REVIEW ARTICLE
Comparative outcomes of endodontically treated teeth versus dental implant-supported prostheses: a systematic review
Miguel Fernando Bordaa, Salomón Páez-Garcíab, Luisa Fernanda Murciac, Luis Carlos Venegas-Sanabriac,d and Miguel Germán Bordae,f
aBGR Dental, West Palm Beach, FL, USA; bSemillero de Neurociencias y Envejecimiento, Ageing Institute, Medical School, Pontificia Universidad Javeriana, Bogotá, Colombia; cResearch Department, Hospital Universitario Mayor-Méderi, Universidad del Rosario, Bogotá, Colombia; dRosarist Institute for the Study of Aging and Longevity, Universidad del Rosario, Bogotá, Colombia; eCentre for Age-Related Medicine (SESAM), Stavanger University Hospital, Stavanger, Norway; fDepartment of Neurology, Clínica Universidad de Navarra, Pamplona, Spain.
ABSTRACT
Objective: The objective of this study was to compare the clinical and patient-related outcomes of root canal therapy (RCT) and dental implants (DIs) in managing severe tooth damage, supporting evidence-based treatment decisions.
Material and methods: A systematic review was performed in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Six databases were searched: Cochrane Library, Embase, Medline, LILACS, Scopus, and Web of Science. Studies comparing clinical and patient-reported outcomes in adult patients treated with either RCT or DIs were included. The Joanna Briggs Institute Critical Appraisal Checklists were used to assess the risk of bias. Due to significant heterogeneity among studies, meta-analysis was not feasible, and findings were synthesised qualitatively. PROSPERO registration: CRD42024584113.
Results: Out of 1,876 initial records, 12 studies met inclusion criteria: 7 cohort studies, 4 case-control studies, and 1 randomised controlled trial. Most studies had low to moderate risk of bias. Both RCT and DIs demonstrated high survival rates, with RCT slightly outperforming DIs in terms of success. Failure rates ranged from 0.7% to 12.0%, with no significant differences between treatments. DIs were associated with a higher frequency of postoperative interventions and complications. Patient-reported outcomes such as pain, satisfaction, and quality of life (QoL) were comparable across both modalities.
Conclusion: RCT and DIs both offer viable and effective solutions for restoring severely damaged teeth, with high survival and success rates and low failure rates. Both treatments were also associated with favourable patient-reported outcomes, including minimal pain, high satisfaction, and improved QoL. The decision between treatments should consider clinical factors, patient preferences, cost, accessibility, potential complications, and patient-centred outcomes. Shared decision-making is essential for optimal patient care.
KEYWORDS: root canal therapy; endodontics; dental implant; single tooth implant; outcomes assessment
Citation: ACTA ODONTOLOGICA SCANDINAVICA 2025; VOL. 84: 386–396. DOI: https://doi.org/10.2340/aos.v84.43871.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Odontologica Scandinavica Society. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 10 December 2024; Accepted: 13 May 2025; Published: 24 June 2025.
CONTACT: Miguel G. Borda, MD, PhD. mmborda@gmail.com Centre for Age-Related Medicine (SESAM), Stavanger University Hospital, PB 8100, N-4068 Stavanger, Norway
Supplemental data for this article can be accessed online at https://doi.org/10.2340/aos.v84.43871
Competing interests and funding: The authors report there are no competing interests to declare.
The study funding was provided by a grant from the Norwegian Health Association. This paper represents independent research supported by the Norwegian government through hospital owner Helse Vest (Western Norway Regional Health Authority).
Introduction
When a tooth experiences significant structural damage because of decay, trauma, or infection, it can lead to serious dental conditions such as pulpitis and periapical pathology. These issues compromise the function and integrity of the affected tooth, potentially leading to complications like abscesses, systemic infections, or persistent pain if not promptly managed. Timely intervention is therefore essential to preserve oral health and prevent further deterioration [1–3].
Dental practitioners often face two primary options for managing such cases: preserving the natural tooth through root canal therapy (RCT) followed by appropriate prosthetic restoration, or extracting the tooth and replacing it with a standalone prosthetic solution, typically a dental implant (DI). RCT focuses on preserving the natural tooth by removing the infected or inflamed pulp tissue, disinfecting the canal system, and sealing it to prevent reinfection. In contrast, when preservation is no longer feasible, extraction and replacement with an implant-supported prosthesis provide an alternative that restores function and aesthetics.
Each treatment approach offers distinct benefits and limitations. RCT aims to preserve the natural tooth, maintaining its original structure and function. However, it may require multiple appointments, carries a risk of reinfection, and can weaken the tooth over time. In contrast, tooth extraction results in edentulism – a condition linked to adverse outcomes in older adults, including malnutrition, functional disability, cognitive decline, and poor self-rated health status [4]. DIs provide a highly effective alternative when tooth preservation is not feasible, offering excellent durability, and long-term success. Nevertheless, implant placement is more invasive, entails higher initial costs, and requires a longer recovery period, with potential complications such as implant failure or bone loss [5, 6]. As such, RCT and DIs differ markedly in terms of procedural complexity, healing time, cost, patient preference, and both clinical and patient-reported outcomes [7]. These factors are critical in guiding individualised treatment decisions.
Despite widespread use of both RCT and DIs, few studies directly compare their clinical and patient-reported outcomes using standardised definitions. Existing literature often focuses on survival or success rates without adequately addressing patient-centred metrics such as pain, satisfaction, or quality of life (QoL).
This systematic review aims to critically evaluate and compare the clinical outcomes and patient experiences associated with RCT and DI-supported prostheses. By synthesising current evidence, this study aims to guide clinicians in making informed treatment decisions in collaboration with their patients.
Materials and methods
This systematic review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (shown in Appendix2 B) [8].
PICO Strategy
- Population: Adults (≥18 years) with compromised teeth due to pulpal or periapical diseases who required dental treatment.
- Interventions: Initial endodontic treatment, non-surgical or surgical endodontic retreatment.
- Comparators: Dental implants, including single or multiple dental prostheses.
- Outcomes: Described in the following subsections.
Primary outcomes
- Survival: Defined as the presence of the tooth or implant in the patient’s oral cavity at the last documented follow-up.
- Success: Defined as the presence of the tooth or implant without any further intervention or planned intervention.
- Failure: Defined as the condition requiring retreatment or reconsideration of the treatment option.
Secondary outcomes
- Complications: For endodontic procedures, this included flare-ups, accidental events during treatment, and post-placement issues. For implants, complications included unscheduled visits because of severe pain or swelling, surgical complications, bone loss, and esthetic or phonetic concerns.
- Patient-reported outcomes: Evaluated using patient-reported measures, including pain levels before and after treatment, satisfaction, and QoL assessed by instruments such as the Oral Health Impact Profile (OHIP) [9] in its various forms (OHIP-49, OHIP-14, or OHIP-19).
Search strategy
A systematic search was conducted in six databases, Cochrane Library, Embase, Medline, LILACS (Latin American and Caribbean Health Sciences Literature), Scopus, and Web of Science, to identify studies comparing outcomes in adult patients (aged 18 years or older) who underwent either RCT or received DIs. A combination of key search terms was employed, including ‘root canal therapy’, ‘endodontic treatment’, ‘dental implants’, and ‘tooth implant’. The development of the search strategy, including the identification of appropriate search terms (both index terms and keywords) and the definition of the search structure (use of Boolean operators, truncation, and wildcards), was initially carried out by one author (LFM). To ensure the strategy’s accuracy and comprehensiveness, it was subsequently reviewed and refined by two additional authors (MGB and LCV). The final search was performed by LFM and completed in February 2025.
In addition, a supplementary screening was conducted in February 2025 using Google Scholar and BASE (Bielefeld Academic Search Engine), along with manual searches of the reference lists of selected studies and relevant systematic reviews. This complementary search did not identify any additional studies meeting the eligibility criteria for inclusion in the review.
Selection criteria
The following inclusion criteria were applied:
- Original research studies: interventional (randomised controlled trial) and observational studies (cohort, case-control, and cross-sectional studies).
- Studies written in any language.
- Studies that directly compare outcomes between RCT and DIs.
Reviews, dissertations conference proceedings, letters or poster abstracts were excluded. No publication date restrictions were applied. The complete search strategy is detailed in Appendix A.
Screening and data collection
Following removing duplicate records, two independent reviewers (LFM, MGB) screened the titles and abstracts of identified studies using the RAYYAN web-based application [10]. Full-text articles of potentially eligible studies were then reviewed to ensure they met all inclusion criteria (MFB, LFM). Any discrepancies between reviewers were resolved through discussion, and if necessary, a third reviewer was consulted to achieve consensus (MFB). When multiple articles from the same study population met the inclusion criteria, preference was given to the article with the most comprehensive outcome data, the largest sample size, or the most recent publication date.
Data extraction and analysis
Two independent reviewers used a standardised data extraction form to extract data (MFB, LFM). The extracted data included the principal author, publication year, country, type of study, collection dates, selection criteria, sample size, age, sex, treatment details, follow-up duration, outcomes, and key findings. Discrepancies in data extraction were resolved by discussion or consulting a third reviewer.
Risk of bias assessment
Two authors (LFM and MFB) independently evaluated each study for risk of bias using the Joanna Briggs Institute (JBI) Critical Appraisal Checklists [11], which were appropriate for the study design. Based on the responses to the checklist items, studies were categorised as having low, moderate, high, or critical risk of bias. Any disagreements among reviewers during the risk of bias assessment were resolved through discussion or, if needed, by consultation with a third reviewer (LCV).
The study protocol was registered in PROSPERO (CRD42024584113).
Results
The database search initially identified 1,876 records. Following a review of titles and abstracts, 21 articles were selected for full-text review. Of these, 9 articles and 3 studies [12–14] were excluded because they reported data already presented in other studies included in this review; 5 studies [15–19] were excluded for evaluating interventions not aligned with the scope of this review or addressing outcomes beyond its predefined objectives; 1 article [20] was excluded due to being published in Persian, as a suitable translation could not be obtained for proper assessment (Figure 1).

Figure 1. Flowchart of the systematic review process [21].
Risk of bias assessment
The results of the critical appraisal process are reported in Figure 2 [22]. Most of the included studies showed low to moderate risk of bias across the evaluated domains. Specifically, the studies presented some concerns in confounding adjustment [23–31] and follow-up process [27, 28, 30, 31].

Figure 2. Risk of bias assessment for (a) case-control studies, (b) cohort studies, and (c) randomised controlled trial. The ROBVIS tool® was used to generate this figure [22].
In addition, in four studies [28, 30–32], it was unclear whether participants were free of the outcome at the start of the study or at the moment of exposure. The single randomised controlled trial included [33] showed a high risk of bias in several domains, most notably because of the substantial discrepancy between the estimated sample size of 240 participants (120 per group) and the final analysis, which was based on only 20 patients, as well as deviations from the intended intervention. A global summary of quality assessment is presented in Figure 3 [22].
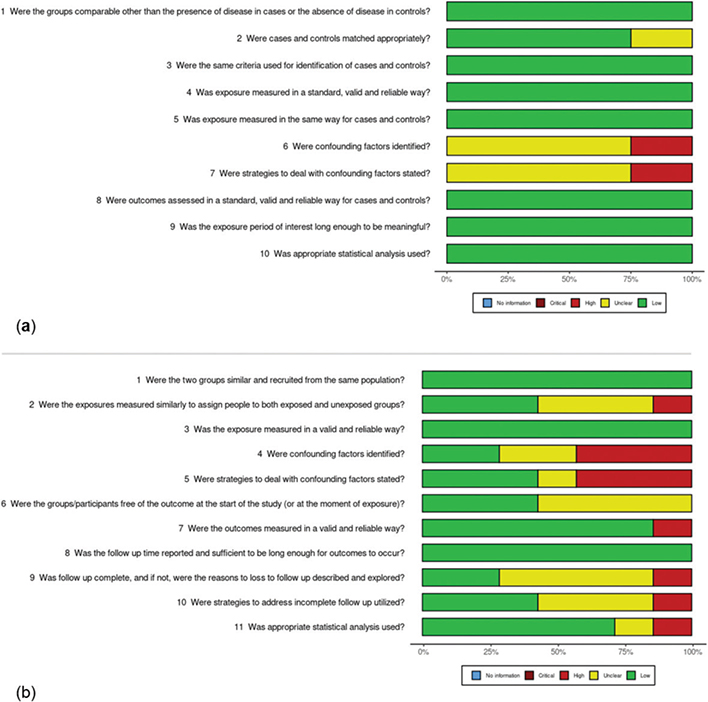
Figure 3. Global quality assessment for (a) case-control studies, (b) cohort studies. The ROBVIS tool® was used to generate this figure [22].
Due to the considerable heterogeneity among the included studies, a meta-analysis was not performed. This heterogeneity was related to differences in study design, population characteristics, and the timing and methods used to measure both primary and secondary outcomes. These variations limited the comparability of results across studies, making it unfeasible to generate a pooled estimate. Consequently, a qualitative and descriptive synthesis of the findings was conducted.
Overview of included studies
A total of 12 studies were included in the systematic review, comprising 7 cohort studies [27, 28, 30–32, 34, 35], 4 case-control studies [23–26], and 1 randomised controlled trial [33]. In general, the studies had a minimum follow-up time of 1 year, and considering all follow-up times for both treatments, the mean follow-up time was 2.8 years. They described non-surgical RCT followed by subsequent coronal restoration performed by dental students, graduate residents, or staff clinicians. Implants were generally described as single-tooth restorations supported by a single implant, surgically placed by staff or resident oral surgeons or periodontists, and restored by staff or resident prosthodontists. The studies compared the outcomes of RCT and DIs across the primary outcomes, including survival rates [23–25, 32, 34], success rates [23–25, 27, 31–33, 35], and failure rates [23–25, 27, 31, 33, 34], and secondary outcomes, including complications [23–25, 27, 30, 33] and patient-reported outcomes, such as QoL, measured by OHIP scores [23, 25, 30, 32] (Table 1).
Survival, success, and failure rates
Regarding the survival rates, both RCT and DIs showed high survival rates across multiple studies [24, 31, 32, 34] and reported a >95% survival rate for both treatments, having a similar good prognosis. Success rates varied between treatments, with RCT generally showing slightly higher success rates. Two case-control studies [23, 25] reported lower success rates, with 73.5% for DIs and 82.1% for RCT in one study and 75.3% for RCT and 56.7% for DIs in the other. Failure rates ranged from 0.7% to 12% across the studies [23–25, 27, 33, 34], with no significant differences noted, except in a cohort study [34] where implant therapy exhibited significantly lower failure rates than RCT (1.1% vs. 4.1%).
In terms of postoperative complications, implants were associated with more postoperative interventions compared to RCT. One cohort study reported that implants required more postoperative treatments to maintain them despite having similar success rates to RCT [25]. Three case-control studies noted that DI was associated with more postoperative complications than RCT, reported survival with intervention (17.9% vs. 3.6%), reinterventions (12.4% vs. 1.3%), additional treatment (42% vs. 11%), or a number of clinical or technical complications [25, 30]. In the clinical trial [33], three patients in the endodontic group experienced one complication each, compared to a single complication reported in the implant group; this difference was not statistically significant (Table 2).
Patient-reported outcomes
Patient-reported outcomes such as pain, satisfaction, and overall QoL were generally similar between the two treatments [24–26, 28]. No significant differences were detected in overall OHIP scores between RCT and DIs, although some dimensions, like physical pain, showed slight differences favouring DI (Table 3).
Discussion
This systematic review compared primary and secondary outcomes of RCT and DIs to support evidence-based shared decision-making in dental practice. Overall, no differences were found between the two procedures. Therefore, other factors, such as cost or the impact of edentulism, should guide treatment decisions. Edentulism, particularly in older adults, is associated with adverse outcomes such as depression, malnutrition, and cognitive decline [36–38]. Hakeem et al. found that each missing tooth increases frailty risk in individuals aged 60 years and older. These considerations are important when deciding whether to extract a natural tooth [39].
Dentists should provide patients with detailed and objective information on each treatment option – including costs, success and failure rates, complications, and patient-reported outcomes like pain and QoL – to enable shared decision-making. Despite the relevance of these issues, few studies have directly compared outcomes between RCT and DIs.
Both treatments demonstrated high survival rates. One study reported a 95% survival rate at 5 years, while another found slightly higher DI survival at 3 years (98.7% vs. 95.1%) [24]. Another study reported 99% DI survival and 87.6% RCT survival at 5 years [32]. However, inconsistencies in survival definitions – such as including teeth with unhealed or uncertain status [23], or using different criteria like absence of mobility or radiolucency [31] – make comparisons challenging. These variations notwithstanding, both treatments generally showed strong survival rates.
Success rates also varied across studies because of differing definitions. Most defined success as the absence of reintervention, often supplemented by radiographic criteria such as the absence of radiolucency (RCT) or marginal bone loss ≤4 mm (DIs) [35]. Lee et al. found DIs had higher clinical (97.2% vs. 83.7%) and radiological success (96.4% vs. 81.2%) at 5 years [32]. Zang et al. also favoured DIs (100% vs. 88%) [35], whereas Doyle and Hamasha found better outcomes for RCT (75.3%–82.1% vs. 56.7%–73.5%) [23, 25]. Some studies found similar success rates for both [24, 27], though factors like periodontal disease and caries influenced DI outcomes. Suganna et al. reported no significant difference, noting that overlapping definitions of success and survival complicate comparisons [31]. Thus, success rates depend largely on study definitions and clinician expertise.
Failure rates were low and comparable across treatments. Failure was generally defined as the removal or planned removal of the treated tooth or implant. Causes of failure included prosthetic, periodontal and endodontic issues [23], infections, foreign body reactions [27], loss of osseointegration, and fractures [34]. Risk factors such as age, anxiety [34], systemic disease, smoking, and bone density influenced outcomes in both procedures. Clinician skills remain critical to minimising failure risk.
Complications varied in type and frequency. DI was associated with more reinterventions. Hannahan et al. reported 12.4% for DIs versus 1.3% for RCT [27], and Vahdati et al. reported 42.0% for DIs versus 11.0% for RCT [24]. RCT complications included caries, procedural mishaps, flare-ups, and fractures [24, 30, 33]. DI complications involved more frequent medication use (100% vs. 2%) [24], abutment loosening [33], sensory disturbances, bone loss, and esthetic or mechanical issues [24]. Despite these, patient-reported satisfaction and perceived complication rates remained high for both treatments [24]. Although direct comparison is difficult due to heterogeneous reporting, complication rates were low and should be discussed with patients during treatment planning.
Patient-related outcomes – including pain, satisfaction, and QoL – were favourable for both treatments. QoL was assessed using the OHIP, particularly the OHIP-14 scale [9], which showed notable improvements after both procedures [24, 25, 28]. Hamasha et al. found that gender influenced perceived improvement, with women reporting more significant gains [25]. Pain levels were minimal across both treatments in the short and long term [26, 30], and no significant differences in satisfaction were found [30]. While RCT may cause more procedural discomfort, overall patient experiences were positive and comparable.
This review should be interpreted with caution because of certain limitations. Inconsistencies in outcome definitions and follow-up durations limited direct comparisons. Study quality varied, with issues such as incomplete confounding control, loss to follow-up, and insufficient baseline data. While procedures were conducted by trained clinicians, many studies lacked details on prognostic factors like systemic health, radiographic findings, and patient preferences. Some included studies were older and may not reflect current clinical practices. In addition, most studies were from the USA [23, 24, 27, 28, 30, 32, 34], China [35], Spain [26], India [31], Italy [33], and Saudi Arabia [25]. The lack of data from Latin America, Africa, or Oceania may limit generalisability due to cultural, socioeconomic, and healthcare disparities.
A key limitation of this review is the reliance on observational studies, which are prone to bias because of lack of randomisation. For instance, patients with less severe cases may have been more likely to receive RCT, while more complex cases were directed to implant treatment, introducing selection bias. In addition, uncontrolled confounders such as patient health status or clinician experience may affect outcomes and limit the strength of causal conclusions.
Despite these limitations, this review contributes meaningfully to the existing literature. It builds upon earlier systematic reviews [40–42], including Torabinejad et al., which compared outcomes of RCT, DIs, fixed prostheses, and extraction without replacement [43]. A more recent review done by Sinsareekul et al. included eight observational studies and found mixed results: some reported no difference in short-term survival, while others found higher DI survival or fewer complications [40]. Patient satisfaction remained high across treatments.
Future research should standardise definitions of success and failure, and adopt prospective designs with clear follow-up criteria [44]. Studies should also assess periodontal and peri-implant health, as well as patient-level risk factors such as age, systemic disease, and lifestyle. Investigating long-term effects in diverse populations will enhance the generalisability of findings [45]. Personalising treatment by considering individual health status, gender, and preferences can further improve outcomes [38, 44, 46]. Lastly, incorporating cost-effectiveness analyses would aid in balancing clinical benefits with patient and systemic financial constraints [18, 35, 47, 48].
Conclusions
This systematic review found that both RCT and DIs are effective treatment options for managing severely compromised teeth, demonstrating high survival and success rates, alongside low complication and failure rates. Importantly, both treatments were also associated with favourable patient-reported outcomes, including low levels of pain, high satisfaction, and comparable improvements in QoL. These findings support the importance of incorporating patient-centred outcomes into treatment planning. The choice between treatments should be guided by a thorough assessment of individual clinical factors, patient preferences, anticipated long-term outcomes, and economic considerations. Future research should incorporate more diverse populations and emphasise standardised definitions, patient-centred outcomes, and cost-effectiveness analyses to enhance evidence-based clinical decision-making.
Review registration
The protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO) No. CRD42024584113. As part of the review process, the original search strategy defined in the PROSPERO-registered protocol was updated in February 2025. In addition to the databases originally specified (MEDLINE, EMBASE, LILACS, and The Cochrane Library), the search was expanded to include Scopus, Web of Science, BASE (Bielefeld Academic Search Engine), and Google Scholar. This update aimed to ensure a more comprehensive identification of relevant studies and minimise publication bias.
Author contributions
MGB, SPG, MFB, LFM: Conception of work, formal analysis, methodology, visualisation, writing-reviewing and editing.
MGB, MFB, and LFM: Preparation of the initial draft, manuscript writing, review, and approval.
LCV, SPG, LFM and MFB: Revision and approval of the final version.
References
[1] Galler KM, Weber M, Korkmaz Y, Widbiller M, Feuerer M. Inflammatory response mechanisms of the dentine-pulp complex and the periapical tissues. Int J Mol Sci. 2021;22:1480. https://doi.org/10.3390/ijms22031480
[2] De Armas V, Erdogan O, Yoon H, Abdennour M, Gibbs JL. Contribution of endodontic pathology to persistent orofacial paIn: a case report. J Endod. 2022;48:1178–84. https://doi.org/10.1016/j.joen.2022.06.010
[3] Ye L, Cao L, Song W, Yang C, Tang Q, Yuan Z. Interaction between apical periodontitis and systemic disease (Review). Int J Mol Med. 2023;52:60. https://doi.org/10.3892/ijmm.2023.5263
[4] Venegas-Sanabria LC, Moreno-Echeverry MM, Borda MG, Chavarro-Carvajal DA, Cano-Gutierrez CA. Oral health and self-rated health in community-dwelling older adults in Colombia. BMC Oral Health. 2023;23:772. https://doi.org/10.1186/s12903-023-03401-4
[5] Cecchinato D, Marino M, Håkansson J, Lindhe J, Derks J. Occurrence of complications in patients restored with implants. Clin Oral Implants Res. 2022;33:913–20. https://doi.org/10.1111/clr.13970
[6] Huang Y, Levin L. Barriers related to dental implant treatment acceptance by patients. Int J Oral Maxillofac Implants. 2022;37:1210–16. https://doi.org/10.11607/jomi.9643
[7] Iqbal MK, Kim S. A review of factors influencing treatment planning decisions of single-tooth implants versus preserving natural teeth with nonsurgical endodontic therapy. J Endod. 2008;34:519–29. https://doi.org/10.1016/j.joen.2008.01.002
[8] Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1. https://doi.org/10.1186/2046-4053-4-1
[9] Slade GD, Spencer AJ. Development and evaluation of the oral health impact profile. Community Dent Health. 1994;11:3–11.
[10] Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5:210. https://doi.org/10.1186/s13643-016-0384-4
[11] Joanna Briggs Institute. Critical appraisal tools [Internet]. 2017 [cited 2020 Nov 3]. Available from: https://joannabriggs.org/critical-appraisal-tools
[12] Alfred P. A retrospective comparison of single tooth implants with endodontically treated teeth. J Periodontol. 2022;93(2):E48.
[13] Esposito M, Tallarico M, Trullenque-Eriksson A, Gianserra R. Endodontic retreatment vs dental implants of teeth with an uncertain endodontic prognosis: 1-year results from a randomised controlled trial. Eur J Oral Implant. 2017;10:293–308.
[14] Doyle SL, Hodges JS, Pesun IJ, Baisden MK, Bowles WR. Factors affecting outcomes for single-tooth implants and endodontic restorations. J Endod. 2007;33:399–402. https://doi.org/10.1016/j.joen.2006.12.025
[15] Asopa SS, Asopa V, Arya A, Attargekar V, Chabra C, Gupta D. Comparison of long-term outcome of implant supported crowns and root canal treated crowns: an observational study. NeuroQuantology. 2022;20:2866–9. https://doi.org/10.14704/nq.2022.20.10.NQ55276
[16] Woodmansey KF, Ayik M, Buschang PH, White CA, He J. Differences in masticatory function in patients with endodontically treated teeth and single-implant-supported prostheses: a pilot study. J Endod. 2009;35:10–14. https://doi.org/10.1016/j.joen.2008.10.016
[17] Pennington MW, Vernazza CR, Shackley P, Armstrong NT, Whitworth JM, Steele JG. Evaluation of the cost-effectiveness of root canal treatment using conventional approaches versus replacement with an implant. Int Endod J. 2009;42:874–83. https://doi.org/10.1111/j.1365-2591.2009.01582.x
[18] Ermatinger S, Lee W-Z, Thoma DS, Hüsler J, Hämmerle CHF, Naenni N. Clinical outcomes of tooth- and implant- supported restorations performed in a university-based undergraduate program after 13 to 15 years. Int J Prosthodont. 2024;37:261–70. https://doi.org/10.11607/ijp.8264
[19] de España C, Olivieri J-G, Ortega-Martinez J, Morelló S, Roig-Cayón M, Durán-Sindreu F. Dental anxiety, cardiovascular changes and patient preconceptions toward implants and root canal treatments: an observational study. J Clin Exp Dent. 2022;14:e809–14. https://doi.org/10.4317/jced.59281
[20] Momeni G, Rafiei E, Ranjbarian P, Babaei S. Evaluation of oral health related quality of life after implant treatment versus root canal treatment. J Isfahan Dent Sch. 2022;18(4):348–55. https://doi.org/10.18502/ijds.v18i4.12092
[21] Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: an R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and open synthesis. Campbell Syst Rev. 2022;18:e1230. https://doi.org/10.1002/cl2.1230
[22] McGuinness LA, Higgins JPT. Risk-of-bias VISualization (robvis): an R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods. 2021;12:55–61. https://doi.org/10.1002/jrsm.1411
[23] Doyle SL, Hodges JS, Pesun IJ, Law AS, Bowles WR. Retrospective cross sectional comparison of initial nonsurgical endodontic treatment and single-tooth implants. Compend Contin Educ Dent. 2007;28:296–301. https://doi.org/10.1016/S0084-3717(08)70479-3
[24] Vahdati SA, Torabinejad M, Handysides R, Lozada J. A retrospective comparison of outcome in patients who received both nonsurgical root canal treatment and single-tooth implants. J Endod. 2019;45:99–103. https://doi.org/10.1016/j.joen.2018.10.018
[25] Hamasha A-H, Nbhan A. Root canal treatment with postcore restoration versus implant restoration: clinical and radiographic outcome and quality of life after treatment. Saudi Endod J. 2019;9:88. https://doi.org/10.4103/sej.sej_67_18
[26] Sanz E, Azabal M, Arias A. Quality of life and satisfaction of patients two years after endodontic and dental implant treatments performed by experienced practitioners. J Dent. 2022;125:104280. https://doi.org/10.1016/j.jdent.2022.104280
[27] Hannahan JP, Eleazer PD. Comparison of success of implants versus endodontically treated teeth. J Endod. 2008;34:1302–5. https://doi.org/10.1016/j.joen.2008.08.011
[28] Gatten DL, Riedy CA, Hong SK, Johnson JD, Cohenca N. Quality of life of endodontically treated versus implant treated patients: a university-based qualitative research study. J Endod. 2011;37:903–9. https://doi.org/10.1016/j.joen.2011.03.026
[29] Shabahang S, Bohsali K, Boyne PJ, Caplanis N, Lozada J, Torabinejad M. Effect of teeth with periradicular lesions on adjacent dental implants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:321–6. https://doi.org/10.1016/S1079-2104(03)00367-6
[30] Torabinejad M, Salha W, Lozada JL, Hung Y-L, Garbacea A. Degree of patient pain, complications, and satisfaction after root canal treatment or a single implant: a preliminary prospective investigation. J Endod. 2014;40:1940–5. https://doi.org/10.1016/j.joen.2014.08.022
[31] Suganna M, Jena D, Jhala NS, Baghel RS, Afzal N, Singh S. Single tooth implant vs non‑surgical root canal: long‑term survival rates. J Pharm Bioall Sci. 2024;16:S3156–9. https://doi.org/10.4103/jpbs.jpbs
[32] Lee C, Alfred P, Tran D, James J, Makins SR, Gajjar D, et al. A long‐term retrospective analysis of single tooth implants and endodontic therapies in a university setting. J Periodontol. 2022;93:1510–24. https://doi.org/10.1002/JPER.21-0390
[33] Esposito M, Sbricoli L, Buti J, Uccioli U, Tallarico M. Endodontic retreatment of teeth with uncertain endodontic prognosis versus dental implants : 5-year results from a randomised controlled trial. Clin Trials Dent. 2020;2:27–43. https://doi.org/10.36130/CTD.04.2020.03
[34] Chatzopoulos GS, Koidou VP, Lunos S, Wolff LF. Implant and root canal treatment: survival rates and factors associated with treatment outcome. J Dent. 2018;71:61–6. https://doi.org/10.1016/j.jdent.2018.02.005
[35] Zang H-L, Zhang Y, Hao X-W, Yang L, Liang Y-H. Cost-effectiveness analysis: nonsurgical root canal treatment versus single-tooth implant. BMC Oral Health. 2023;23:489. https://doi.org/10.1186/s12903-023-03173-x
[36] Azzolino D, Passarelli PC, De Angelis P, Piccirillo GB, D’Addona A, Cesari M. Poor oral health as a determinant of malnutrition and sarcopenia. Nutrients. 2019;11:2898. https://doi.org/10.3390/nu11122898
[37] Desai JP, Nair RU. Oral health factors related to rapid oral health deterioration among older adults: a narrative review. J Clin Med. 2023;12:3202. https://doi.org/10.3390/jcm12093202
[38] Borda MG, Castellanos-Perilla N, Patiño JA, Castelblanco S, Cano CA, Chavarro-Carvajal D, et al. Edentulism and its relationship with self-rated health: secondary analysis of the SABE Ecuador 2009 Study. Acta Odontol Latinoam. 2017;30:83–9.
[39] Hakeem FF, Bernabé E, Sabbah W. Association between oral health and frailty among American older adults. J Am Med Dir Assoc. 2021;22:559–63.e2. https://doi.org/10.1016/j.jamda.2020.07.023
[40] Sinsareekul C, Saengthong-Aram P, Limpuangthip N. Survival, complications, and patient-reported outcomes of endodontically treated teeth versus dental implant-supported prostheses: a systematic review. J Prosthet Dent. 2025;133(3):669–76. https://doi.org/10.1016/j.prosdent.2024.02.007
[41] Torabinejad M, Lozada J, Puterman I, White SN. Endodontic therapy or single tooth implant? A systematic review. J Calif Dent Assoc. 2008;36:429–37. https://doi.org/10.1080/19424396.2008.12221510
[42] Torabinejad M, Dinsbach NA, Turman M, Handysides R, Bahjri K, White SN. Survival of intentionally replanted teeth and implant-supported single crowns: a systematic review. J Endod. 2015;41:992–8. https://doi.org/10.1016/j.joen.2015.01.004
[43] Torabinejad M, Anderson P, Bader J, Brown LJ, Chen LH, Goodacre CJ, et al. Outcomes of root canal treatment and restoration, implant-supported single crowns, fixed partial dentures, and extraction without replacement: a systematic review. J Prosthet Dent. 2007;98:285–311. https://doi.org/10.1016/S0022-3913(07)60102-4
[44] Bhattacharyya S, Das DP, Bhattacharyya A, Maity AB, Das D. Clinical guideline and treatment planning decisions of single-tooth implants versus preserving natural teeth with nonsurgical endodontic therapy. J Fam Med Prim Care. 2020;9:2654–8. https://doi.org/10.4103/jfmpc.jfmpc_128_20
[45] King S, Thaliph A, Laranjo L, Smith BJ, Eberhard J. Oral health literacy, knowledge and perceptions in a socially and culturally diverse population: a mixed methods study. BMC Public Health. 2023;23:1446. https://doi.org/10.1186/s12889-023-16381-5
[46] Orishko A, Imber J-C, Roccuzzo A, Stähli A, Salvi GE. Tooth- and implant-related prognostic factors in treatment planning. Periodontol 2000. 2024;95:102–28. https://doi.org/10.1111/prd.12597
[47] Wigsten E, Kvist T, Husberg M, EndoReCo, Davidson T. Cost‐effectiveness of root canal treatment compared with tooth extraction in a Swedish Public Dental Service: A prospective controlled cohort study. Clin Exp Dent Res. 2023;9:661–9. https://doi.org/10.1002/cre2.759
[48] Duncan HF, Kirkevang L-L, Peters OA, El-Karim I, Krastl G, Del Fabbro M, et al. Treatment of pulpal and apical disease: the European Society of Endodontology (ESE) S3-level clinical practice guideline. Int Endod J. 2023;56(Suppl. 3):238–95. https://doi.org/10.1111/iej.13974