ORIGINAL ARTICLE
Prostate cancer incidence and mortality among immigrants in Finland between 2000 and 2017 – a register-based cohort study
Katja M. Mustonena,b  , Maarit H. Lamminmäkib , Tytti M. Sarkealab,c and Sirpa H. Heinävaarab,d
, Maarit H. Lamminmäkib , Tytti M. Sarkealab,c and Sirpa H. Heinävaarab,d
aFaculty of Medicine, University of Helsinki, Helsinki, Finland; bFinnish Cancer Registry, Helsinki, Finland; cFaculty of Social Sciences, University of Tampere, Tampere, Finland; dDepartment of Public Health, Faculty of Medicine, University of Helsinki, Helsinki, Finland
Abstract
Background and purpose: Prostate cancer impacts millions of men worldwide each year, and its significance will continue to rise as populations age. Literature demonstrates differences in cancer burden between immigrant groups and non-immigrants across the world. Despite its prevalence, little research has focused primarily on prostate cancer among immigrants.
Patients/material and methods: We utilized individual-level data on all immigrant men who had lived in Finland for over a year between 1973 and 2017 and aggregate data on Finnish-born men to determine immigrants’ incidence of and mortality from prostate cancer in relation to the men born in Finland. This gave us a study population of 162,844 non-Western and 56,127 Western immigrant men. Cases and deaths from the study period (2000–2017) were analyzed with the multivariate Poisson regression model for the groups, non-Western and Western immigrants separately.
Results and Interpretation: Non-Western men had a relative risk (RR) of 0.663 (95% confidence interval [CI] 0.609–0.722) for cases and 0.803 (0.646–0.997) for deaths. Western men had RRs of 0.876 (0.784–0.978) and 0.78 (0.567–1.072), respectively. A longer duration of residence and a younger age at immigration increased the risk for prostate cancer. Compared to the men born in Finland, both immigrant groups showed a lower risk of prostate cancer. Non-Western men may have also had a lower risk of death from it. Prostate cancer mortality in non-Western immigrants appears to be high compared to its incidence. While uncertain, this implication is concerning enough to warrant further research into the topic.
KEYWORDS: Prostate cancer; epidemiology; inequality; migrant health; registry data
Citation: ACTA ONCOLOGICA 2025, VOL. 64, 830–836. https://doi.org/10.2340/1651-226X.2025.43328.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Oncologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Received: 9 March 2025; Accepted: 12 June 2025; Published: 29 June 2025
CONTACT: Katja M. Mustonen katja.mustonen@cancer.fi Finnish Cancer Registry, Mäkelänkatu 2, 00500 Helsinki, Finland
Supplemental data for this article can be accessed online at https://doi.org/10.2340/1651-226X.2025.43328
Competing interests and funding: The authors report there are no competing interests to declare.
Introduction
Immigrants are often at a disadvantageous position in society [1], which has been linked to worse survival of many cancers [2]. In addition, although all who are residing in a municipality in Finland are entitled to highly affordable and comprehensive public health services [3], immigrants face unique barriers to accessing healthcare, including language barriers, cultural conflicts and misunderstandings, discrimination and prejudice, insufficient knowledge of available services, and worse quality of care [4–6]. Perhaps due to these barriers, immigrants utilize health services less than their locally-born counterparts [7]. Addressing these issues begins with providing policymakers and clinicians with accurate and specific information on the special characteristics of immigrants’ disease burden.
The relative size of the immigrant population of Finland increased by approximately 260% during our study period of 2000–2017, from around 2.7% of the total population to nearly 7.1% [8]. Most of these immigrants come from regions with different cultures and healthcare systems, as seen in Table 1. For these reasons, immigrant health is no longer a marginal issue, but warrants careful consideration.
According to estimates, there are 1.4 million new prostate cancer (PCa) cases and 375,000 deaths annually worldwide [9]. PCa is the second most common non-skin malignancy in the world, and the fifth most common cause of cancer death in men [9]. However, incidence and mortality rates exhibit significant variation between regions: both are generally highest in Western countries, with the exception of many sub-Saharan African regions and the Caribbean, which in addition to a high incidence, exhibit exceptionally high mortalities [9]. An important cause for the differences in incidence is the abundant and controversial use of prostate-specific antigen (PSA) testing [10], which varies starkly between countries [9]. Very few countries, Finland not among them, have ever implemented organized PCa screening programs, and debate over its advantages and disadvantages is ongoing [11].
Due to PCa’s strong association with advanced age [12], its impact on disability-adjusted life years will grow in the future as different populations age and life-expectancies grow [13], underlining the importance of understanding all aspects of the disease. Previous studies from around the world have examined different aspects of immigrant health extensively [14–16], including many cancer-focused studies [17, 18]. However to our knowledge, none have studied PCa among immigrants in Finland, even though there have been results from other Nordic countries of differences between non-immigrants and immigrants [17].
The aim of our study is to establish immigrants’ relative risk (RR) of and death from PCa in Finland in comparison to that of men born in Finland. To this end, we compared the PCa risks of Western and non-Western immigrants separately to those of the men born in Finland using long-term registry data analyzed with the Poisson regression model.
Materials and methods
We compared the incidence of and mortality from prostate cancer (ICD code C61) among immigrant men in Finland between the years 2000 and 2017 to that of Finnish men. We first gathered individual-level data on immigrant men from the Finnish Digital and Population Data Services Agency (DPDSA) and Statistics Finland. Individual data on all men with PCa were gathered from Finnish Cancer Registry (FCR) databases.
An immigrant was defined as an individual born outside Finland. From the DPDSA, we extracted data on the birth country of all immigrant men who had lived in Finland between 1973 and 2017 (Figure 1). These data were linked with first primary PCa diagnoses and deaths obtained for the same period. The data on the causes of death were obtained from Statistics Finland. The data on possible emigrations of immigrants were obtained from the DPDSA.
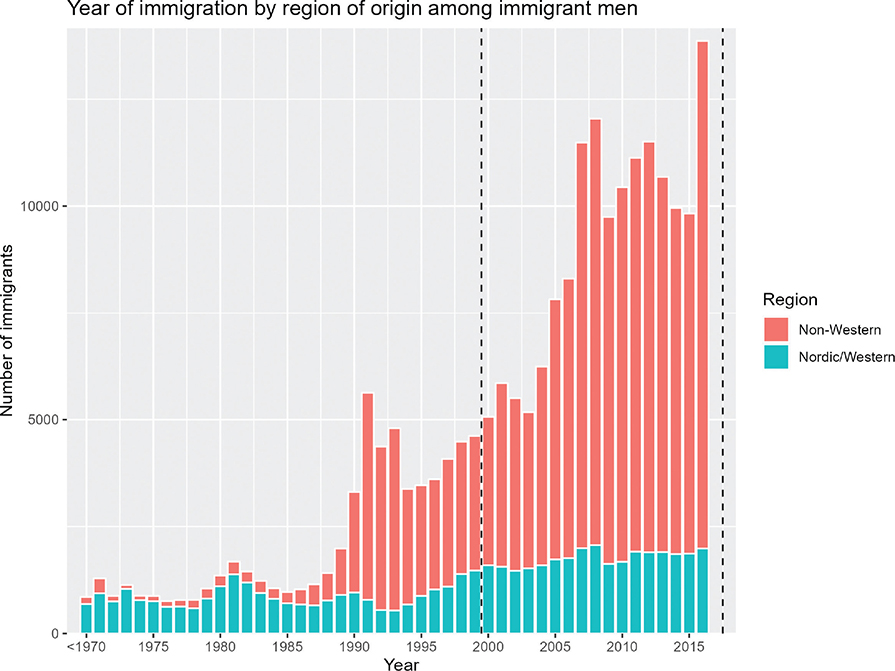
Figure 1. Number of male immigrants by year of immigration. Dotted lines show the follow-up period.
Immigrants were divided into the groups, non-Western and Western. The non-Western group was pooled from more specific subgroups of Central and South Asia, East Asia and Pacific, Latin America and Caribbean, Middle East and North Africa, Eastern Europe, and sub-Saharan Africa. The Western group came from the subgroups: Nordic and Western. A complete list of which countries of origin of the immigrant men were classified into which subgroups for analysis can be found in the Supplementary Material.
For immigrants, we aggregated individual data on cancer diagnoses, cancer deaths, and follow-up time by 10-year age group, 10-year calendar period, and region of birth. The data on PCa diagnoses and deaths of the men born in Finland were aggregated by the same age groups and calendar periods.
We did not have individual level follow-up data on men born in Finland, and thus we approximated their person-years (pyrs) by subtracting immigrants’ pyrs from the annual mean population counts for each year of the study period obtained from Statistics Finland.
An immigrant was excluded from the data if his date of birth was missing, he was aged more than 90, his follow-up ended before 2000, or he had stayed in Finland for less than a year (Figure 2). Thus, out of 183,118 non-Western immigrants, 162,844, and out of 87,389 Western immigrants, 56,127 were included after these exclusions. In total, 20,274 (11.1%) and 31,262 (35.8%) were excluded, respectively.
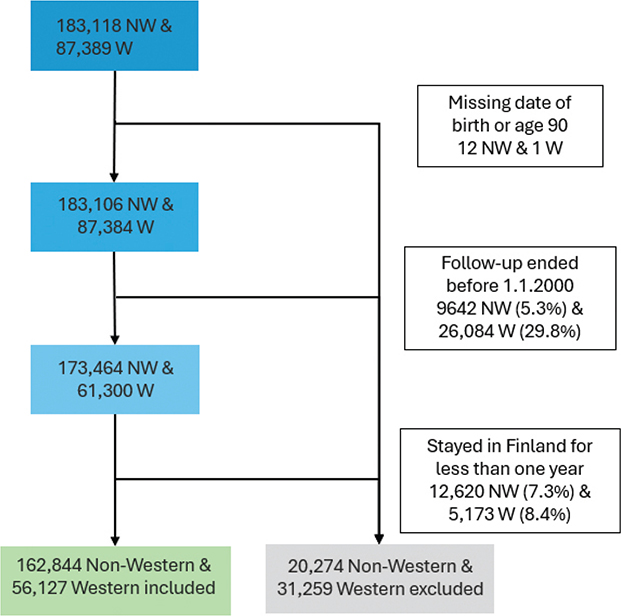
Figure 2. The formulation of the study population of non-Western (NW) and Western (W) immigrants in Finland in 2000–2017. Individuals were excluded from the study population on the following grounds: 1. Missing date of birth, 2. age 90 or older, 3. follow-up ended before 1.1.2000, and 4. stayed in Finland for less than a year. Percentages are shown for those >1%.
If the individual had immigrated to Finland before the year 2000, his follow-up began on January 1st, 2000. Otherwise, his follow-up began at immigration. An individual’s follow-up was ended at death, emigration from Finland, or age 90, whichever occurred first. For the incidence analysis, follow-up ended also at the time of PCa diagnosis.
We used a multivariate Poisson regression model to compare 10-year age- and calendar-specific incidence and mortality between the immigrants and the men born in Finland. These analyses were adjusted for the region of origin, age group and calendar period. These calculations were also done separately for both the Western and the non-Western groups. In addition, we also studied the trend between the categories. All data processing and analyses were performed using the R program version 4.3.2.
We report the results by RRs with their 95% confidence intervals (CI) (shown in parenthesis). Among immigrants, we calculated how the RR of being diagnosed and dying of PCa changed by the duration of residence and the immigration age. To do this, we grouped the cases and the deaths into the categories 1–9, 10–19, and 20+ years for the duration of residence, and into 1–19, 20–29, 30–39, and 40+ years for the immigration age.
Results
In our study population of 56,127 Western and 162,844 non-Western immigrant men, there were roughly 0.5 million pyrs in the Western and 1.4 million pyrs in the non-Western group. In terms of pyrs, the Western group was divided into equally sized subgroups, Nordic and other Western. However, in the non-Western group, the subgroup Eastern Europe dominated over the five other subgroups, and Latin America and Caribbean stood out as insignificant to the whole. The other subgroups were comparatively equal in sizes (Table 1). Baseline descriptives of the study populations are provided in Table 2.
Among men born in Finland, there were 81,363 PCa cases and 13,484 deaths. In the non-Western immigrant group, there were 536 cases and 82 deaths, and in the Western immigrants, 318 cases and 38 deaths (Table 3).
Compared to the men born in Finland, the incidence of PCa was significantly lower in non-Western men: an adjusted RR of 0.66 (0.61–0.72) was observed. The RR of the mortality from PCa was 0.80 (0.65–1.00) (Table 3). In the Western group, the incidence was also lower than in the men born in Finland (0.88, 0.78–0.98). However, the mortality RR in Western men, based on a rather small number of observations, was statistically insignificant (0.78, 0.57–1.11).
In the non-Western group, a majority of both cases (77.2%) and deaths (86.6%) came from the subgroup Eastern Europe. Conversely, RRs for cases were strikingly low across all Asian subgroups. There were next to no deaths in subgroups other than Eastern Europe. A complete table of the absolute figures for all subgroups can be found in Supplementary Table 1.
We also found that for non-Western immigrants, the likelihood of being diagnosed with PCa was greatest if the duration of residence was 20 years or longer (Table 4). Additionally, we found that the risk of being diagnosed with PCa was inversely proportional to age at immigration for non-Western immigrants: the younger the immigrant was at immigration, the greater his risk of PCa. Neither of these findings were seen in the Western immigrant group. Similar figures of deaths cannot be reported due to the small number of them.
Discussion
Our study sought to find possible differences in the relative incidence of and mortality from PCa between men born in Finland and immigrant men. We found that the incidence of PCa is lower in non-Western immigrants than in the men born in Finland. For the non-Western immigrants, we found a lower incidence compared to men born in Finland. Our result for the mortality from PCa seems to also be lower than that of the men born in Finland. However, caution must be used in interpreting this finding, as the CI is broad (RR = 0.80, CI = 0.65–1.00). In Western immigrants, the incidence of PCa was lower than the men born in Finland, but no statistically significant difference was observed for PCa mortality in this group.
PCa often remains latent without causing a clinically significant disease during the patient’s lifetime [19]. Because of widespread opportunistic PSA testing, overdiagnosis is common and causes undue anxiety for patients [20]. Testing varies greatly due to differences in accessibility of healthcare and even clinical practices [10, 21], which can be seen in PCa incidences between different countries. For example, Estonia’s high PCa incidence is largely explainable by the largescale opportunistic PSA testing employed by clinicians [21].
Northern European countries generally have high incidence rates, and Finland is no exception [22]. This is due to either increased risk of PCa, pervasive overdiagnosis, or both. Overdiagnosis among men born in Finland may help to explain the differences we observed: diagnoses of clinically insignificant cancers would inflate the perceived incidence of PCa. It can be hypothesized that immigrants might be subject to this less due to a lower utilization of healthcare [7], leading to fewer diagnosed PCa cases.
We found that Western immigrants had a higher incidence than non-Westerners, which is congruent with other studies’ findings [17, 23]. Literature shows that cultural similarities between the host population and immigrant groups may predict less inequality in healthcare [24]. Thus, it is reasonable to theorize that if overdiagnosis of PCa is associated with the utilization of healthcare, it could in part explain this observation. Still, other factors must be considered as well [25].
For a disease as common as PCa, surprisingly little is known of its risk factors. Advanced age and a family history are known to be important non-modifiable risk factors [12]. Many modifiable risk factors have been proposed, but only a handful have been widely accepted as certain. Often cited ones include meat consumption, dietary inflammation index, and trans fatty acid intake. Plentiful soy consumption and exercise are known to be protective factors [26, 27]. Indeed, the Western lifestyle has been linked to increased risk of prostate cancer, which may in part explain the lower incidence in non-Western immigrants compared to both the men born in Finland and Western immigrants seen in our study.
Our results show that non-Western immigrants had a lower risk of diagnosis than the men born in Finland. This may be explained by a worse socioeconomic position [1], lacking knowledge of available services [6], and barriers in communication between healthcare professionals and patients [4].
Our finding of a positive association between long duration of residence and young age at immigration and higher RR of diagnosis in non-Western men is consistent with a Swedish study [28]. The same study also demonstrates the effect of integration into society on PCa risk in immigrants. Another Swedish paper concludes that a young age at immigration predicts better social integration [29]. Therefore, it can be interpreted that young immigrants adjust well to the culture and lifestyle of the host country, which results in epidemiological findings similar to the Finnish-born population.
It can be assumed that immigrants who live in Finland longer are exposed to environmental and lifestyle-related risk factors for longer. The fact that we did not see similar effects in the Western immigrants’ RRs supports the theory that cultural differences are less of an obstacle for them, and that they are exposed to the same risk factors associated with the Western lifestyle as the men born in Finland in our study even before immigration. These findings on the effect of age at immigration and duration of residence are supported by literature [23].
Our findings are congruent with the literature in demonstrating a lower PCa risk in non-Western immigrants [30]. However, non-Western immigrants are a highly heterogenous group which includes people from all over the world and from many different backgrounds. This diversity is well demonstrated also in our results, with Asians standing out with very low RRs for cases, and conversely Eastern Europeans and sub-Saharan Africans having an above average RR for cases among the non-Western subgroups. These results are to be expected based on epidemiological [9] and genetic studies [25].
In our study, the majority of the non-Western cases and deaths came from the subgroup Eastern European. This overrepresentation is partially explained by the small study populations in other non-Western subgroups, but it also has basis in literature: the finding of an above average risk of PCa in Eastern Europeans compared to other non-Western immigrants is consistent with a Norwegian study [17].
Concerningly, another Norwegian study also found a worse survival of PCa among Eastern European immigrants [31], while other studies have found ambiguous results in the incidence of PCa [30]. Our study does not unambiguously demonstrate a worse PCa survival in immigrants, but it is possible in non-Western immigrants, and it is clear that these immigrants do not survive their cancers better than the men born in Finland. Further research should be conducted into this matter in the future.
A major strength of our study is the quality of our data. The register-data we utilized are reliable, and the data from the FCR are comprehensive even with its follow-ups [32]. However, we were not able to assess the potential effect of opportunistic PSA testing via the stage of PCa since the stage classification adapted by the FCR is unfortunately too crude for that purpose.
Our study was limited by the number of observations of both immigrant PCa cases and deaths, due to the low number of immigrants in Finland and the relative youth of this population. While the stark differences in the age distributions of men born in Finland [33] and immigrant men did not affect our results due to adjustment for age group, the low amount of elderly immigrants decreased the number of observations in these groups, since PCa is typically diagnosed late in life [34]. Individual-level data on Finnish men were unavailable to us and as such we utilized aggregate data. This may have affected our data to a small degree, but this is likely a marginal issue and does not impact our results.
We were unable to reliably determine the effect of duration of residence and age at immigration on the mortality from PCa, mainly due to the small number of deaths on record. Additionally, in the case of age at immigration, meaningful analysis was impossible because nearly all of the deaths occur in the oldest age group. This is likely because the men who immigrated at a younger age have not yet reached an age at which PCa mortality is observed, as few immigrated into Finland before the year 1990 (Figure 1).
Encouragingly, our results indicate that immigrants are at a lower risk of both incidence of and mortality from PCa compared to the men born in Finland. However, our findings do not rule out a worse PCa survival among non-Western immigrants, especially Eastern European ones which has been observed in Norway [31]. This may be due to factors such as immigrants’ cancers being detected at a later stage [35]. Further research is needed into this possibility, for example by comparing the survival from similar grade cancers between immigrants and men born in Finland.
Acknowledgments
This research received no external funding. The authors would like to thank Eetu Mäkinen from the Finnish Cancer Registry for his input and support throughout this study process.
Data availability statement
Aggregated data are available from the corresponding author upon reasonable request. Due to data protection regulations, the register data are not openly shared. Permission for the dataset can be applied for from Findata (https://findata.fi/en/permits/).
Ethics declarations and trial registry information
All phases of the study were conducted in accordance with relevant guidelines and regulations in Finland. All administrative permissions to access the raw data used in the study were applied and granted according to the European Union’s General Data Protection Regulation (article 30). The data were used in accordance with the Act on the National Institute of Health and Welfare (668/2008) and based on authorizations (VRK VRK/3059/2018-2 and THL/1081/6.02.00/2018) granted under the Act on Secondary Use of Health and Social Data (552/2019).
Authors’ contributions
Katja Mustonen: conceptualization, visualization, writing – original draft, writing – reviewing and editing.
Maarit Lamminmäki: conceptualization, project administration, visualization, writing – reviewing and editing.
Tytti Sarkeala: conceptualization, supervision, writing – reviewing and editing.
Sirpa Heinävaara: formal analysis, methodology, supervision, writing – reviewing and editing.
References
[1] Poverty and social exclusion of migrants in the European Union – Publications – European Centre for Social Welfare Policy and Research [Internet]. [cited 2024 Jul 25]. Available from: https://www.euro.centre.org/publications/detail/396
[2] Dalton SO, Schüz J, Engholm G, Johansen C, Kjaer SK, Steding-Jessen M, et al. Social inequality in incidence of and survival from cancer in a population-based study in Denmark, 1994–2003: summary of findings. Eur J Cancer. 2008 Sep;44(14):2074–85. https://doi.org/10.1016/j.ejca.2008.06.018
[3] infoFinland.fi. Health services in Finland. 2025 [cited 2025 Jun 2]. Available from: https://www.infofinland.fi/en/health/health-services-in-finland
[4] Ahmed S, Lee S, Shommu N, Rumana N, Turin T. Experiences of communication barriers between physicians and immigrant patients: a systematic review and thematic synthesis. Patient Exp J. 2017 Apr 24;4(1):122–40. https://doi.org/10.35680/2372-0247.1181
[5] Gil-Salmerón A, Katsas K, Riza E, Karnaki P, Linos A. Access to healthcare for migrant patients in Europe: healthcare discrimination and translation services. IJERPH. 2021 Jul 26;18(15):7901. https://doi.org/10.3390/ijerph18157901
[6] Ulkomaalaistaustaisten terveys ja hyvinvointi Suomessa FinMonik-tutkimus 2018–2019. (Health and well-being of people with a foreign background in Finland. FinMonik study 2018–2019). Eds Kuusio H, Seppänen A, Jokela A, Somersalo A, Linja E. THL, 2020. https://www.julkari.fi/handle/10024/139210.
[7] Sarría-Santamera A, Hijas-Gómez AI, Carmona R, Gimeno-Feliú LA. A systematic review of the use of health services by immigrants and native populations. Public Health Rev. 2016 Dec;37(1):28. https://doi.org/10.1186/s40985-016-0042-3
[8] Official Statistics of Finland (OSF). Population structure. Statistics of Finland population structure database. [cited 2025 Jun 2]. Available from: https://stat.fi/en/statistics/vaerak
[9] Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J Clin. 2021 May;71(3):209–49. https://doi.org/10.3322/caac.21660
[10] Zhou CK, Check DP, Lortet‐Tieulent J, Laversanne M, Jemal A, Ferlay J, et al. Prostate cancer incidence in 43 populations worldwide: an analysis of time trends overall and by age group. Int J Cancer. 2016 Mar 15;138(6):1388–400. https://doi.org/10.1002/ijc.29894
[11] Beyer K, Leenen R, Venderbos LDF, Helleman J, Denijs F, Bramer W, et al. Health policy for prostate cancer early detection in the European Union and the impact of opportunistic screening: PRAISE-U Consortium. J Pers Med. 2024 Jan 11;14(1):84. https://doi.org/10.3390/jpm14010084
[12] Bergengren O, Pekala KR, Matsoukas K, Fainberg J, Mungovan SF, Bratt O, et al. 2022 Update on prostate cancer epidemiology and risk factors – a systematic review. Eur Urol. 2023 Aug;84(2):191–206. https://doi.org/10.1016/j.eururo.2023.04.021
[13] United Nations Department of Economic and Social Affairs. World Social Report 2023: leaving no one behind in an ageing world. World Social Report. United Nations; 2023 [cited 2024 Jul 28]. Available from: https://www.un-ilibrary.org/content/books/9789210019682
[14] Abraído-Lanza AF, Dohrenwend BP, Ng-Mak DS, Turner JB. The Latino mortality paradox: a test of the ‘salmon bias’ and healthy migrant hypotheses. Am J Public Health. 1999 Oct;89(10):1543–8. https://doi.org/10.2105/AJPH.89.10.1543
[15] Place V, Nabb B, Viksten Assel K, Bäärnhielm S, Dalman C, Hollander AC. Interventions to increase migrants’ care-seeking behaviour for stigmatised conditions: a scoping review. Soc Psychiatry Psychiatr Epidemiol. 2021 Jun;56(6):913–30. https://doi.org/10.1007/s00127-021-02065-1
[16] Vonneilich N, Bremer D, Von Dem Knesebeck O, Lüdecke D. Health patterns among migrant and non-migrant middle- and older-aged individuals in Europe – analyses based on share 2004–2017. Int J Environ Res Public Health. 2021 Nov 16;18(22):12047. https://doi.org/10.3390/ijerph182212047
[17] Hjerkind KV, Qureshi SA, Møller B, Weiderpass E, Deapen D, Kumar B, et al. Ethnic differences in the incidence of cancer in Norway. Int J Cancer. 2017 Apr 15;140(8):1770–80. https://doi.org/10.1002/ijc.30598
[18] Mousavi SM, Sundquist K, Hemminki K. Morbidity and mortality in gynecological cancers among first‐ and second‐generation immigrants in Sweden. Int J Cancer. 2012 Jul 15;131(2):497–504. https://doi.org/10.1002/ijc.26395
[19] Draisma G, Boer R, Otto SJ, van der Cruijsen IW, Damhuis RAM, Schröder FH, et al. Lead times and overdetection due to prostate-specific antigen screening: estimates from the European Randomized Study of Screening for Prostate Cancer. J Natl Cancer Inst. 2003 Jun 18;95(12):868–78. https://doi.org/10.1093/jnci/95.12.868
[20] Ilic D, Neuberger MM, Djulbegovic M, Dahm P. Screening for prostate cancer. Cochrane Database Syst Rev. 2013;2013(1):CD004720. https://doi.org/10.1002/14651858.CD004720.pub3
[21] Innos K, Baburin A, Kotsar A, Eiche IE, Lang K. Prostate cancer incidence, mortality and survival trends in Estonia, 1995–2014. Scand J Urol. 2017 Dec;51(6):442–9. https://doi.org/10.1080/21681805.2017.1392600
[22] Dyba T, Randi G, Bray F, Martos C, Giusti F, Nicholson N, et al. The European cancer burden in 2020: incidence and mortality estimates for 40 countries and 25 major cancers. Eur J Cancer. 2021 Nov;157:308–47. https://doi.org/10.1016/j.ejca.2021.07.039
[23] Loeb S, Drevin L, Robinson D, Holmberg E, Carlsson S, Lambe M, et al. Risk of localized and advanced prostate cancer among immigrants versus native-born Swedish men: a nation-wide, population-based study. Cancer Causes Control. 2013 Feb;24(2):383–90. https://doi.org/10.1007/s10552-012-0124-6
[24] Tzogiou C, Boes S, Brunner B. What explains the inequalities in health care utilization between immigrants and non-migrants in Switzerland? BMC Public Health. 2021 Mar 18;21(1):530. https://doi.org/10.1186/s12889-021-10393-9
[25] Wang G, Zhao D, Spring DJ, DePinho RA. Genetics and biology of prostate cancer. Genes Dev. 2018 Sep 1;32(17–18):1105–40. https://doi.org/10.1101/gad.315739.118
[26] Kolonel LN, Hankin JH, Whittemore AS, Wu AH, Gallagher RP, Wilkens LR, et al. Vegetables, fruits, legumes and prostate cancer: a multiethnic case-control study. Cancer Epidemiol Biomarkers Prev. 2000 Aug;9(8):795–804.
[27] Torti DC, Matheson GO. Exercise and prostate cancer. Sports Med. 2004 May 1;34(6):363–9. https://doi.org/10.2165/00007256-200434060-00003
[28] Beiki O, Ekbom A, Allebeck P, Moradi T. Risk of prostate cancer among Swedish-born and foreign-born men in Sweden, 1961–2004. Int J Cancer. 2009 Apr 15;124(8):1941–53. https://doi.org/10.1002/ijc.24138
[29] Age at migration and social integration [Internet]. [cited 2024 Jul 22]. Available from: https://www.iza.org/publications/dp/4263/age-at-migration-and-social-integration
[30] Arnold M, Razum O, Coebergh JW. Cancer risk diversity in non-western migrants to Europe: an overview of the literature. Eur J Cancer. 2010 Sep;46(14):2647–59. https://doi.org/10.1016/j.ejca.2010.07.050
[31] Thøgersen H, Møller B, Robsahm TE, Babigumira R, Aaserud S, Larsen IK. Differences in cancer survival between immigrants in Norway and the host population. Int J Cancer. 2018 Dec 15;143(12):3097–105. https://doi.org/10.1002/ijc.31729
[32] Leinonen MK, Miettinen J, Heikkinen S, Pitkäniemi J, Malila N. Quality measures of the population-based Finnish Cancer Registry indicate sound data quality for solid malignant tumours. Eur J Cancer. 2017 May 1;77:31–9. https://doi.org/10.1016/j.ejca.2017.02.017
[33] Tilastokeskus. Statistics Finland; [cited 2024 Jul 25]. Available from: https://stat.fi/tup/suoluk/suoluk_vaesto_en.html
[34] Key statistics for prostate cancer. Prostate cancer facts [Internet]. [cited 2024 Jul 24]. Available from: https://www.cancer.org/cancer/types/prostate-cancer/about/key-statistics.html
[35] Coughlin SS. A review of social determinants of prostate cancer risk, stage, and survival. Prostate Int. 2020 Jun;8(2):49–54. https://doi.org/10.1016/j.prnil.2019.08.001