SHORT REPORT
Gender differences in palliative care needs among Swedish cancer patients prior to specialist palliative care referral
Karin Boo Hammasa,b, Juliet Jacobsena,c, Rebecca Selbergd, Sanjoy Mahajana,e and Jenny Klintmana,b,f
aDepartment of Clinical Sciences Lund, Medical Oncology, Lund University, Lund, Sweden; bDepartment of Specialised Palliative Care, Advanced Home Health Care, Kristianstad, Sweden; cHarvard Medical School and Massachusetts General Hospital, Boston, MA, USA; dDepartment of Sociology, Lund University, Lund, Sweden; eCentre for Mathematical Sciences, Lund University, Lund, Sweden; fThe Institute for Palliative Care, Lund, Sweden
Abstract
Background and purpose: Few studies, in Sweden or internationally, have examined gender differences regarding the use of palliative care. This study investigates gender differences in palliative care needs prior to referral in a regional cohort of Swedish cancer patients.
Patient/material and methods: Adult cancer patients who died throughout 1 year and were referred to a specialized palliative care service in southern Sweden during their last 3 years of life (n = 192) were included. Information on gender, age, diagnosis, performance status, admissions to hospital, and serious illness conversations was collected through chart review.
Results: Ninety-nine (52%) women and 93 (48%) men were included. Survival from diagnosis until death was comparable (p = 0.27) for women (341.0 days, IQR 77.0–902.0) and men (463.0 days, IQR 141.0–1035.0), as was survival from palliative care referral (p = 0.06) (women 48.0 days, IQR 19.0‑107.5; men 36.0 days, IQR 17.0‑85.0). Performance status at the time of referral was also comparable (p = 0.59). Gender differences were observed in healthcare utilization with fewer hospitalizations and emergency department visits for women in the 6 months prior to referral (p = 0.03) and significantly more men among those with the highest healthcare utilization (≥4 hospitalizations and emergency department visits) (p = 0.005). During the month before referral, women were more likely to have a serious illness conversation (p = 0.01).
Interpretation: Compared to women, men have more hospitalizations and fewer serious illness conversations prior to referral to specialized palliative care, suggesting greater unmet palliative care needs.
KEYWORDS: Palliative care; gender equity; healthcare disparities; health communication
Citation: ACTA ONCOLOGICA 2025, VOL. 64, 672–676. https://doi.org/10.2340/1651-226X.2025.43308
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Oncologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Received: 5 March 2025; Accepted: 29 April 2025; Published: 14 May 2025
CONTACT: Jenny Klintman jenny.klintman@med.lu.se Department of Clinical Sciences Lund, Medical Oncology, Lund University, Sölvegatan 19, SE-22362 Lund, Sweden
Competing interests and funding: The authors report there are no competing interests to declare.
Introduction
Previous studies on gender differences in end-of-life care (mostly conducted in the UK and USA [1]) suggest that men have greater unmet palliative care needs. Men are less likely to communicate about serious illness. For example, men diagnosed with advanced cancer are less likely to state that their tumor is incurable or to have a conversation about prognosis [2] or mortality [3]. Men more frequently make treatment decisions at the end of life that are associated with more aggressive, generally nonbeneficial care [4]. Men in the last stages of life are more likely to receive intensive care unit treatment, cardiopulmonary resuscitation, mechanical ventilation, hemodialysis, and surgical procedures [5–7]. Similarly, men in the last days of life are more likely to receive chemotherapy and less likely to request palliative care [8] or to receive hospice care [7].
In Sweden, few studies focus on gender differences in palliative care, and the findings are somewhat contradictory. On one hand, men and women who wish to die at home do so to the same extent [9]. For patients with ALS, there is no gender difference in access to palliative care [10], and men and women with brain tumors have comparable access to specialized palliative care (SPC) in the last month of life although men are more likely to be hospitalized [11]. However, in hematologic malignancies, women were more likely to receive SPC during the last 3 months of life [12]. Contrary to the American findings, Swedish women tend to receive more aggressive care than men. Swedish women are more likely than men to receive palliative chemotherapy [13], and women with esophageal cancer spend a higher proportion of their time hospitalized than men in the first year after diagnosis [14].
These studies focused on end-of-life care. As the value of palliative care is increasingly recognized and evidence supports earlier integration of palliative care [15], there is a need to investigate barriers to care access (including gender) in healthcare settings outside of SPC. Thus, we aimed to investigate gender differences in primary palliative care needs of cancer patients, focusing on timing of SPC-referral, healthcare utilization, and communication about serious illness prior to referral.
Patients/material and methods
This is a retrospective observational study. Region Skane has one regional provider of comprehensive SPC with eight local sites. This study was conducted in one local site with a catchment area population of approximately 110,000 inhabitants. Hospital care is provided by a 24-h-service regional hospital with approximately 250 beds and 2,500 staff. The study included all adults with a diagnosis of incurable cancer who died between 1 September 2022 and 31 August 2023 and who had been referred to the local SPC unit in the last 3 years of life (n = 192). Using chart review, we collected the date of the last systemic anticancer treatment before death and baseline information at referral: gender, age, living situation, date of primary cancer diagnosis, and performance status (ECOG). We also collected Supportive and Palliative Care Indicators Tool (SPICT) indicators of palliative care needs (general indicators of poor or deteriorating health and clinical indicators of serious illnesses or health conditions) [16], unplanned hospitalizations, and emergency department (ED) visits during the 6 months prior to referral to SPC (or from date of diagnosis if cancer diagnosis was <6 months before referral). Finally, because serious illness communication (SIC) is important for advance care planning and goals-of-care discussions [17], we screened for four key components of an SIC (information about disease progression/prognosis, patient priorities, treatment options/plan in case of deterioration/withholding of life-sustaining treatment, and options for symptom relief) during the month before referral to SPC. Referring clinicians were from a wide range of clinics including oncology, gynecology, lung, surgery, and urology. Gender of the referring clinician was not collected. Chart review was done by the first author, an experienced primary and palliative care physician (KBH).
Data analysis and statistics
Data were collected and stored in REDCap. Descriptive information on background characteristics of the study group is presented as frequencies, percentages, median, and interquartile range (IQR). Comparisons of medians between women and men were performed using the Mann‑Whitney test for continuous parameters and Fisher’s exact test and the chi-squared test with Yates’ continuity correction for proportions. A p < 0.05 was considered statistically significant. Statistical analyses were made in Microsoft Excel (version 2402 for Windows, Microsoft Corporation, Redmond, WA, USA), with the programming language R (version 4.3.0, R Core Team (2023) R Foundation for Statistical Computing, Vienna, Austria) and with GraphPad Prism (version 9.1.2, GraphPad Software Inc., La Jolla, California, USA).
Results
Ninety-nine women (52%) and 93 men (48%) were included (Table 1). All patients fulfilled ≥1 general SPICT indicator and the clinical indicator related to cancer (i.e. progressive disease or no curative treatment intent). The most common cancer forms were upper gastrointestinal (n = 46, 24%), colorectal (n = 29, 15%), and lung (n = 21, 11%) (Table 1). The median age at referral was 75.9 years. Most women (n = 89, 90%) and men (n = 88, 95%) were living at home; 49/89 women (49%) and 33/88 men (35%) lived alone (p = 0.07). The median number of days from the last systemic anticancer treatment until death was similar in women (64.5 days; IQR 37.8‑178.0) and men (66.5 days; IQR 38.5‑127.0, p = 0.67). Median days were comparable between women and men from referral to SPC until death (women 48.0 days (IQR 19.0‑107.5) and men 36.0 days (IQR 17.0‑85.0, p = 0.06) and from primary cancer diagnosis until death (women 341 days; IQR 77.0‑902.0) and men (463.0 days; IQR 141.0‑1035.0, p = 0.27). There was no gender difference in performance status (WHO/ECOG) at referral (p = 0.59). Six months prior to referral to SPC, the median number of ED visits/hospitalizations was significantly fewer for women (1.0; IQR 0.0‑2.0) than men (2.0; IQR 0.0‑3.0, p = 0.03). In a subset analysis of healthcare utilization in patients with ≤200 survival days from SPC referral (n = 153: n women 76 and n men 77), significantly more men (n = 24, 31.2% of 77 men and n = 9, 11.8% of 76 women, p = 0.005) had ≥4 ED visits/hospitalizations (Figure 1).
| Variables investigated | Total | Women | Men | p* | |||||
| Included patients (n, %) | 192 | 99 (52) | 93 (48) | na | |||||
| Median age at first referral (IQR) (n = 192) | 75.9 (68.5–82.5) | 76.5 (68.4–84.2) | 74.8 (69.4–81.6) | 0.55 | |||||
| Residing in own home (n, %) (n = 192) | 177 (92) | 89 (90) | 88 (95) | 0.29 | |||||
| Nursing home resident (n, %) (n = 192) | 15 (8) | 10 (10) | 5 (5) | 0.29 | |||||
| Living alone (n, %) (n = 192) | 82 (43) | 49 (49) | 33 (35) | 0.07 | |||||
| Median survival from cancer diagnosis (days, IQR) (n = 192) | 395.0 (103–1020) | 341.0 (77.0–902.0) | 463.0 (141.0–1035.0) | 0.27 | |||||
| Median survival from last systemic anticancer treatment (days, IQR) (n = 122)a | 65.5 (37.8–161.5) | 64.5 (37.8–178.0, n = 58) | 66.5 (38.5–127.0, n = 64) | 0.67 | |||||
| Cancer diagnosis (n, %) (n = 192) | Upper GI, bile, pancreatic | 46 (24.0) | 26 (56.5) | 20 (43.5) | na | ||||
| Colorectal | 29 (15.1) | 9 (31.0) | 20 (69.0) | na | |||||
| Lung | 21 (10.9) | 13 (61.9) | 8 (30.1) | na | |||||
| Prostate | 17 (8.9) | na | 17 | na | |||||
| Gynecological | 13 (6.8) | 13 | na | na | |||||
| Hematological | 12 (6.3) | 8 (66.7) | 4 (33.3) | na | |||||
| Breast | 11 (5.7) | 11 | na | na | |||||
| CNS | 10 (5.2) | 4 (40.0) | 6 (60.0) | na | |||||
| Unknown primary | 9 (4.7) | 6 (66.7) | 3 (33.3) | na | |||||
| Urological | 6 (3.1) | 0 | 6 (100) | na | |||||
| Ear, nose, throat | 6 (3.1) | 2 (33.3) | 4 (66.7) | na | |||||
| Hepatocellular | 5 (2.6) | 3 (60.0) | 2 (40.0) | na | |||||
| Melanoma | 5 (2.6) | 2 (40.0) | 3 (60.0) | na | |||||
| Sarcoma | 2 (1.0) | 2 (100) | 0 | na | |||||
| ECOG at referral (median, IQR) (n = 185)b | 3.0 (3.0–3.0) | 3.0 (3.0–3.0, n = 96) | 3.0 (2.0–3.0, n = 89) | 0.59 | |||||
| Hospital admissions and ED visits <6 months prior to the first PC referral (median, IQR) (n = 192) | 1.0 (0.0–3.0) | 1.0 (0.0–2.0) | 2.0 (0.0–3.0) | 0.03 | |||||
| Median survival from SPC referral (days, IQR) (n = 182)c | 42.0 (17.0–95.0) | 48.0 (19.0–107.5, n = 95) | 36.0 (17.0–85.0, n = 87) | 0.06 | |||||
| * Comparisons were performed using the Mann‑Whitney test for continuous parameters and Fisher’s exact test for proportions. a Includes patients who received systemic anticancer treatment with palliative intent. b ECOG performance status was not assessable for seven patients c Includes patients referred for assessment of full enrolment in specialized palliative care. Patients referred for limited care provision (e.g. erythrocyte transfusion, antibiotic treatment, etc.) were not included in this analysis. GI: gastrointestinal; CNS: central nervous system; ECOG: Eastern Cooperative Oncology Group; ED: emergency department; SPC: specialized palliative care; IQR: interquartile range. |
|||||||||
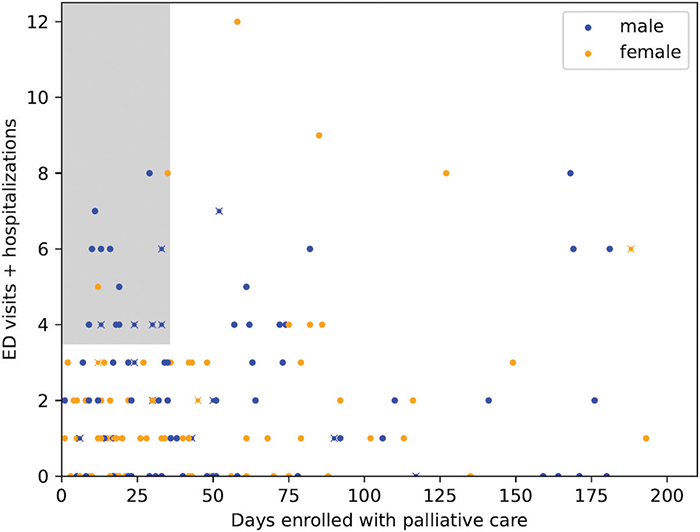
Figure 1. Healthcare utilization in a subset of patients with ≤200 survival days from SPC referral (n = 153: n women 76, n men 77). Significantly more men (blue) than women (yellow) had ≥4 ED visits/hospitalizations (n = 24, 31.2% of 77 men and n = 9, 11.8% of 76 women, p = 0.005). Men (blue) were the most of patients (n men = 14/16, 87.5%) with the highest palliative care needs defined as highest utilization of unplanned hospital care (≥4 ED visits/hospitalizations), latest palliative care referral (≤35 days before death), and no documented SIC (n = 5/14 of men, 35.7%) (grey box, those with an x).
Women were more likely than men to have documentation of at least one of four components of an SIC prior to SPC referral (p = 0.01). More women than men had a documented conversation about disease progression/prognosis (p = 0.02) and priorities (p = 0.049) (Table 2). When adjusted for living alone, the gender difference was still significant regarding total frequency of SIC (p = 0.01). Finally, we analyzed SIC in a subset of patients with the highest healthcare utilization (≥4 ED visits/hospitalizations) and latest SPC referral (≤35 days before death) (n = 16, grey box Figure 1) in which men were the majority (n = 14, 87.5%) and among which 35.7% (n = 5/14) had no documented SIC.
| SIC components | Total | Women | Men | p-value* |
| Information regarding prognosis/disease progression (n, %) (n = 192) | 140 (72.9) | 80 (80.8) | 60 (64.5) | 0.02 |
| Patient priorities (n, %) (n = 192) | 66 (34.4) | 41 (41.4) | 25 (26.9) | 0.049 |
| Treatment in case of deterioration/withholding of life-sustaining treatment (n, %) (n = 192) | 79 (41.1) | 47 (47.5) | 32 (34.4) | 0.09 |
| Symptom relief (n, %) (n = 192) | 95 (49.5) | 56 (56.6) | 39 (41.9) | 0.06 |
| Conversation about any of the four themes (n, %) (n = 192) | 163 (81.9) | 91 (91.9) | 72 (77.4) | 0.01 | * Comparisons were performed using the chi-squared test with Yates’ continuity correction. |
Discussion and conclusion
We present an investigation of gender differences in palliative care needs prior to SPC referral in a regional Swedish cancer cohort, and we find men having more unmet palliative care needs than women. Compared to women, men had more ED visits and hospital admissions and fewer documented SICs prior to SPC referral.
We did not find any clear structural factors that explain these gender differences. The groups were similar in age, living accommodations, time of last systemic anticancer treatment, and performance status. Because survival from diagnosis was similar for men and women, we could not explain the difference as due to more aggressive disease progression among men. A potential structural difference identified was a trend toward men cohabitating more frequently than women (p = 0.07). This difference accords with an earlier study showing that men rely more than women on social support from their partners, while it is important for women to communicate with and receive support from healthcare personnel [14]. Living with a partner could potentially influence healthcare utilization and communication needs. However, after adjusting for living with a partner or not, men still had significantly fewer SICs and a trend toward more healthcare utilization.
The gender distribution in diagnoses could have influenced our results. However, apart from for lung and urothelial cancers, the gender distribution was comparable in the included cancer types and in the number of patients with gendered cancers (gynecological and breast versus prostate) (Table 1). Furthermore, all the included patients fulfilled at least one SPICT criterion for palliative care needs [16]. Even so, only 27% of men (versus 41% of women) had a documented SIC about priorities, goals of care, etc. prior to referral to SPC, which indicates an unmet palliative care need.
Interestingly, our results contradict some Swedish studies that show no gender difference in use of palliative care [9–11]. However, in hematologic malignancies, women were more likely to be enrolled in SPC at the end of life [12], and international studies have shown higher healthcare utilization and less access to palliative care among men [2, 3, 5–8]. Differences could be explained by study design or epidemiologic reasons. Several of the Swedish studies included cohorts with specific diagnosis and uneven gender distribution, whereas our study includes an unselected, consecutively collected, cohort of cancer patients. Furthermore, the healthcare setting may influence the results. Most of the previous Swedish studies were conducted in the capital region of Stockholm, whereas our cohort resides in a more rural area, albeit still rather densely populated, a difference that might affect access to care and referral patterns. SPC is organized differently across healthcare regions in Sweden, which makes nationwide conclusions difficult to draw based on results from regional studies.
An important finding is that men have fewer documented SICs compared to women. This lower conversation rate is both an outcome and a potential mediator of increased healthcare utilization for men. One possible explanation for the lower conversation rate is poor and/or biased communication skills among clinicians. Studies have found that clinicians lack adequate communication skills training [17] and therefore the confidence and ability to engage in SICs. This lacuna could result in a gender-biased communication practice, in which clinicians more easily approach women for conversations [17]. In society in general, women are thought of as better communicators, while men are thought of as less inclined to express and share feelings – sometimes described as women being ‘expressive’ and men ‘instrumental’ in their communication styles [18]. Such perceived differences could be emphasized by physicians who feel insecure in their communication skills to the detriment of male patients. Alternatively, gendered communication practices may reflect patients’ actual communication preferences; one previous study indicated that female patients tend to be more vocal about their needs and preferences than male patients [19]; perhaps men, more than women, avoid conversations about their illness. Gendered communication differences may not only reflect unmet palliative care needs but may also reflect patients’ wishes [20].
In the clinical setting, there is a fine line between respecting patients’ information and communication preferences and enabling informed medical decision making, which necessitates some prognostic awareness of what lies ahead and the potential benefits (and risks) of treatments and other care options, such as palliative care. Our results indicate that by the time men are enrolled in SPC, they have had few SICs and therefore may need more end-of-life preparation and support. More research on the gender gap in communication is needed [21, 22].
A strength of this study is that it includes all cancer patients referred to a single SPC practice within a geographic region. This approach limits selection bias and ensures that the study represents the needs of a population with a range of different cancer types. A limitation is the small cohort that could be disproportionally impacted by local traditions and referral patterns. All patients in this study were referred to SPC, and the results might have differed if we also had included patients never referred at all. Our next step is therefore to expand the analysis with region-wide registry data.
In conclusion, although care equity is one of the main principles in Swedish healthcare, our study suggests a gendered difference in palliative care needs. Prior to referral to SPC, men have more ED visits and hospitalizations and fewer opportunities for SICs than women. These results are an argument for more research and a greater awareness of potential structural biases in the provision of palliative care.
Acknowledgements
The authors would like to thank Carver Mead for his mentorship and support and Dr. Oskar Hagberg for support with statistical analyses. Jenny Klintman was supported by grants from ALF, a national agreement between the Swedish government and seven regions to support clinical research and the education of physicians. The research project was funded by Mrs. Berta Kamprad’s Cancer Foundation.
Data availability statement
The data are available upon request from the corresponding author.
Ethics declarations & trial registry information
All data were on deceased patients (not considered sensitive personal data) and are exempt from the requirement for an ethics application according to Swedish law. Data were handled in accordance with research ethics principles and in accordance with the Declaration of Helsinki. Region Skane approved the data extraction (KVB dnr 249-23 and 273-23).
Author contributions
KBH, JJ, and JK designed this study. KBH collected the data. KBH and JK planned the quantitative analyses and KBH performed them with support from statistical expert Dr Oscar Hagberg. KBH, JJ, RS, SM, and JK analyzed the results. KBH, JJ, and JK drafted the manuscript. All authors reviewed, edited, and approved the final manuscript.
References
[1] Wong AD, Phillips SP. Gender disparities in end of life care: a scoping review. J Palliat Care. 2023;38(1):78–96. https://doi.org/10.1177/08258597221120707
[2] Fletcher K, Prigerson HG, Paulk E, Temel J, Finlay E, Marr L, et al. Gender differences in the evolution of illness understanding among patients with advanced cancer. J Support Oncol. 2013;11(3):126–32. https://doi.org/10.12788/j.suponc.0007
[3] Skulason B, Hauksdottir A, Ahcic K, Helgason AR. Death talk: Gender differences in talking about one’s own impending death. BMC Palliative Care. 2014;13(1):8. https://doi.org/10.1186/1472-684X-13-8
[4] Ferrell BR, Temel JS, Temin S, Alesi ER, Balboni TA, Basch EM, et al. Integration of Palliative Care Into Standard Oncology Care: American Society of Clinical Oncology Clinical Practice Guideline update. J Clin Oncol. 2017;35(1):96–112. https://doi.org/10.1200/JCO.2016.70.1474
[5] Just E, Casarett DJ, Asch DA, Dai D, Feudtner C. Differences in terminal hospitalization care between U.S. Men and women. J Pain Symptom Manage. 2016;52(2):205–11. https://doi.org/10.1016/j.jpainsymman.2016.01.013
[6] Sharma RK, Prigerson HG, Penedo FJ, Maciejewski PK. Male-female patient differences in the association between end-of-life discussions and receipt of intensive care near death. Cancer. 2015;121(16):2814–20. https://doi.org/10.1002/cncr.29417
[7] Miesfeldt S, Murray K, Lucas L, Chang CH, Goodman D, Morden NE. Association of age, gender, and race with intensity of end-of-life care for Medicare beneficiaries with cancer. J Palliat Med. 2012;15(5):548–54. https://doi.org/10.1089/jpm.2011.0310
[8] Saeed F, Hoerger M, Norton SA, Guancial E, Epstein RM, Duberstein PR. Preference for palliative care in cancer patients: Are men and women alike? J Pain Symptom Manage. 2018;56(1):1–6 e1. https://doi.org/10.1016/j.jpainsymman.2018.03.014
[9] Nilsson J, Bergstrom S, Hallberg H, Berglund A, Bergqvist M, Holgersson G. Prospective study of preferred versus actual place of death among Swedish palliative cancer patients. Am J Hosp Palliat Care. 2024;41(9):969–77. https://doi.org/10.1177/10499091231213640
[10] Strang P, Schultz T, Ozanne A. Partly unequal receipt of healthcare in last month of life in amyotrophic lateral sclerosis: a retrospective cohort study of the Stockholm region. Upsala J Med Sci. 2024;129:e9856. https://doi.org/10.48101/ujms.v129.9856
[11] Lindskog M, Schultz T, Strang P. Acute healthcare utilization in end-of-life among Swedish brain tumor patients – a population based register study. BMC Palliat Care. 2022;21(1):133. https://doi.org/10.1186/s12904-022-01022-2
[12] Von Bahr L, Strang P, Schultz T, Fürst P. Receipt of specialized palliative care and health care utilization at the end of life in hematological cancer patients – the Stockholm experience. Acta Oncol. 2025;64:234–40. https://doi.org/10.2340/1651-226X.2025.42189
[13] Randen M, Helde-Frankling M, Runesdotter S, Strang P. Treatment decisions and discontinuation of palliative chemotherapy near the end-of-life, in relation to socioeconomic variables. Acta Oncol. 2013;52(6):1062–6. https://doi.org/10.3109/0284186X.2012.758872
[14] Linder G, Klevebro F, Edholm D, Johansson J, Lindblad M, Hedberg J. Burden of in-hospital care in oesophageal cancer: national population-based study. BJS Open. 2021;5(3):zrab037. https://doi.org/10.1093/bjsopen/zrab037
[15] Haun MW, Estel S, Rucker G, Friederich HC, Villalobos M, Thomas M, et al. Early palliative care for adults with advanced cancer. Cochrane Database Syst Rev. 2017;6(6):CD011129. https://doi.org/10.1002/14651858.CD011129.pub2
[16] Pham L, Arnby M, Benkel I, Dahlqvist Jonsson P, Kallstrand J, Molander U, et al. Early integration of palliative care: translation, cross-cultural adaptation and content validity of the Supportive and Palliative Care Indicators Tool in a Swedish healthcare context. Scand J Caring Sci. 2020;34(3):762–71. https://doi.org/10.1111/scs.12781
[17] Bernacki RE, Block SD, Force ftACoPHVCT. Communication about serious illness care goals: a review and synthesis of best practices. JAMA Intern Med. 2014;174(12):1994–2003. https://doi.org/10.1001/jamainternmed.2014.5271
[18] Mohindra V, Azhar S. Gender communication: a comparative analysis of communicational approaches of men and women at workplaces. J Hum Soc Sci. 2012;2(1):18–27. https://doi.org/10.9790/0837-0211827
[19] Schnitzer S, Kuhlmey A, Adolph A, Holzhausen J, Schenk L. Complaints as indicators of health care shortcomings: which groups of patients are affected? Int J Qual Health Care. 2012;24(5):476–82. https://doi.org/10.1093/intqhc/mzs036
[20] Ullrich A, Grube K, Hlawatsch C, Bokemeyer C, Oechsle K. Exploring the gender dimension of problems and needs of patients receiving specialist palliative care in a German palliative care unit – the perspectives of patients and healthcare professionals. BMC Palliat Care. 2019;18(1):59. https://doi.org/10.1186/s12904-019-0440-7
[21] Wu C, McLaughlin K. Bridging the gender gap in communication skills. Adv Health Sci Educ. 2013;18(1):129–31. https://doi.org/10.1007/s10459-012-9420-x
[22] Driscoll AM, Suresh R, Popa G, Berglund L, Azer A, Hed H, et al. Do educational interventions reduce the gender gap in communication skills? – a systematic review. BMC Med Educ. 2024;24(1):827. https://doi.org/10.1186/s12909-024-05773-9