LETTER
Is the risk of ischemic heart disease in women after radiotherapy for breast cancer nowadays still (linearly) associated with the mean heart dose?
Henk Struikmansa, Anna Petoukhovab, Joop H.M. Schreurc, Mirjam E. Masta and Philip M. Poortmansd,e
and Philip M. Poortmansd,e
aDepartment of Radiation Therapy, Haaglanden Medical Center, Leidschendam, The Netherlands; bDepartment of Medical Physics, Haaglanden Medical Center, Leidschendam, the Netherlands; cCardiology Department, Haaglanden Medical Center, Leidschendam, The Netherlands; dDepartment of Radiation Oncology, Iridium Netwerk, Wilrijk-Antwerp, Belgium; eAntwerp University, Wilrijk-Antwerp, Belgium
Citation: ACTA ONCOLOGICA 2024, VOL. 63, 175–178. https://doi.org/10.2340/1651-226X.2024.34751.
Copyright: © 2024 The Author(s). PPublished by MJS Publishing on behalf of Acta Oncologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, with the condition of proper attribution to the original work.
Received: 6 December 2023; Accepted: 29 February 2024; Published: 10 April 2024
CONTACT Mirjam E. Mast m.mast@haaglandenmc.nl Department of Radiation Therapy, Haaglanden Medical Center, Burgemeester Banninglaan 1, 2262BA, Leidschendam, the Netherlands
Competing interests and funding: All authors state that no actual or potential conflicts of interest exist in relation of the contents of this manuscript.
From the US-SEER cancer registries, it appeared that radiation therapy (RT), administered between 1973 and 1982, resulted in an increased mortality rate up to 10–20 years after treatment for left-sided breast cancer (BC) patients [1]. Furthermore, Darby et al. reported that major cardiac events (MCE) incidence rates increased linearly with mean heart dose (MHD) by 7.4% relative per Gray [2]. Similar results were found in two Dutch and one Danish study [3–5]. Thereafter, MHD is used as a normative planning parameter in BC-RT in daily practice as well as in studies [6–8]. Recently, though, the presence of a dose–effect relationship was not confirmed [9, 10]. Therefore, we decided to evaluate whether a linear association between MHD and MCE-incidence rates still applies and noted:
- The reported ‘relative excessive risks relative per Gy’ for these six studies varied substantially (0%–19%) [2, 3, 4, 5, 9];
- In the Darby study, analyses were based on ‘a standard patient’ and in early cases only analogue RT-charts, to estimate dose levels, were available, negatively impacting the reliability of their findings [2, 3, 5];
- RT details differed or were absent. In contrast to the older studies, in the more recent studies, the majority of patients were treated after 2000 [4, 9, 10]. Whereas after 2000, more homogeneous and conformal 3D dose calculation and delivery was feasible [11, 12];
- van den Bogaard et al. concluded that their multivariable normal tissue complication probability model, predicting the occurrence of an acute coronary event, included the 5Gy left ventricle volume, but not MHD [4];
- Age-restrictions as well as countries of residence differed, while age-standardized prevalence of coronary vascular diseases as well as death rates from ischemic heart disease for women vary substantially between European countries, impacting the correct interpretation of these studies [13–15];
- Only relative risks were provided, whereas clinical relevance is determined also by absolute figures;
- Information about tobacco use was unknown in >50% of cases [2] and not considered in two other studies [5, 9]. This is relevant since tobacco use is associated with an increased risk of developing MCEs after BC-RT [16–18]. For the combination of tobacco use and BC-RT, even a synergistically increased rate of fatal myocardial infarction was noted [16].
Subsequently, we investigated results of (more recent) phase-III trials, because its prospective design ensures that the reliability of findings of phase-III trials is not hampered by observed differences and methodological flaws. And to confirm whether the reported higher MHD values for locoregional RT, including the internal mammary chain (IMC) [11, 12, 19, 20] coincide with significantly higher MCE-incidence rates. To summarise, firstly the DBCG-82bc trial (n = 3,083), after 30-year follow-up, reported no significant excess deaths of ischemic heart disease [21]. Patients were randomized (1982–1990) between yes or no postoperative RT to the chest wall and nodal regions (including IMC). Secondly, in 2023, the meta-analysis of the ‘Early Breast Cancer Trialists’ Collaborative Group’, evaluating the role of regional lymph node irradiation (RNI) in 16 phase-III trials (n = 14,324), was reported. With 15 years of follow-up, no increased non-breast cancer-related mortality (including cardiac deaths) was noted in the eight more recent trials (n = 12,167), in which patients were treated from 1989 till 2008 [22]. Thirdly, in the EORTC 22922-10925 trial (1996–2004), 4,004 patients were randomized between irradiation of the ipsilateral IMC and ipsilateral medio-supraclavicular chain or not [23]. Special attention was given to prospectively assess incidences of late side effects. After 15.7 years, cardiac death rates were identical in both arms (1.4%). No differences were found between left-sided versus right-sided cases. While cumulative incidence rates for any heart disease after nodal RT showed a limited increase of 1.7%, no increased incidence rates of cross-sectionally registered cardiac diseases, with a score of 2 or higher (CTC-AE 2, assessed every 5 years after treatment), were seen. Moreover, a RT-planning study using a fractionation scheme of 40.05Gy/15fr and representing >75% (concerning irradiation technique) of the participants of the EORTC 10925-22922 trial, revealed that the mean of the MHD values after left-sided whole breast RT and IMC-RT, when compared to that after whole breast RT only, was 13.9 Gy higher (Figure 1A) [19].
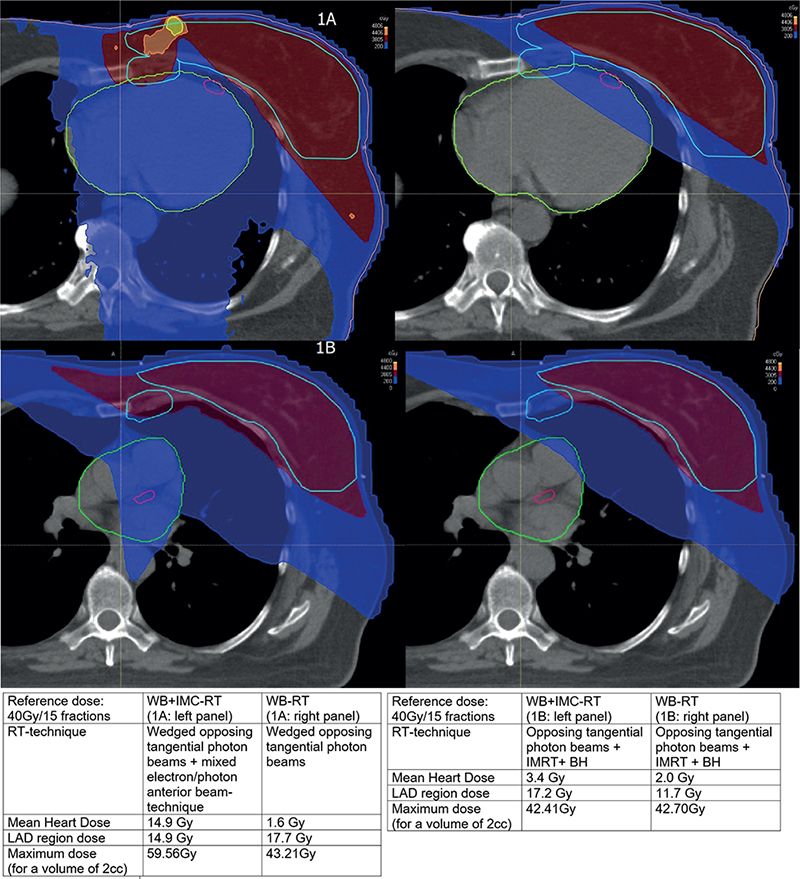
Figure 1. (A) Central plane of a left-sided RT-treatment plan in FB*. Left panel: WB**+IMC***-RT. Right panel: WB-RT. *FB: free breathing; **WB: whole breast; ***IMC: internal mammary chain. Light blue line: PTV*-GBT** and PTV-IMC. Pink line: LAD*** region. Green line: Heart (including pericardium). *PTV: planning target volume; **GBT: glandular breast tissue; ***LAD: left anterior descending coronary artery. Dark red area: 95% reference dose. Dark blue area: 5% reference dose. Orange area: 110% reference dose. Yellow area: 120% reference dose. (B) Central plane of a left-sided RT-treatment plan in BH*. Left panel: WB**+IMC***-RT. Right panel: WB-RT. *BH: breath-hold; **WB: whole breast; ***IMC: internal mammary chain. Technique: Hybrid IMRT*+BH. *IMRT: intensity modulated radiation therapy. Light blue lines: PTV*-GBT** and PTV-IMC. Pink line: LAD*** region. Green line: Heart (including pericardium). *PTV: planning target volume; **GBT: glandular breast tissue; ***LAD: left anterior descending coronary artery. Dark red area: 95% reference dose. Blue area: 5% reference dose. Orange area: 110% reference dose (not applicable). Yellow area: 120% reference dose (not applicable).
This contradicts the findings of Darby et al., predicting an increased MCE-incidence in the treatment arm of this trial of about 100% (13.9 × 7.4%) [2]. According to the results of two similar studies, even more pronounced increased MCE incidences were predicted [4, 5]. The following changes over time should be considered also, between 1970 and 2000, for women in Western Europe, an almost linear decline in death rates, ranging from 65% to 50%, for ischemic heart disease was noted [15]. After 1990, a significant lowering of heart doses in radiotherapy was achieved [11, 12]. More recently, introduction of 3D-treatment planning and, subsequently, intensity-modulated RT (IMRT) and respiratory control enabled even further improved heart sparing [19, 24] (Figure 1A+1B). Another RT-planning study (not considering IMRT), concluded that breath-hold as well as volumetric arc therapy enabled improved heart sparing after nodal RT (including IMC) [20]. After 2008, total RT-doses of 50 Gy/25 fr decreased towards 40 Gy/15 fr [25], resulting in correspondingly decreased mean heart physical doses. Furthermore, according to the results of the ‘Fast-Forward trial’, RT doses for local treatment are decreasing further towards 26Gy/5fr [26]. Radiobiological calculations, though, show that hypofractionation does not increase the probability of RT-associated MCE incidences. Finally, MHD is not a specific tool to predict the incidence of (major) atherosclerotic coronary artery disease, because the dose distribution in the heart is inhomogeneous, especially when using tangential beam-based RT techniques [10, 27].
We conclude that MHD cannot be seen as a reliable tool predicting increased MCE-incidences after BC-RT. Hence, nowadays there is no convincing evidence to support the use of MHD as a normative RT-planning parameter in daily practice nor in studies. The reliability of future findings of studies still using MHD as a normative RT planning parameter is hampered. We state that, in daily practice as well as in studies, cardiac risk assessment in BC-RT is of importance and preferably determined according to reported ‘evidence-based’ guidelines [14]. To predict radiation associated major coronary event incidence rates, we recommend evaluating the relevance of dose-volume relationships for both coronary arteries and left ventricle.
Acknowledgements
SLC Bogers, medical physicist, for providing Figure 1A and 1B. Department of Medical Physics, Haaglanden Medical Center, Leidschendam, the Netherlands.
Ethical approval
No ethical approval was requested since no own data were used.
Data availability statement
No specific data were used to compose this letter.
References
1. Darby SC, McGale P, Taylor CW, Peto R. Long-term mortality from heart disease and lung cancer after radiotherapy for early breast cancer: prospective cohort study of about 300,000 women in US SEER cancer registries. Lancet Oncol. 2005;6:557–65. https://doi.org/10.1016/S1470-2045(05)70251-5
2. Darby SC, Ewertz M, McGale P, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368:987–98. https://doi.org/10.1056/NEJMoa1209825
3. Jacobse JN, Duane FK, Boekel NB, et al. Radiation dose-response for risk of myocardial infarction in breast cancer survivors. Int J Radiat Oncol Biol Phys. 2019;103(3):595–604. https://doi.org/10.1016/j.ijrobp.2018.10.025
4. van den Bogaard VAB, Ta BDP, van der Schaaf A, et al. Validation and modification of a prediction model for acute cardiac events in patients with breast cancer treated with radiotherapy based on three-dimensional dose distributions to cardiac substructures. J Clin Oncol. 2017;35(11):1171–8. https://doi.org/10.1200/JCO.2016.69.8480
5. Lorenzen EL, Rehammar JC, Jensen MB, Ewertz M, Brink C. Radiation-induced risk of ischemic heart disease following breast cancer radiotherapy in Denmark, 1977–2005. Radiother Oncol. 2020;152:103–10. https://doi.org/10.1016/j.radonc.2020.08.007
6. Mutter RW, Choi I, Jimenez RB, et al. Proton therapy for breast cancer: a consensus statement from the particle therapy cooperative group breast cancer subcommittee. Int J Radiat Oncol Biol Phys. 2021;111(2):337–59. https://doi.org/10.1016/j.ijrobp.2021.05.110
7. National Guideline Alliance (UK). Evidence reviews for breast radiotherapy: early and locally advanced breast cancer: diagnosis and management: evidence review H [Internet]. London: National Institute for Health and Care Excellence (NICE); 2018 Jul. (NICE Guideline, No. 101.) [Cited date: 30-11-2023] Available from: https://www.ncbi.nlm.nih.gov/books/NBK576827/
8. Stick LB, Lorenzen EL, Yates ES, et al. Selection criteria for early breast cancer patients in the DBCG-proton trial – the randomised phase III trial strategy. Clin Transl Radiat Oncol. 2021;27:126–31. https://doi.org/10.1016/j.ctro.2021.01.012
9. Baaken D, Merzenich H, Schmidt M, et al. A nested case-control study on radiation dose-response for cardiac events in breast cancer patients in Germany. Breast. 2022;65:1–7. https://doi.org/10.1016/j.breast.2022.05.007
10. Holm Milo ML, Slot Møller D, Bisballe Nyeng T, et al. Radiation dose to heart and cardiac substructures and risk of coronary artery disease in early breast cancer patients: a DBCG study based on modern radiation therapy techniques. Radiother Oncol. 2023;180:109453. https://doi.org/10.1016/j.radonc.2022.109453
11. Duane FK, Boekel NB, Jacobse JN, et al. Exposure of the heart and cardiac valves in women irradiated for breast cancer 1970–2009. Clin Transl Radiat Oncol. 2022;36:132–9. https://doi.org/10.1016/j.ctro.2022.07.004
12. Taylor CW, Wang Z, Macaulay E, Jagsi R, Duane F, Darby SC. Exposure of the heart in breast cancer radiation therapy: a systematic review of heart doses published during 2003 to 2013. Rev Int J Radiat Oncol Biol Phys. 2015;93(4):845–53. https://doi.org/10.1016/j.ijrobp.2015.07.2292
13. WHO Mortality Database. Notes: Data are age-standardised to the 2013 European standard population [Internet]. Available from: [Cited date: 30-11-2023] http://apps.who.int/healthinfo/statistics/mortality/whodpms/
14. Visseren FLJ, Mach F, Smulders YM, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42(34):3227–37. https://doi.org/10.1093/eurheartj/ehab484
15. Kesteloot H, Sans S, Kromhout D. Dynamics of cardiovascular and all-cause mortality in Western and Eastern Europe between 1970 and 2000. Eur Heart J. 2006;27:107–13. https://doi.org/10.1093/eurheartj/ehi511
16. Hooning MJ, Botma A, Aleman BM, et al. Long-term risk of cardiovascular disease in 10-years survivors of breast cancer. J Natl Cancer Inst. 2007;99:365–75. https://doi.org/10.1093/jnci/djk064
17. Taylor C, Correa C, Duane FK, et al. Estimating the risks of breast cancer radiotherapy: evidence from modern radiation doses to the lungs and heart and from previous randomized trials. J Clin Oncol 2017;35(15):1641–9. https://doi.org/10.1200/JCO.2016.72.0722
18. Mehta LS, Watson KE, Barac A, et al. Cardio-vascular disease and breast cancer: where these entities intersect: a scientific statement from the American Heart Association. Circulation. 2018;137(8):e30–66. https://doi.org/10.1161/CIR.0000000000000556
19. Bogers SLC, Petoukhova AL, Penninkhof JJ, et al. Target volume coverage and organ at risk doses for left-sided whole breast irradiation with or without internal mammary chain irradiation: a comparison between 3 techniques representing the past and the present. Clin Oncol (R Coll Radiol). 2022;34(8):537–44. https://doi.org/10.1016/j.clon.2022.04.004
20. Ranger A, Dunlop A, Hutchinson K, et al. A Dosimetric comparison of breast radiotherapy techniques to treat locoregional lymph nodes including the internal mammary chain. Clin Oncol (R Coll Radiol). 2018;30(6):346–53. https://doi.org/10.1016/j.clon.2018.01.017
21. Overgaard M, Nielsen HM, Tramm T, et al. Postmastectomy radiotherapy in high-risk breast cancer patients given adjuvant systemic therapy. A 30-year long-term report from the Danish breast cancer cooperative group DBCG 82bc trial. Radiother Oncol. 2022;170:4–13. https://doi.org/10.1016/j.radonc.2022.03.008
22. EBCTCG. Radiotherapy to regional nodes in early breast cancer: an individual patient data meta-analysis of 14 324 women in 16 trials. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) Lancet. 2023;402(10416):1991–2003. https://doi.org/10.1016/S0140-6736(23)01082-6
23. Poortmans PM, Struikmans H, de Brouwer P, et al. Side effects 15-years after lymph node irradiation in breast cancer: randomized EORTC Trial 22922/10925. J Natl Cancer Inst. 2021;113(10):1360–8. https://doi.org/10.1093/jnci/djab113
24. Mast ME, van Kempen-Harteveld L, et al. Left-sided breast cancer radiotherapy with and without breath-hold: does IMRT reduce the cardiac dose even further? Radiother Oncol. 2013;108(2):248–53. https://doi.org/10.1016/j.radonc.2013.07.017
25. Bentzen SM, Agrawal RK, Aird EG, et al. The UK standardisation of breast radiotherapy (START) trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet. 2008;371(9618):1098–107. https://doi.org/10.1016/S0140-6736(08)60348-7
26. Brunt AM, Haviland JS, Wheatley DA, et al. Hypofractionated breast radiotherapy for 1 week versus 3 weeks (FAST-Forward): 5-year efficacy and late normal tissue effects results from a multicentre, non-inferiority, randomised, phase 3 trial. Lancet. 2020;395(10237):1613–26. https://doi.org/10.1016/S0140-6736(20)30932-6
27. Taylor CW, Povall JM, McGale P, et al. Cardiac dose from tangential breast cancer radiotherapy in the year 2006. Int J Radiat Oncol Biol Phys. 2008;72:501–7. https://doi.org/10.1016/j.ijrobp.2007.12.058