ORIGINAL REPORT
Paediatric Mycosis Fungoides: Clinical Variants, Treatment Modalities and Response to Therapy
Orna MIRMOVICH MORVAY1, Michal RAMON1, Ziad KHAMAYSI1,2 and Emily AVITAN-HERSH1,2
1Department of Dermatology, Rambam Health Care Campus and 2Bruce Rappaport Faculty of Medicine, Technion Institute of Technology, Haifa, Israel
Mycosis fungoides is a rare cutaneous lymphoma in the paediatric population. The aim of this study was to examine the epidemiological, clinical, and histological characteristics, as well as the treatment modalities and response to therapy of paediatric patients with mycosis fungoides. This retrospective cohort study reviewed the records of 37 paediatric patients treated at Rambam Medical Center, Israel, between 2013 and 2021. Extracted data included epidemiology, clinical presentation, histological reports, infiltrate clonality status, treatment modalities and response to therapy. The mean follow-up period was 60 months. All patients were diagnosed with stage IA or IB disease. Folliculotropic mycosis fungoides was the most prevalent variant (49%). Most patients were treated with phototherapy (90%), with a response rate of 85%, and a complete response rate of 55% after the first course. There were no significant differences in response to phototherapy between the folliculotropic or other variants (p = 0.072). Similarly, delayed diagnosis, atopic diathesis, clonality, phototherapy type or number of treatments, were not associated with response to therapy, while protracted phototherapy was associated with prolonged remission. In conclusion, mycosis fungoides in the paediatric population is an indolent disease with a favourable prognosis and potentially prolonged response to phototherapy.
Key words: mycosis fungoides; folliculotropic; paediatric; cutaneous lymphoma; phototherapy.
SIGNIFICANCE
Mycosis fungoides is the most cutaneous T cell lymphoma in general population. In children, mycosis fungoides is an indolent disease with overall good prognosis. This study analysed data for a cohort of 37 paediatric patients for a long follow-up period. The results show that the folliculotropic variant is more common than previously thought. In addition, the results showed that initial treatment with narrowband ultraviolet B phototherapy can be considered for paediatric patients with folliculotropic mycosis fungoides, especially if the lymphocytic infiltrate is superficial.
Citation: Acta Derm Venereol 2023; 103: adv6557. DOI https://doi.org/10.2340/actadv.v103.6557.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Mar 28, 2023; Published: Jul 14, 2023
Corr: Orna Mirmovich Morvay, Department of Dermatology, Rambam Health Care Campus, Haifa, Israel. E-mail: orna.mir@gmail.com
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Mycosis fungoides (MF) is the most common cutaneous T-cell lymphoma in the general population (1). However, it is a rare disease in the paediatric population, with estimated prevalence of 5% of all cases (2, 3). In the general population, the classical variant, which is characterized clinically by patches and plaques covered with scales in sun-hidden areas, is most abundant. However, the clinical presentation in children is versatile and entails a high prevalence of atypical variants (4, 5). Hypopigmented MF, which is clinically characterized by hypopigmented patches and plaques with variable scaling and no skin atrophy, has been reported as the most frequent type in children (6). Histologically it cannot be differentiated from the classical variant, but it is characterized by an increased frequency of cytotoxic T cells that are positive for CD8 in immunohistochemical staining.
Another common variant in the paediatric population is the folliculotropic variant characterized clinically by erythematous or skin-coloured coalescing papules and plaques with follicular accentuation and sparseness of hair. In histology, tropism of malignant T lymphocytes toward the follicular epithelium is seen (4). The different variants not only have a versatile clinical and histological presentation, but they also differ in therapeutic approach, with psoralen-UVA (PUVA) phototherapy as the preferred treatment for deep folliculotropic MF (7).
Histological diagnosis of MF is based on the presence of a T-cell infiltrate with cytomorphological atypia and epidermotropism, without significant spongiosis. Intraepidermal clustering of atypical lymphocytes known as Pautrier microabscesses is almost pathognomonic, but not always present (8, 9). Additional histological findings are present in the atypical variants of MF; for example, in the folliculotropic variant, malignant T-cell infiltrate is seen in the follicular epithelium and the peri-adnexal structures. In immunohistochemical staining, which is ancillary in establishing the diagnosis, decreased or full loss of expression of T-cell antigens, such CD7, is common (10). T-cell receptor gene rearrangement (TCR-GR) helps determine the clonality status of the infiltrate and may aid in establishing the diagnosis in equivocal cases.
The low prevalence of MF in the paediatric population, its versatile clinical presentation, and an understandably cautious approach to obtaining biopsies in children, are responsible for delayed diagnosis (11). Nevertheless, most children are diagnosed with an early disease, stage IA/IB, most probably due to its indolent nature.
For limited disease, topical corticosteroids are the mainstay of therapy. However, for more extensive disease, phototherapy is the treatment of choice (6). Narrowband ultraviolet B (NB-UVB) phototherapy is the most commonly used therapy in children, due to its high safety and efficacy profile in early disease (13). PUVA is most frequently used when NB-UVB phototherapy fails or for treatment of the folliculotropic variant (14, 15). Other skin-directed therapies suitable for early-stage MF include topical corticosteroids, retinoids, carmustine and nitrogen mustard (16–18). On rare occasions, local irradiation or surgical excision are required (19). In a progressive or recalcitrant disease in the adult population, systemic retinoids, methotrexate, or interferon alpha can be used. However, these are less common therapeutic choices when treating children (20–22).
Due to the low prevalence of MF in children, most available data are retrospective, with few case series involving children, some of them also originated from Israel (4, 7, 23). The aim of this study was to examine the epidemiological, clinical, and histological characteristics, treatment modalities and response to therapy in children diagnosed with MF and treated in a tertiary medical centre in Israel.
MATERIALS AND METHODS
This retrospective cohort study included paediatric patients, aged 0–18 years, who were treated for MF in the Dermatology Department at Rambam Health Care Campus, Israel between 2013 and 2021. Epidemiological and clinical presentation, histological diagnosis and classification, clonality status of the infiltrate, treatment modalities, and response to therapy were reviewed. The diagnosis of MF was based on clinical presentation combined with histological findings and was supported by immunohistochemical staining, based on the guidelines of the International Society of Cutaneous Lymphoma and the European Organization for Research and Treatment of Cancer (24). TCR-GR was used as an ancillary test. Study approval was obtained from the Rambam Health Care Campus Institutional Review Board (Helsinki) committee (approval number: 0308-21-RMB).
Statistical analysis
Descriptive statistical methods were used to present patients, disease, and treatment characteristics. The interaction between categorical variables was examined by χ2 test. The interaction between latency to diagnosis and categorical variables was examined using the Kruskal-Wallis rank-sum test. Correlation between treatment duration or number of treatments and response was quantified by Pearson correlation. Statistical significance was set a priori at p < 0.05. The data were analysed using R, version 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Clinical characteristics
A total of 37 paediatric patients with MF were examined in our clinic during the study period. Of these, 28 were male and 9 were female; a ratio of 3.1:1. Age at disease onset ranged from 5 months to 18 years. The mean age at diagnosis was 10.44 years, with a mean delay in MF diagnosis of almost 2 years (1.96, range 0.33–5 years). The mean follow-up period was 60 months, ranging from 5 months to a maximum of 132 months (11 years). Of the 37 patients, 32 (86.5%) had no comorbidities. Five patients had a past medical history of: recurrent infections (2/5), VACTERL syndrome (1/5), primary dyskinesia (1/5), epilepsy (1/5), and attention-deficit hyperactivity disorder (ADHD) (1/5). Thirty percent (11/37) of the patients had a personal or family history of atopic diathesis, defined by the presence of asthma, atopic dermatitis, or allergic rhinitis.
All patients presented with an early disease, stage IA/IB, with no systemic involvement; 54% (20/37) of the patients presented with stage IA disease and the remaining patients (46%) with stage IB. Systemic involvement was evaluated by complete physical examination, ancillary laboratory studies that included complete blood count, chemistry and lactate dehydrogenase, and imaging studies (chest X-ray and sonography of lymph nodes). Upon presentation, there was a high rate of lower limb involvement (57%, 21/37), followed by involvement of the upper limbs and trunk, 54% (20/37) each. Folliculotropic MF was the most common variant, presenting in 49% (18/37) of the patients, followed by hypopigmented and classical variants, each in 22% of the patients (8/37). An additional 3 patients had mixed presentation, combining the classical and folliculotropic features. There were no significant differences in atopic diathesis between the different clinicopathological variants (p = 1).
Clonality of the infiltrate
To aid in establishing diagnosis, a TCR-GR study was conducted in 89% (33/37) of the patients (all with ample DNA material). Overall positive monoclonality was present in 65% of the patients. Monoclonality in TCR-GR was observed in only 44% of the patients with folliculotropic MF, whereas the other variants of MF (classical and hypopigmented) were monoclonal in 84% of the patients (p = 0.017).
We examined whether a longer delay in diagnosis was correlated with monoclonality, but no correlation was found (Fig. 1). Patients with monoclonal infiltrate had a mean diagnosis delay of 1.85 years; those with polyclonal infiltrate in TCR-GR studies had a delay of 1.88 years (p = 0.41). Moreover, there was no correlation between atopic diathesis and clonality status of the infiltrate (p = 1).
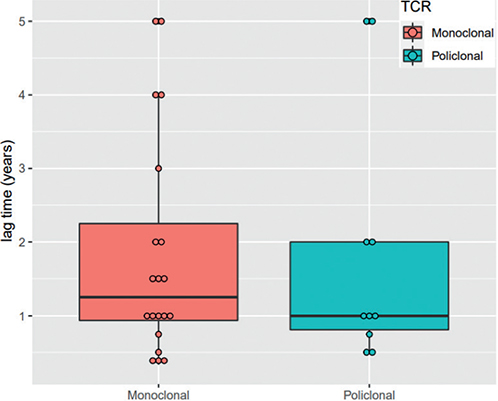
Fig. 1. Correlation between clonality status of the infiltrate and delay in diagnosis. TCR: T-cell receptor.
Treatment
To study the responses to different treatments in the paediatric population, they were classified into 3 categories: complete response, defined as documentation of complete skin clearance, a skin biopsy showing no evidence of disease, or both, when applicable; incomplete response; and disease progression.
Three patients had limited disease and were treated only topically, with complete remission. Of these, 1 patient was treated with nitrogen mustard and the others, topical corticosteroids. Most patients (92%, 34/37) received phototherapy treatment during their follow-up, during which no patient progressed to advanced disease or systemic involvement.
NB-UVB was the first line of treatment in 73% (25/34) of those treated with phototherapy. Among the NB-UVB-treated group, with a mean of 50 treatments, 56% (14/25) reached full remission that lasted 31 months (range 3–96 months); 36% of the patients had a partial response, and 2 patients had no response at all. A single patient was treated with a combination of UVA + UVB, reaching full remission after 47 treatments and no recurrence. Eight patients received PUVA therapy as the first line of treatment; 5/8 (63%) reached full remission, which lasted 35 months on mean (range 7–69 months); the remaining patients had no response.
Following the first course of phototherapy, overall response rate (complete or partial) was 85% (29/34). However, only 32% (11/34) of the patients remained in complete remission. Those who recurred were treated with additional courses of phototherapy or skin-directed therapy. A second course of phototherapy was given to 35% (12/34) of the patients, with at least some response (partial or complete) in all cases; 9% (3/34) required a third course and 1 patient needed a fourth course. Other adjuvant modalities after phototherapy failure included topical corticosteroids or nitrogen mustard, oral retinoids, or interferon alpha injection.
In addition, the current study looked for prognostic factors for early recurrence and non-response. Delay in diagnosis and clonality status did not correlate with response (p = 0.57 and p = 0.41, respectively). Moreover, a higher number of treatments did not correlate with better response (p = 0.57). However, when examining the correlation between total duration of phototherapy and maintenance of at least a partial response, patients who had a protracted course of phototherapy (mean of 8.46 months and median 7 months) maintained a lengthy response after cessation of therapy (p = 0.044) (Fig. 2).
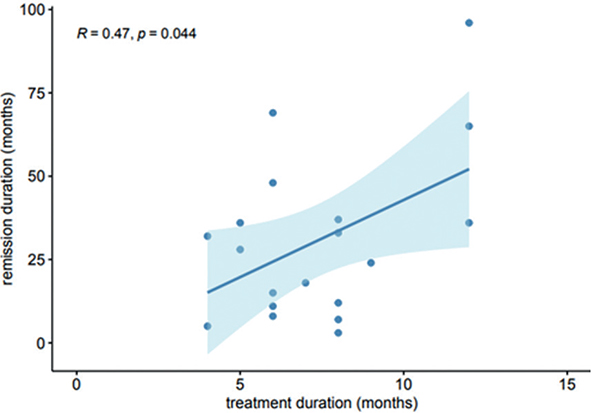
Fig. 2. Correlation between treatment duration and remission duration.
The study also examined the correlation between clinical variant and response to phototherapy. Interestingly, all non-responders were diagnosed with folliculotropic MF (5/34), whereas all patients who presented with another variant (classical or hypopigmented MF) had some response (14/14). Nevertheless, there was no significant difference in the response to therapy between the different variants (p = 0.072), possibly due to the small size of the sample group (Fig. 3).
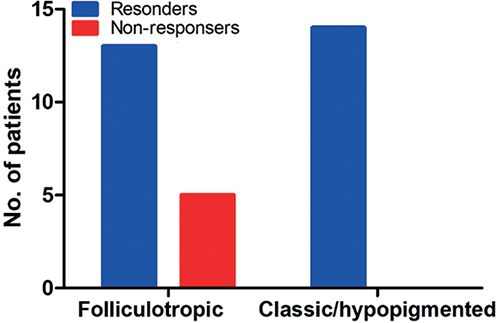
Fig. 3. Mycosis fungoides (MF) variant and response to therapy.
Because of the high prevalence of folliculotropic MF in the current study, response to therapy was further analysed in this group. The type of phototherapy (PUVA or NB-UVB) resulted in similar response rates (p = 0.24). Focusing on the 5 non-responders with folliculotropic MF, 3 patients were treated with PUVA phototherapy, and 2 with NB-UVB. The response to NB-UVB phototherapy in the folliculotropic MF patients was unexpected, and therefore we reviewed their pathological reports, to evaluate whether this could be explained by a more superficial infiltrate. In the current study, 18 patients had a diagnosis of folliculotropic MF. Biopsy was available in 89% (16/18) of the cases. In 9 of these patients (56%), superficial infiltrate involving only the infundibulum of the hair follicle was seen.
DISCUSSION
This retrospective cohort study reviewed epidemiological, clinical and histological characteristics, as well as response to therapy, in paediatric patients with MF over an 8-year period in a tertiary medical centre in Israel.
MF is a cutaneous lymphoma with a versatile clinical presentation and multiple histological variants. In the adult population, the classical variant is most often reported, whereas in children, according to the limited available data, hypopigmented MF is most common (6, 25). These findings are in line with the work of Hodak et al. (4), who showed increased prevalence of the folliculotropic variant, second only to the hypopigmented type. However, in contrast to the accepted paradigm, in the current study folliculotropic MF was predominant. The increased prevalence of folliculotropic MF could be partially explained by the high index of suspicion in a tertiary referral centre. Moreover, other studies conducted in Israel, including most recently published by Reiter et al. (4, 7, 23), showed increased prevalence of the folliculotropic variant, possibly suggesting unique predisposing ethnic, immunological or genetic factors for this variant.
The diagnosis of MF relies primarily on clinical and histological findings, with TCR-GR as an ancillary test in establishing a diagnosis. In early lesions, a reactive inflammatory dermal infiltrate dominates, whereas the malignant infiltration is relatively sparse, thus resulting in a negative clonality in TCR-GR studies. In later stages, the malignant infiltrate is denser and more extensive, thus resulting in an increasingly positive clonality (27). In the adult population, depending on the case series, monoclonality in TCR-GR is seen in 50–90% of cases. In the paediatric population, the rates are lower, ranging from 21% to 71% (1, 3, 26). In the current study, overall positive monoclonal T-cell infiltrate was seen in 65% (24/35) of the patients. Considering the clonality status among the different histological variants, only 44% of patients with folliculotropic MF had a monoclonal infiltrate, whereas the remaining variants had a positive monoclonality rate of 84% (p = 0.017). Many factors can influence the clonality status of the infiltrate, including technical aspects, such as the selected primers and the PCR products (27), as well as lesion stage. All of the current patients presented with early-stage MF. Similarly, in the available histological reports of the patients with folliculotropic MF, most of the cases (56%) had a malignant infiltrate confined to the infundibular portion of the hair follicle, indicating an early and superficial disease (6). Furthermore, in the current cohort of paediatric patients with MF, TCR-GR was performed during the initial evaluation, with no re-evaluation during follow-up visits. Thus, negative clonality in TCR-GR may reflect an early disease or its indolent nature.
Persistent antigenic stimulation is one of the pathological mechanisms suggested in the development of lymphoma in general, as exemplified by exposure to Borrelia burgdorferi and the development of cutaneous B-cell lymphoma (28). Thirty percent (11/37) of the current patients had a significant personal or family history of atopic diathesis. Atopic diathesis in general, and atopic dermatitis in particular, is characterized by chronic inflammation with a type II immunological response (29). We suspect that persistent antigenic stimulation in atopic dermatitis may facilitate a shift from polyclonal to monoclonal infiltrate. MF can mimic atopic dermatitis, and there are several reported cases of patients with a long-standing diagnosis of atopic dermatitis, who, after long-term follow-up, developed MF (30). However, in this study, there was no correlation between atopic diathesis and clonality status in the infiltrate (p = 1).
In the current study cohort, there was a mean lag period of almost 2 years (mean 1.96 years) from disease onset to diagnosis. In the literature, a much longer period (approximately 5 years) has been reported (26). Hodak et al.’s (4) report from Israel, with relatively similar medical facilities, also showed a mean diagnosis delay of 4.2 years (4). The shorter delay found here might be explained by increased clinician awareness and a high index of suspicion of the dermatopathologist at our institute. To our knowledge, correlations between temporal delay in diagnosis and clonality status have never been examined. In the current study, there was no correlation between diagnosis delay and clonality status of the infiltrate (p = 0.41) or response to therapy (p = 0.57). This might indicate that MF is an indolent cutaneous lymphoma, with limited progression and a favourable overall prognosis. On the other hand, the relatively short diagnosis delay, compared with other reports in the literature, may explain this lack of correlation. Therefore, additional studies are required.
There are no randomized controlled studies to determine the optimal treatment protocols for paediatric MF. Therapy is partially extrapolated from the adult practice, and previous case series showing good response to phototherapy in the paediatric population (7, 13, 14). A predominance of the folliculotropic variant was shown, which ideally requires a phototherapy modality that enables deeper penetration to the dermal infiltrate. Bath PUVA (immersion in diluted psoralen before exposure to UVA) based phototherapy was less available in our institution, along with the desire to avoid long-term side-effects of systemic PUVA. Thus, most of our patients (55%) were initially treated with NB-UVB phototherapy. According to the available histological reports of folliculotropic MF, in 56% (9/16) of the cases, the malignant infiltrate was superficial and confined to the follicular infundibulum, potentially explaining the success of this therapy. However, due to the small sample in the current study, we could not statistically analyse the correlation between depth of the infiltrate and response to therapy. In addition, there was no correlation between response to therapy and the different histological variants. With regard to the folliculotropic variant, there was no difference in response to the different types of phototherapies (p = 0.24). In other words, NB-UVB phototherapy was as efficient as PUVA phototherapy in inducing remission in children with early folliculotropic MF. This is in contrast to the work of Reiter et al., which mostly used PUVA phototherapy for folliculotropic MF. However, no consideration was given regarding the depth of the infiltrate, in choosing treatment modality, or allocation of bath vs systemic PUVA therapy (7)
In adult patients, maintenance phototherapy following remission is a common practice, especially during treatment with PUVA (31). In the current study, only 4 patients received long-term maintenance therapy. The study examined the hypothesis that a protracted course of phototherapy can yield better results in maintaining remission after the treatment is terminated. Accordingly, patients who were treated with a lengthy phototherapy course (a mean of 8.46 months) enjoyed a longer remission period (p = 0.044). It is possible that a gradual decrease of phototherapy treatment frequency, spread over a protracted period, can prevent disease rebound and the need for additional interventions. This in line with the work of Reiter et al., which suggested that phototherapy can modify the course of cutaneous disease (7). No similar correlation was found between the absolute number of treatments and length of remission (p = 0.57).
Study limitations
The limitations of this study are its retrospective nature and the small number of patients. However, one must bear in mind the rarity of the disease, the versatility of the study population, the follow-up period of up to 11 years, and the different treatment modalities. Additional prospective studies are required to characterize the disease in paediatric patients and to help determine the optimal treatment.
Conclusion
This is a retrospective cohort study of 37 paediatric patients with MF who were treated between 2013 and 2021, with a maximum follow-up period of 11 years, at a tertiary medical centre in Israel. The findings reinforce the hypothesis that MF is an indolent disease with an overall good prognosis in children. Thus, balance is required in choosing an appropriate therapy that will achieve remission with minimal long-term side-effects.
REFERENCES
- Ceppi F, Pope E, Ngan B, Abla O. Primary cutaneous lymphomas in children and adolescents. Pediatr Blood Cancer 2016; 63: 1886–1894.
- Assaf C, Gellrich S, Steinhoff M, Nashan D, Weisse F, Dippel E, et al. Cutaneous lymphomas in Germany: an analysis of the Central Cutaneous Lymphoma Registry of the German Society of Dermatology (DDG). J Dtsch Dermatol Ges 2007; 5: 662–668.
- Jung JM, Lim DJ, Won CH, Chang SE, Lee MW, Lee WJ. Mycosis fungoides in children and adolescents: a systematic review. JAMA Dermatol 2021; 157: 431–438.
- Hodak E, Amitay-Laish I, Feinmesser M, Davidovici B, David M, Zvulunov A, et al. Juvenile mycosis fungoides: cutaneous T-cell lymphoma with frequent follicular involvement. J Am Acad Dermatol 2014; 70: 993–1001.
- Virmani P, Levin L, Myskowski PL, Flores E, Marchetti MA, Lucas AS, et al. clinical outcome and prognosis of young patients with mycosis fungoides. Pediatr Dermatol 2017; 34: 547–553.
- Wu JH, Cohen BA, Sweren RJ. Mycosis fungoides in pediatric patients: clinical features, diagnostic challenges, and advances in therapeutic management. Pediatr Dermatol 2020; 37: 18–28.
- Reiter O, Amitay-Laish I, Oren-Shabtai M, Feinmesser M, Ben-Amitai D, Hodak E. Paediatric mycosis fungoides – characteristics, management and outcomes with particular focus on the folliculotropic variant. J Eur Acad Dermatol Venereol 2022; 36: 671–679.
- Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016; 127: 2375–2390.
- Larocca C, Kupper T, Mycosis fungoides and Sézary syndrome: an update. Hematol Ocol Clin North Am 2019; 33: 103–120.
- Nuckols JD, Shea CR, Horenstein MG, Burchette JL, Prieto VG. Quantitation of intraepidermal T-cell subsets in formalin-fixed, paraffin-embedded tissue helps in the diagnosis of mycosis fungoides, J Cutan Pathol 1999; 26: 169–175.
- Boccara O, Blanche S, de Prost Y, Brousse N, Bodemer C, Fraitag S, Cutaneous hematologic disorders in children, Pediatr Blood Cancer 2012; 58: 226–232.
- Boulos S, Vaid R, Aladily TN, Ivan DS, Talpur R, Duvic M, Clinical presentation, immunopathology, and treatment of juvenile-onset mycosis fungoides: a case series of 34 patients. J Am Acad Dermatol 2014; 71: 1117–1126.
- Koh M J-A, Chong W-S. Narrow-band ultraviolet B phototherapy for mycosis fungoides in children. Clin Exp Dermatol 2014; 39: 474–478.
- Brazzelli V, Bernacca C, Segal A, Barruscotti S, Bolcato V, Michelerio A, et al. Photo-photochemotherapy in juvenile-onset mycosis fungoides: a retrospective study on 9 patients. J Pediatr Hematol Oncol 2019; 41: 34–37.
- Krutmann J. Therapeutic photoimmunology: photoimmunological mechanisms in photo(chemo)therapy. J Photochem Photobiol B 1998; 44: 159–164.
- Nanda A, AlSaleh QA, Al-Ajmi H, Al-Sabah H, Elkashlan M, Al-Shemmari S, et al. Mycosis fungoides in Arab children and adolescents: a report of 36 patients from Kuwait, Pediatr Dermatol 2010; 27: 607–613.
- Yazganoglu KD, Topkarci Z, Buyukbabani N, Baykal C. Childhood mycosis fungoides: a report of 20 cases from Turkey. J Eur Acad Dermatol Venereol 2013; 27: 295–300.
- Ramsay DL, Parnes RE, Dubin N. Response of mycosis fungoides to topical chemotherapy with mechlorethamine, Arch Dermatol 1984; 120: 1585–1590.
- Micaily B, Miyamoto C, Kantor G, Lessin S, Rook A, Brady L, et al. Radiotherapy for unilesional mycosis fungoides. Int J Radiat Oncol Biol Phys 1998; 42: 361–364.
- Huen AO, Kim EJ. The role of systemic retinoids in the treatment of cutaneous T-cell lymphoma. Dermatol Clin 2015; 33: 715–729.
- Zackheim HS, Kashani-Sabet M, McMillan A. Low-dose methotrexate to treat mycosis fungoides: a retrospective study in 69 patients, J Am Acad Dermatol 2003; 49: 873–878.
- Whittaker S, Hoppe R, HM. How I treat mycosis fungoides and Sézary syndrome. Blood 2016; 127: 3142–3153.
- Ben-Amitai D, Michael D, Feinmesser M, Hodak E. Juvenile mycosis fungoides diagnosed before 18 years of age. Acta Derm Venereol 2003; 83: 451–456.
- Willemze R, Jaffe ES, Burg G, Cerroni L, Berti E, Swerdlow SH, et al. WHO-EORTC classification for cutaneous lymphomas, Blood 2005; 105: 3768–3785.
- Hodak E, Amitay-Laish I. Mycosis fungoides: a great imitator. Clin Dermatol 2019; 37: 255–267.
- Walia R, Yeung CCS. An update on molecular biology of cutaneous T cell lymphoma. Front Oncol 2019; 9: 1558.
- Ponti R, Quaglino P, Novelli M, Fierro MT, Comessatti A, Peroni A, et al. T-cell receptor gamma gene rearrangement by multiplex polymerase chain reaction/heteroduplex analysis in patients with cutaneous T-cell lymphoma (mycosis fungoides/Sézary syndrome) and benign inflammatory disease: correlation with clinical, histological and immunophenotypical findings. Br J Dermatol 2005; 153: 565–573.
- Travaglino A, Varricchio S, Pace M, Russo D, Picardi M, Baldo A. Borrelia burgdorferi in primary cutaneous lymphomas: a systematic review and meta-analysis. J Dtsch Dermatol Ges 2020; 18: 1379–1384.
- Brunner PM, Guttman-Yassky E, Leung DYM. The immunology of atopic dermatitis and its reversibility with broad-spectrum and targeted therapies. J Allergy Clin Immunol 2017; 139: S65–S76.
- Zhou H, Luo ZD, Tang XH, Han JD, Gao Q. Folliculotropic mycosis fungoides associated with atopic dermatitis. Australas J Dermatol 2018; 59: e143–e145.
- Olsen EA, Hodak E, Anderson T, Carter JB, Henderson M, Cooper K, et al. Guidelines for phototherapy of mycosis fungoides and Sézary syndrome: a consensus statement of the United States Cutaneous Lymphoma Consortium. J Am Acad Dermatol 2016; 74: 27–58.