RESEARCH ARTICLE
Effect of occlusal reduction on post-operative pain of symptomatic and asymptomatic molar teeth
Aysenur Kamacı Esena, Fatma Furuncuoğlua, Fatima Betul Basturkb, Muhammet Nuri Taşcıoğlua and Masoud Parirokhc
aDepartment of Endodontics, Sakarya University, Sakarya, Türkiye; bDepartment of Endodontics, Istanbul Gelisim University, Istanbul, Türkiye; cDepartment of Endodontics, Kerman University of Medical Sciences, Kerman, Iran
ABSTRACT
Objective: This study aimed to compare the intensity of post-operative pain after single-visit root canal treatment of symptomatic or asymptomatic teeth following occlusal reduction.
Methods: A total of 140 symptomatic or asymptomatic patients in need of root canal therapy were registered in this prospective, single-centre, single-blind, randomised clinical trial. For all patients, root canal treatment was carried out in a single visit, and the teeth were restored using composite resin. The patients were randomly allocated into four treatment groups, two of which included occlusal reduction while two treatments left the occlusional contacts intact. Patients’ pain were assessed using a 0–3 verbal rate scale 1, 3, and 7 days following root canal treatment. The pain incidence and intensity were compared using the chi-square and Fisher’s exact tests.
Results: Overall, the post-operative pain intensity was low. Symptomatic individuals had significantly more discomfort at day 1 post-operatively compared to asymptomatic patients (p < 0.008). The pain incidence significantly decreased over time for symptomatic patients. When compared to asymptomatic patients without occlusal reduction, symptomatic patients with occlusal reduction had a greater pain incidence at day 3 (p < 0.011). For other time intervals, no significant differences in post-operative pain incidence or intensity were found.
Conclusion: Single-visit root canal treatments involving occlusal reduction in both symptomatic or asymptomatic molars had no significant effect on post-operative pain.
KEYWORDS: analgesics; occlusal reduction; post-operative pain; single-visit endodontic treatment; time interval
Citation: ACTA ODONTOLOGICA SCANDINAVICA 2025; VOL. 84: 371–376. DOI: https://doi.org/10.2340/aos.v84.43872.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Odontologica Scandinavica Society. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 14 June 2024; Accepted: 13 May 2025; Published: 11 June 2025.
CONTACT: Aysenur Kamacı Esen a.kamaci@windowslive.com Department of Endodontics, Mithatpaşa, Adnan Menderes Cd. No:122/B, 54100 Sakarya University, Sakarya, Türkiye
Competing interests and funding: The authors deny any conflicts of interest related to this study.
No funding was obtained for this study.
Introduction
Post-operative pain is a type of discomfort that develops following root canal therapy. Post-operative pain is uncomfortable for both patients and clinicians, and it begins a few hours after endodontic treatment [1]. Studies indicate that a significant number of patients experience post-operative pain following endodontic therapy [2–4]. The incidence of post-operative endodontic pain has been reported in 24% of cases on average, but it may increase up to 80% within the first 24 hours [5–7].
Several factors can contribute to the development of post-operative pain including pre-operative discomfort, traumatic occlusion, root canal obturation technique, tooth type, age, gender, and the presence of pre-operative pain [8]. As a result, managing discomfort during root canal therapy is a crucial concern. Multiple clinical investigations have evaluated the impact of various factors on post-operative pain, including the use of intracanal medication, single- or multiple-visit endodontic therapy, and the impact of irrigation activation [1, 9–11].
One key factor linked to post-operative discomfort is the effect of occlusal reduction. This has been a significant focus of research, because pain following endodontic treatment remains a major concern for both patients and practitioners. Studies have shown that occlusal reduction can help alleviate pain by minimising mechanical allodynia and reducing the activation of hypersensitive nociceptors [12]. Extensive research has been conducted to evaluate its impact both before and after endodontic treatment.
However, despite extensive research on the topic, the effect of occlusal reduction on post-operative pain remains controversial. While some studies suggest that occlusal reduction helps alleviate discomfort following endodontic treatment [13–15], others find no significant benefit in the management of post-operative pain [16–18]. These conflicting results may be due to differences in case selection criteria and treatment approaches across studies. Given these variations, the current study aims to evaluate the impact of occlusal reduction on post-operative pain in both symptomatic and asymptomatic molar teeth.
The study was designed using the Population, Intervention, Comparison, Outcome, and Study [4, 19] framework to investigate whether occlusal reduction (I) reduces post-operative pain (O) compared to teeth without occlusal reduction (C) in symptomatic and asymptomatic patients (P) following single-visit root canal treatment in a randomised clinical trial (S). The null hypothesis states that occlusal reduction has no significant effect on post-operative pain after single-visit root canal treatment.
Materials and methods
A prospective, single-centre, single-blind, randomised clinical trial was designed with the approval of the Sakarya University Faculty of Medicine Ethical Committee (Approval number: E-71522473-050.01.04-39802-329), and the research protocol was retrospectively registered in the ClinicalTrials.gov database (NCT/06953856). Volunteers who accepted to participate in this study were informed about the procedure. A written consent was signed, and a copy was given to volunteers.
Sample size calculation
Minimum sample size was determined as 30 [20] using G*Power 3.1 (Heinrich Heine University, Düsseldorf, Germany) software from a similar study. This minimum value served as the basis for determining the number of samples, as per the groups.
Patient selection and allocation
A total of 325 patients with a non-contributory medical history applied to Sakarya University Faculty of Dentistry Department of Endodontics with endodontic treatment needs between August 2020 and January 2021.
The inclusion and exclusion are listed in Table 1. The clinical diagnosis of irreversible pulpitis was confirmed through periapical radiographs, patient dental history, and a combination of diagnostic tests, including the electric pulp test (Parkell Inc., Farmingdale, NY, USA) and the cold test (Roeko Endo-Frost; Roeko, Langenau, Germany), particularly in cases where pain assessment was unclear. In addition, the duration of pulp bleeding during root canal therapy was also taken into account when diagnosing irreversible pulpitis. Figure 1 shows the patients’ distribution to the groups.
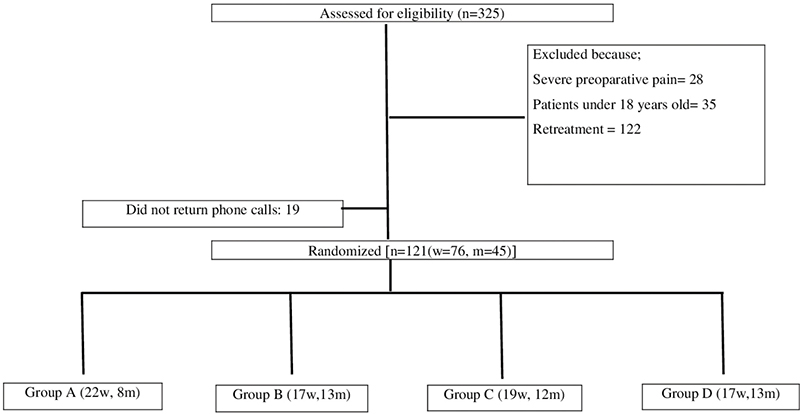
Figure 1. Flowchart of patients’ distribution to the groups.
A total of 140 patients fulfilled the inclusion criteria and were selected to take part in this clinical trial. Informed consent was obtained from all patients after they were fully informed about the procedure. The patients were notified that they would be contacted on the first, third, and seventh days after treatment, and they were given the option to reach out in case of any unexpected issues or severe pain.
Randomisation
Due to ethical considerations, patients requiring full cuspal coverage restorations who were referred from the prosthodontics department were randomly allocated to the treatment groups. All intervention and control treatment groups were assigned a number and masked from the patients. The patients scheduled to receive crowns after root canal therapy were asked to select an envelope containing a number that assigned them to one of the four treatment groups.
Root canal treatment procedure
The same endodontist (AKE), with a minimum of 5-year experience performed all root canal treatments in a single visit. The groups were as follows (n = 35):
Group A: Symptomatic teeth, occlusal contacts left intact
Group B: Asymptomatic teeth, occlusal contacts left intact
Group C: Symptomatic teeth that underwent occlusal reduction
Group D: Asymptomatic teeth that underwent occlusal reduction
Local anaesthesia was administered using 3.6 mL of lidocaine with 1:100,000 epinephrine (Adeka İlaç A.Ş, Turkey), and the affected tooth was isolated with a rubber dam. An access cavity was prepared, and any existing coronal restorations were removed. The root canal length was determined using a size #10 K-file (Micro-Mega, Besançon, France) in conjunction with an electronic apex locator (Woodpex-III, Guilin Woodpecker Medical Instrument Co., Ltd., China), with measurements taken until the device indicated a 0.0 reading. The working lengths were then calculated by subtracting 1 mm from that point. Depending on the condition of the individual root canal, apical preparation was performed using ProTaper Next rotary instruments (Dentsply Maillefer, Ballaigues, Switzerland), selecting two sizes larger than the initial apical binding file.
Between each instrument, root canals were irrigated with 2 mL of 3% NaOCl (Coltene/Whaledent, Switzerland) with a 30G side-vented endodontic needle (NaviTip, Ultradent, UT, USA) positioned 2 mm short from the working length. Before obturation, x-rays were taken with matched Gutta Percha, and final irrigation was performed as follows: 2 mL of 5% EDTA, 4 mL of 3% NaOCl, and 2 mL of distilled water.
All treatments were performed in a single session, and all teeth were obturated with AH Plus root canal sealer (Dentsply Maillefer, Ballaigues, Switzerland) and matched Gutta Percha cones. All occlusal reduction cases were selected from teeth in need of full cuspal coverage restorations. Restoration of the teeth was done in the same session using bulk-fill resin (SDR, Dentsply/DeTrey, Konstanz, Germany) and posterior resin composite (Estelite Posterior Quick, Tokuyama, Tokyo, Japan).
All occlusal contacts in the intervention groups (groups C and D) were removed and those in the control groups (groups A and B) were maintained.
The patients were advised to take 200 mg of ibuprofen every 8 hours as needed for pain management. Following the procedure, they were contacted on the first, third, and seventh days to assess and document their pain levels using the Verbal Rating Scale (VRS). The scale ranges from 0 to 3, where 0 indicates no discomfort or pain, 1 represents mild pain (not requiring analgesic medication), 2 signifies moderate pain (requiring analgesic medication), and 3 denotes severe pain (interfering with physical activity and minimally responsive to analgesics).
Statistical analysis
The data were analysed using IBM SPSS version 26.0 (SPSS Inc., Chicago, IL, USA). The Chi-square test was used to compare categorical variables between groups. The daily pain distributions by groups were assessed using the Friedman and Fisher’s Exact tests.
Results
Out of 325 patients, 140 were enrolled in the study (Figure 1). However, 19 patients were excluded due to failure to respond to follow-up phone calls regarding pain assessment. The remaining 121 patients (40 male and 81 female) completed the study, with 61 in the intervention and 60 in the control groups. In the intervention group, there were 25 males and 36 females, whereas in the control group, there were 21 males and 39 females. In addition, 18 smokers were in the intervention group, compared to 7 smokers in the control group. There was no statistically significant difference between the groups in terms of gender distribution (p = 0.5) or smoking status (p = 0.115) (Table 2). Pre-operative pain was reported by 60 patients, with half of these individuals belonging to the intervention group.
The mean pain scores are presented in Figure 2. They indicate that asymptomatic patients experienced significantly less pain than symptomatic patients on post-operative day 1 and day 3. On post-operative day 1, the pain intensity was significantly higher in symptomatic patients (groups A and C) compared to asymptomatic (groups B and D) patients (p < 0.008). However, the pain incidence gradually decreased over time in groups A and C. By day 3, the symptomatic patients continued to report significantly more discomfort than the asymptomatic patients (p < 0.011). By day 7, there were no significant differences in post-operative pain incidence or intensity between the groups.
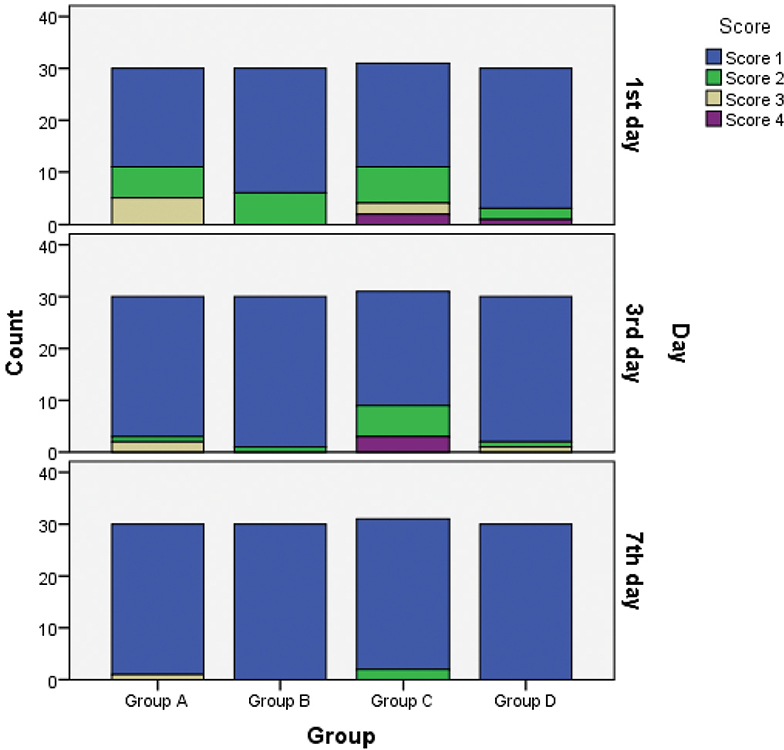
Figure 2. The pain distribution by group on the first, third, and seventh days.
The pain incidence and intensity gradually decreased over time in all groups, with no significant difference between them (p > 0.05). By post-operative day 7, there were no significant differences in post-endodontic pain among the groups (p > 0.05). However, on day 3, the differences between groups C and D and groups A and B were statistically significant (p < 0.011). Overall, occlusal reduction in molar teeth had no significant impact on post-operative pain following single-visit root canal treatment (p > 0.05).
Discussion
This study found that occlusal reduction had no significant effect on post-operative pain following single-visit root canal treatment in both symptomatic and asymptomatic molar teeth. The pain incidence and intensity were higher in both groups during the first 3 post-operative days but significantly decreased by day 7.
Several methods have been used to assess post-operative endodontic pain, often comparing pain intensity at different time points using the Visual Analogue Scale (VAS) [21] or multi-level pain classification systems [16]. We used a four-level VRS, selected for its simplicity for patients to use. Moreover, previous studies have reported that the pain classification system had no effect on the post-operative pain results across different time intervals [21, 22].
This study is a randomised, single-blind, single-centred clinical trial with patient-reported outcome measures. Participants were blinded to the interventions used to minimise performance and detection bias.
All root canal treatments in this study were performed in a single visit, as systematic reviews and meta-analyses did not reveal any significant difference in the incidence or the intensity of post-operative pain between single-visit and multiple-visit root canal treatment, even in necrotic teeth [23, 24].
Recent systematic reviews have highlighted the need for further clinical trials to better understand the role of occlusal reduction in post-operative pain [5]. However, few studies have investigated the effect of occlusal reduction in single-visit cases with a wider range of pulpal and periapical conditions. Most previous research has focused on patients with symptomatic irreversible pulpitis [25] with tenderness to percussion [15, 16] or with non-vital teeth [4]. This study, however, included vital teeth with or without symptoms and randomly allocated patients to two balanced groups based on the intervention.
Several confounding factors can influence post-endodontic pain, including gender, tooth type, and pre-operative pain [4, 13]. To minimise these effects, the study balanced the intervention and control groups based on each confounder; the gender, pre-operative pain, and smoking habit. There was no statistically significant difference in the incidence or intensity of post-operative pain between groups based on gender.
Previous studies on the effect of occlusal reduction have included both molars and premolars [13, 16], whereas some focused solely on mandibular molars [4, 22]. In this study, both maxillary and mandibular first and second molars were included to provide a broader evaluation of tooth type.
The cause of post-operative pain might be attributed to debris extrusion, instrument kinematics, and apical third enlargement [12]. Given the variation in initial apical diameters across each root canal, we decided to standardise the apical preparation to two sizes larger than the initial apical binding file with a 6% or 7% taper. A previous study comparing different preparation sizes and tapers found that apical enlargement to two sizes larger than the initial apical file with a 4% taper had lower success rates compared to a 6% taper [26]. Since all instrumentation techniques cause some degree of apical debris extrusion, this can trigger an inflammatory response in periradicular tissues [12]. In a recent systematic review and meta-analysis [27], rotary instrumentation resulted in a lesser debris extrusion into the periapical areas compared to reciprocation; therefore, in the present study, each tooth was treated using rotary instruments with a crown-down approach to minimise debris extrusion.
After chemo-mechanical preparation, the same operator completed the root canal treatment. The amount of apically extruded obturation material might differ according to the filling techniques. Warm vertical compaction technique had a higher percentage of sealer extrusion to periradicular tissues [23]. In the studies where filling techniques were the same between groups, the choice of sealer did not affect post-operative pain [28]. Therefore, the root canals were filled using the lateral compaction technique with a resin-based sealer. One of the limitations of this study is the lack of contribution of several operators, which might have enhanced the external validity of the results [4, 29].
All occlusal reduction cases in this study were selected from teeth requiring full cuspal coverage restorations, allowing for the inclusion of asymptomatic patients as well. However, if a tooth undergoing occlusal reduction does not receive a full cuspal coverage afterwards, it may lose functionality [16]. Thus, clinicians should inform patient about the potential drawbacks of occlusal reduction [16].
In addition, the presence of pre-operative pain might be a strong predictor of post-operative pain [7, 16], a finding that was confirmed in this study. On post-operative days 1 and 3, the symptomatic patients reported higher levels of pain incidence and intensity compared to the asymptomatic patients. However, by day 7, there was no statistically significant difference in post-operative pain between the two groups.
In the present study, patients were categorised based on the presence or absence of pre-operative pain, with the primary objective being to assess pain resolution following occlusal reduction rather than comparing the severity of the pre-operative pain. Consequently, only the presence or absence of pain was considered in the analysis. However, given the potential consequences of variations in pre-operative pain levels among groups, this circumstance may be regarded as a limitation of the present study.
Clinical trials are required to be uploaded prospectively to a clinical trial database. However, this study was uploaded retrospectively, despite the initial intention for prospective submission. This deviation may be considered as another limitation of the current study, as it could potentially increase the risk of bias.
The results revealed that pain incidence and intensity were most evident during the first three post-operative days, significantly decreasing thereafter. By day 7, over 96% of patients reported an absence of any level of discomfort, supporting a previous research by Ahmed et al. [15] suggesting that pain reduction may be attributed to the healing of a symptomatic pulp after undergoing pulpectomy. This study confirms that even in symptomatic teeth, substantial periapical healing occurs by the seventh day following root canal therapy.
Conclusion
Occlusal reduction in both symptomatic or asymptomatic molars had no significant impact on post-operative pain following single-visit root canal treatment. However, it is important to note that occlusal reduction is not an independent determinant for the relief of post-endodontic pain.
Acknowledgement
The authors deny any conflicts of interest related to this study. Aysenur Kamacı Esen affirm that we have no financial affiliation or involvement with any commercial organisation with direct financial interest in the subject or materials discussed in this manuscript, nor have any such arrangements existed in the past 3 years. Any other potential conflict of interest is disclosed.
Declarations
Author contribution
Each author contributed to the creation of the research and approved the final manuscript. The study was designed by A.K.E. and F.F., the treatments were carried out by A.K.E., M.N.T provided patient follow-up for 1–3 days and 7 days. The paper was written by A.K.E. and F.B.B. The final revisions were made by M.P.
Ethics approval and consent to participate
Ethical committee approval was obtained from Sakarya University Faculty of Medicine Ethical Committee with the approval number of E-71522473-050.01.04-39802-329.
Participants were informed about the procedure and an informed consent form was taken from all of the participants.
References
[1] Monteiro CMC, Martins ACR, Reis A, de Geus JL. Effect of endodontic sealer on postoperative pain: a network meta-analysis. Restor Dent Endod. 2023;48(1):e5. https://doi.org/10.5395/rde.2023.48.e5
[2] Sathorn C, Parashos P, Messer H. The prevalence of postoperative pain and flare-up in single- and multiple-visit endodontic treatment: a systematic review. Int Endod J. 2008;41(2):91–9. https://doi.org/10.1111/j.1365-2591.2007.01316.x
[3] Hou XM, Su Z, Hou BX. Post endodontic pain following single-visit root canal preparation with rotary vs reciprocating instruments: a meta-analysis of randomized clinical trials. BMC Oral Health. 2017;17(1):86. https://doi.org/10.1186/s12903-017-0355-8
[4] Mostafa M, El-Shrief YAI, Anous WIO, Hassan MW, Salamah FTA, El Boghdadi RM, et al. Postoperative pain following endodontic irrigation using 1.3% versus 5.25% sodium hypochlorite in mandibular molars with necrotic pulps: a randomized double-blind clinical trial. Int Endod J. 2020;53(2):154–66. https://doi.org/10.1111/iej.13222
[5] Nguyen D, Nagendrababu V, Pulikkotil SJ, Rossi-Fedele G. Effect of occlusal reduction on postendodontic pain: a systematic review and meta-analysis of randomised clinical trials. Aust Endod J. 2020;46(2):282–94. https://doi.org/10.1111/aej.12380
[6] Pak JG, White SN. Pain prevalence and severity before, during, and after root canal treatment: a systematic review. J Endod. 2011;37(4):429–38. https://doi.org/10.1016/j.joen.2010.12.016
[7] Ng YL, Glennon JP, Setchell DJ, Gulabivala K. Prevalence of and factors affecting post-obturation pain in patients undergoing root canal treatment. Int Endod J. 2004;37(6):381–91. https://doi.org/10.1111/j.1365-2591.2004.00820.x
[8] Nagendrababu V, Gutmann JL. Factors associated with postobturation pain following single-visit nonsurgical root canal treatment: a systematic review. Quintessence Int. 2017;48(3):193–208.
[9] Aneja K, Gupta A, Abraham D, Aggarwal V, Sethi S, Chauhan P, et al. Influence of vehicle for calcium hydroxide on postoperative pain: a scoping review. J Dent Anesth Pain Med. 2022;22(2):75–86. https://doi.org/10.17245/jdapm.2022.22.2.75
[10] Mergoni G, Ganim M, Lodi G, Figini L, Gagliani M, Manfredi M. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst Rev. 2022;12(12):CD005296. https://doi.org/10.1002/14651858.CD005296.pub4
[11] Adam M, Wootton J. Conventional vs ultrasonic irrigation – which leads to less post-operative pain? Evid Based Dent. 2022;23(2):50–1. https://doi.org/10.1038/s41432-022-0274-7
[12] Siqueira JF, Jr., Rocas IN, Favieri A, Machado AG, Gahyva SM, Oliveira JC, et al. Incidence of postoperative pain after intracanal procedures based on an antimicrobial strategy. J Endod. 2002;28(6):457–60. https://doi.org/10.1097/00004770-200206000-00010
[13] Rosenberg PA, Babick PJ, Schertzer L, Leung A. The effect of occlusal reduction on pain after endodontic instrumentation. J Endod. 1998;24(7):492–6. https://doi.org/10.1016/S0099-2399(98)80054-X
[14] Emara RS, Abou El Nasr HM, El Boghdadi RM. Evaluation of postoperative pain intensity following occlusal reduction in teeth associated with symptomatic irreversible pulpitis and symptomatic apical periodontitis: a randomized clinical study. Int Endod J. 2019;52(3):288–96. https://doi.org/10.1111/iej.13012
[15] Ahmed YE, Emara RS, Sarhan SM, El Boghdadi RM, El-Bayoumi MAA, El-Far HMM, et al. Post-treatment endodontic pain following occlusal reduction in mandibular posterior teeth with symptomatic irreversible pulpitis and sensitivity to percussion: a single-centre randomized controlled trial. Int Endod J. 2020;53(9):1170–80. https://doi.org/10.1111/iej.13328
[16] Parirokh M, Rekabi AR, Ashouri R, Nakhaee N, Abbott PV, Gorjestani H. Effect of occlusal reduction on postoperative pain in teeth with irreversible pulpitis and mild tenderness to percussion. J Endod. 2013;39(1):1–5. https://doi.org/10.1016/j.joen.2012.08.008
[17] Arslan H, Seckin F, Kurklu D, Karatas E, Yanikoglu N, Capar ID. The effect of various occlusal reduction levels on postoperative pain in teeth with symptomatic apical periodontitis using computerized analysis: a prospective, randomized, double-blind study. Clin Oral Investig. 2017;21(3):857–63. https://doi.org/10.1007/s00784-016-1835-y
[18] Jostes JL, Holland GR. The effect of occlusal reduction after canal preparation on patient comfort. J Endod. 1984;10(1):34–7. https://doi.org/10.1016/S0099-2399(84)80251-4
[19] Shamszadeh S, Shirvani A, Asgary S. Does occlusal reduction reduce post-endodontic pain? A systematic review and meta-analysis. J Oral Rehabil. 2020;47(4):528–35. https://doi.org/10.1111/joor.12929
[20] Comparin D, Moreira EJL, Souza EM, De-Deus G, Arias A, Silva EJNL. Postoperative pain after endodontic retreatment using rotary or reciprocating instruments: a randomized clinical trial. J Endod. 2017;43(7):1084–8. https://doi.org/10.1016/j.joen.2017.02.010
[21] Attar S, Bowles WR, Baisden MK, Hodges JS, McClanahan SB. Evaluation of pretreatment analgesia and endodontic treatment for postoperative endodontic pain. J Endod. 2008;34(6):652–5. https://doi.org/10.1016/j.joen.2008.02.017
[22] Farzaneh S, Parirokh M, Nakhaee N, Abbott PV. Effect of two different concentrations of sodium hypochlorite on postoperative pain following single-visit root canal treatment: a triple-blind randomized clinical trial. Int Endod J. 2018;51(Suppl. 1):e2–11. https://doi.org/10.1111/iej.12749
[23] Yu YH, Kushnir L, Kohli M, Karabucak B. Comparing the incidence of postoperative pain after root canal filling with warm vertical obturation with resin-based sealer and sealer-based obturation with calcium silicate-based sealer: a prospective clinical trial. Clin Oral Investig. 2021;25(8):5033–42. https://doi.org/10.1007/s00784-021-03814-x
[24] Su Y, Wang C, Ye L. Healing rate and post-obturation pain of single- versus multiple-visit endodontic treatment for infected root canals: a systematic review. J Endod. 2011;37(2):125–32. https://doi.org/10.1016/j.joen.2010.09.005
[25] Vianna ECB, Herkrath FJ, Martins IEB, Lopes LPB, Marques AAF, Sponchiado Junior EC. Effect of occlusal adjustment on postoperative pain after root canal treatment: a randomized clinical trial. Braz Dent J. 2020;31(4):353–9. https://doi.org/10.1590/0103-6440202003248
[26] Fatima S, Kumar A, Andrabi S, Mishra SK, Tewari RK. Effect of apical third enlargement to different preparation sizes and tapers on postoperative pain and outcome of primary endodontic treatment: a prospective randomized clinical trial. J Endod. 2021;47(9):1345–51. https://doi.org/10.1016/j.joen.2021.05.010
[27] Ahmad MZ, Sadaf D, MacBain MM, Merdad KA. Effect of mode of rotation on apical extrusion of debris with four different single-file endodontic instrumentation systems: systematic review and meta-analysis. Aust Endod J. 2022;48(1):202–18. https://doi.org/10.1111/aej.12612
[28] Atav Ates A, Dumani A, Yoldas O, Unal I. Post-obturation pain following the use of carrier-based system with AH plus or iRoot SP sealers: a randomized controlled clinical trial. Clin Oral Investig. 2019;23(7):3053–61. https://doi.org/10.1007/s00784-018-2721-6
[29] Thorpe KE, Zwarenstein M, Oxman AD, Treweek S, Furberg CD, Altman DG, et al. A pragmatic-explanatory continuum indicator summary (PRECIS): a tool to help trial designers. J Clin Epidemiol. 2009;62(5):464–75. https://doi.org/10.1016/j.jclinepi.2008.12.011