ORIGINAL ARTICLE
Validated prediction of xerostomia in a real-world population: a step toward model-guided radiotherapy
Emmy Dalqvista,b  , Tiziana Rancatic , Anna Embringa,d , Gabriella Alexandersson von Döbelnd,e, Ingmar Laxa,f, Signe Frieslanda,f and Eva Onjukkaa,b
, Tiziana Rancatic , Anna Embringa,d , Gabriella Alexandersson von Döbelnd,e, Ingmar Laxa,f, Signe Frieslanda,f and Eva Onjukkaa,b
aDepartment of Oncology Pathology, Karolinska Institutet, Stockholm, Sweden; bDepartment of Nuclear Medicine and Medical Physics, Karolinska University Hospital, Stockholm, Sweden; cData Science Unit, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy; dDepartment of Radiotherapy, Karolinska University Hospital, Stockholm, Sweden; eDepartment of Clinical Science, Intervention and Technology, Karolinska Institutet, Stockholm, Sweden; fDepartment of Head, Neck, Lung and Skin Tumors, Karolinska University Hospital, Stockholm, Sweden
ABSTRACT
Background and purpose: The aim of this study is to validate an Normal Tissue Complication Probability (NTCP) model for xerostomia in a large quality-registry cohort, enabling its future use in individualized NTCP-based treatment planning.
Material and methods: A model predicting grade ≥ 2 xerostomia (6 months post-radiotherapy) was selected for validation, including the mean dose to both the parotid and the submandibular glands, in addition to the baseline score for xerostomia, as predictors. Our local validation cohort consisted of 674 patients (204 events), treated between 2012 and 2024, with a median follow-up of 10.3 months (range 5–24). A closed testing procedure was performed to investigate the need for model updating, and the performance of the models was assessed with calibration curves, discrimination, the Brier score, and the Hosmer-Lemeshow test.
Results: The calibration curve demonstrated that the model predicted the dose–response relationship well. The validation cohort showed a slightly stronger dose response, with a slope of 1.16. The calibration intercept of −0.12 revealed an overestimation of xerostomia.
However, the closed testing procedure indicated that a recalibration of the model was needed, and the HL-test showed a significant deviation. The recalibrated model showed perfect calibration but still limited discrimination (Area Under the Curve (AUC) 0.62).
Conclusion: The validated model performed well in our real-life dataset despite the differences between the training and validation cohorts, particularly considering the lack of baseline score in our cohort. This highlights the potential for improved performance with baseline inclusion but still suggests that an individualized NTCP-based treatment-planning protocol can be developed using the recalibrated published model.
KEYWORDS: external validation; xerostomia; head and neck cancer; dose–response relationship; normal tissue complication probability; radiation therapy
Citation: ACTA ONCOLOGICA 2025, VOL. 64, 1087–1094. https://doi.org/10.2340/1651-226X.2025.43462.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Oncologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Received: 1 May 2025; Accepted: 31 July 2025; Published: 18 August 2025
CONTACT: Emmy Dalqvist emmy.dalqvist@ki.se Department of Oncology Pathology, Karolinska Institutet, Stockholm, Sweden; Department of Nuclear Medicine and Medical Physics, Karolinska University Hospital, Anna Stackséns gata 45, Solna, Sweden
Competing interests and funding: This study was funded by a research grant from Varian/Siemens Healthineers Int. AG. EO’s contribution was funded by a fellowship from the Swedish Cancer Society.
Introduction
Xerostomia, or dry mouth, is a common and debilitating side effect of head and neck radiotherapy, resulting from radiation-induced damage to the salivary glands and significantly reducing patients’ quality of life [1]. The relationship between radiation dose and xerostomia has been extensively studied using Normal Tissue Complication Probability (NTCP) models [2–8]. Historically, these models have primarily focused on the mean dose to the parotid glands [3, 7, 8]. However, more recent studies have also incorporated the submandibular glands [9, 10] and the minor salivary glands within the oral cavity [2]. When modeling xerostomia, previous research has highlighted the importance of accounting for baseline patient characteristics, which is evaluated before treatment [2, 3]. Evidence suggests that non-dosimetric factors also influence the risk of xerostomia; for example, age and concomitant chemotherapy [3, 6] have been identified as important contributors. Technological advancements have further propelled progress in the field by incorporating radiomic features [11], spatial information [12, 13], and other features of the 3D dose-distribution [10, 14] to improve the predictive accuracy of NTCP models for xerostomia. While these developments significantly enhance our understanding of the multifactorial mechanisms underlying the occurrence of side effects on an individual basis, their integration into routine clinical workflows remains challenging. Despite these advancements, many clinical practices continue to rely on non-individualized dose constraints, such as point doses or dose-volume histogram (DVH) metrics, rather than adopting the NTCP-based dose reporting to organs at risk (OAR), as recommended by the International Commission on Radiation Units and Measurements (ICRU) [15]. Therefore, the validation of NTCP models that are more readily implementable in a clinical setting is the key to a more evidence-based treatment-planning approach.
The Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) statement [16] is widely used for reporting model development or evaluation, but it does not outline specific methodologies for these tasks. A systematic review from Sharabiani et al. [17] highlighted that only a limited number of studies on NTCP models for head and neck toxicities have been subject to external validation. External validation is necessary to assess a model’s reproducibility and generalizability, which are critical concerns when relying on the model for decision support in clinical practice. Many researchers have emphasized the importance of external validation [17, 18], and several methodological frameworks have been published in recent years [18–22]. The focus should now be placed on validation studies to prove the validity of preexisting models.
Van den Bosch et al. [2] have identified individual toxicity risk profiles for head and neck treatments and developed models for xerostomia and dysphagia at multiple time points after treatment. The national Dutch protocol by Langendijk et al. [23] refined these models through recalibration, using a combined cohort of 1145 patients, achieving the level of a TRIPOD type 4a model. This model is currently used in the Netherlands to allocate patients to proton or photon treatments, based on the estimated benefit [24]. In Sweden, patient selection for proton therapy is based on a consensus-driven approach. The aim of this validation is not to challenge the current national strategy but rather to pave the way for an alternative clinical application of NTCP models. Specifically, models may support personalized treatment planning by allowing dose prescription to be tailored according to individual anatomical characteristics and the associated personal risk of side effects.
Since 2014, acute and late side-effects after radiotherapy have been systematically recorded in a local quality registry for head and neck cancer at the Karolinska University Hospital. The current study aims to externally validate the NTCP model for grade ≥ 2 xerostomia from the national Dutch protocol within a suitable subgroup of this registry. The objective is to assess the generalizability of the model to our clinical patient cohort, with the potential future use of iso-NTCP prescription to optimize treatment outcomes while maintaining an acceptable toxicity profile.
Material and methods
The model for xerostomia of grade ≥ 2 (6 months post-radiotherapy) from the Dutch National Indication Protocol for Proton Therapy [23] was selected for validation (hereafter referred to as the LIPP model).
Patient selection
A validation cohort was extracted from the local quality registry for head and neck cancer at the Karolinska University Hospital. Details of the registry have been described previously by Onjukka et al. [4]. The inclusion criteria for the current cohort were as follows: treatment between 2012 and 2024 with a follow-up time between 5 months and 2 years; the parotid- and submandibular glands contoured as part of clinical routine; curative intent (i.e. prescribed dose ≥ 50 Gy); and tumor location in the proximity of the salivary glands, including cancer of the oral cavity, oropharynx, nasopharynx, hypopharynx, oral cavity, larynx, or other sites (nasal cavity, paranasal sinuses, or metastases in the neck with an unknown primary). Patients who received plan adaptation during the radiotherapy course were excluded due to the risk of anatomical changes leading to considerable uncertainty in the accumulated dose to the evaluated OAR. Similarly, patients who received reirradiation or a brachytherapy boost were also excluded. Dose-volume histograms (DVHs) for the parotid and the submandibular glands were extracted from the Eclipse treatment-planning system (Varian, USA) using a locally developed script.
Treatment
All patients received high-dose radiotherapy with a curative intent, 50 to 84 Gy in 17 to 35 fractions, alone or with induction chemotherapy and/or concomitant medical therapy (chemotherapy or targeted therapy). The predominant treatment approach was the simultaneous integrated boost (SIB) technique (since 2016). In 2020, the consensus guidelines from Grégoire et al. [25] including the 5 + 5-mm clinical target volume (CTV) expansion were implemented, with 68 Gy in 34 fractions to the gross tumor volume (GTV), 61.2 Gy to CTV_68 + 5 mm, and 51.68 Gy to the elective volume. Previously, the 68 Gy CTV included the GTV with a 10-mm margin, while the elective CTV was unchanged (meaning only two prescription levels were used). The parotid and the submandibular glands were delineated based on their appearance in the CT image. Knowledge-based auto-planning (RapidPlan: Varian Medical Systems, Palo Alto, USA) was used from 2019.
Xerostomia endpoint
The modeled toxicity endpoint was late xerostomia of grade ≥ 2 (moderate-to-severe xerostomia), assessed by clinicians according to the RTOG/EORTC Radiation Morbidity Scales [26]. As the registry consists of real-world data, the follow-up time is not consistently at 6 months post-radiotherapy, as for the LIPP cohort. The number of follow-up assessments registered for each patient varied across the cohort. Where multiple assessments were available, the follow-up nearest 6 months was selected but limited to a maximum of 2 years (as per the inclusion criteria). This study was approved by the regional ethics committee (2016/268-31/1).
Statistical analysis
Reference model
Van den Bosch et al. developed a model on the prospective CITOR cohort with data from the University Medical Centre Groningen (UMCG) in the Netherlands (750), validated on data from UMCG, the Maastro Clinic, and the Radiotherapeutic Institute Friesland (RIF) (395) [2]. The latest version of the LIPP model (version 2.2) represents an updated and recalibrated version of the Van den Bosch model, developed using a combined cohort of 1145 patients [23]. Model refinement was conducted using a closed testing procedure [27]. In the combined cohort, the prevalence of the endpoint was 46%, assessed via the EORTC QLQ-H&N35 questionnaire. The model incorporates the mean dose to both the parotid (ipsilateral [ips] parotid and contralateral [con] parotid) and the submandibular (SMG) glands, in addition to the baseline score for xerostomia.
NTCPLIPP = (1+e-S)-1
where:
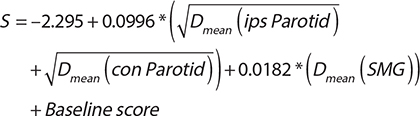
The baseline score was 0 for none, 0.459 for mild, and 1.207 for moderate to severe xerostomia, at baseline.
Validation procedure
Possible differences between the current cohort and the LIPP cohort were evaluated using a chi-square test for categorical values and a t-test for continuous values, setting the significance threshold at p < 0.05. Specifically, the following patient and treatment characteristics were considered: sex, age, tumor site, human papillomavirus (HPV) status (for patients with oropharyngeal cancer), concomitant medical treatments, induction chemotherapy, radiotherapy schedule, radiotherapy technique, xerostomia rate, and the mean physical doses to the parotid and the submandibular glands.
In the validation cohort of the current study, baseline data were only available for a minority of the patients (around 15%), and a baseline score of zero was assumed for all patients. The closed testing procedure [27] was employed to evaluate the necessity for model updates, considering three potential approaches: calibration-in-the-large (re-estimation of the model intercept), recalibration (re-estimation of both the intercept and slope), and model revision (re-estimation of all model coefficients). Based on the results of the closed testing procedure, the appropriate updates were applied to optimize the model’s predictive performance and ensure its suitability for clinical application.
The model performance was assessed by calibration and discrimination metrics. A calibration curve was generated to visually compare the predicted versus observed probabilities of xerostomia grade ≥ 2. The calibration was evaluated using calibration-in-the-large, calibration intercept and slope, together with the Brier score and the Hosmer-Lemeshow (HL) goodness-of-fit test. The discrimination was tested using the area under the receiver operating characteristic curve (AUC). The clinical usefulness of the model was analyzed using the net benefit [28, 29] metric. A detailed description of this approach is provided in the Supplementary Materials.
MATLAB (version R2019a) was used for all statistical analyses, and all DVHs were converted to equivalent dose in 2 Gy per fraction (EQD2) using the linear-quadratic model, with α/β = 3 Gy.
Results
Cohort characteristics
At the time of this analysis, the registry comprised 2366 patients. Out of these, 840 patients fulfilled the inclusion criteria. After excluding 61 patients who received plan adaptation, 34 patients who received brachy boost, and 71 patients who were reirradiated, 674 patients remained for the analysis (Figure 1). A search in the clinical database for the two largest tumor sites (tonsil and base of tongue), from 2012 to 2019, identified 890 treated cases, of which 524 (59%) were included in the registry, demonstrating the representativeness of the registry population.
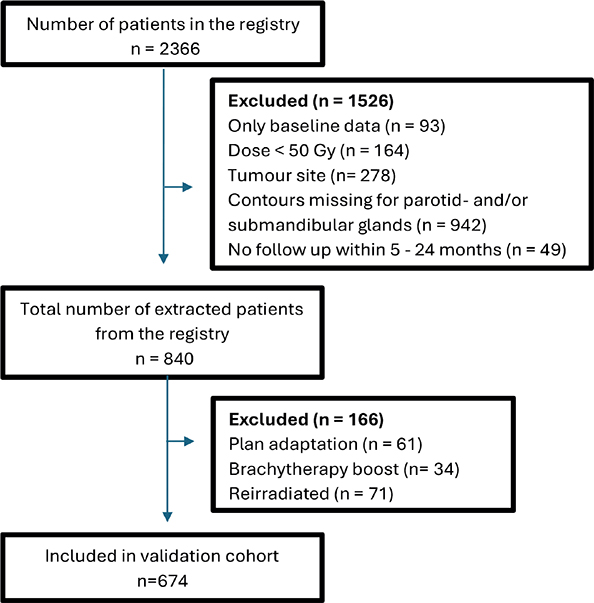
Figure 1. Flow chart of patient exclusion of the KUH cohort. The number of excluded patients prior to data extraction from the registry is presented in the order in which the exclusion criteria were applied, as overlaps between criteria may occur.
The resulting cohort had a median follow-up of 10.3 months (range 5–24), and the prevalence of grade ≥ 2 xerostomia was 30%. The cohort was treated over different time periods: 16% of patients received treatment between 2012 and 2016, 36% between 2017 and 2019, and 48% between 2020 and 2024. In the earliest time period, the submandibular glands were not systematically delineated in clinical practice, leading to a greater proportion of patients being excluded from the analysis compared to the more recent time periods. Patient characteristics are described in Table 1 together with the corresponding values in the development cohort. A significant difference can be seen between the two cohorts for tumor site, concomitant/induction medical treatment, prescribed treatment, treatment technique, xerostomia prevalence, and mean doses to OAR. The oropharynx was the dominant tumor site in our cohort (76%), whereas the larynx (44%) was the most common site in the development cohort. The development cohort also received less concomitant medical treatment and excluded patients with induction chemotherapy. Both the parotid and the submandibular glands received higher doses in the development cohort compared to the validation cohort, with a mean-dose difference of 3.0 Gy and 1.8 Gy for the parotid and the submandibular glands, respectively. In the validation cohort, baseline data were available for only 99 patients. Among these, 83% had no xerostomia, 16% grade-1 xerostomia, and 1% had grade-2 xerostomia before radiotherapy.
| Patient characteristics | KUH (674) | LIPP (1145) | CITOR cohort (750 pat) | Initial validation cohort (395) | p |
| Sex | 0.18 | ||||
| Male | 481 (71%) | 850 (74%) | 560 (75%) | 290 (73%) | |
| Female | 193 (29%) | 295 (26%) | 190 (25%) | 105 (27%) | |
| Age (mean, SD) | 63.0 (10.3) | 63.3 (10.0) | 63 (10.3) | 64 (9.4) | 0.54 |
| Tumor site | < 0.001 | ||||
| Oropharynx | 509 (76%) | 411 (36%) | 271 (36%) | 140 (35%) | |
| Nasopharynx | 20 (3.0%) | 45 (3.9%) | 30 (4.0%) | 15 (3.8%) | |
| Hypopharynx | 33 (4.9%) | 121 (11%) | 71 (9.5%) | 50 (13%) | |
| Larynx | 35 (5.2%) | 502 (44%) | 334 (45%) | 168 (43%) | |
| Oral cavity | 29 (4.3%) | 66 (5.8%) | 44 (5.9%) | 22 (5.6%) | |
| Other | 48 (7.1%) | 0 | 0 | 0 | |
| HPV status (only oropharynx) | - | ||||
| Positive | 466 (92%) | ||||
| Negative | 38 (7.5%) | ||||
| Missing | 5 (1.0%) | ||||
| Concomitant medical treatmentsa | 457b (68%) | 466 (41%) | 242 + 65 (41%) | 134 + 25 (40%) | < 0.001 |
| Induction chemotherapy | 84c (12%) | - | |||
| Prescribed treatmentd | < 0.001 | ||||
| 51–64 Gy in 17–32 fractions | 25 (3.7%) | 20 (1.7%) | 1 (0.1%) | 19 (4.8%) | |
| 66–70 Gy in 33–35 fractions | 593 (88%) | 1118 (98%) | 747 (100%) | 371 (94%) | |
| 71.4–84 Gy in 34–35 fractions | 56 (8.3%) | 7 (0.6%) | 2 (0.3%) | 5 (1.3%) | |
| Treatment technique | < 0.001 | ||||
| VMAT | 668 (99%) | 500 (44%) | 118 (16%) | 382 (97%) | |
| IMRT | - | 553 (48%) | 546 (73%) | 7 (1.8%) | |
| 3D-CRT | 6 (0.9%) | 92 (8.0%) | 86 (11%) | 6 (1.5%) | |
| Xerostomia grade ≥ 2 | 204 (30%) | 531 (46%) | 342 (46%) | 189 (48%) | < 0.001 |
| Median physical mean dose to OAR in Gy (IQR) | |||||
| Parotid ipsilateral | 28.3 (22.4–37.9) | ||||
| Parotid contralateral | 16.2 (11.0–19.6) | ||||
| SMG ipsilateral | 65.2 (59.0–67.6) | ||||
| SMG contralateral | 46.2 (39.6–51.7) | ||||
| Parotid glands | 22.6 (17.6–27.4) | 25.6 (14.4–33.8) | 28.0 (15.9–37.0) | 21.2 (11.5–27.6) | - |
| Submandibular glands | 54.8 (46.3–59.3) | 56.6 (42.2–62.5) | 58.9 (44.6–64.3) | 51.9 (37.5–58.9) | - |
| SD: standard deviation; HPV: human papillomavirus; VMAT: Volumetric Modulated Arc Therapy; IMRT: Intensity Modulated Radiation Therapy; CRT: Conformal Radiation Therapy; OAR: organs at risk; IQR: Interquartile Range; SMG: submandibular. aMedical treatment describes systemic therapy, which, for the validation cohort, was in the form of chemotherapy (51%), targeted therapy (13%), or a combination of both (3.9%). b48% cisplatin, 13% cetuximab, 4% both, or 3% other. cMostly TPF (docetaxel, cisplatin, and fluorouracil) dAssuming 2–2.4 Gy fractions from Van den Bosh et al. [2]. The p-value refers to differences between the KUH and the total LIPP cohort (comparison not possible for the median OAR dose). |
|||||
Validation
The closed testing procedure indicated that the model should be recalibrated, and all the results are summarized in Table 2. Calibration-in-the-large showed a mean predicted risk of 36.2%, while the observed risk was 30.3%, indicating an overestimation of the risk by the model, which was also seen in the calibration intercept of −0.12. The calibration curve (Figure 2) demonstrated a calibration slope of 1.16, indicating a slightly stronger dose response in the validation cohort. A significant difference between predicted and observed xerostomia incidence was identified, as indicated by the HL-test (p = 0.014). After model recalibration, the HL-test indicated no significant lack of fit (p = 0.26), suggesting improved agreement between the predicted and observed outcomes.
| Model parameters and performance | KUH cohort in the LIPP model (validation) | KUH cohort in the recalibrated LIPP model | CITOR + Internal validation cohort in the LIPP model (development) |
| Intercept | −2.2951 | −3.2132 | −2.2951 |
 |
0.0996 | 0.1354 | 0.0996 |
| Dmean (SMG) | 0.0182 | 0.0247 | 0.0182 |
| Log-likelihood | −404 | −398 | - |
| Calibration intercept | −0.12 | 0.00 | 0.00 |
| Calibration slope | 1.16 | 1.00 | 1.00 |
| AUC | 0.62 | 0.62 | 0.72 |
| Hosmer-Lemeshow test p-value | 0.014 | 0.26 | 0.23 |
| Brier score | 0.21 | 0.20 | - |
| AUC: Area Under the Curve. | |||

Figure 2. Calibration curves with the distribution of the true outcome shown at the bottom of the graph. The circles indicate the observed frequencies by deciles of predicted probability, approximately 70 patients in each bin. (A) Calibration curve before updating, with the KUH cohort in the LIPP model. (B) Calibration curve after updating by recalibration, with the KUH cohort in the recalibrated LIPP model.
The model’s discrimination decreased from an AUC of 0.72 in the development cohort to 0.62 in the validation cohort. At an NTCP threshold of 30% (corresponding to our clinical dose constraints), the model showed a sensitivity of 89% and a net benefit of 0.035.
Discussion
An external validation of the xerostomia prediction model, from the Dutch national protocol for indication of proton therapy, was conducted using a cohort of 674 patients from our local quality registry. The model required a small recalibration, which is not surprising, given the different definitions of the endpoint in the development and validation studies. However, the good fit of the recalibrated model indicates that the dose response of the parotid and the submandibular glands is well captured by the model, and that this is robust to a range of differences in cohort characteristics.
The low AUC (0.62) and Brier score (0.21) indicate weak discriminative ability, which limits the model’s accuracy when applied to an individual. Poor discrimination with good calibration may arise from a homogeneous case mix [29, 30], as in our cohort. The range of doses to the parotid and the submandibular glands and, consequently, the range of predicted probabilities were relatively narrow. The omission of the baseline symptoms also inherently reduces the discriminative ability [30]. Since the AUC reflects the performance of the model across the full range of its parameters, in practice, specific thresholds are more relevant for patient risk stratification. For our current clinical dose constraints (mean parotid dose < 25 Gy and mean submandibular gland dose < 39 Gy), the LIPP model estimates a risk of 30% (with no baseline toxicity); at this level of risk, the model shows a fair sensitivity at 89%. Although the calibration intercept and slope indicate a good calibration, the HL-test suggests a weak agreement between the predicted and observed outcomes. However, this test has been questioned due to its sensitivity to sample size and binning choices [18, 19].
A key strength of this study is that the cohort represents a real-world patient population, inspiring confidence in NTCP models for broader clinical application [17]. However, this also introduced one of the main limitations of the validation, as the timepoint for xerostomia assessment varied considerably in our cohort, ranging from 5 to 24 months post-treatment. In contrast, the original model development cohort employed a standardized assessment at 6 months. We chose the 5-to-24-month interval to avoid potential confounding from lingering acute symptoms typically seen up to 5 months, while also capturing clinically meaningful late toxicity, as xerostomia that persists up to 2 years is generally considered stable and chronic. While the primary interest was to apply the model to clinically relevant long-term xerostomia, we nonetheless explored, in a separate analysis, the effect on calibration when restricting the follow-up window to 5–12 months, to more closely mirror the original development cohort. The results remained consistent with those from the full cohort and similarly indicated a need for model recalibration, as demonstrated by a calibration intercept of –0.21 and a calibration slope of 1.48 (data provided in the Supplementary Materials). Hence, the LIPP model seemed at least equally applicable when including follow-up data up to 2 years post-radiotherapy.
The predictive accuracy for our cohort could be improved by incorporating baseline data. However, limiting the testing cohort to patients with recorded baseline data would have significantly reduced the cohort size; only 15% of the patients had baseline data available. The frequency of baseline reporting is improving in the registry, and future studies may be able to validate the impact of baseline xerostomia, provided sufficient event numbers are available for robust statistical analysis. Additionally, the absence of reported baseline xerostomia rate in the original development cohort prevents a direct comparison between the cohorts and verification of the effect size. Still, since baseline xerostomia was not present for the great majority of the patients for whom baseline data were available in our cohort, the current analysis can be considered generally applicable.
The prevalence of grade ≥ 2 xerostomia in our cohort (30%) was lower than in the LIPP cohort (46%); a difference is to be expected since xerostomia was scored according to different scales. Furthermore, differences between the cohorts likely contributed to the observed difference. For example, in our cohort, the median physical mean dose to the parotid glands was 22.6 Gy, compared to 25.6 Gy in the LIPP cohort, while the median mean dose to the submandibular glands was 54.8 Gy versus 56.6 Gy. Additionally, the higher prevalence in the LIPP cohort may be explained by differences in follow-up times, as salivary glands can recover over time [31]. The follow-up time in the validation cohort extended up to 2 years, whereas in the LIPP cohort, it was limited to 6 months. The LIPP cohort (2007–2017) and our validation cohort (2012–2024) span periods marked by considerable progress in radiotherapy and shifts in patient demographics, which can affect model performance [32]. In our clinic, notable developments include the replacement of the sequential boost technique by SIB in 2016, the introduction of RapidPlan optimization in 2019, and the reduction of the GTV-to-CTV margin in 2020 (through the 5+5-mm expansion). We are currently evaluating the impact of the latter two changes on the OAR dose and the rate of side effects, and a manuscript is in preparation. Nevertheless, despite the highlighted differences, we observed a strong correlation between predicted and observed outcomes, which supports the model’s robustness and suggests that it maintains its predictive value even when applied across differing assessment approaches and evolving clinical contexts.
The comprehensive individual toxicity risk (CITRO) profile from Van den Bosch et al. [2], including a xerostomia NTCP model, identified the oral cavity as a relevant OAR in xerostomia modeling, but only in the acute phase. Other NTCP models for xerostomia have similarly reported an association between the oral cavity dose and the xerostomia risk [12, 33, 34]. Furthermore, there is some evidence of the importance of specifically sparing the stem cell region within the salivary glands [34, 35], although this was not confirmed in a recent randomized controlled trial [13]. Proper delineation of this region requires extensive contouring guidelines and MRI for accurate identification.
De Vette et al. [36] have recently validated the CITRO profile of NTCP models from Van den Bosch et al. [2], showing a promising generalizability of the models. They had an excellent calibration close to the identity line (calibration slope ~ 1) for the xerostomia model at 6 months post-radiotherapy but showed some underestimation of the risk with an intercept of 0.43, which may be explained by the difference in side-effect assessment between the cohorts [36].
The validation of the LIPP model demonstrated good overall agreement with our data, with a further improved calibration after recalibration, supporting its applicability for predicting xerostomia in our population. As our registry expands with more baseline data, further refinements may enhance the predictive accuracy and the discrimination. While the model performed well, developing a tailored model trained on our cohort could enable the inclusion of additional predictive factors specific to our patient population, potentially enhancing the performance. Notably, differences in the xerostomia prevalence between our cohort and the LIPP cohort suggest that variations in the radiation dose distributions, follow-up duration, and grading systems may influence model performance. A locally trained model could better account for these variations, leading to an improved discrimination.
With a coverage of the registry of around 60% for the current cohort, the risk of bias needs to be considered when relying on the model in treatment planning. The missing data are expected to predominantly result from logistical challenges during data collection. Patient exclusion likely occurred without systematic bias, suggesting that the incompleteness of the dataset should have minimal impact on the results. However, the missing data will be further characterized in future work and considered in any clinical implementation.
Ultimately, our goal is to ensure validity and maximize clinical utility in the context of NTCP-based treatment planning. Depending on the planning strategy, model calibration to the population of interest may be more or less critical, that is, depending on whether decisions are made based on relative or absolute NTCP estimates. By continuously refining and externally validating predictive models, we can support more personalized and evidence-based radiotherapy strategies, improving the post-treatment quality of life for head and neck cancer patients.
Conclusion
Despite differences in the endpoint definition and the cohort characteristics, our findings demonstrate that the LIPP model exhibits transportability and can be generalized to our real-world data after recalibration, supporting the validity of the Dutch national protocol’s model for radiation-induced xerostomia. While the recalibrated model showed good calibration, its limited discriminative ability suggests the possibility for further refinements to improve individual risk stratification.
In conclusion, our validation suggests that the recalibrated LIPP model is applicable for NTCP-based treatment planning. Further efforts should focus on integrating additional predictive factors to enhance clinical decision-making and improve post-treatment quality of life for head and neck cancer patients.
Acknowledgments
We sincerely thank everyone involved in the patient registration in the quality registry. We would like to acknowledge Claes Mercke for his exceptional efforts in initiating the quality registry facilitating and supporting the research program underlying this study. A special thanks to Erik Almhagen for providing the scripts used for DVH extraction. We also greatly appreciate the team at EpiStat for their valuable discussions and insights.
Data availability statement
The data underlying this study are not publicly available due to ethical constraints. Access to the analysis code may be granted upon reasonable request to the first author.
Ethics declarations & trial registry information
This study was approved by the regional ethics committee (2016/268-31/1).
Author contributions
EO, TR, AE, GAD, and ED contributed to the study design. Data analysis was performed by ED with support from EO, TR, AE, and GAD. The first draft of the manuscript was written by ED with contributions from EO, TR, AE, and GAD. All authors critically reviewed, edited, and approved the final manuscript.
References
[1] Langendijk JA, Doornaert P, Verdonck-de Leeuw IM, Leemans CR, Aaronson NK, Slotman BJ. Impact of late treatment-related toxicity on quality of life among patients with head and neck cancer treated with radiotherapy. J Clin Oncol. 2008;26(22):3770–6. https://doi.org/10.1200/jco.2007.14.6647
[2] Van den Bosch L, van der Schaaf A, van der Laan HP, Hoebers FJP, Wijers OB, van den Hoek JGM, et al. Comprehensive toxicity risk profiling in radiation therapy for head and neck cancer: a new concept for individually optimised treatment. Radiother Oncol. 2021;157:147–54. https://doi.org/10.1016/j.radonc.2021.01.024
[3] Beetz I, Schilstra C, van der Schaaf A, van den Heuvel ER, Doornaert P, van Luijk P, et al. NTCP models for patient-rated xerostomia and sticky saliva after treatment with intensity modulated radiotherapy for head and neck cancer: the role of dosimetric and clinical factors. Radiother Oncol. 2012;105(1):101–6. https://doi.org/10.1016/j.radonc.2012.03.004
[4] Onjukka E, Mercke C, Björgvinsson E, Embring A, Berglund A, Alexandersson von Döbeln G, et al. Modeling of xerostomia after radiotherapy for head and neck cancer: a registry study. Front Oncol. 2020;10:1647. https://doi.org/10.3389/fonc.2020.01647
[5] Lee TF, Liou MH, Huang YJ, Chao PJ, Ting HM, Lee HY, et al. LASSO NTCP predictors for the incidence of xerostomia in patients with head and neck squamous cell carcinoma and nasopharyngeal carcinoma. Sci Rep. 2014;4:6217. https://doi.org/10.1038/srep06217
[6] Beetz I, Steenbakkers RJ, Chouvalova O, Leemans CR, Doornaert P, van der Laan BF, et al. The QUANTEC criteria for parotid gland dose and their efficacy to prevent moderate to severe patient-rated xerostomia. Acta Oncol. 2014;53(5):597–604. https://doi.org/10.3109/0284186x.2013.831186
[7] Lee TF, Fang FM. Quantitative analysis of normal tissue effects in the clinic (QUANTEC) guideline validation using quality of life questionnaire datasets for parotid gland constraints to avoid causing xerostomia during head-and-neck radiotherapy. Radiother Oncol. 2013;106(3):352–8. https://doi.org/10.1016/j.radonc.2012.11.013
[8] Gabryś HS, Buettner F, Sterzing F, Hauswald H, Bangert M. Parotid gland mean dose as a xerostomia predictor in low-dose domains. Acta Oncol. 2017;56(9):1197–203. https://doi.org/10.1080/0284186x.2017.1324209
[9] Hawkins PG, Lee JY, Mao Y, Li P, Green M, Worden FP, et al. Sparing all salivary glands with IMRT for head and neck cancer: longitudinal study of patient-reported xerostomia and head-and-neck quality of life. Radiother Oncol. 2018;126(1):68–74. https://doi.org/10.1016/j.radonc.2017.08.002
[10] Buettner F, Miah AB, Gulliford SL, Hall E, Harrington KJ, Webb S, et al. Novel approaches to improve the therapeutic index of head and neck radiotherapy: an analysis of data from the PARSPORT randomised phase III trial. Radiother Oncol. 2012;103(1):82–7. https://doi.org/10.1016/j.radonc.2012.02.006
[11] van Dijk LV, Noordzij W, Brouwer CL, Boellaard R, Burgerhof JGM, Langendijk JA, et al. (18)F-FDG PET image biomarkers improve prediction of late radiation-induced xerostomia. Radiother Oncol. 2018;126(1):89–95. https://doi.org/10.1016/j.radonc.2017.08.024
[12] van Rijn-Dekker MI, van Luijk P, Schuit E, van der Schaaf A, Langendijk JA, Steenbakkers R. Prediction of radiation-induced parotid gland-related xerostomia in patients with head and neck cancer: regeneration-weighted dose. Int J Radiat Oncol Biol Phys. 2023;117(3):750–62. https://doi.org/10.1016/j.ijrobp.2023.04.034
[13] Steenbakkers R, van Rijn-Dekker MI, Stokman MA, Kierkels RGJ, van der Schaaf A, van den Hoek JGM, et al. Parotid gland stem cell sparing radiation therapy for patients with head and neck cancer: a double-blind randomized controlled trial. Int J Radiat Oncol Biol Phys. 2022;112(2):306–16. https://doi.org/10.1016/j.ijrobp.2021.09.023
[14] Astaburuaga R, Gabryś HS, Sánchez-Nieto B, Floca RO, Klüter S, Schubert K, et al. Incorporation of dosimetric gradients and parotid gland migration into xerostomia prediction. Front Oncol. 2019;9:697. https://doi.org/10.3389/fonc.2019.00697
[15] ICRU. Prescribing, recording, and Reporting Photon-Bean Intensity-Modulated Radiation Therapy (IMRT). ICRU Report 83. J ICRU. 2010;10:27.
[16] Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. Bmj. 2015;350:g7594. https://doi.org/10.1136/bmj.g7594
[17] Sharabiani M, Clementel E, Andratschke N, Hurkmans C. Generalizability assessment of head and neck cancer NTCP models based on the TRIPOD criteria. Radiother Oncol. 2020;146:143–50. https://doi.org/10.1016/j.radonc.2020.02.013
[18] Ramspek CL, Jager KJ, Dekker FW, Zoccali C, van Diepen M. External validation of prognostic models: what, why, how, when and where? Clin Kidney J. 2021;14(1):49–58. https://doi.org/10.1093/ckj/sfaa188
[19] Binuya MAE, Engelhardt EG, Schats W, Schmidt MK, Steyerberg EW. Methodological guidance for the evaluation and updating of clinical prediction models: a systematic review. BMC Med Res Methodol. 2022;22(1):316. https://doi.org/10.1186/s12874-022-01801-8
[20] Moons KG, Kengne AP, Grobbee DE, Royston P, Vergouwe Y, Altman DG, et al. Risk prediction models: II. External validation, model updating, and impact assessment. Heart. 2012;98(9):691–8. https://doi.org/10.1136/heartjnl-2011-301247
[21] Van Calster B, McLernon DJ, van Smeden M, Wynants L, Steyerberg EW. Calibration: the Achilles heel of predictive analytics. BMC Med. 2019;17(1):230. https://doi.org/10.1186/s12916-019-1466-7
[22] Riley RD, Archer L, Snell KIE, Ensor J, Dhiman P, Martin GP, et al. Evaluation of clinical prediction models (part 2): how to undertake an external validation study. BMJ. 2024;384:e074820. https://doi.org/10.1136/bmj-2023-074820
[23] Landelijk Platform Protonentherapie (LPPT). Landelijk Indicatieprotocol Protonentherapie Hoofdhals. (v 2.2). 2017. Available from: http://www.nvro.nl/publicaties/rapporten [Cited date: 2024 Dec 9]
[24] Langendijk JA, Lambin P, De Ruysscher D, Widder J, Bos M, Verheij M. Selection of patients for radiotherapy with protons aiming at reduction of side effects: the model-based approach. Radiother Oncol. 2013;107(3):267-73. https://doi.org/10.1016/j.radonc.2013.05.007
[25] Grégoire V, Evans M, Le QT, Bourhis J, Budach V, Chen A, et al. Delineation of the primary tumour Clinical Target Volumes (CTV-P) in laryngeal, hypopharyngeal, oropharyngeal and oral cavity squamous cell carcinoma: AIRO, CACA, DAHANCA, EORTC, GEORCC, GORTEC, HKNPCSG, HNCIG, IAG-KHT, LPRHHT, NCIC CTG, NCRI, NRG Oncology, PHNS, SBRT, SOMERA, SRO, SSHNO, TROG consensus guidelines. Radiother Oncol. 2018;126(1):3–24. https://doi.org/10.1016/j.radonc.2017.10.016
[26] Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys. 1995;31(5):1341–6. https://doi.org/10.1016/0360-3016(95)00060-c
[27] Vergouwe Y, Nieboer D, Oostenbrink R, Debray TPA, Murray GD, Kattan MW, et al. A closed testing procedure to select an appropriate method for updating prediction models. Stat Med. 2017;36(28):4529–39. https://doi.org/10.1002/sim.7179
[28] Vickers AJ, Cronin AM, Elkin EB, Gonen M. Extensions to decision curve analysis, a novel method for evaluating diagnostic tests, prediction models and molecular markers. BMC Med Inform Decis Mak. 2008;8:53. https://doi.org/10.1186/1472-6947-8-53
[29] Steyerberg EW. Clinical prediction models – a practical approach to development, validation, and updating. Springer, New York; 2009.
[30] Iacovacci J, Palorini F, Cicchetti A, Fiorino C, Rancati T. Dependence of the AUC of NTCP models on the observational dose-range highlights cautions in comparison of discriminative performance. Phys Med. 2023;113:102654. https://doi.org/10.1016/j.ejmp.2023.102654
[31] Li Y, Taylor JM, Ten Haken RK, Eisbruch A. The impact of dose on parotid salivary recovery in head and neck cancer patients treated with radiation therapy. Int J Radiat Oncol Biol Phys. 2007;67(3):660–9. https://doi.org/10.1016/j.ijrobp.2006.09.021
[32] Nakatsugawa M, Cheng Z, Kiess A, Choflet A, Bowers M, Utsunomiya K, et al. The needs and benefits of continuous model updates on the accuracy of RT-induced toxicity prediction models within a learning health system. Int J Radiat Oncol Biol Phys. 2019;103(2):460–7. https://doi.org/10.1016/j.ijrobp.2018.09.038
[33] Eisbruch A, Kim HM, Terrell JE, Marsh LH, Dawson LA, Ship JA. Xerostomia and its predictors following parotid-sparing irradiation of head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2001;50(3):695–704. https://doi.org/10.1016/s0360-3016(01)01512-7
[34] van Rijn-Dekker MI, la Bastide-van Gemert S, Stokman MA, Vissink A, Coppes RP, Langendijk JA, et al. Radiation-induced xerostomia is related to stem cell dose-dependent reduction of saliva production. Int J Radiat Oncol Biol Phys. 2024;120(3):772–82. https://doi.org/10.1016/j.ijrobp.2024.04.012
[35] Chu H, de Vette SPM, Neh H, Sijtsema NM, Steenbakkers R, Moreno A, et al. Three-dimensional deep learning normal tissue complication probability model to predict late xerostomia in patients with head and neck cancer. Int J Radiat Oncol Biol Phys. 2025;121(1):269–80. https://doi.org/10.1016/j.ijrobp.2024.07.2334
[36] de Vette SPM, van Rijn-Dekker MI, Van den Bosch L, Keijzer K, Neh H, Chu H, et al. Evaluation of a comprehensive set of normal tissue complication probability models for patients with head and neck cancer in an international cohort. Oral Oncol. 2025;163:107224. https://doi.org/10.1016/j.oraloncology.2025.107224