SHORT COMMUNICATION
Systemic Sarcoidosis with Cutaneous Tattoo Involvement Following COVID-19 Vaccination
Carolin Constanze ALBERS, Dieter METZE, Kerstin STEINBRINK and Markus BÖHM
Department of Dermatology, University of Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: carolin.albers@ukmuenster.de
Citation: Acta Derm Venereol 2023; 103: adv6244. DOI https://doi.org/10.2340/actadv.v103.6244.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Feb 21, 2023; Published: Mar 28, 2023
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
We would like to present a special case in the context of the COVID-19 pandemic. A 41-year-old man was admitted to our Department of Dermatology at the University of Münster, Germany with changes to a 20-year-old black-coloured tattoo located on his right deltoid muscle. The changes had developed over a period of 5 months. He had noted these changes approximately 10 days after the second vaccination with the mRNA Comirnaty© vaccine (BNT162b2 Pfizer-BioNTech COVID-19 vaccine; Pfizer (New York, USA) - BioNTech (Mainz, Germany)). The second dose of the vaccine was administered to his left arm, the opposite side to his tattoo. Mild swelling of the injection area and fatigue were also reported by the patient. However, these symptoms disappeared within 2–3 days. He did not recall any previous changes to his tattoo. His history further disclosed allergic asthma and allergic rhinoconjunctivitis. The patient reported that topical corticosteroids and tacrolimus had no effect on the skin lesions.
Dermatological examination revealed a sharply defined swelling of the entire black-coloured tattoo (Fig. 1). No other skin changes were detected. A skin biopsy from the swollen tattooed skin showed sarcoidal granulomatous dermatitis with exogenous pigment deposits consistent with granulomatous tattoo reaction or cutaneous manifestation of sarcoidosis (Fig. 2). Additional laboratory tests revealed elevated angiotensin converting enzyme (ACE 56 U/L; normal range 8–52 U/L) and soluble interleukin-2 receptor (sIL-2R 1,069 U/mL; normal range 158–623 U/mL). All other laboratory parameters were within normal ranges. A computed tomography scan of the chest further disclosed mediastinal lymphadenopathy, in accordance with the diagnosis of systemic sarcoidosis, stage I. Intralesional triamcinolone injections and/or peroral hydroxychloroquine was/were recommended. Under medication with hydroxychloroquine, 200 mg twice a day, the swelling decreased, but the patient lost his appetite and lost weight; hence he reduced the dose and then stopped taking the medication.

Fig. 1. Swelling of the black-coloured tattoo.
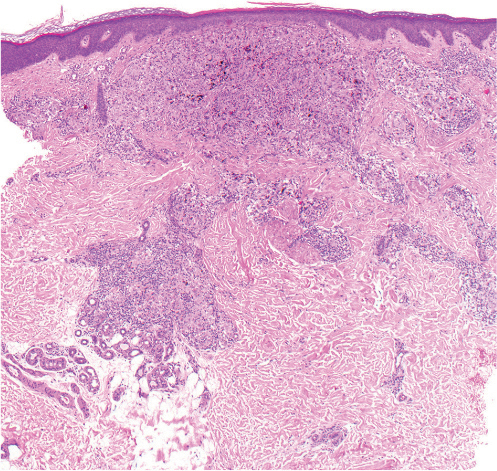
Fig. 2. Sarcoidal granulomatous dermatitis with exogenous pigment deposits (haematoxylin and eosin (H&E), original magnification 50×).
DISCUSSION
Tattoo-induced skin and systemic sarcoidosis have been reported previously (1). Thus, vaccinations against influenza or with Bacillus Calmette-Guérin have been described as triggers for sarcoidosis (2, 3). With regard to COVID-19 disease, both COVID-19 infections and vaccinations against COVID-19 have been associated with onset of a variety of inflammatory and autoimmune-mediated diseases, including systemic sarcoidosis (4). In 2021, an acute, ulcerative, sarcoidal tattoo reaction following COVID-19 vaccination was reported and described as a “Sweet-like phenomenon”. However, in the latter case, laboratory markers, such as ACE and lung imaging, were inconspicuous, excluding the diagnosis of sarcoidosis (5). In contrast to this case, the patient in the current report showed clear signs of sarcoidosis, such as mediastinal lymphadenopathy and elevated levels of ACE. To the best of our knowledge, systemic sarcoidosis with a granulomatous tattoo reaction following COVID-19 vaccination has not been described previously. Possible pathophysiological mechanisms include pro-inflammatory mechanisms, such as the release of interferon gamma produced by T-cells after COVID-19 vaccination (6). Interferon gamma also activates macrophages, which are key players in tattoo reactions (7) and in sarcoidosis (8). Cytokine storms associated with COVID-19 (9) and COVID-19 vaccination (10) may favour the development of granulomas at cutaneous sites of high antigenic content, such as tattoos. The current case highlights that changes in tattoos can be the first clinical sign of sarcoidosis and also reports that this complication developed following COVID-19 vaccination.
REFERENCES
- Kluger N. Sarcoidosis on tattoos: a review of the literature from 1939 to 2011. Sarcoidosis Vasc Diffuse Lung Dis 2013; 30: 86–102.
- Psaltis NM, Gardner RG, Denton WJ. Systemic sarcoidosis and red dye granulomatous tattoo inflammation after influenza vaccination: a case report and review of literature. Ocul Immunol Inflamm 2014; 22: 314–321.
- Osborne GE, Mallon E, Mayou SC. Juvenile sarcoidosis after BCG vaccination. J Am Acad Dermatol 2003; 48: S99–S102.
- Gracia-Ramos AE, Martin-Nares E, Hernández-Molina G. New onset of autoimmune diseases following COVID-19 diagnosis. Cells 2021; 10: 3592.
- Manci R, Jennings T, Mclarney RM, Heymann WR, Sommer LL. An acute, ulcerative, sarcoidal tattoo reaction following SARS-CoV-2 mRNA-1273 vaccination. Dermatol Online J 2021; 27: 1–3.
- Sahin U, Muik A, Derhovanessian E, Vogler I, Kranz LM, Vormehr M, et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020; 586: 594–599.
- Lo Schiavo A, Ruocco E, Gambardella A, O’Leary RE, Gee S. Granulomatous dysimmune reactions (sarcoidosis, granuloma annulare, and others) on differently injured skin areas. Clin Dermatol 2014; 32: 646–653.
- Drent M, Crouser ED, Grunewald J. Challenges of sarcoidosis and its management. N Engl J Med 2021; 385: 1018–1032.
- Hu B, Huang S, Yin L. The cytokine storm and COVID-19. J Med Virol 2021; 93: 250–256.
- Murata K, Nakao N, Ishiuchi N, Fukui T, Katsuya N, Fukumoto W, et al. Four cases of cytokine storm after COVID-19 vaccination: case report. Front Immunol 2022; 13: 967226.