especially in crusted scabies (extreme of 22 months). De Sainte Marie et al. (12) described a mean delay in diagnosis of 4 months (extreme of 13 months) in a series of 31 patients with scabies (mostly common scabies). In the series of crusted scabies by Yélamos et al. (9), the delay was also long, with a median of 7 months and an extreme of up to 16 months. The delayed diagnosis may be explained by a lack of specific clinical signs for severe scabies and insufficient knowledge of the clinical presentation by physicians (9–11). The 2020 International Alliance for the Control of Scabies has facilitated the standardization of common scabies diagnosis (13). However, no diagnostic criteria for severe scabies have been established.
In the current study, severe scabies was more frequent during winter periods. Studies from Scotland and Israel demonstrated higher rates during cooler seasons, possibly related to increased human personal contact and overcrowding, as well as increased mite fertility and survival in cold weather (14).
Half of the patients in the current study were subject to initial misdiagnosis. A majority of them were initially diagnosed with eczema. The other most common differential diagnoses include psoriasis, and adverse drug reaction (15–26). The onset of pruritus and/or skin lesions in the patient’s relatives or failure to respond to the first treatment led to the diagnosis in most cases. Misdiagnosis is associated with 2 serious consequences. First, patients with an undiagnosed condition may infest several contacts, as severe scabies are highly contagious. For example, 16 million mites were quantified using in vivo confocal microscopy on a crusted scabies skin and thousands of live mites were found in scales collected in bed sheets of patients with severe scabies (3, 27). In institutions and residential homes, this leads to prolonged and difficult-to-control outbreaks, requiring considerable resources to be managed (28–32). Thus, accurate diagnosis allows disease control. Moreover, misdiagnosis can lead to incorrect prescriptions of treatments (mainly topical corticosteroids), initially improving pruritus, but finally aggravating the infestation, which might cause profuse or crusted scabies and life-threatening complications. A late diagnosis or an inappropriate treatment increases the risk of secondary infection with Staphylococcus aureus or Streptococcus pyogenes. Specific scabies mite proteins act as inhibitors on all 3 complement pathways, inhibiting host innate immunity (33–38), fostering the growth of bacteria. Previous case reports and series highlighted the misuse of topical corticosteroids (39–48), but no epidemiological studies were able to prove causality. In the current study, more than half of the patients received immunosuppressive drugs and more than 40% had applied topical corticosteroids. Topical corticosteroids alter the skin immune system by reducing or even suppressing local cell-mediated immune responses, resulting in a failure of the host to control the proliferation of mites in the skin. In a porcine model, systemic corticosteroids (oral dexamethasone 0.2 mg/kg/day) increased intensity and duration of infestation with Sarcoptes scabiei (49). Pigs treated with corticosteroids develop severe scabies especially crusted scabies, unlike non-treated pigs (50).
Most patients in the series by Roberts et al. (7), Davis et al. (8), and Hasan et al. (11) (97%, 100%, 95% of patients respectively) belonged to Australian indigenous communities. These populations seem to develop severe scabies without known triggering factors. A genetic predisposition that is currently unknown can be the cause. As in the current series, patients in the study by Davis et al. (n = 49) were mainly males (59%) (8). Yélamos et al. (9) reported a median age of 73 years among their 4 patients, whereas the 3 Australian studies reported younger patients with a median age of 44 years (7, 8, 10). In the current study, the median age was 63 years with a majority of elderly patients over 75 years old. The majority of patients in our retrospective study cohort had comorbidities (89%), which is consistent with the other series (7–11).
Contrary to what has been reported in the literature suggesting crusted scabies is not itchy (24, 51–55), all patients in the current study complained of itch, at time of diagnosis. Complications included secondary bacterial infection, electrolyte imbalance, and erythroderma (24). Patients with severe scabies are also at higher risk of developing vasculitis (56–63) and bullous pemphigoid (64), which were seen in 2% and 4% of our patients, respectively. It is assumed that the mites’ antigens could share similarities with those of the dermo-epidermal junction leading to antibody production against proteins of the dermo-epidermal junction (65). The complications of severe scabies make the mortality of this entity non-negligible. In the current series, 3 patients died (3.1%). Roberts et al. and Hasan et al. reported a higher mortality of 14% (4) and 16%, respectively (9). While scabies is often considered as a benign infection, it can become a serious condition when not well-controlled (66–68).
Treatment of severe scabies is long, often requiring a prolonged hospital stay. Different treatment protocols were used in the current study, testifying a lack of standardization: topical treatments were associated or not with oral ivermectin, and different numbers of applications and dosing intervals were used. The majority of patients were treated with oral ivermectin (200 µg/kg/dose) and 10% benzoyl benzoate + 2% monosulfiram. On the one hand, topical treatments differed because of lack of consensus on the treatment, and, on the other hand, because availabilities of topical treatments have changed during the study period. Ten percent benzyl benzoate with 2% sulfiram was out of stock from November 2012, then replaced by an imported product (10% benzyl benzoate alone) from Germany in February 2013. A French commercial product then became available in October 2015 (also with 10% benzyl benzoate only). Esdepallethrin with piperonyl butoxide was used as an alternative, which was withdrawn from the French market in July 2017. Permethrin was not available in France until after July 2015. Treatment usually consists of a combination of topical acaricides and systemic ivermectin at repeated doses (69–71). Only a few therapeutic studies for treatment of crusted scabies including more than 5 patients exist in the literature (summarized in Table II) (6, 8, 11, 72, 73). A Cochrane review for the treatment of scabies does not mention severe scabies (74). The recent development of a porcine model holds a significant potential for developing scabies treatment (75–77), in addition to the development of randomized controlled clinical trials, such as the one granted in France by the French Ministry of Health, comparing the efficacy of ivermectin given orally at a dose of 400 µg/kg vs the conventional treatment dose of 200 µg/kg, 3 times 7 days apart (on D0, D7, and D14), with application in both arms of daily emollient therapy and topical 5% permethrin on D0 and D7 (GALECRUSTED, NCT02841215) (78).
| Author(s) | Year | Treatment studied | Results | Patients n |
| Hasan et al. (11) | 2020 | Ivermectin 200 µg/kg/dose 3–7 doses (median 5, ranges 0–13) |
71% efficacy | 92 |
| Davis (8) | 2013 | Ivermectin 200 µg/kg/dose 2–10 doses 47 patients: + benzyl benzoate + tea tree oil 2 patients: + permethrin 5% |
100% efficacy | 49 |
| Nofal (72) | 2009 | Ivermectin 200 µg/kg/dose Day 10 ± day 14 ± day 28 |
30% efficacy at day 14 90% at day 28 |
8 |
| Roberts et al. (7) | 2005 | Ivermectin 200 µg/kg/dose Days 0, 1, 7, 8, 14, ± 21 ± 28 + keratolytic treatment |
100% efficacy at day 30 | 78 |
| Dia et al. (73) | 1999 | Ivermectin 200 µg/kg/dose 2 doses |
100% efficacy | 11 |
Although the current study is among the largest retrospective study on severe scabies, it has some limitations. Besides its retrospective nature, it includes only hospitalized patients, who are usually older patients with comorbidities. Moreover, not all cases were confirmed by a paraclinical examination, although all clinically-confirmed cases were reviewed by experts in scabies. Management was based on French practice, noting the unavailability of topical treatments such as permethrin during the studied period. The current study did not evaluate the efficacy of the treatments, because this was not the objective of the study. Ongoing clinical trials for optimal treatments in crusted scabies will give a better highlight on the preferred therapeutic modalities.
Conclusion
Severe cases of scabies hospitalized in the French Parisian area were mostly seen in elderly, immunosuppressed people with comorbidities who live in residential institutions. Clinical presentation might lead to misdiagnosis in many cases. Contrary to what has been reported in the literature about crusted scabies causing no or less itch, all patients in the current study reported itch, at time of diagnosis. Severe forms of scabies are often misdiagnosed with eczema, and previous treatments with topical corticosteroids may increase complications. To date, there is no consensus on the clinical management of these cases. Standardization of the diagnosis and treatment is essential, and educating general physicians and geriatricians about these entities is indispensable for optimizing management.
ACKNOWLEDGEMENTS
The authors would like to gratefully acknowledge David Smith, PhD, QIMR Berghofer MRI, Brisbane, Australia for his help for the statistical analysis.
MA, CG, and CB were supported by a Mobility, a Master 2, and a PhD scholarship from the French Society of Dermatology, respectively.
REFERENCES
- Thomas C, Coates SJ, Engelman D, Chosidow O, Chang AY. Ectoparasites: scabies. J Am Acad Dermatol 2020; 82: 533–548.
- Bernigaud C, Monsel G, Delaunay P, Chosidow O. Arthropods. In: C. Griffiths, J. Barker, T. Bleiker, R. Chalmers, D. Creamer, editors. Rook’s textbook of dermatology. Wiley, 2022, 10th edn.
- Niode NJ, Adji A, Gazpers S, Kandou RT, Pandaleke H, Trisnowati DM, et al. Crusted scabies, a neglected tropical disease: case series and literature review. Infect Dis Rep 2022; 14: 479–491.
- World Health Organization (WHO). Scabies. Geneva: World Health Organization, 2015. [Accessed 31/01/2022] Available from https://www.who.int/news-room/fact-sheets/detail/scabies.
- Chosidow O. Clinical practices. Scabies. N Engl J Med 2006; 354: 1718–1727.
- Cinotti E, Perrot JL, Labeille B, Vercherin P, Chol C, Besson E, Cambazard F. Reflectance confocal microscopy for quantification of Sarcoptes scabiei in Norwegian scabies. J Eur Acad Dermatol Venereol 2013; 27: e176–8.
- Roberts LJ, Huffam SE, Walton SF, Currie BJ. Crusted scabies: clinical and immunological findings in seventy-eight patients and a review of the literature. J Infect 2005; 50: 375–381.
- Davis JS, McGloughlin S, Tong SY, Walton SF, Currie BJ. A novel clinical grading scale to guide the management of crusted scabies. PLoS Negl Trop Dis 2013; 7: e2387.
- Yélamos O, Mir-Bonafé JF, López-Ferrer A, Garcia-Muret MP, Alegre M, Puig L. Crusted (Norwegian) scabies: an under-recognized infestation characterized by an atypical presentation and delayed diagnosis. J Eur Acad Dermatol Venereol 2016; 30: 483–485.
- O’Donnell BF, O’Loughlin S, Powell FC. Management of crusted scabies. Int J Dermatol 1990; 29: 258–266.
- Hasan T, Krause VL, James C, Currie BJ. Crusted scabies; a 2-year prospective study from the Northern Territory of Australia. PLoS Negl Trop Dis 2020; 14: e0008994.
- De Sainte Marie B, Mallet S, Gaudy-Marqueste C, Baumstarck K, Bentaleb N, Loundou A, et al. Gales en échec de traitement: étude observationnelle. Ann Dermatol Venereol 2016; 143: 9–15.
- Hay RJ, Steer AC, Engelman D, Walton S. Scabies in the developing world – its prevalence, complications, and management. Clin Microbiol Infect 2012; 18: 313–323.
- Engelman D, Yoshizumi J, Hay RJ, Osti M, Micali G, Norton S, et al. The 2020 International Alliance for the Control of Scabies Consensus Criteria for the Diagnosis of Scabies. Br J Dermatol 2020; 183: 808–820.
- Sandre M, Ralevski F, Rau N. An elderly long-term care resident with crusted scabies. Can J Infect Dis Med Microbiol 2015; 26: 39–40.
- Gach J, Heagerty A. Crusted scabies looking like psoriasis. Lancet 2000; 356: 650.
- Fonseca V, Price HN, Jeffries M, Alder SL, Hansen RC. Crusted scabies misdiagnosed as erythrodermic psoriasis in a 3-year-old girl with Down syndrome. Pediatr Dermatol 2014; 31: 753–754.
- Murugaiyan R, Sengottian KLB, Karthikeyan K. Crusted scabies presenting as palmoplantar psoriasis in Down’s syndrome. Indian Dermatol Online J 2015; 6: 140–141.
- Kutlu NS, Turan E, Erdemir A, Gürel MS, Bozkurt E. Eleven years of itching: a case report of crusted scabies. Cutis 2014; 94: 86–88.
- Hong MY, Lee CC, Chuang MC, Chao SC, Tsai MC, Chi CH. Factors related to missed diagnosis of incidental scabies infestations in patients admitted through the emergency department to inpatient services. Acad Emerg Med 2010; 17: 958–964.
- Askour M, Kissou A, Lyagoubi M, Hassam B. Gale hyperkératosique mimant un eczéma : difficultés diagnostiques devant des lésions croûteuses chroniques. Presse Med 2016; 45: 1193–1194.
- Almond DS. Lesson of the week Norwegian scabies misdiagnosed as an adverse drug reaction. BMJ 2000; 320: 35–36.
- Costa JB, Rocha de Sousa VL, da Trindade Neto PB, Paulo Filho Tde A, Cabral VC, Pinheiro PM. Norwegian scabies mimicking rupioid psoriasis. An Bras Dermatol 2012; 87: 910–913.
- Das A, Bar C, Patra A. Norwegian scabies: rare cause of erythroderma. Indian Dermatol Online J 2015; 6: 52–54.
- Goyal NN, Wong GA. Psoriasis or crusted scabies. Clin Exp Dermatol 2008; 33: 211–212.
- Burch JM, Krol A, Weston WL. Sarcoptes scabiei infestation misdiagnosed and treated as Langerhans cell histiocytosis. Pediatr Dermatol 2004; 21: 58–62.
- Walton SF, McBroom J, Mathews JD, Kemp DJ, Currie BJ. Crusted scabies: a molecular analysis of Sarcoptes scabiei variety hominis populations from patients with repeated infestations. Clin Infect Dis 1999; 29: 1226–1230.
- Hewitt KA, Nalabanda A, Cassell JA. Scabies outbreaks in residential care homes: factors associated with late recognition, burden and impact. A mixed methods study in England. Epidemiol Infect 2015; 143: 1542–1551.
- Cassell JA, Middleton J, Nalabanda A, Lanza S, Head MG, Bostock J, et al. Scabies outbreaks in ten care homes for elderly people: a prospective study of clinical features, epidemiology, and treatment outcomes. Lancet Infect Dis 2018; 18: 894–902.
- De Beer G, Miller MA, Tremblay L, Monette J. An outbreak of scabies in a long-term care facility: the role of misdiagnosis and the costs associated with Control. Infect Control Hosp Epidemiol 2006; 27: 517–518.
- Makigami K, Ohtaki N, Ishii N, Tamashiro T, Yoshida S, Yasumura S. Risk factors for recurrence of scabies: a retrospective study of scabies patients in a long-term care hospital. J Dermatol 2011; 38: 874–879.
- Murakonda P, Yazdanbaksh K, Dharmarajan TS. Scabies in the nursing home, misdiagnosis means costs, and embarrassment: story of a centenarian smitten by scabies! J Am Med Dir Assoc 2014; 15: 74–75.
- Bergström FC, Reynolds S, Johnstone M, Pike RN, Buckle AM, Kemp DJ, et al. Scabies mite inactivated serine protease paralogs inhibit the human complement system. J Immunol 2009; 182: 7809–7817.
- Mika A, Reynolds SL, Mohlin FC, Willis C, Swe PM, Pickering DA, et al. Novel scabies mite serpins inhibit the three pathways of the human complement system. PLoS One 2012; 7: e40489.
- Mika A, Reynolds SL, Pickering D, McMillan D, Sriprakash KS, Kemp DJ, Fischer K. Complement inhibitors from scabies mites promote streptococcal growth – a novel mechanism in infected epidermis? PLoS Negl Trop Dis 2012; 6: e1563.
- Swe PM, Fischer K. A scabies mite serpin interferes with complement-mediated neutrophil functions and promotes staphylococcal growth. PLoS Negl Trop Dis 2014; 8: e2928. Erratum in: PLoS Negl Trop Dis. 2014; 8: e3415.
- Swe PM, Christian LD, Lu HC, Sriprakash KS, Fischer K. Complement inhibition by Sarcoptes scabiei protects Streptococcus pyogenes – an in vitro study to unravel the molecular mechanisms behind the poorly understood predilection of S. pyogenes to infect mite-induced skin lesions. PLoS Negl Trop Dis 2017; 11: e0005437.
- Swe PM, Reynolds SL, Fischer K. Parasitic scabies mites and associated bacteria joining forces against host complement defence. Parasite Immunol 2014; 36: 585–593.
- Binić I, Janković A, Jovanović D, Ljubenović M. Crusted (Norwegian) scabies following systemic and topical corticosteroid therapy. J Korean Med Sci 2010; 25: 188–191.
- Marlière V, Roul S, Labrèze C, Taïeb A. Crusted (Norwegian) scabies induced by use of topical corticosteroids and treated successfully with ivermectin. J Pediatr 1999; 135: 122–124.
- Baccouche K, Sellam J, Guegan S, Aractingi S, Berenbaum F. Crusted Norwegian scabies, an opportunistic infection, with tocilizumab in rheumatoid arthritis. Joint Bone Spine 2011; 78: 402–404.
- Melgar E, Liegeon AL, Truchetet F. Développement d’une gale mortelle sous dermocorticoïdes. Presse Med 2017; 46: 335–337.
- Martínez Braga G, Di Martino Ortiz B, Rodríguez Masi M, Bolla De Lezcano L. [Erythrodermic crusted scabies induced by corticosteroids treated with ivermectin. A case report]. Rev Espanola Geriatr Gerontol 2011; 46: 174–175 (in Spanish).
- Jaramillo-Ayerbe F, Berrío-Muñoz J. Ivermectin for crusted Norwegian scabies induced by use of topical steroids. Arch Dermatol 1998; 134: 143–145.
- Walton SF, Beroukas D, Roberts-Thomson P, Currie BJ. New insights into disease pathogenesis in crusted (Norwegian) scabies: the skin immune response in crusted scabies. Br J Dermatol 2008; 158: 1247–1255.
- Millard LG. Norwegian scabies developing during treatment with fluorinated steroid therapy. Acta Derm Venereol 1977; 57: 86–88.
- Lipitz R, Tur E, Brenner S, Krakowski A. Norwegian scabies following topical corticosteroid therapy. Isr J Med Sci 1981; 17: 1165–1168.
- Clayton R, Farrow S. Norwegian scabies following topical steroid therapy. Postgrad Med J 1975; 51: 657–659.
- Mounsey K, Ho MF, Kelly A, Willis C, Pasay C, Kemp DJ, et al. A tractable experimental model for study of human and animal scabies. PLoS Negl Trop Dis 2010; 4: e756.
- Mounsey KE, Murray HC, Bielefeldt-Ohmann H, Pasay C, Holt DC, Currie BJ, et al. Prospective study in a porcine model of Sarcoptes scabiei indicates the association of Th2 and Th17 pathways with the clinical severity of scabies. PLoS Negl Trop Dis 2015; 9: e0003498.
- Johnston G, Sladden M. Scabies: diagnosis and treatment. BMJ 2005; 331: 619–622.
- Banerji A. Canadian Paediatric Society, First Nations, Inuit and Métis Health Committee. Scabies. Paediatr Child Health 2015; 20: 395–402.
- Stamm LV, Strowd LC. Ignoring the “Itch”: the global health problem of scabies. Am J Trop Med Hyg 2017; 97: 1647–1649.
- Walton SF, Currie BJ. Problems in diagnosing scabies, a global disease in human and animal populations. Clin Microbiol Rev 2007; 20: 268–279.
- Jannic A, Bernigaud C, Brenaut E, Chosidow O. Scabies itch. Dermatol Clin 2018; 36: 301–308.
- Nishihara K, Shiraishi K, Sayama K. Leukocytoclastic vasculitis associated with crusted scabies. Eur J Dermatol 2018; 28: 242–243.
- Hay RJ. Norwegian scabies in a patient with a cutaneous vasculitis. Guys Hosp Rep 1974; 123: 177–185.
- Fremont G, Benamor S, Gaulier A, Sigal Grinberg M, Petit A. Eruption prurigineuse et purpurique. Ann Dermatol Venereol 2003; 130: 61–62.
- Valks R, Buezo GF, Daudén E. Scabies and leukocytoclastic vasculitis in an HIV-seropositive man. Int J Dermatol 1996; 35: 605–606.
- Jarrett P, Snow J. Scabies presenting as a necrotizing vasculitis in the presence of lupus anticoagulant. Br J Dermatol 1998; 139: 701–703.
- Menné T, Christophersen J, Gram N, Bjerrehus T. Scabietic leucocytoclastic vasculitis with focal glomerulonephritis. Acta Derm Venereol 1984; 64: 445–447.
- Clevy C, Brajon D, Combes E, Benzaquen M, Dales JP, Koeppel MC, Berbis P. Vasculite scabieuse: 2 cas. Ann Dermatol Venereol 2017; 144: 349–355.
- Estève E, Maitre F, Legac E. Purpura vasculaire au cours d’une gale sévère. Ann Dermatol Venereol 2001; 128: 911–914.
- Chung S-D, Lin H-C, Wang K-H. Increased risk of pemphigoid following scabies: a population-based matched-cohort study. J Eur Acad Dermatol Venereol 2014; 28: 558–564.
- Ostlere LS, Harris D, Rustin MH. Scabies associated with a bullous pemphigoid-like eruption. Br J Dermatol 1993; 128: 217–219.
- Currie B, Huffain S, O’Brien D, Walton S. Ivermectin for scabies. Lancet 1997; 350: 1551.
- Carapetis JR, Steer AC, Mulholland EK, Weber M. The global burden of group A streptococcal diseases. Lancet Infect Dis 2005; 5: 685–694.
- Lynar S, Currie BJ, Baird R. Scabies and mortality. Lancet Infect Dis 2017; 17: 1234.
- Scott GR, Chosidow O, IUSTI/WHO. European guideline for the management of scabies, 2010. Int J STD AIDS 2011; 22: 301–303.
- Salavastru CM, Chosidow O, Boffa MJ, Janier M, Tiplica GS. European guideline for the management of scabies. J Eur Acad Dermatol Venereol 2017; 31: 1248–1253.
- Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. N Engl J Med 2010; 362: 717–725.
- Nofal A. Variable response of crusted scabies to oral ivermectin: report on eight Egyptian patients. J Eur Acad Dermatol Venereol 2009; 23: 793–797.
- Dia D, Dieng MT, Ndiaye AM, Ndiaye B, Develoux M. La gale croûteuse (norvégienne) à Dakar (Sénégal). Dakar Med 1999; 44: 243–245.
- Rosumeck S, Nast A, Dressler C. Ivermectin and permethrin for treating scabies. Cochrane Database Syst Rev 2018; 4: CD012994.
- Mounsey KE, Bernigaud C, Chosidow O, McCarthy JS. Prospects for moxidectin as a new oral treatment for human scabies. PLoS Negl Trop Dis.2016; 10: e0004389.
- Bernigaud C, Fang F, Fischer K, Lespine A, Aho LS, Dreau D, et al. Preclinical study of single-dose moxidectin, a new oral treatment for scabies: efficacy, safety, and pharmacokinetics compared to two-dose ivermectin in a porcine model. PLoS Negl Trop Dis 2016; 10: e0005030.
- Bernigaud C, Fang F, Fischer K, Lespine A, Aho LS, Mullins AJ, et al J. Efficacy and pharmacokinetics evaluation of a single oral dose of afoxolaner against sarcoptes scabiei in the porcine scabies model for human infestation. Antimicrob Agents Chemother 2018; 62: e02334-17.
- Efficacy study between two different dosages of an antiparasitic in patients with crusted scabies – ClinicalTrials.gov. [first cited 2016 July 22; last update 2020 November 23]. Available from: https://clinicaltrials.gov/ct2/show/NCT02841215.