REVIEW ARTICLE
Gastric cancer causing Schnitzler’s metastasis: case report and systematic review of the features
Huimin Xue, MDa, Xiaomei Yang, MDa, Qing Shen, MDa, Jinglei Qu, PhDa,b,c,d, Xiujuan Qu, PhDa,b,c,d* and Ying Chen, PhDa,b,c,d*
and Ying Chen, PhDa,b,c,d*
aDepartment of Medical Oncology, The First Hospital of China Medical University, Shenyang, People’s Republic of China; bKey Laboratory of Anticancer Drugs and Biotherapy of Liaoning Province, The First Hospital of China Medical University, Shenyang, People’s Republic of China; cLiaoning Province Clinical Research Center for Cancer, Shenyang, People’s Republic of China; dKey Laboratory of Precision Diagnosis and Treatment of Gastrointestinal Tumors, Ministry of Education, The First Hospital of China Medical University, Shenyang, People’s Republic of China
ABSTRACT
Background: Rectal metastasis from gastric cancer (GC), also known as Schnitzler’s metastasis, is a rare phenomenon. The clinicopathological characteristics, outcomes, and prognostic factors of this condition remain poorly understood.
Methods: We describe a case of GC causing Schnitzler’s metastasis and present a systematic review on case reports and case series. Data extracted and analyzed include clinicopathological features, treatment modalities received, outcomes, and follow-up.
Results: A total of 34 records, including our own, encompassing 41 cases were incorporated into the study. The median age of patients at admission was 59 years, with females accounting for 53.7% of cases. The predominant histological subtype of Schnitzler’s metastasis was moderate-to-poorly differentiated adenocarcinoma, representing 31 cases (86.1%). Among the patients in this cohort, 38.9% exhibited signet-ring cell carcinoma. Regarding the initial diagnosis of GC, 28.6% were categorized as stage IIIA, and 28.6% were classified as stage IV. The median overall survival (OS) time was 72 months (95% confidence interval [CI]: 27-NA), while the median OS since the diagnosis of metastatic cancer was 16 months (95% CI: 9-NA).
Interpretation: Schnitzler’s metastasis presents a challenge in the pathology of colorectal endoscopy and may lead to treatment delays. Imaging features such as increased thickness of the intestinal wall and significant layered enhancement can aid in diagnosis; however, deep core biopsy of intestinal lesions remains the gold standard for diagnosing rectal metastases. Accurately distinguishing rectal metastases from primary rectal cancer is crucial for preventing unnecessary therapeutic interventions.
KEYWORDS Schnitzler’s metastasis; rectal metastasis from gastric cancer; clinicopathological characteristics; case report; systematic review
Citation: ACTA ONCOLOGICA 2025, VOL. 64, 312–318. https://doi.org/10.2340/1651-226X.2025.41296.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Oncologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Received: 6 August 2024; Accepted: 31 January 2025; Published: 26 February 2025
CONTACT Ying Chen and Xiujuan Qu dongyechenying@126.com; xjqu@cmu.edu.cn Department of Medical Oncology, The First Hospital of China Medical University, Shenyang, 110001, People’s Republic of China
*These authors contributed equally to this work.
Competing interests and funding: The authors declare that they have no competing interests.
The authors declare that no funds, grants, or other support was received during the preparation of this manuscript.
Introduction
Globally, gastric cancer (GC) is the fifth most common cancer and the fourth leading cause of cancer death, accounting for 7.7% of cancer fatalities [1]. After radical resection of GC, it commonly spreads through lymphatic, peritoneal, hematogenous routes, or local recurrence, often affecting the liver, lung, bone, lymph nodes, and brain. Rectal metastasis, termed Schnitzler’s metastasis, is exceedingly rare. Given the unique site of metastasis, distinguishing between GC intestinal metastasis and primary colorectal cancer poses a clinical challenge.
Rectal metastasis presents symptoms similar to primary rectal cancer, such as abdominal pain, ascites, constipation, diarrhea, and severe cases of bowel obstruction and bleeding, leading to reduced quality of life and poor treatment outcomes [2]. Diagnosis primarily involves digital rectal examination, colonoscopy, and endoscopic ultrasonography (EUS), with computed tomography (CT) and fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) scans essential for identifying metastases. Biopsies can be challenging, often requiring deep tissue samples to confirm malignancy.
This article reviews global case reports and series on Schnitzler’s metastasis, focusing on its clinical presentation, imaging, histopathology, treatment, and prognosis. It aims to improve clinical understanding and management of rectal metastases from GC by consolidating existing knowledge.
Methods
We present a case of rectal metastasis from GC treated at our institution and conducted a systematic review of case reports and series on GC causing Schnitzler’s metastasis. The search strategies apply the following terms: ‘Stomach Neoplasms’ (Mesh term), ‘Rectum’ (Mesh term), ‘Neoplasm Metastasis’ (Mesh term), ‘Stomach Carcinoma’ (free text), ‘Stomach Cancer’ (free text), ‘Stomach Neoplasm’ (free text), ‘rectum’ (free text), and ‘Metastasis’ (free text). These terms were combined using ‘AND’ and ‘OR’. The databases ‘PubMed’ (https://pubmed.ncbi.nlm.nih.gov/), ‘Embase’ (https://www.embase.com/), ‘CNKI’ (https://www.cnki.net/), and ‘Cochrane’ (https://www.cochrane.org/) were thoroughly reviewed.
On November 13, 2023, investigators HX and XY independently reviewed relevant articles, resolving discrepancies through discussion. Studies were excluded if off-topic, duplicates, lacking full text, or insufficient clinical data, and references were checked to avoid omissions. Figure 3 illustrates the selection process per PRISMA guidelines [3]. As all articles were case reports, no risk bias assessment tool was used. Extracted data included authorship, publication year, patient demographics, clinical details, and outcomes, which were then synthesized and analyzed.
Statistical analysis
Descriptive data were presented as median (interquartile range) or number and percentages. The overall survival (OS) was measured from the date of primary GC diagnosis to the date of death, while survival subsequent to rectal metastasis was calculated from the date of metastasis diagnosis to the date of death. Survival data were analyzed using the Kaplan–Meier method. Statistical analyses were performed using R software (Version 4.3.3; The R Foundation for Statistical Computing, Vienna, Austria).
Results
Case report
In December 2019, a 39-year-old woman was diagnosed with stage IIA GC (T3N0M0) and human epidermal growth factor receptor 2 (HER-2) negative. She had a total gastrectomy, six cycles of S-1 and oxaliplatin (SOX) chemotherapy, and one cycle of tegafur gimeracil and oteracil potassium capsules (S-1) monotherapy. By June 2021, she reported defecation difficulties, decreased stool caliber, and increased bowel movement frequency.
A follow-up enhanced abdominal CT scan revealed rectal wall thickening and circumferential enhancement (Figure 1a). An FDG PET/CT scan showed increased metabolic activity in the rectum, with a standardized uptake value (SUV) of 11.5 (Figure 2). A colonoscopy at another hospital found irregular, friable mucosa prone to bleeding from 4 to 10 cm from the anal verge. A superficial biopsy indicated nonspecific chronic inflammation (Figure 1d). Intraluminal ultrasonography confirmed a thickened rectal wall, narrowed lumen, and increased blood flow (Figure 1c). An ultrasonography-guided core needle biopsy using an 18G coaxial cutting needle diagnosed poorly differentiated adenocarcinoma from the stomach (Figure 1e). So, the patient was diagnosed with Schnitzler’s metastasis.
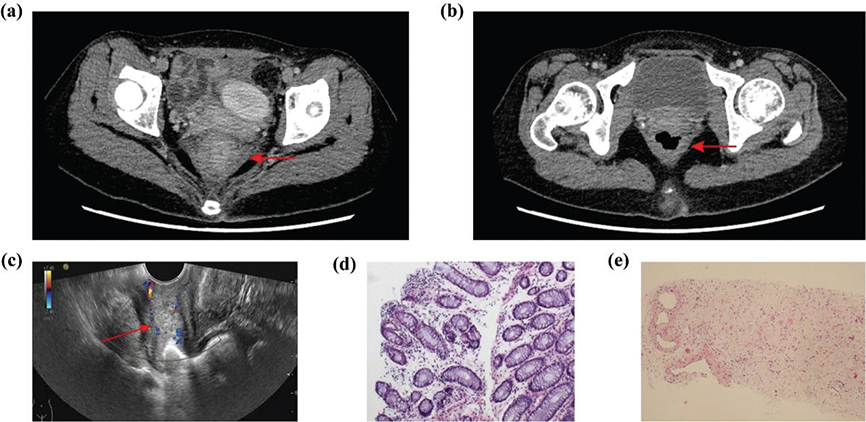
Figure 1. (a) Enhanced abdominal CT scan on Jun. 2021 showed thickening and circumferential enhancement of the rectal wall (red arrow). (b) Enhanced abdominal CT scan after treatment on Dec. 2021. (c) Endorectal EUS showed a thickened rectal wall, narrowing of the intestinal lumen, and increased blood flow in the thickened wall (red arrow). (d) Superficial biopsy from colonoscopy revealed nonspecific chronic inflammatory changes. (e) Deep puncture biopsy from endorectal EUS showed poorly differentiated adenocarcinoma originating from stomach (hematoxylin and eosin stain). CT, Computed Tomography; EUS, Endoscopic Ultrasound.
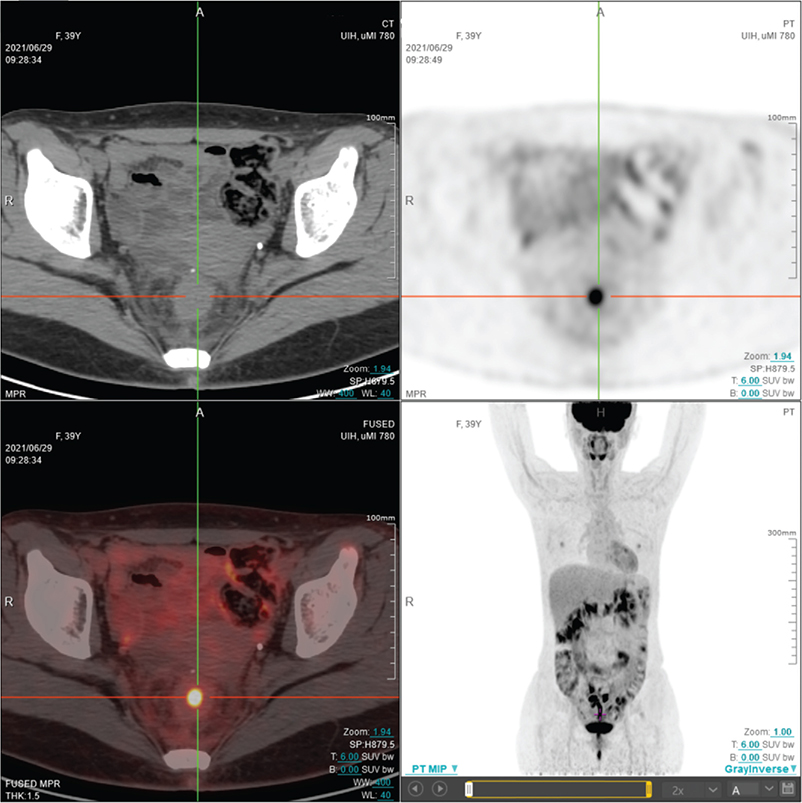
Figure 2. FDG-PET showed hypermetabolism in the middle section of rectum on Jun. 2021. FDG: F-18-fluoro-deoxy-glucose; PET: positron emission tomography.
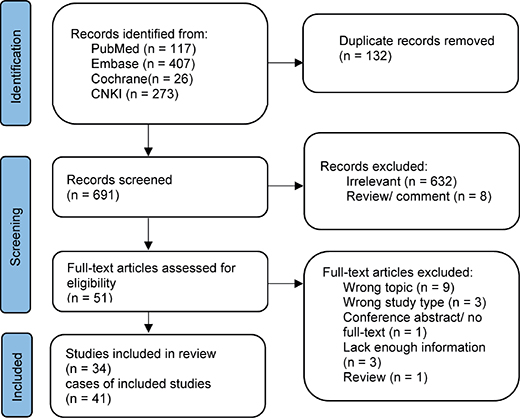
Figure 3. Flowchart of the selection process according to PRISMA statement.
Immunohistochemistry showed C-erbB-2(2+), while fluorescence in situ hybridization (FISH)-HER-2 was negative. The patient received chemotherapy with apatinib and albumin-bound paclitaxel from August 2021 to June 2022, maintaining stable disease. In July 2022, disease progression occurred, prompting 27 cycles of disitamab vedotin for rectal metastasis with HER-2 2+ status. Apatinib was added in December 2022 for combined therapy. As of October 2023, no tumor recurrence was detected. This study complies with CARE guidelines, and the patient consented to the case report [4].
Literature review
A total of 41 cases were included in this review, combining 40 from the literature with our case (Figure 3) [5–37]. The median participant age was 59 years, with 46.3% male and 53.7% female. Geographically, cases came from Japan (36.6%), China (31.7%), the USA (17.1%), Turkey (7.3%), and one each from Germany, Italy, and South Korea. Most cases involved moderate-to-poorly differentiated adenocarcinoma (86.1%), with 38.9% being signet-ring cell carcinoma and 36.1% poorly differentiated adenocarcinoma. Highly differentiated adenocarcinoma appeared in only 2.8% of cases. Initial GC diagnoses were stage IIIA or IV in 28.6% of cases each. Among the 29 cases that specified the number of metastatic sites, nine cases (31.0%) presented with metastasis at a single site at the time of diagnosis, while 20 cases (69.0%) reported metastases other than rectum metastases. Synchronous metastases accounted for 16 cases (40.0%), while metachronous metastases were observed in 24 cases (60.0%) (Table 1). The predominant symptoms associated with Schnitzler’s metastasis included mechanical bowel obstruction, manifested as abdominal mass, distension, discomfort, and/or pain (57.5%), followed by constipation (52.5%), rectal discharge or hematochezia (17.5%), and nausea, dyspepsia, or vomiting (10.0%). The median distance of the rectal mass from the anal verge was 4 cm. Diagnostic modalities included endoscopy in 80.5% of cases, EUS in 7.3%, CT scan in 70.7%, and magnetic resonance imaging in 22.0%. PET/CT scan was utilized in 17.1% of cases (Table 2). For primary stomach cancer, the most common treatment was surgery alone (61.1%), followed by chemotherapy (25.0%), surgery with chemotherapy (11.1%), and surgery with chemoradiation (2.8%). The treatment modalities for rectal metastasis include surgery alone (46.9%), chemotherapy (25.0%), a combination of surgery and chemotherapy (25.0%), and a combination of chemotherapy and targeted therapy (2.8%). As for outcomes, 60.9% of patients were alive, while 39.1% succumbed to the disease with a median follow-up of 9 months (interquartile range, 5–20) after Schnitzler’s metastasis. The median OS of patients was 72 months (95% confidence interval [CI]: 27-NA), and the survival time after the diagnosis of metastatic cancer was 16 months (95% CI: 9-NA) (Figure 4, Table 3).
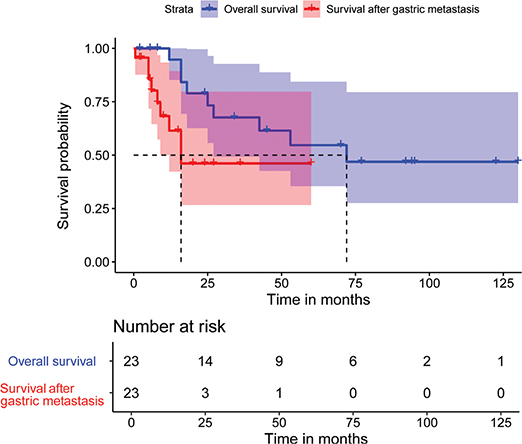
Figure 4. Kaplan–Meier curves for overall survival time and survival time after GC Schnitzler’s metastasis. The median OS of patients was 72 months (95% CI: 27-NA), and the survival time after the diagnosis of Schnitzler’s metastatic cancer was 16 months (95% CI: 9-NA). GC, gastric cancer.
Discussion
Rectal metastasis from GC, also known as Schnitzler’s metastasis, is underrepresented in medical literature, leading to potential oversight in clinical practice. Giri et al. reported a case of pancreatic carcinoma causing Schnitzler’s metastasis [38], expanding the definition of Schnitzler’s metastasis. Considering the diagnostic and therapeutic challenges, we described a case of rectum metastasis from gastric adenocarcinoma, which was confirmed by CT, PET-CT, endoscopy, EUS, tissue biopsy, and immunohistochemistry. Additionally, 41 cases were systematically analyzed to elucidate their clinical characteristics.
Schnitzler’s metastasis is primarily reported in Japan and China due to high rates of gastrointestinal tumors in East Asia. It is more common in females, with our study showing 53.7% female patients. Primary GC often involves moderate-to-poorly differentiated adenocarcinoma, with 70% of our cases having poorly differentiated tumor cells and 30% having signet-ring cells. Additionally, 69% of patients had multiple metastases, likely due to advanced primary GC. Rectal metastases can occur at initial diagnosis or during recurrence, with 40% synchronous and 60% heterochronous cases in our study.
The precise mechanism underlying Schnitzler’s metastasis remains unclear. Detecting tumor cells in rectal biopsies is challenging, possibly due to the spread of gastric adenocarcinoma through rectal submucosa veins and lymphatics, and the sparse tumor cell distribution in gastric impression cell carcinoma [5]. Additionally, intestinal wall thickening might result from fibrous tissue and inflammatory cell accumulation due to lymphatic obstruction by cancer cells causing edema, rather than direct tumor cell infiltration [18]. Peritoneal dissemination, where cancer cells accumulate in the uterorectal or vesicorectal crypts leading to implantation metastasis, is another possible explanation [37]. The ‘dormancy’ theory suggests that malignant cells spread early, remain inactive in distant organs, and reactivate under stress, explaining the long latency between initial cancer and distant metastasis.
Distinguishing between recurrent intestinal metastases and primary colorectal cancer post-stomach resection is difficult due to overlapping symptoms like abdominal pain and bowel issues. Tang et al. described a case misdiagnosed as rectal cancer, resulting in unnecessary radiation therapy [32]. Our study found rectal stenosis blocking fecal passage due to metastasis, along with changes in bowel habits.
Diagnosis
Digital rectal examination is crucial for detecting rectal issues, with palpation revealing severe stenosis 5–6 cm from the dentate line [7]. Colonoscopy, performed in 80.5% of cases, typically shows diffuse wall thickening [39]. The median mass distance from the anal verge is 4 cm. EUS is recommended for a detailed view of rectal layers, detecting tumor infiltration even with normal mucosa [40].
CT imaging typically reveals thickening and circumferential enhancement of the bowel wall, often characterized by homogeneous thickening and stratified enhancement [41]. The abnormal thickening of the bowel wall has been attributed to the infiltration of cancer cells into the mesenchyme and the subsequent formation of fibrous tissue within the bowel wall. However, the limited resolution of CT precludes differentiation of the individual layers of the bowel wall. FDG PET/CT is vital for detecting recurrent metastases after GC surgery and staging advanced cases, often identifying lesions missed by other imaging methods [42]. Lim et al. and Dogan et al. highlighted cases of rectal hypermetabolism with SUVs of 7.6 and 5.8, respectively [7, 10]. In our case, we noted diffuse FDG uptake in the recto-anal area with a maximum SUV of 11.4. The use of FDG PET/CT for Schnitzler’s metastases could provide insights into intestinal obstruction after radical gastrectomy for GC, aiding treatment strategies.
The diagnosis of submucosal lesions through endoscopic mucosal biopsy can be challenging, with some studies confirming diagnoses via surgical pathology [5, 18, 22]. We recommend intraluminal ultrasound-guided deep biopsy as it facilitates the diagnosis of submucosal lesions while minimizing tissue damage. Imaging showed rectal wall thickening, and difficulty in tumor cell identification on biopsy should raise suspicion of Schnitzler metastasis. A detailed patient history and further investigations, including FDG PET/CT and deep biopsies, are essential to determine the lesion’s nature.
Treatment
The management of Schnitzler’s metastasis should consider factors such as location, extent, histological type, and primary tumor stage. Patients with colonic metastases occurring 5 years after aggressive GC surgery, who underwent surgical intervention, showed an average survival of 26 months [17]. Decompression therapy, such as colostomy or colonic stent placement, is commonly used for the prevention and management of intestinal obstruction resulting from metastatic colonic stenosis [21]. Presently, the use of S-1 predominates in most cases, possibly due to its widespread use in Japan, where GC cases are more prevalent. Targeted therapies and immunotherapy for metastatic GC have received increased attention in recent years [43]. However, results of targeted and immunological tests were not mentioned due to early case inclusion and incomplete data. It is recommended to improve microsatellite and HER-2 indicators to guide further treatment.
Survival
Larger-scale clinical studies reporting overall 5-year survival rates for Schnitzler’s metastasis are still lacking [32]; however, our study revealed a median survival time of 16 months (95% CI: 9-NA), following diagnosis of metastatic cancer. Rectal metastasis manifests with various symptoms, significantly affecting the physical and psychological well-being of patients. Therefore, we believe that the prognosis of patients with Schnitzler’s metastasis is characterized by decreased OS rates and reduced quality of life. Regular follow-up is crucial in managing patients with rectal metastases from GC, and it facilitates the early detection of tumor recurrence, metastasis, or any treatment-related complications. Research should also aim to identify biomarkers for early screening, diagnosis, and prognosis.
Limitations
Our review relies upon case series or case reports, thus entailing a substantial risk for systematic biases. Furthermore, the small sample size is a limitation inherent to case reports.
Conclusions
In conclusion, Schnitzler’s metastasis is uncommon, and its identification via colonoscopy pathology poses challenges, potentially leading to treatment delays. Imaging features, such as concentric thickening of the intestinal wall with notable layered enhancement, can aid in diagnosis. Nonetheless, deep puncture biopsy of bowel lesions remains the diagnostic gold standard for rectal metastases, particularly in patients with symptoms of mechanical bowel obstruction. Accurate differentiation between rectal metastasis and primary rectal cancer is imperative to prevent unnecessary therapeutic interventions.
Statements and declarations
Author contributions
H.X. contributed to collecting the data and drafting the manuscript; X.Y. and Q.S. contributed to interpretation and writing the paper; J.Q. contributed to pathologic review; Y.C. and X.Q. helped design and revise the manuscript.
Data availability statement
Available upon request to the corresponding author.
Ethics statement
Informed consent was obtained from the patient and her husband.
References
[1] Thrift AP, Wenker TN, El-Serag HB. Global burden of gastric cancer: epidemiological trends, risk factors, screening and prevention. Nat Rev Clin Oncol. 2023;20:338–49. https://doi.org/10.1038/s41571-023-00747-0
[2] Janjic O, Labgaa I, Hübner M, Demartines N, Joliat GR. Metastasis to the rectum: a systematic review of the literature. Eur J Surg Oncol. 2022;48:822–33. https://doi.org/10.1016/j.ejso.2021.10.004
[3] Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. https://doi.org/10.1136/bmj.b2700
[4] Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D. The CARE guidelines: consensus-based clinical case reporting guideline development. Glob Adv Health Med. 2013;2:38–43. https://doi.org/10.7453/gahmj.2013.008
[5] Olano C, De Simone F, Gonzalez F, Gonzalez N, Tchekmedyian A, Pose A, et al. Stomach cancer presenting with rectal stenosis: Schnitzler’s metastasis. Gastrointest Endosc. 2009;70:809–10. https://doi.org/10.1016/j.gie.2009.01.031
[6] Derici ZS, Sokmen S. Gastric carcinoma presenting with severe rectal stenosis: ‘Schnitzler’s metastasis’: case report and review of the literature. Eur Surg. 2016;48:246–9. https://doi.org/10.1007/s10353-016-0390-8
[7] Doğan S, Demirbaş S, Samadov E, Öziş SE, Uslu HY. Rectal resection for Schnitzler’s metastasis in a patient presenting with severe rectal stenosis: case report and review of the literature. Eur Res J. 2019;5:196–201. https://doi.org/10.18621/eurj.378526
[8] Yamagishi H, Ueda Y, Oka T. A case report of immunotherapy on a patient with advanced gastric cancer by adoptive transfer of OK-432-reactive HLA-matched allogeneic lymphocytes. Cancer Immunol Immunother. 1998;46:113–19. https://doi.org/10.1007/s002620050469
[9] Hamada Y, Tanaka K, Katsurahara M, Baba Y. Solitary rectal metastasis from primary gastric cancer. Intern Med. 2019;58:1037–8. https://doi.org/10.2169/internalmedicine.1902-18
[10] Lim SW, Huh JW, Kim YJ, Kim HR. Laparoscopic low anterior resection for hematogenous rectal metastasis from gastric adenocarcinoma: a case report. World J Surg Oncol. 2011;9:148. https://doi.org/10.1186/1477-7819-9-148
[11] Aoki M, Fukunari H, Kawai Y, Watanabe A, Umebayashi Y, Saito T, et al. Two cases of surgical treatment for disseminated gastric carcinoma. Gan To Kagaku Ryoho. 2018;45:2378–80.
[12] Udagawa M, Mizuno Y, Ohnishi I, Sugishita T, Kakuta S, Murase Y, et al. A case report of gastric cancer with positive peritoneal lavage cytology and metachronous Schnitzler’s metastasis treated with multimodality therapy. Gan To Kagaku Ryoho. 2017;44:1626–8.
[13] Makker J, Karki N, Sapkota B, Niazi M, Remy P. Rare presentation of gastroesophageal carcinoma with rectal metastasis: a case report. Am J Case Rep. 2016;17:611–15. https://doi.org/10.12659/AJCR.898534
[14] Man-I M, Tsujinaka T, Nishisho I, Mishima H. A case of metastatic diffuse infiltrative carcinoma of the colon and rectum from gastric cancer 7 years after curative resection. Nippon Daicho Komonbyo Gakkai Zasshi. 2001;54:335–41. https://doi.org/10.3862/jcoloproctology.54.335
[15] Matsutani T, Sasajima K, Amano H, Egam K, Kan H, Miyashita M, et al. A case of expandable metallic stent placement for the stenosis in the sigmoid colon and rectum due to Schnitzler’s metastasis from gastric cancer. Gastroenterol Endosc. 2005;47:343–7.
[16] Nishikawa K, Matsuda C, Kawada J, Fujitani K, Endo S, Hirao M, et al. A case of rectal metastasis of gastric cancer associated with dermatomyositis. Gan To Kagaku Ryoho. 2016;43:2401–3.
[17] Noji T, Yamamura Y, Muto J, Kuroda A, Koinuma J, Yoshioka T, et al. Surgical resection of colorectal recurrence of gastric cancer more than 5 years after primary resection. Int J Surg Case Rep. 2014;5:954–7. https://doi.org/10.1016/j.ijscr.2014.10.005
[18] Rausei S, Frattini F, Dionigi G, Boni L, Rovera F, Diurni M. Unusual rectal stenosis. J Surg Oncol. 2010;102:713. https://doi.org/10.1002/jso.21632
[19] Sai K, Aomatsu N, Sakano Y, Okada T, Yonemitsu K, Fukui Y, et al. A case of advanced gastric cancer-recurrence of skin metastasis nine years after surgery and rectal stenosis due to peritoneal dissemination ten years later. Gan To Kagaku Ryoho. 2021;48:1865–7.
[20] Scheid JE, Crile G, Jr. Metastasis of carcinoma of the stomach to the submucosa of the rectum. Am J Surg. 1952;83:827–9. https://doi.org/10.1016/0002-9610(52)90191-8
[21] Okugawa T, Oshima T, Ikeo K, Kondo T, Tomita T, Fukui H, et al. Successful self-expandable metallic stent placement for a case of distal rectal stenosis due to gastric cancer metastasis. Case Rep Gastroenterol. 2013;7:214–18. https://doi.org/10.1159/000351818
[22] Tariq T, Turk A, Reaume M, Muddasani A, Parmar M. Blocked by a ring: a case of gastric linitis plastica presenting as large bowel obstruction secondary to rectal stenosis. ACG Case Rep J. 2019;6:1–3. https://doi.org/10.14309/crj.0000000000000007
[23] Tabata T, Fujimura M, Sato I, Masuda S, Chino Y, Okita A, et al. A case of rectal metastasis from gastric cancer with rectal perforation. Jpn J Gastroenterol Surg. 2010;43:710–16. https://doi.org/10.5833/jjgs.43.710
[24] Takahashi M, Kurosawa H, Masui H, Fukushima T, Mogaki M, Nagahori K. A case of diffuse invasive metastatic carcinoma of the rectum occurred 5.5 years after resection for gastric cancer. Nihon Rinsho Geka Gakkai Zasshi. 2009;70:3616–22. https://doi.org/10.3919/jjsa.70.3616
[25] Tural D, Selçukbiricik F, Erçalişkan A, Inanç B, Günver F, Büyükünal E. Metachronous rectum metastases from gastric adenocarcinoma: a case report. Case Rep Med. 2012;2012:1–4. https://doi.org/10.1155/2012/726841
[26] Uemura N, Kurashige J, Kosumi K, Iwatsuki M, Yamashita K, Iwagami S, et al. Early gastric cancer metastasizing to the rectum, possibly via a hematogenous route: a case report and review of literature. Surg Case Rep. 2016;2:58. https://doi.org/10.1186/s40792-016-0180-3
[27] Watanabe Y, Iwamoto R, Kitagawa S, Kinoshita S, Ueno M, Mineta S, et al. A resected case of rectal metastasis from gastric cancer. Gan To Kagaku Ryoho. 2019;46:2378–9.
[28] Wada Y, Okada K, Ebisui C, Yanagisawa T, Okamura S, Fukuchi N, et al. A case of long-term survival of advanced gastric cancer with Schnitzler metastasis effectively treated with combination chemotherapy. Jpn J Cancer Chemother. 2014;41:2411–13.
[29] Yamamoto M, Matsuyama A, Kameyama T, Okamoto M, Okazaki J, Utsunomiya T, et al. A case of advanced gastric cancer with Schnitzler’s metastases effectively treated by the combination of paclitaxel and S-1. Gan To Kagaku Ryoho. 2008;35:829–31.
[30] He ZC, He YC, Zhu BL, Luo JH, Wang XR, Zhou HJ, et al. Rectal metastasis of gastric cancer: report of 3 cases. J. Xiangnan Univ. 2015;17:42–4.
[31] Xu S, Zhao J, Kang L, Zhou RM, Shi XM, Zhao WH, et al. Gastric signet ring cell metastasis in colorectal carcinoma, 2 cases of misdiagnosis and literature review. Oncology Prog J. 2021;19:1833–5.
[32] Tang L, Li H, Lv J, Fang C, Zhang H, Meng J. Rectal metastasis of gastric cancer: a case report. J Int Med Res. 2023;51:1–7. https://doi.org/10.1177/03000605231198407
[33] Bolliet M, Green M, Damadi A. Gastric adenocarcinoma metastasis to the rectum causing complete obstruction, a case report. J Surg Case Rep. 2023;10:1–3. https://doi.org/10.1093/jscr/rjad560
[34] Yu X, Zhang J. Gastric cancer with large bowel obstruction as the first presentation: a case report. Oncol Lett. 2013;6:1377–9. https://doi.org/10.3892/ol.2013.1540
[35] Zhu L. Synchronous rectal metastases from gastric adenocarcinoma: a case. M.S. thesis, Zhejiang University; 2010.
[36] Dong C, Wang Z, Hu ZL, Xing YN. Schnitzler metastasis of gastric cancer to the rectum: a case report and literature review. J China Med Univ. 2023;52:461–4.
[37] Chen JH, Zou W, Su SB. Rectal metastasis of gastric signet ring cell carcinoma: report of 3 cases and review of literature. Chin J Gastroenterol. 2022;27:509–12.
[38] Giri LB, Sunil J, Stephen N, Shaikh O, Balasubramanian G. Pancreatic carcinoma causing Schnitzler’s metastasis. Cureus. 2023;15:e42465. https://doi.org/10.7759/cureus.42465
[39] Galanopoulos M, Gkeros F, Liatsos C, Pontas C, Papaefthymiou A, Viazis N, et al. Secondary metastatic lesions to colon and rectum. Ann Gastroenterol. 2018;31:282–7. https://doi.org/10.20524/aog.2018.0244
[40] Keogh CF, Brown JA, Phang PT. Linitis plastica of the rectum: utility of transrectal ultrasonography. J Ultrasound Med. 2002;21:103–6. https://doi.org/10.7863/jum.2002.21.1.103
[41] Jang H-J, Lim HK, Kim HS, Cho EY, Lee SJ, Kim KA, et al. Intestinal metastases from gastric adenocarcinoma: helical CT findings. J Comput Assist Tomogr. 2001;25:61–7. https://doi.org/10.1097/00004728-200101000-00011
[42] Findlay JM, Antonowicz S, Segaran A, El Kafsi J, Zhang A, Bradley KM, et al. Routinely staging gastric cancer with (18)F-FDG PET-CT detects additional metastases and predicts early recurrence and death after surgery. Eur Radiol. 2019;29:2490–8. https://doi.org/10.1007/s00330-018-5904-2
[43] Sexton RE, Al Hallak MN, Diab M, Azmi AS. Gastric cancer: a comprehensive review of current and future treatment strategies. Cancer Metastasis Rev. 2020;39:1179–203. https://doi.org/10.1007/s10555-020-09925-3