SHORT REPORT
Work ability following breast cancer – the MyHealth randomized controlled trial
Trine A. Horsbøla,b , Lena Saltbækb,c, Caroline Urhammerb, Randi V. Karlsenb, Christoffer Johansenb,d,e,f, Pernille E. Bidstrupf,g, Beverley L. Høegf, Vibeke Zoffmannh, Federica Belmontei, Ingelise Andersenj, Anne S. Fribergb, Mads N. Svendsenc, Helle G. Christensenc, Vesna Glavicicc, Dorte L. Nielsend,k and Susanne O. Daltonb,c,d
, Lena Saltbækb,c, Caroline Urhammerb, Randi V. Karlsenb, Christoffer Johansenb,d,e,f, Pernille E. Bidstrupf,g, Beverley L. Høegf, Vibeke Zoffmannh, Federica Belmontei, Ingelise Andersenj, Anne S. Fribergb, Mads N. Svendsenc, Helle G. Christensenc, Vesna Glavicicc, Dorte L. Nielsend,k and Susanne O. Daltonb,c,d
aNational Institute of Public Health, University of Southern Denmark, Copenhagen, Denmark; bCancer Survivorship, Danish Cancer Institute, Copenhagen, Denmark; cDepartment of Clinical Oncology and Palliative Care, Zealand University Hospital, Denmark; dInstitute of Clinical Medicine, Faculty of Health, Copenhagen University, Copenhagen, Denmark; eDepartment of Oncology, CASTLE, Copenhagen University Hospital, Copenhagen, Denmark; fPsychological Aspects of Cancer, Cancer Survivorship, Danish Cancer Institute, Copenhagen, Denmark; gInstitute of Psychology, Faculty of Social Sciences, Copenhagen University, Copenhagen, Denmark; hResearch Unit of Women’s and Children’s Health, the Juliane Marie Center, Copenhagen University Hospital, Copenhagen, Denmark; iStatistics and Data Analysis, Danish Cancer Institute, Copenhagen, Denmark; jSection of Social Medicine, Department of Public Health, Faculty of Health and Medical Sciences, University of Copenhagen, Denmark; kDepartment of Oncology, Herlev and Gentofte University Hospital, Herlev, Denmark
ABSTRACT
Background and purpose: We previously demonstrated positive effects on quality of life and mental health following breast cancer when comparing a nurse-led follow-up program without scheduled visits (MyHealth) to regular follow-up. This study aims to examine whether MyHealth also positively impacts self-reported work ability.
Patients/material and methods: A total of 288 patients, potentially active on the labour market, were randomized to MyHealth or control follow-up after primary treatment for early-stage breast cancer (2017–2019). MyHealth included individual self-management sessions, electronic symptom monitoring, and assistance with navigating healthcare services. Control follow-up consisted of biannual outpatient visits with a physician. Linear mixed-effect models were applied to evaluate the effect of MyHealth on self-reported work ability at 6, 12, 24, and 36 months after randomization as measured by the Work Ability Score (WAS).
Results: Work ability increased significantly in both groups during the first 6 months (mean WAS increase MyHealth: 1.64, 95% confidence interval [CI]: 1.26; 2.02 and control: 1.57, 95% CI: 1.17; 1.97) and continued to increase slightly but non-significantly (p-values > 0.13) until end of follow-up at 36 months. Improvement was especially pronounced among patients reporting poor work ability at baseline. Differences in mean WAS between patients in MyHealth and control follow-up were non-significant and close to zero at all time points (–0.21 to 0.48).
Interpretation: The MyHealth follow-up program had no additional effect on self-reported work ability compared to regular follow-up. Future interventions should target patients with poor work ability and include components specifically designed to enhance work ability.
KEYWORDS: Randomized controlled trial; work ability; breast cancer
Citation: ACTA ONCOLOGICA 2025, VOL. 64, 34–39. https://doi.org/10.2340/1651-226X.2025.42221.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Oncologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Received: 13 October 2024; Accepted: 13 December 2024; Published: 8 January 2025
CONTACT Trine Allerslev Horsbøl tria@sdu.dk National Institute of Public Health, University of Southern Denmark, Copenhagen, Denmark
Competing interests and funding: The authors report that there are no competing interests to declare.
Introduction
In Nordic countries, 21,640 women are diagnosed with breast cancer yearly, with almost half being 25–64 of age, and likely to be occupationally active [1]. For many, maintaining or resuming employment is vital [2], motivated by the need for financial stability and a sense of normalcy [3]. Thus, it is crucial to provide these women with support to maintain or regain their work ability.
Findings from a meta-analysis show that 70% (95% confidence interval [CI]: 69–82%) of women return to work within 2 years after a breast cancer diagnosis [4]. However, women who have returned to work, have more sick leave [5] and report poorer work ability than the general population [6–8]. Work ability is a multidimensional concept encompassing a worker’s physical, psychological, and social capacity to manage job demands [9]. Reduced work ability after breast cancer is often attributed to physical or psychosocial challenges [10, 11].
We lack evidence-based strategies to support breast cancer survivors’ work ability [12, 13]. A recent systematic review on interventions to support return to work among patients with breast cancer identified nine randomized controlled trials (RCTs) [14], of which only one intervention proved effective. This intervention comprised a 2-week multicomponent program with physical and nutritional elements, which led to increased self-reported work ability at 12 months of follow-up [15].
We conducted an RCT assessing the effect of a nurse-led follow-up program including self-management sessions and electronic symptom monitoring without scheduled visits (MyHealth) compared to scheduled outpatient visits with physicians following primary breast cancer treatment. As recently reported, MyHealth significantly improved health-related quality of life and reduced fear of recurrence, anxiety, and depression through 3 years of follow-up [16]. The MyHealth follow-up program did not have a specific occupational focus, but we hypothesize that the positive effect on quality of life and mental health may subsequently improve self-reported work ability, as this association has been established in previous research [10, 11]. Thus, in this study, we report results on self-reported work ability as a secondary outcome in the MyHealth study.
Patients/material and methods
MyHealth is a randomized two-group parallel trial comparing nurse-led individualized follow-up to regular physician-led follow-up conducted at the Department of Clinical Oncology and Palliative Care, Zealand University Hospital, Denmark [16, 17].
Participants and randomization
All consecutive patients were screened for eligibility over a period spanning January 2017–January 2019. Eligible patients were women, at least 40 years old, who had completed primary treatment with curative intent for stage I or II breast cancer within 2 months, who scored 0–3 in Eastern Cooperative Oncology Group (ECOG) performance status and were able to understand and speak Danish. Exclusion criteria were recurrent breast cancer, residual disease, genetic predisposition for breast cancer, presence of other active cancers except non-melanoma skin cancer, severe cognitive impairment or psychiatric disease, or addiction to alcohol or narcotics.
In all, 503 patients were randomized either to MyHealth or control follow-up using an electronic platform that secured concealed allocation. In the present study, we only included participants who were potentially active at the labour market at randomization. Thus, we excluded patients who had retired due to age (n = 150) or were granted disability pension or flexi job due to permanently reduced work ability (n = 35). We also excluded patients aged 65 years or older (n = 26), as we assumed that they would retire due to age during follow-up. Lastly, we excluded patients with missing values on work status or work ability (n = 4). This left 149 patients to MyHealth and 139 to control follow-up for this analysis.
MyHealth follow-up
The MyHealth follow-up program included a self-management intervention, regular symptom reporting, and support by experienced breast cancer nurses who had completed a 6-day course covering the Guided Self-Determination (GDS) method, breast cancer late effects, recurrence symptoms, and navigation [16, 17]. MyHealth consisted of three to five 1-hour individual sessions during a 6-month period after randomization following the GDS method, which aims to empower patients in decision-making and problem-solving [18]. The sessions were structured by reflection sheets to identify the patient’s challenges and improve self-management strategies. Further, the patients reported symptoms electronically every third months the first year, and every sixth months the following 2 years, which were monitored by the nurses to identify symptoms of late effects or potential breast cancer recurrence. The electronic questionnaire included the 23-item Breast Cancer Recurrence instrument [19] and 19 items on adverse or late effects of cancer treatment [16, 17]. If the symptoms exceeded predefined thresholds, the nurses would contact the patient to clarify the need for support or referral to further evaluation or appropriate medical care. Patients could also directly contact the nurses by phone if needed [16, 17].
Control follow-up
Patients in the control group received biannual consultations with physicians at the oncology outpatient clinic, including physical examination and unstructured symptom assessment to screen for breast cancer recurrence and late effects. If needed, the patients could request extra consultations [16, 17].
Work ability
Self-reported work ability was measured at baseline (randomization), and after 6, 12, 24, and 36 months using the single-item Work Ability Score (WAS) [20, 21] from the Work Ability Index [22], which has been found valid to assess status and progress of work ability. Respondents are asked to evaluate their ‘current work ability compared with the lifetime best’ through a score on a scale of 0 (‘completely unable to work’) to 10 (‘work ability at its best’).
We utilized both a continuous and categorical measure of work ability (poor: 0–5; moderate to excellent: 6–10) [9].
Statistics
A linear mixed model was used to estimate the effect of MyHealth follow-up on work ability. To assess the effect of MyHealth follow-up over time, the model included an interaction between randomization group and time (baseline, and after 6, 12, 24, and 36 months), assuming that there was no difference between the groups at baseline [23]. The model included a random intercept for each patient. Missing data on work ability were assumed to be missing at random. The analyses were conducted on the entire population, and separately among patients with poor (WAS 0–5) and moderate to excellent work ability (WAS 6–10). The analyses were performed using Stata version 18.
Results
At baseline, the majority of the 288 patients were working (89% in MyHealth and 90% in control follow-up), while the remaining patients were either on sick leave or unemployed (Table 1). Among those allocated to MyHealth follow-up, a total of 43% reported poor work ability (WAS, 0–5), as did 39% in the control group while the median WAS was 6 in both groups (Table 1).
| MyHealth follow-up | Control follow-up | |||
| No. 149 | % | No. 139 | % | |
| Age | ||||
| 40–55 years | 71 | 48 | 74 | 53 |
| 56–65 years | 78 | 52 | 65 | 47 |
| Cohabitation | ||||
| Yes | 106 | 71 | 115 | 83 |
| No | 43 | 29 | 24 | 17 |
| Education | ||||
| Primary and lower secondary school (9–10 years) | 15 | 10 | 16 | 12 |
| Senior high school and vocational education (10–12 years) | 21 | 14 | 23 | 17 |
| University level 1–2 years 12–15 years) | 26 | 17 | 33 | 24 |
| University level ≥ 3 years (≥15 years) | 87 | 58 | 67 | 48 |
| Employment | ||||
| Employed/self-employed | 133 | 89 | 125 | 90 |
| On sick leave | 10 | 7 | 8 | 6 |
| Unemployed | 6 | 4 | 6 | 4 |
| Menopausal status | ||||
| Premenopausal | 56 | 38 | 52 | 37 |
| Postmenopausal | 93 | 62 | 87 | 63 |
| Tumour size | ||||
| <21 mm | 115 | 77 | 118 | 85 |
| 21–49 mm | 34 | 23 | 21 | 15 |
| Histology | ||||
| Ductal | 120 | 81 | 119 | 86 |
| Lobular | 17 | 11 | 12 | 9 |
| Other | 12 | 8 | 8 | 6 |
| Grade of malignancy | ||||
| I | 27 | 18 | 26 | 19 |
| II | 76 | 51 | 73 | 53 |
| III | 32 | 21 | 29 | 21 |
| Not relevant1 or unknown | 14 | 9 | 11 | 8 |
| Oestrogen receptor status | ||||
| Positive (≥1%) | 137 | 92 | 124 | 89 |
| Negative | 12 | 8 | 15 | 11 |
| HER2 status | ||||
| Amplified | 20 | 13 | 14 | 10 |
| Not amplified | 129 | 87 | 125 | 90 |
| Number of lymph nodes with macro metastases | ||||
| No lymph nodes | 119 | 80 | 106 | 76 |
| 1–3 lymph nodes | 22 | 15 | 30 | 22 |
| >3 lymph nodes | 8 | 5 | 3 | 2 |
| Breast surgery | ||||
| Lumpectomy | 128 | 86 | 118 | 85 |
| Mastectomy | 21 | 14 | 21 | 15 |
| Axillary surgery | ||||
| Sentinel node biopsy | 121 | 81 | 106 | 76 |
| Axillary dissection | 28 | 19 | 33 | 24 |
| (Neo-) Adjuvant chemotherapy | ||||
| Yes | 98 | 66 | 87 | 63 |
| No | 51 | 34 | 52 | 37 |
| Adjuvant radiotherapy | ||||
| Yes | 132 | 89 | 126 | 91 |
| No | 17 | 11 | 13 | 9 |
| Adjuvant endocrine therapy | ||||
| Yes | 132 | 89 | 120 | 86 |
| No | 17 | 11 | 19 | 14 |
| Adjuvant trastuzumab | ||||
| Yes | 20 | 13 | 14 | 10 |
| No | 129 | 87 | 125 | 90 |
| Work ability (WAS) | ||||
| Poor (0–5) | 64 | 43 | 54 | 39 |
| Moderate (6–7) | 35 | 23 | 34 | 24 |
| Good (8–9) | 42 | 28 | 40 | 29 |
| Excellent (10) | 8 | 5 | 11 | 8 |
| HER2: Human epidermal growth factor receptor 2. 1 Grade of malignancy not relevant as histology is neither ductal nor lobular. |
||||
For both groups, WAS increased significantly during the first 6 months following randomization (mean WAS increase MyHealth: 1.64, 95% CI: 1.26; 2.02 and control: 1.57, 95% CI: 1.17; 1.97) (Table 2), and continued to increase slightly but non-significantly (p-values > 0.13) until end of follow-up at 36 months, where it reached a mean score of 8.09, 95% CI: 7.71; 8.49 for patients in MyHealth follow-up and 7.85, 95% CI: 7.44; 8.25 for those in control follow-up (Figure 1A). Improvements in work ability were most pronounced among patients reporting poor work ability at baseline, with WAS increasing from less than 3 to more than 7 during follow-up for patients in both MyHealth and control follow-up (Figure 1C, Table 2).
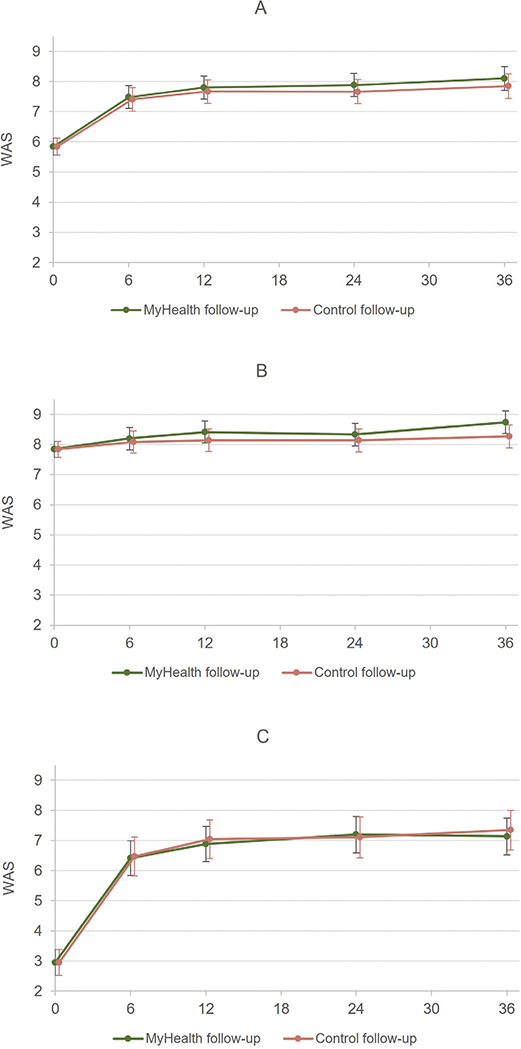
Figure 1. (A) Levels of work ability for all patients in MyHealth and control follow-up at baseline (randomization) and at 6, 12, 24, and 36 months of follow-up. (B) Levels of work ability for patients in MyHealth and control follow-up with initial moderate, good, or excellent work ability (WAS 6–10) at baseline and at 6, 12, 24, and 36 months of follow-up. (C) Levels of work ability for patients in MyHealth and control follow-up with initial poor work ability (WAS 0–5) at baseline and at 6, 12, 24 and 36 months of follow-up.
Effect of intervention
We did not find improved work ability among the patients in MyHealth follow-up compared to the control group at six, 12, 24, and 36 months after randomization (Figure 1A, Table 2). Differences in mean WAS between the two groups were close to zero at all time points (0.07–0.25) and were not statistically significant (Table 2). This was also the case, when we stratified the population on poor and moderate to excellent work ability at randomization (Figure 1B-C, Table 2).
Discussion
Work ability improved significantly over time in both follow-up programs, especially among patients with poor work ability at randomization. The improvements were similar in the MyHealth and control follow-up, and thus MyHealth had no additional effect on self-reported work ability compared to regular follow-up.
It is encouraging that patients in both follow-up programs experienced a rapid improvement in self-reported work ability following primary breast cancer treatment. Patients in both groups achieved what is considered moderate to good work ability (mean WAS 8.1/7.9), approaching levels comparable to those of female general populations (mean WAS 8.2–8.9) [6–9]. Self-reported work ability among patients with breast cancer varies across Scandinavian studies (mean WAS 6.3–8.7) [6, 7, 24]. Comparisons to our results are challenged by a lack of prospective studies, differences in time since diagnosis, and as the study populations vary in age and stage of disease [6, 7, 24].
Previous studies suggest that interventions to improve work ability should specifically target patients with poor work ability [13]. One third of the population in this study reported good to excellent work ability already at randomization and were thus not subject to considerable improvements. When we examined the effects of MyHealth separately for patients with poor and moderate to excellent work ability, no effect on work ability was seen in either of the groups. Still, it is noteworthy that work ability increased considerably during follow-up for those with poor work ability at randomization (from WAS less than 3 to more than 7). Although they did not reach the same levels as those with good to excellent work ability at randomization, they achieved a moderate level of work ability. We did not have information on work ability prior to the breast cancer diagnosis, and for some patients reporting poor work ability at randomization, their habitual work ability might already have been lower than in the general population for reasons other than breast cancer.
No previous RCTs have assessed the effect of a multicomponent follow-up program on self-reported work ability among patients with breast cancer. Furthermore, previous intervention studies tend to focus solely on return to work, number of working hours, and sick leave [14]. Emphasizing enhancement of perceived work ability, rather than solely focusing on return to work, is crucial, as cancer survivors often continue to face physical and psychosocial late effects that affect their work ability beyond return to work [10, 11].
Several studies underline the importance of including elements aimed to explicitly enhance work ability, and to involve the workplace in interventions that aim at supporting cancer patients to return to work [25–27]. The MyHealth follow-up program did not include a systematic occupational focus. The reflection sheets used to structure the sessions with nurses were designed to identify the challenges experienced by each patient. Thus, the sessions covered a range of topics, and not all women mentioned work ability as one of their concerns. The absence of an effect on work ability may be due to the lack of elements directly targeting work.
Strengths and limitations
Internal validity in the MyHealth study is high due to the randomized design, low attrition, long follow-up, and modest amount of missing information. The main limitation is that the MyHealth follow-up program did not include a targeted occupational element. Second, one third of the population reported good to excellent work ability already at randomization and were thus not subject to considerable improvements. Third, no sample size calculation was conducted for self-reported work ability as an outcome, and this study could be under-powered. However, the differences in work ability between patients in MyHealth and control follow-up were consistently close to zero, and confidence intervals were not considerably broad. Fourth, of invited patients, 57% consented to participate. There may be systematic differences between participants and non-participants for example in terms of educational level, and the results of this study may not be generalizable to patients with low educational level. It further limits generalizability that the participants only included women aged 40–64 years old with early-stage breast cancer.
Conclusions
The MyHealth follow-up program had no additional effect on self-reported work ability compared to regular follow-up. It is though encouraging that work ability increased rapidly over time across both groups following primary treatment.
Future interventions that aim to support patients with breast cancer in regaining work ability should be targeted those with poor work ability during or after breast cancer treatment. Also, such interventions should include elements aimed to explicitly enhance work ability.
Ethics declaration
The MyHealth study has been approved by the Danish Ethical Committee System (H-16035885) and complies with the ethical principles in the Helsinki Declaration. The study is registered on ClinicalTrials.gov (identifier NCT02949167).
Acknowledgements
The authors express their gratitude to all participants in the study. They also thank Jane Maher, Lonneke Van De Poll-Franse, and Ruth McCorkle (in memoriam) for guidance in the development of the MyHealth follow-up program. Further, the authors thank senior consultants Birgitte Offersen, Michael Andersson, Niels Kroman, and Anders Bonde for contributions to the recurrence items in the PRO questionnaire. Lastly, the authors give special thanks to the project nurses Linda J. Jensen, Tina Bom, Susanne P. Nielsen, Karin F. Sørensen, and Jette Illum for dedicated participation and Tatiana Hansen for data management.
This work was supported by the Danish Cancer Society (grant number DCS 12714019), Region Zealand, and Copenhagen University Hospital, Rigshospitalet (grant number not applicable).
Data availability statement
Danish legislation prohibits sharing patient data, but collaboration with other researchers is welcomed. Data can be analysed under collaborative study protocols at the Danish Cancer Institute.
References
[1] Engholm G, Ferlay J, Christensen N, Bray F, Gjerstorff ML, Klint A, et al. NORDCAN – a Nordic tool for cancer information, planning, quality control and research. Acta Oncol. 2010;49:725–36. https://doi.org/10.3109/02841861003782017
[2] Nilsson MI, Saboonchi F, Alexanderson K, Olsson M, Wennman-Larsen A, Petersson LM. Changes in importance of work and vocational satisfaction during the 2 years after breast cancer surgery and factors associated with this. J Cancer Surviv. 2016;10:564–72. https://doi.org/10.1007/s11764-015-0502-7
[3] Tan FSI, Shorey S. Experiences of women with breast cancer while working or returning to work: a qualitative systematic review and meta-synthesis. Support Care Cancer. 2022;30:2971–82. https://doi.org/10.1007/s00520-021-06615-w
[4] de Boer AG, Torp S, Popa A, Horsboel T, Zadnik V, Rottenberg Y, et al. Long-term work retention after treatment for cancer: a systematic review and meta-analysis. J Cancer Surviv. 2020;14:135–50. https://doi.org/10.1007/s11764-020-00862-2
[5] Plym A, Johansson ALV, Bower H, Voss M, Holmberg L, Fredriksson I, et al. Causes of sick leave, disability pension, and death following a breast cancer diagnosis in women of working age. Breast. 2019 Jun;45:48-55. https://doi.org/10.1016/j.breast.2019.02.012
[6] Carlsen K, Jensen AJ, Rugulies R, Christensen J, Bidstrup PE, Johansen C, et al. Self-reported work ability in long-term breast cancer survivors. A population-based questionnaire study in Denmark. Acta Oncol. 2013;52:423–9. https://doi.org/10.3109/0284186X.2012.744877
[7] Lindbohm ML, Taskila T, Kuosma E, Hietanen P, Carlsen K, Gudbergsson S, et al. Work ability of survivors of breast, prostate, and testicular cancer in Nordic countries: a NOCWO study. J Cancer Surviv. 2012;6:72–81. https://doi.org/10.1007/s11764-011-0200-z
[8] Gregorowitsch ML, van den Bongard H, Couwenberg AM, Young-Afat DA, Haaring C, Van Dalen T, et al. Self-reported work ability in breast cancer survivors; a prospective cohort study in the Netherlands. Breast. 2019;48:45–53. https://doi.org/10.1016/j.breast.2019.08.004
[9] Gould R, Ilmarinen J, Järvisalo J. Dimensions of work ability. Results of the Health 2000 Survey. Eläketurvakeskus, Finland: Finnish Centre for Pensions. Helsinki, Finland: The Social Insurance Institution. Helsinki, Finland: National Public Health Institute. Helsinki, Finland: Finnish Institute of Occupational Health; 2008.
[10] Duijts SF, van Egmond MP, Spelten E, van Muijen P, Anema JR, van der Beek AJ. Physical and psychosocial problems in cancer survivors beyond return to work: a systematic review. Psychooncology. 2014;23:481–92. https://doi.org/10.1002/pon.3467
[11] Kim SY, Kissane DW, Richardson G, Senior J, Morgan J, Gregory P, et al. The role of depression and other psychological factors in work ability among breast cancer survivors in Australia. Psychooncology. 2022;31(2):167–75. https://doi.org/10.1002/pon.5802
[12] de Boer AG, Tamminga SJ, Boschman JS, Hoving JL. Non-medical interventions to enhance return to work for people with cancer. Cochrane Database Syst Rev. 2024;3:CD007569. https://doi.org/10.1002/14651858.CD007569.pub4
[13] de Boer A, de Wind A, Coenen P, van Ommen F, Greidanus MA, Zegers AD, et al. Cancer survivors and adverse work outcomes: associated factors and supportive interventions. Br Med Bull. 2023;145:60–71. https://doi.org/10.1093/bmb/ldac028
[14] Algeo N, Bennett K, Connolly D. Rehabilitation interventions to support return to work for women with breast cancer: a systematic review and meta-analysis. BMC Cancer. 2021;21:895. https://doi.org/10.1186/s12885-021-08613-x
[15] Mourgues C, Gerbaud L, Leger S, Auclair C, Peyrol F, Blanquet M, et al. Positive and cost-effectiveness effect of spa therapy on the resumption of occupational and non-occupational activities in women in breast cancer remission: a French multicentre randomised controlled trial. Eur J Oncol Nur. 2014;18:505–11. https://doi.org/10.1016/j.ejon.2014.04.008
[16] Saltbæk L, Bidstrup PE, Karlsen RV, Høeg BL, Horsboel TA, Belmonte F, et al. Nurse-led individualized follow-up versus regular physician-led visits after early breast cancer (MyHealth): a phase III randomized, controlled trial. J Clin Oncol. 2024;42:2038–49. https://doi.org/10.1200/JCO.23.01447
[17] Saltbaek L, Karlsen RV, Bidstrup PE, Hoeg BL, Zoffmann V, Horsbol TA, et al. MyHealth: specialist nurse-led follow-up in breast cancer. A randomized controlled trial – development and feasibility. Acta Oncol. 2019;58:619–26. https://doi.org/10.1080/0284186X.2018.1563717
[18] Zoffmann V, Lauritzen T. Guided self-determination improves life skills with type 1 diabetes and A1C in randomized controlled trial. Patient Educ Couns. 2006;64:78–86. https://doi.org/10.1016/j.pec.2005.11.017
[19] Høeg BL, Saltbæk L, Christensen KB, Karlsen RV, Johansen C, Dalton SO, et al. The development and initial validation of the Breast Cancer Recurrence instrument (BreastCaRe)-a patient-reported outcome measure for detecting symptoms of recurrence after breast cancer. Qual Life Res. 2021;30(9):2671–82. https://doi.org/10.1007/s11136-021-02841-1
[20] Ahlstrom L, Grimby-Ekman A, Hagberg M, Dellve L. The work ability index and single-item question: associations with sick leave, symptoms, and health – a prospective study of women on long-term sick leave. Scand J Work Environ Health. 2010;36:404–12. https://doi.org/10.5271/sjweh.2917
[21] Ebener M, Hasselhorn HM. Validation of short measures of work ability for research and employee surveys. Int J Environ Res Public Health. 2019;16(18):3386. https://doi.org/10.3390/ijerph16183386
[22] Ilmarinen J. The Work Ability Index (WAI). Occup Med. 2007;57(2):160. https://doi.org/10.1093/occmed/kqm008
[23] Coffman CJ, Edelman D, Woolson RF. To condition or not condition? Analysing ‘change’ in longitudinal randomised controlled -trials. BMJ Open. 2016;6(12):e013096. https://doi.org/10.1136/bmjopen-2016-013096
[24] Vandraas K, Falk RS, Bøhn SKH, Kiserud C, Lie HC, Smedsland SK, et al. Work ability 8 years after breast cancer: exploring the role of social support in a nation-wide survey. Breast Cancer Res Treat. 2022;193:685–94. https://doi.org/10.1007/s10549-022-06599-z
[25] Cocchiara RA, Sciarra I, D’Egidio V, Sestili C, Mancino M, Backhaus I, et al. Returning to work after breast cancer: a systematic review of reviews. Work. 2018;61:463–76. https://doi.org/10.3233/WOR-182810
[26] Algeo N, Bennett K, Connolly D. Prioritising the content and delivery of a work-focused intervention for women with breast cancer using the nominal group technique. Work. 2022;73:1337–45. https://doi.org/10.3233/WOR-211160
[27] Butow P, Laidsaar-Powell R, Konings S, Lim CYS, Koczwara B. Return to work after a cancer diagnosis: a meta-review of reviews and a meta-synthesis of recent qualitative studies. J Cancer Surviv. 2020;14:114–34. https://doi.org/10.1007/s11764-019-00828-z