Epidermolysis bullosa acquisita is a pemphigoid disease characterized by autoantibodies against type VII collagen. This study compared the sensitivity and specificity of 6 diagnostic assays: type VII collagen non-collagenous domains enzyme-linked immunoassay (NC1/2 ELISA) (MBL, Nagoya, Japan); type VII collagen NC1 ELISA (Euroimmun, Lübeck, Germany); indirect immunofluorescence (IF) microscopy test based on the expression of recombinant NC1 in a human cell line (NC1 BIOCHIP®; Euroimmun); full-length recombinant type VII collagen ELISA; immunoblotting with full-length type VII collagen in the extract of human dermis; and immunoblotting with recombinant NC1. Immunoblotting with recombinant NC1 showed a sensitivity of 93.1% and specificity of 100%, followed by NC1 BIOCHIP® (sensitivity, 89.1%; specificity, 100%), immunoblotting with human dermis (sensitivity, 87.1%; specificity 100%), NC1-ELISA (sensitivity 82.2%; specificity 98.6%), NC1/NC2 ELISA (sensitivity 88.1%; specificity 93.3%), and full-length type VII collagen ELISA (sensitivity 80.2%; specificity 93.8%).
Key words: epidermolysis bullosa acquisita; autoantibody; type VII collagen; BIOCHIP; enzyme-linked immunoassay; immunoblot.
Accepted Feb 23, 2021; Epub ahead of print Mar 9, 2021
Acta Derm Venereol 2021; 101: adv00420.
doi: 10.2340/00015555-3774
Corr: Stephanie Goletz, Lübeck Institute for Experimental Dermatology, University of Lübeck, Ratzeburger Allee 160, DE-23538 Lübeck, Germany. E-mail: stephanie.goletz@uksh.de
SIGNIFICANCE
Epidermolysis bullosa acquisita belongs to the autoimmune blistering skin diseases. The disease is characterized by autoantibodies against type VII collagen, a structural protein of the junction between the epidermis and the dermis. In this study we compared the sensitivities and specificities of 6 diagnostic assays. The highest diagnostic performance was observed for immunoblotting using the recombinant non-collagenous NC1 domain of collagen type VII and the commercial NC1 BIOCHIP®.
INTRODUCTION
Epidermolysis bullosa acquisita (EBA) is a rare autoimmune bullous disease (AIBD) with a prevalence of 2.8/million in Germany (1). The disease is characterized by tissue-bound and circulating autoantibodies against type VII collagen (Col7), which is part of the basal membrane zone (BMZ) of the skin (2–4). The binding of anti-Col7 autoantibodies leads to complement activation at the BMZ and, subsequently, to the influx of leukocytes and dermal–epidermal splitting, which manifests as subepidermal blistering (5, 6). Clinically, EBA can present as inflammatory variant with erythemas and tense blisters/erosions resembling bullous pemphigoid or linear IgA disease, and a mechanobullous form with non-inflammatory lesions predominantly on mechanically-stressed parts of the skin (Fig. 1a) (7). Approximately 50% of patients also show lesions on surface-close mucous membranes (8).
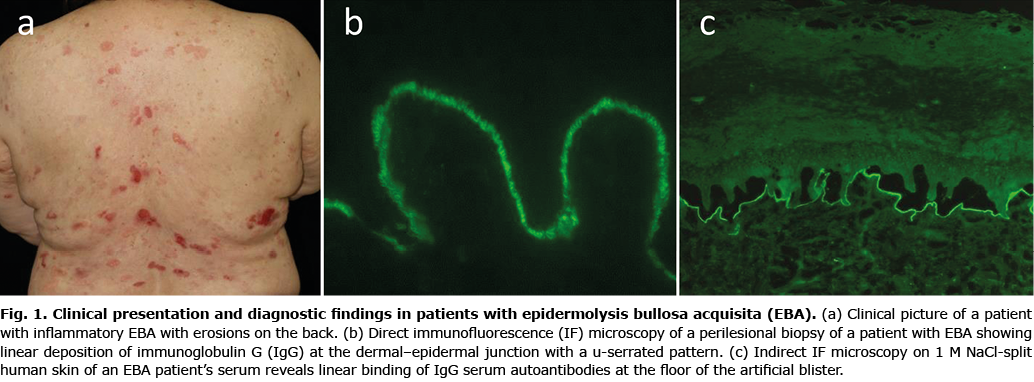
Diagnosis of EBA relies on: (i) clinical presentation; (ii) detection of autoantibodies by direct immunofluorescence (IF) or immunoelectron microscopy of perilesional skin biopsies showing linear deposits of IgG (in some cases IgA alone or combined with IgG) and/or complement C3 along the BMZ; and/or (iii) evidence for serum antibodies against Col7 (Fig. 1b) (9). Circulating autoantibodies against Col7 have been reported in approximately 60% of patients with EBA, and can be detected by different assays (7). Serration pattern analysis of direct IF microscopy allows the differentiation of EBA from other pemphigoid diseases with a so-called u-serrated pattern, seen only in autoimmunity against Col7 (10). This method has a high inter-rater reliability and can easily be integrated in a routine laboratory using 6-µm cryosections and a standard IF microscope with a ×400 magnification (11, 12). Serum autoantibodies in EBA label the dermal side of the artificial blister by indirect IF on human salt-split skin (SSS). This binding pattern contrasts the epidermal binding seen in bullous pemphigoid, the, by far, more frequent AIBD, but is indistinguishable from the labelling seen in the about equally frequent anti-laminin 332 pemphigoid and the approximately 5-fold more frequent anti-p200 pemphigoid (Fig. 1c) (9, 13). Circulating autoantibodies against Col7 can be detected by different assays including both commercial and in-house systems. Col7 is composed of 3 identical α1 chains, which build a triple helical structure. Each chain contains a large collagenous domain flanked by 2 non-collagenous domains (NC1 and NC2) (3). Lapiere et al. (14) described the NC1 domain as the immunodominant region in EBA, while some patients also develop autoantibodies against the NC2 domain (4, 14–16).
This retrospective blinded study included a large number of sera from patients with EBA and other AIBD to determine the sensitivities and specificities of 3 commercial and 3 in-house assays for the detection of serum anti-Col7 IgG.
MATERIALS AND METHODS
Human sera
In this multicentre study sera from patients with EBA (n = 101) were collected retrospectively at the dermatology departments in Lübeck (Germany, n = 36), Kurume (Japan, n = 52), and Rome (Italy, n = 13). EBA was diagnosed based on: (i) a compatible clinical picture (7, 8); and/or (ii) linear deposits of IgG, IgA and/or C3 at the dermal–epidermal junction by direct IF of a perilesional biopsy; and (iii) reactivity with Col7 by immunoblotting with extract of human dermis, reactivity with the recombinant NC1 domain of Col7 by enzyme-linked immunoassay (ELISA) (Euroimmun, Lübeck, Germany) (17) or reactivity with the recombinant NC1/NC2 domain of Col7 by ELISA (MBL, Nagoya, Japan) (9, 14). As controls, sera from patients with anti-p200 pemphigoid (n = 65), anti-laminin 332 mucous membrane pemphigoid (n = 6), bullous pemphigoid (n = 99), and pemphigus vulgaris (n = 40) were applied as diagnosed by national or international guidelines (18–20) or as previously detailed (21, 22). The study was performed following the Declaration of Helsinki and approved by the ethics committee of the University of Lübeck (12-178, amended 15.02.2019). Sera were stored at –20°C or –80°C until use.
Serum analysis
All sera (diluted 1:10 in PBS) were analysed by indirect IF microscopy on 6-µm cryosections of human SSS using a fluorescein isothiocyanate (FITC)-conjugated monoclonal anti-human IgG detection antibody (1:50; Sigma Aldrich, Munich, Germany). All Col7-specific assays detailed below were performed blinded in Paris (full-length Col7 ELISA) and Lübeck (all other tests).
NC1 and NC1/NC2 enzyme-linked immunoassay
The Col7-NC1 ELISA (anti-type VII collagen ELISA, Euroimmun) and the Col7-NC1/NC2 ELISA (MESACUP Anti-Type VII Collagen Test, MBL, Fig. 2a) were performed according to the manufacturers’ instructions. Sere were diluted 1:101 and the absorbance of each well was measured at 450 nm using a plate reader (GloMax® Discover, Promega, Walldorf, Germany). A reference wavelength of 620 nm was applied. The relative units/ml (RU/ml) and units/ml (U/ml), respectively, were calculated for each ELISA according to the information provided by the manufacturers. Data were analysed using Excel, and values were illustrated as dot plots using the software GraphPad Prism8 (GraphPad Software Inc., San Diego, California USA).

Full-length Col7 enzyme-linked immunoassay
Recombinant full-length Col7 was purified from conditioned medium of a SV40-immortalized recessive dystrophic epidermolysis bullosa (RDEB) keratinocyte cell line (23) transduced with a COL7A1 retroviral vector, as described previously (24). The protein was purified from serum-free culture supernatant by anion-exchange chromatography on an AKTA prime FPLC (Amersham Biosciences, Amersham, UK) according to Chen et al. (25) after concentration using a Vivaflow tangential flow filtration system (cut-off 100 kDa; Sartorius, Göttingen, Germany).
Patient sera (diluted 1:50 up to 1:3200) were incubated on Nunc MaxiSorp 96-well microtitre plates coated with Col7 (540 ng/well). Control wells without serum or healthy control serum were run on each plate in parallel. Bound anti-Col7 antibodies were detected with peroxidase- conjugated antibody to human immunoglobulins (ab8504, Abcam, Cambridge, UK). Signal was revealed using 3,3’,5,5’-tetramethylbenzidine (TMB) peroxidase substrate (09743, Sigma-Aldrich, St Louis, USA) on a plate reader (Packard).
In previously published full-length Col7 ELISA, a standard curve was made with a serial dilution of a pool of 10 EBA patient sera. Using this pool, the ELISA score cut-off threshold was calculated at 17.9 (26, 27). However, as this standard pool was exhausted, a serial dilution of commercially available human IgG against human Col7 (CA 1947-0101, Euroimmun) was used as standard curve in the current study. The test was validated using a cohort of 20 healthy donors and EBA patient sera. Receiver operating characteristic (ROC) plot established the new cut-off threshold for the ELISA score at 174, with a sensitivity and specificity of the assay of 82% and 95%, respectively (calculations were performed using Graphpad Prism 5).
NC1 BIOCHIP®
Slides with BIOCHIP® mosaics (Euroimmun) containing recombinant NC1-Col7 expressing HEK293 cells and empty plasmid transfected HEK293 cells were used as previously reported (Fig. 2B) (17). Briefly, HEK293 cells growing on cover glasses were transfected with a plasmid containing the sequence for the NC1 domain of Col7 or with the empty plasmid, respectively. After 48 h, cells were fixed, cover glasses were cut into millimetre-sized biochips and glued onto incubation slides. Slides were incubated with sera diluted 1:10 according to the manufacturer’s instructions.
Immunoblotting
Recombinant NC1 (amino acids 1-1253; Euroimmun (17)) and extract of human dermis (28) were fractionated by sodium dodecylsulfate polyacrylamide gel electrophoresis (SDS-PAGE), transferred to nitrocellulose membrane and immunoblotted as reported (Fig. 2C) (29). Human sera were diluted 1:50 in Tris-buffered saline with 0.05% Tween20 (TBST) containing 5% skimmed-milk powder plus 1% bovine serum albumin (BSA) in TBST and incubated overnight at 4°C. As secondary antibody horseradish peroxidase (HRP)-conjugated monoclonal mouse anti-human IgG4 antibody (Southern Biotech, Birmingham, AL, USA) was used. The proteins were visualized by diaminobenzidine (Merck, Darmstadt, Germany).
RESULTS
Indirect IF microscopy on human salt-split skin
Of the 101 EBA sera, 97 revealed IgG labelling along the dermal side of the artificial blister, resulting in a sensitivity of 96%. Of the 211 control sera, 5 BP sera showed dermal binding in addition to IgG reactivity along the blister roof, at titres of 1:10, while anti-BP180 NC16A ELISA values ranged between 48 and 1566 U/ml. These 5 BP sera were positive in the full-length Col7 ELISA, but not in any other assay (Table I).

Col7-specific assays
The highest sensitivity was observed in immunoblotting with recombinant NC1, with a sensitivity of 93.1%, followed by the NC1 BIOCHIP® (89.1%), NC1/NC2 ELISA (88.1%) and the immunoblotting employing extract of human dermis (87.1%). The Col7-specific assays with the highest specificities of 100% were the NC1 BIOCHIP® and the 2 immunoblottings with dermal extract, and the NC1 domain, followed by the NC1 ELISA (specificity, 98.6%; Table I). The tests with the lowest specificities, at 93.3% and 93.8%, were the NC1/NC2 ELISA and the full-length Col7 ELISA, respectively. When only sera from patients with anti-p200 pemphigoid and anti-laminin 332 mucous membrane pemphigoid, which showed an identical binding pattern to that of EBA sera by indirect IF on human SSS, were used, the specificities were 97.2% (NC1 ELISA) 87.3% (NC1/NC2 ELISA) and 93.0% (full-length Col7 ELISA). The highest diagnostic accuracy determined by combining sensitivity and specificity of the individual test systems was observed for immunoblotting with recombinant NC1, followed by the NC1 BIOCHIP® (Table I). The values for the 3 Col7-specific ELISA are detailed in Fig. 3. When results for anti-Col7 serum reactivities were analysed separately for European and Japanese patients with EBA, the highest sensitivities for the different assays in the Japanese patients were observed in the Col7 NC1/NC2 ELISA and Col7 NC1 immunoblot (both 96.2%) followed by immunoblotting with dermal extract and the NC1 BIOCHIP® (sensitivities of 92.0%; Table II). In the European EBA sera, the highest sensitivities were obtained by immunoblotting with Col7 NC1 (91.8%) and the NC1 BIOCHIP® (85.7%) followed by immunoblotting with dermal extract and the full-length Col7 ELISA (both 83.7%).


DISCUSSION
The aim of this retrospective study was the blinded determination of the diagnostic accuracy of several Col7-specific assays for the detection of serum IgG autoantibodies in a large cohort of patients with EBA and other AIBD.
EBA usually requires long-term immunosuppressive and/or immunomodulatory therapy, including high-dose corticosteroids, azathioprine, mycophenoles, colchicine, dapsone, rituximab, and high-dose intravenous immunoglobulins (6, 8, 30, 31). Disease activity in EBA is more difficult to suppress than most other AIBDs, including bullous pemphigoid, mucous membrane pemphigoid, and anti-p200 pemphigoid (6, 8, 21, 30). Thus, an exact diagnosis of EBA is essential to initiate optimal treatment.
Direct immunoelectron microscopy was considered the diagnostic gold-standard for EBA (8, 28, 34). Since this method is available only in a few laboratories worldwide, and biopsies need to be analysed immediately and cannot be sent away, in most EBA patients the diagnosis is based on other methods. The introduction of the serration pattern analysis by Vodegel et al. in 2004 provided an alternative for the detection of tissue-bound antibodies against Col7 (10). This method is, however, not yet widely used, although it has revealed a high inter-rater reliability and requires only 6-µm cryosections and a standard IF microscope with a ×400 magnification (11, 12). At present, most physicians rely on various serological assays to detect circulating Col7-specific autoantibodies for the diagnosis of EBA. However, only a few data are available about the comparative performance of these assays.
In the current study, sera from large cohorts of patients with AIBD, collected at different centres, were subjected to 3 commercial and 3 in-house assays for the detection of serum anti-Col7 IgG. The highest diagnostic accuracy was observed for the in-house immunoblot applying recombinant NC1 (sensitivity 93.1%, specificity 100%), followed by the commercial NC1 BIOCHIP® (sensitivity 89.1%, specificity 100%). For the NC1 BIOCHIP®, this finding is in line with previous studies by Komorowski et al. (17), who reported a sensitivity and specificity of 91.8% and 99.8%, respectively, and by Marzano et al. (33), who found reactivity in all 6 EBA and none of the 11 other AIBD and control sera, but contrasts with data by Seta et al. (27), who found only 27% of EBA sera were positive in the NC1 BIOCHIP®. This discrepancy may be explained by the different inclusion criteria of the latter study, which assayed sera based on immunoelectron microscopy results, and not on the presence of Col7-specific serum antibodies as in the current study. The different study designs are also reflected by the low number of SSS-positive EBA sera (43%) (27), compared with 96% in the present study.
Among the 2 other commercially available Col7- specific tests, the NC1 ELISA had a slightly higher performance than the NC1/NC2 ELISA, which was mainly due to the higher specificity of 98.6%, compared with 93.3%, while the sensitivity of the NC1 ELISA was lower (82.2% vs 88.1%). Other studies with similar inclusion criteria using the NC1/NC2 ELISA have observed sensitivities of 79.2% (n = 24) (34), 80.8% (n = 21) (35), 93.8% (n = 49) (14), 96.7% (n = 30) (36), 97.9% (n = 95) (37), and 100% (n = 6) (33) with specificities between 98.1% and 100%. The only other study that directly compared the NC1 and the NC1/NC2 ELISA showed a higher sensitivity of the NC1/NC2 ELISA (97.9%, n = 95) compared with the NC1 ELISA (89.5%) (37). The higher sensitivity of the NC1/NC2 ELISA may be due to a selection bias, since most, if not all, patients with EBA had been pre-diagnosed using this assay. This view is supported by the sensitivities for both ELISAs, of 82.2% and 88.1%, in the present study, which correspond well with the sensitivity of 89.5% in the NC1 ELISA in the latter study (37). Of note, while the specificities of the NC1 (98.7%, n = 200) and NC1/NC2 ELISA (99.3%) in the previous studies were both relatively high, in the present study, the specificity of the NC1 ELISA of 98.6% was comparable, while it was considerably lower for the NC1/NC2 ELISA (93.3%). This discrepancy was mainly due to the high reactivity of anti-p200 pemphigoid sera in the NC1/NC2 ELISA (12%), an AIBD cohort not included in the other study. This observation might be explained by epitope spreading, which is a common phenomenon in anti-p200 pemphigoid sera (38).
The NC1 immunoblot was identified as the (in-house) test with the highest diagnostic performance. However, this assay is not widely available. In addition, although accredited by the German Accreditation Board (DAkkS, D-ML-13069-06-00), this assay does not have the same level of standardization with regard to storability and batch control systems compared with the commercial systems. The full-length Col7 ELISA showed comparable sensitivity and specificity of 80.6% and 93.8%, respectively, compared with SSS-positive patients with EBA in the original description (80% and 97%) (27). Of interest, indirect IF microscopy on SSS also revealed a high sensitivity (96%) and specificity (97.6%). In particular, the sensitivity of this in-house test varied considerably, with 74.7% (n = 95) (37), 83.3% (n = 24) (34), 91.4% (n = 105) (39), and 100% (n = 49) (14), which is most likely explained by inclusion criteria of the studies and quality of SSS. Unfortunately, indirect IF microscopy on SSS is not sufficient for the diagnosis of EBA, since anti-p200 pemphigoid and anti-laminin 332 mucous membrane pemphigoid have the same binding pattern. In the current study, 5 BP sera also showed binding to the blister floor on SSS at low titres, while anti-BP180 NC16A ELISA reactivity was observed. This phenomenon might be explained by epitope spreading, which can occur during the course of disease (38).
When the sensitivities of the different assays were compared in the subgroups of European and Japanese patients with EBA, a higher autoantibody detection rate in the Japanese patients was observed in all assays beside the full-length Col7 ELISA. This may be explained by a difference in the frequency of serum anti-Col7 autoantibodies between the 2 populations, genetic differences, or differences within the defined inclusion criteria of the present study. Furthermore, the current study shows that the differences in sensitivities between the 2 cohorts in NC1 ELISA and NC1/NC2 ELISA seem to be wider than for the other tests (except for full-length Col7 ELISA), which may be explained by comparing different test systems with different sensitivities and specificities.
The strength of the present study is the large cohort of patients with EBA and the blinded designs. For a high practicability and usability of data, ELISA systems were compared using the cut-off values of the manufacturer, instead of calculating cut-offs based on the chosen study populations. The study is limited by its retrospective approach and the inclusion criteria that required serum reactivity in a Col7-specific assay. As pointed out by Jonkman et al. (40), only approximately half of EBA sera show serum reactivity against Col7. In the present study, those other 50% of patients with EBA who can only be diagnosed by immunoelectron microscopy or serration pattern analysis have not been covered and, as such, the much lower sensitivities for anti-Col7 antibodies in studies that used these diagnostic methods can be explained (27, 41). In detail, the study performed by Terra et al. (41) in 2013 detected a sensitivity of 80% for the Col7-NC1/NC2 ELISA in a subgroup of patients positive in indirect IF using human SSS, whereas it was only 23% in SSS-negative patients. Regarding a subgroup of prospective EBA sera (n = 20), including 10 SSS-negative sera, the authors observed a sensitivity of 45% using Col7 NC1/NC2 ELISA (41). Furthermore, the rare patients with EBA with exclusive IgA autoantibodies have not been included in the current study.
In summary, in this, so far largest, serological study of patients with EBA, the highest diagnostic performance of Col7-specific serological assays was found to be the immunoblot with recombinant NC1 and, among the commercially available tests, the NC1 BIOCHIP®. These tests will be valuable for the diagnosis of EBA for those physicians without access to immunoelectron microscopy and pattern analysis of direct IF microscopy.
ACKNOWLEDGEMENTS
The authors thank Sarah Gaugel, Lübeck, and Pierre Bonnesoeur, Paris, for excellent technical assistance. IDI-IRCCS and the Department of Dermatology, University of Lübeck, are healthcare providers of the European Reference Network (ERN)-Skin.
This work was supported by grants from the Deutsche Forschungsgemeinschaft through CRU 303 Pemphigoid Diseases and Excellence Cluster Precision Medicine in Chronic Inflammation (EXC 2167). Type VII collagen NC1/2 ELISA (MBL, Nagoya, Japan) was purchased for a reduced price, type VII collagen NC1 ELISA and BIOCHIP® (Euroimmun, Lübeck, Germany) were provided free of charge.
DZ and ES have a scientific cooperation with Euroimmun. The other authors have declared no conflicts of interest.
REFERENCES
- Hubner F, Recke A, Zillikens D, Linder R, Schmidt E. Prevalence and age distribution of pemphigus and pemphigoid diseases in Germany. J Invest Dermatol 2016; 136: 2495–2498.
- Woodley DT, Briggaman RA, O’Keefe EJ, Inman AO, Queen LL, Gammon WR. Identification of the skin basement-membrane autoantigen in epidermolysis bullosa acquisita. N Engl J Med 1984; 310: 1007–1013.
- Goletz S, Zillikens D, Schmidt E. Structural proteins of the dermal–epidermal junction targeted by autoantibodies in pemphigoid diseases. Exp Dermatol 2017; 26: 1154–1162.
- Woodley DT, Burgeson RE, Lunstrum G, Bruckner-Tuderman L, Reese M, Briggaman RA. Epidermolysis bullosa acquisita antigen is the globular carboxyl terminus of type VII procollagen. J Clin Invest 1988; 81: 683–687.
- Kasperkiewicz M, Sadik CD, Bieber K, Ibrahim SM, Manz RA, Schmidt E, et al. Epidermolysis bullosa acquisita: from pathophysiology to novel therapeutic options. J Invest Dermatol 2016; 136: 24–33.
- Koga H, Prost-Squarcioni C, Iwata H, Jonkman MF, Ludwig RJ, Bieber K. Epidermolysis bullosa acquisita: the 2019 Update. Front Med (Lausanne) 2018; 5: 362.
- Vorobyev A, Ludwig RJ, Schmidt E. Clinical features and diagnosis of epidermolysis bullosa acquisita. Expert Rev Clin Immunol 2017; 13: 157–169.
- Schmidt E, Groves R. Immunobullous diseases. In: Griffith C, Barker J, Chalmers, Bleiker T, Creamer D, editors. Rook’s textbook of dermatology, part 3, chapter 50, 9th edition. Chichester: Wiley-Blackwell, 2016; 50: p. 1–56.
- Prost-Squarcioni C, Caux F, Schmidt E, Jonkman MF, Vassileva S, Kim SC, et al. International Bullous Diseases Group: consensus on diagnostic criteria for epidermolysis bullosa acquisita. Br J Dermatol 2018; 179: 30–41.
- Vodegel RM, Jonkman MF, Pas HH, de Jong MC. U-serrated immunodeposition pattern differentiates type VII collagen targeting bullous diseases from other subepidermal bullous autoimmune diseases. Br J Dermatol 2004; 151: 112–118.
- Meijer JM, Atefi I, Diercks GFH, Vorobyev A, Zuiderveen J, Meijer HJ, et al. Serration pattern analysis for differentiating epidermolysis bullosa acquisita from other pemphigoid diseases. J Am Acad Dermatol 2018; 78: 754–759e6.
- Terra JB, Meijer JM, Jonkman MF, Diercks GF. The n- vs. u-serration is a learnable criterion to differentiate pemphigoid from epidermolysis bullosa acquisita in direct immunofluorescence serration pattern analysis. Br J Dermatol 2013; 169: 100–105.
- Lau I, Goletz S, Holtsche MM, Zillikens D, Fechner K, Schmidt E. Anti-p200 pemphigoid is the most common pemphigoid disease with serum antibodies against the dermal side by indirect immunofluorescence microscopy on human salt-split skin. J Am Acad Dermatol 2019; 81: 1195–1197.
- Lapiere JC, Woodley DT, Parente MG, Iwasaki T, Wynn KC, Christiano AM, et al. Epitope mapping of type VII collagen. Identification of discrete peptide sequences recognized by sera from patients with acquired epidermolysis bullosa. J Clin Invest 1993; 92: 1831–1839.
- Saleh MA, Ishii K, Kim YJ, Murakami A, Ishii N, Hashimoto T, et al. Development of NC1 and NC2 domains of type VII collagen ELISA for the diagnosis and analysis of the time course of epidermolysis bullosa acquisita patients. J Dermatol Sci 2011; 62: 169–175.
- Ishii N, Yoshida M, Hisamatsu Y, Ishida-Yamamoto A, Nakane H, Iizuka H, et al. Epidermolysis bullosa acquisita sera react with distinct epitopes on the NC1 and NC2 domains of type VII collagen: study using immunoblotting of domain-specific recombinant proteins and postembedding immunoelectron microscopy. Br J Dermatol 2004; 150: 843–851.
- Komorowski L, Muller R, Vorobyev A, Probst C, Recke A, Jonkman MF, et al. Sensitive and specific assays for routine serological diagnosis of epidermolysis bullosa acquisita. J Am Acad Dermatol 2013; 68: e89–e95.
- Feliciani C, Caldarola G, Kneisel A, Podstawa E, Pfutze M, Pfutzner W, et al. IgG autoantibody reactivity against bullous pemphigoid (BP) 180 and BP230 in elderly patients with pruritic dermatoses. Br J Dermatol 2009; 161: 306–312.
- Schmidt E, Sticherling M, Sardy M, Eming R, Goebeler M, Hertl M, et al. S2k guidelines for the treatment of pemphigus vulgaris/foliaceus and bullous pemphigoid: 2019 update. J Dtsch Dermatol Ges 2020; 18: 516–526.
- Joly P, Horwath B, Patsatsi A, Uzun S, Bech R, Beissert S, et al. Updated S2K guidelines on the management of pemphigus vulgaris and foliaceus initiated by the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol 2020; 34: 1900–1913.
- Goletz S, Hashimoto T, Zillikens D, Schmidt E. Anti-p200 pemphigoid. J Am Acad Dermatol 2014; 71: 185–191.
- Goletz S, Probst C, Komorowski L, Schlumberger W, Fechner K, van Beek N, et al. A sensitive and specific assay for the serological diagnosis of antilaminin 332 mucous membrane pemphigoid. Br J Dermatol 2019; 180: 149–156.
- Mecklenbeck S, Compton SH, Mejia JE, Cervini R, Hovnanian A, Bruckner-Tuderman L, et al. A microinjected COL7A1-PAC vector restores synthesis of intact procollagen VII in a dystrophic epidermolysis bullosa keratinocyte cell line. Hum Gene Ther 2002; 13: 1655–1662.
- Titeux M, Pendaries V, Zanta-Boussif MA, Decha A, Pironon N, Tonasso L, et al. SIN retroviral vectors expressing COL7A1 under human promoters for ex vivo gene therapy of recessive dystrophic epidermolysis bullosa. Mol Ther 2010; 18: 1509–1518.
- Chen M, Costa FK, Lindvay CR, Han YP, Woodley DT, The recombinant expression of full-length type VII collagen and characterization of molecular mechanisms underlying dystrophic epidermolysis bullosa. J Biol Chem 2002; 277: 2118–2124.
- Pendaries V, Gasc G, Titeux M, Leroux C, Vitezica ZG, Mejia JE, et al. Immune reactivity to type VII collagen: implications for gene therapy of recessive dystrophic epidermolysis bullosa. Gene Ther 2010; 17: 930–937.
- Seta V, Aucouturier F, Bonnefoy J, Le Roux-Villet C, Pendaries V, Alexandre M, et al. Comparison of 3 type VII collagen (C7) assays for serologic diagnosis of epidermolysis bullosa acquisita (EBA). J Am Acad Dermatol 2016; 74: 1166–1172.
- Zillikens D, Kawahara Y, Ishiko A, Shimizu H, Mayer J, Rank C V et al. A novel subepidermal blistering disease with autoantibodies to a 200-kDa antigen of the basement membrane zone. J Invest Dermatol 1996; 106: 1333–1338.
- Groth S, Recke A, Vafia K, Ludwig RJ, Hashimoto T, Zillikens D, et al. Development of a simple enzyme-linked immunosorbent assay for the detection of autoantibodies in anti-p200 pemphigoid. Br J Dermatol 2011; 164: 76–82.
- Iwata H, Vorobyev A, Koga H, Recke A, Zillikens D, Prost-Squarcioni C, et al. Meta-analysis of the clinical and immunopathological characteristics and treatment outcomes in epidermolysis bullosa acquisita patients. Orphanet J Rare Dis 2018; 13: 153.
- Kridin K, Kneiber D, Kowalski EH, Valdebran M, Amber KT. Epidermolysis bullosa acquisita: a comprehensive review. Autoimmun Rev 2019; 18: 786–795.
- Prost C, Dubertret L, Fosse M, Wechsler J, Touraine R. A routine immuno-electron microscopic technique for localizing an auto-antibody on epidermal basement membrane. Br J Dermatol 1984; 110: 1–7.
- Marzano A V, Cozzani E, Biasin M, Russo I, and Alaibac M, The use of Biochip immunofluorescence microscopy for the serological diagnosis of epidermolysis bullosa acquisita. Arch Dermatol Res 2016; 308: 273–276.
- Calabresi V, Sinistro A, Cozzani E, Cerasaro C, Lolicato F, Muscianese M, et al. Sensitivity of different assays for the serological diagnosis of epidermolysis bullosa acquisita: analysis of a cohort of 24 Italian patients. J Eur Acad Dermatol Venereol 2014; 28: 483–490.
- Horvath O N, Varga R, Kaneda M, Schmidt E, Ruzicka T, Sardy M. Diagnostic performance of the “MESACUP anti-Skin profile TEST”. Eur J Dermatol 2016; 26: 56–63.
- Kim JH, Kim YH, Kim S, Noh EB, Kim SE, Vorobyev A, et al. Serum levels of anti-type VII collagen antibodies detected by enzyme-linked immunosorbent assay in patients with epidermolysis bullosa acquisita are correlated with the severity of skin lesions. J Eur Acad Dermatol Venereol 2012; 27: e224–e230.
- Schmidt T, Hoch M, Lotfi Jad SS, Solimani F, Di Zenzo G, Marzano AV, et al. Serological diagnostics in the detection of IgG autoantibodies against human collagen VII in epidermolysis bullosa acquisita: a multicentre analysis. Br J Dermatol 2017; 177: 1683–1692.
- Holtsche MM, Goletz S, von Georg A, van Beek N, Hubner F, Pigors M, et al. Serological characterization of anti-p200 pemphigoid: epitope spreading as a common phenomenon. J Am Acad Dermatol 2021; 84: 1155–1157.
- Hashimoto T, Jin Z, Ishii N. Clinical and immunological studies for 105 Japanese seropositive patients of epidermolysis bullosa acquisita examined at Kurume University. Expert Rev Clin Immunol 2016; 12: 895–902.
- Jonkman MF, Meijer JM, Diercks GFH, Pas HH. Response to ‘Serological diagnostics in the detection of IgG autoantibodies against human collagen VII in epidermolysis bullosa acquisita: a multicentre analysis’. Br J Dermatol 2018; 178: 573.
- Terra JB, Jonkman MF, Diercks GF, and Pas HH. Low sensitivity of type VII collagen enzyme-linked immunosorbent assay in epidermolysis bullosa acquisita: serration pattern analysis on skin biopsy is required for diagnosis. Br J Dermatol 2013; 169: 164–167.