ORIGINAL ARTICLE
Why are not all paediatric cancer patients treated with protons? A population-based report from Sweden, 2016–2023
Anna Asklida,b  , Ingrid Kristensenc,d , Ulla Martinssone , Martin P. Nilssonc, Malin Blomstrandf,g , Måns Agruph, Anna Flejmere , Anna-Maja Svärdi, Charlotta Fröjdf , Erik Almhagenb,j , Jacob Engellauc and Anna Embringa,b
, Ingrid Kristensenc,d , Ulla Martinssone , Martin P. Nilssonc, Malin Blomstrandf,g , Måns Agruph, Anna Flejmere , Anna-Maja Svärdi, Charlotta Fröjdf , Erik Almhagenb,j , Jacob Engellauc and Anna Embringa,b
aDepartment of Oncology, Karolinska University Hospital, Stockholm, Sweden; bDepartment of Oncology-Pathology, Karolinska Institute, Stockholm, Sweden; cDepartment of Hematology, Oncology and Radiation Physics, Skane University Hospital, Lund, Sweden; dDepartment of Oncology, Clinical Sciences, Lund University, Lund, Sweden; eDepartment of Immunology, Genetics and Pathology, Uppsala University, Uppsala, Sweden; fDepartment of Oncology, Sahlgrenska University Hospital, Gothenburg, Sweden; gDepartment of Oncology, Institute of Clinical Sciences, University of Gothenburg, Sweden; hDepartment of Oncology, and Department of Biomedical and Clinical Sciences, Linköping University, Linköping, Sweden; iDepartment of Radiation Sciences, Oncology, Umeå University, Sweden; jDepartment of Nuclear Medicine and Medical Physics, Karolinska University Hospital, Stockholm, Sweden
ABSTRACT
Background: In 2015, a proton therapy (PT) facility was established in Sweden with one aim being to ensure access for all children expected to benefit from PT. Despite potential dosimetric advantages and full subsidisation, PT is not always selected. This study explores reasons for choosing alternative radiotherapy (RT) modalities in a paediatric population.
Material and methods: RT courses delivered to patients ≤ 18 years during 2016–2023 were identified from a national registry. Medical records were retrospectively reviewed to identify reasons for not selecting PT.
Results: Only 34% (n = 275) of all courses identified were delivered with PT. Of the remaining 66% (n = 544), 90% were photon RT, 9% combined PT and photon RT, and 1% electron RT. Among photon RT courses, 97% were delivered with conventional external beam radiotherapy (EBRT), 2% with stereotactic radiotherapy (SRT), and 1% with brachytherapy. The most common reason for choosing photons was non-curative intent (35%), followed by equal or superior expected outcome compared to PT (23%), total body irradiation (TBI) (15%), and uncertainties due to air, organ motion, or metal in field (15%). Dosimetric comparison led to the selection of a favourable or equal photon plan in 8%. Logistical, social, and technical reasons constituted 4%.
Conclusion: While PT can reduce radiation exposure to healthy tissues, particularly important in children, clinical, logistical, and technical factors often necessitate alternative RT modalities. This study highlights the importance of individualised RT planning and multidisciplinary collaboration to balance medical, technical, and practical considerations to ensure optimal treatment approach in every child.
KEYWORDS: Radiotherapy; paediatrics; proton therapy; clinical practice pattern
Citation: ACTA ONCOLOGICA 2025, VOL. 64, 1160–1167. https://doi.org/10.2340/1651-226X.2025.43726.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Oncologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Received: 28 April 2025; Accepted: 8 August 2025; Published: 2 September 2025
CONTACT: Anna Asklid anna.asklid@ki.se Karolinska University Hospital, Anna Steckséns gata 41, 171 76 Stockholm, Sweden
Supplemental data for this article can be accessed online at https://doi.org/10.2340/1651-226X.2025.43726
Competing interests and funding: The authors report there are no competing interests to declare.
Introduction
Over past decades, the use of radiotherapy (RT) has declined but remains a cornerstone within the multimodal treatment concept for paediatric malignancies [1]. Various RT techniques are applied across a broad range of paediatric diseases, predominantly for malignant and occasionally benign conditions [2–4]. In Sweden, around 350 children are diagnosed with cancer annually. About 25% of these will receive radiation as part of their treatment [5].
Modern conformal RT techniques have continuously evolved over time and proton therapy (PT) represents a major advancement in cancer treatment offering dosimetric advantages by minimising radiation exposure to healthy tissues [6]. Although long-term clinical data remains limited, PT is widely recognised as standard of care for many paediatric malignancies, given its potential to lower the risk of severe late side effects and secondary malignancies [7–9].
In late 2015, a national proton facility opened in Uppsala, Sweden, with one aim being to provide treatment to paediatric patients expected to benefit from PT [10, 11]. At this time, PT use in paediatric cancer showed considerable international variation. Central nervous system (CNS) tumours were the most common diagnoses treated with PT worldwide. However, only a limited number of patients were treated with PT in each centre and a wide range of diagnoses were reported [12]. PT was available in Sweden before 2015, at The Svedberg laboratory (TSL), but with treatment in sitting position and hence used mainly for CNS and head/neck targets and without possibilities to treat patients in need of anaesthesia [11, 13].
All paediatric cancer patients in Sweden are discussed at multidisciplinary tumour boards and all paediatric RT cases are reviewed within the Swedish Working Group of Paediatric Radiotherapy (SBRTG), comprising radiation oncologists working in close collaboration with dosimetrists and physicists at the six paediatric RT centres. The standard approach is to generate comparative photon and proton plans. These are assessed at SBRTG’s bi-weekly national video conferences, where the most appropriate plan is selected for each individual patient. A back-up photon plan is always available for patients receiving PT (except for craniospinal irradiation, CSI), to avoid prolonged treatment interruptions caused by unforeseen technical issues.
Treatment of paediatric cancer, including travel costs and accommodation, is fully subsidised in Sweden and entails no additional financial issues for the families compared to other RT options. Since the opening of the proton facility, experiences have been positive with few serious side effects [13]. The aim of this study was to investigate reasons why paediatric patients in Sweden were treated with an RT modality other than PT, despite PT being readily available.
Material and methods
This observational retrospective cohort study includes all paediatric patients treated with an RT modality other than PT in Sweden during 2016–2023. Treatment courses, clinical and treatment characteristics were identified through RADTOX, a prospectively maintained national RT database [13]. Courses were grouped by treatment year, centre, modality, and diagnosis. Courses including an RT modality other than solely PT were identified. Radiation oncologists from the six paediatric RT centres in Sweden retrospectively reviewed patient records to determine reasons for not selecting PT. In cases where photon therapy was chosen, it was documented whether comparative photon and proton treatment plans had been made.
Statistical analysis
Clinical and treatment characteristics are presented using descriptive statistics. Chi-squared statistics assessed treatment distribution of PT versus non-PT treatment across centres. The Kaplan–Meier estimator was used to estimate overall survival (OS), calculated from the start of the first RT until death or closure of database (31 December 2023), whichever came first. Analyses of OS were performed using R Statistical Software (4.3.3; R Core Team 2024) [14] using ggplot [15] and ggsurvfit packages [16].
Ethics declarations
The study was performed in accordance with current ethical principles and approved by the National Ethical Review Authority (Dnr 2023-04736-02).
Results
In total, 819 RT courses were identified in the RADTOX registry during 2016–2023. Of these, 275 (34%) were delivered with PT to 263 individual patients (57% male, 43% female) and 544 (66%) with other modalities (non-PT), to 464 patients (54% male, 46% female). Twenty-five patients received both PT and non-PT at different timepoints during the study period.
Non-PT remained predominant but declined over time (Figure 1A). PT comprised 40–45% of annual courses, peaking in 2023 after a dip in 2021. PT use was relatively consistent across centres and not significantly associated (p = 0.2) with geographic distance from the proton facility (Figure 1B).
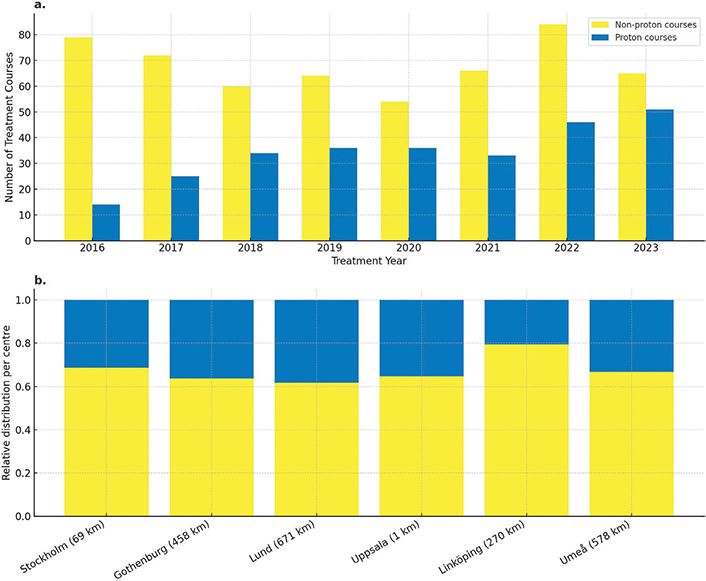
Figure 1. Annual distribution of radiotherapy courses delivered using proton therapy (blue) and non-proton therapy (yellow) between 2016 and 2023 (A). Relative distribution of treatment courses per paediatric radiotherapy centre, with distance to the national proton facility in kilometers (km) indicated in brackets (B). There was no significant association between proton therapy use and the distance from the proton facility (Chi-squared test, p = 0.2).
Diagnoses were classified using International Classification of Childhood Cancer (ICCC-3) [17]. CNS tumours dominated, accounting for one-third of non-PT and over half of PT courses (Figure 2). Other common diagnoses in both groups were sarcoma and neuroblastoma even though a peak in PT for neuroblastomas was noted at the end of the study period. Leukaemias and renal tumours were mainly treated with non-PT. See supplementary material, Table S1 and Figure S1 for details.

Figure 2. Distribution of diagnosis groups for all proton (blue) and non-proton (yellow) treatment courses over the study period. CNS: central nervous system.
Non-proton cohort
The non-PT group (n = 544) constituted the primary study cohort for analysis. Median age at start of first RT was 9.6 years (range 0.1–18.8 years). After a median follow-up time of 26.6 months (range 0.6–96 months), the median OS was not reached, and the 5-year OS was 60% (Figure 3). Most patients (87%) received one RT course while the remainder had two to seven courses during the study period.
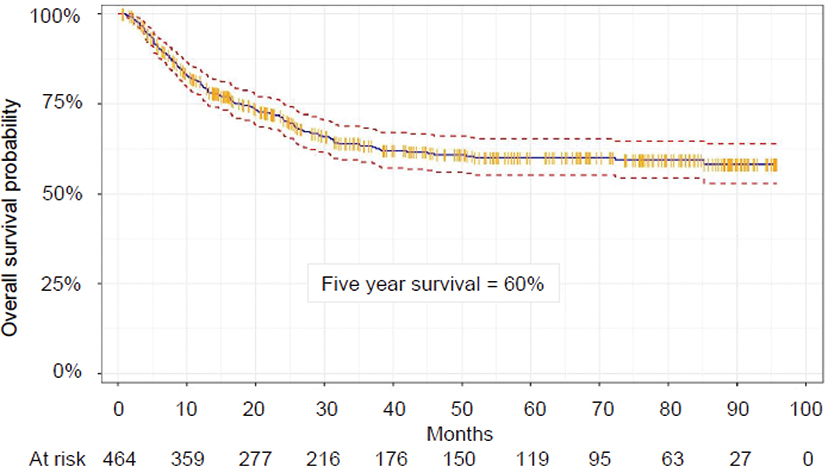
Figure 3. Kaplan–Meier estimate of overall survival in the non-proton group (n = 464). Solid blue curve is the Kaplan–Meier estimator. Red dashed curves show the 95% confidence interval. Orange vertical markers show censored patients. n: number of patients.
Photon RT was used in 90%, combined proton-photon treatment during the same course in 9%, and electron RT in 1%. Of photon RT courses, 97% were external beam radiotherapy (EBRT) (two-dimensional [2D], three-dimensional conformal radiotherapy [3D-CRT], and rotational techniques), 2% stereotactic radiotherapy (SRT), and 1% brachytherapy. SRT included 10 courses in lung and CNS lesions, of which six were delivered with Gamma Knife. Brachytherapy was registered in seven localised rhabdomyosarcomas, five in the urogenital tract, and two in the nose. Electron RT was used in three superficial skin lesions.
A shift in RT techniques occurred over time, with declining use of 2D/3D-CRT and increasing use of rotational techniques (Intensity modulated radiation therapy (IMRT), volumetric modulated arc therapy (VMAT), and helical tomotherapy), becoming the most applied photon technique from 2020. By 2023, rotational techniques accounted for over two-thirds of all non-proton RT courses (Figure 4). Similarly, in the subgroup of total body irradiation (TBI), total marrow irradiation (TMI), or total lymphoid irradiation (TLI), a notable shift to rotational techniques was observed, accounting for 64% in the last 2 years of the study period (data not shown).
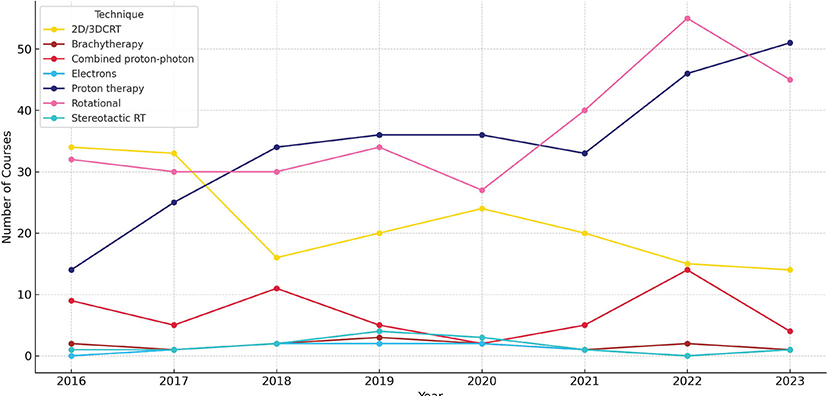
Figure 4. Trends in the use of non-proton radiotherapy techniques and proton therapy over the study period. 2D: two-dimentional; 3D: three dimentional; CRT: conformal radiation therapy; RT: radiotherapy.
Rational for photon RT
The most reported reasons for choosing EBRT were non-curative intent (35%), equal or superior expected outcome (clinical and/or dosimetrical) (23%), and TBI/TMI/TLI (15%) (Table 1). Other reasons included uncertainties with PT due to tissue heterogeneities (e.g. air-bone interface), organ motion or metal in field (15%), dosimetrically favourable (5%) or equal (3%) photon plan, and logistical (2%), social (1%), and technical factors (1%).
In the non-curative group (n = 167), where treatment aimed to relieve symptoms, achieve local control, or prolong life when cure was not deemed achievable, CNS tumours (68%) particularly diffuse intrinsic pontine glioma (DIPG) and diffuse midline glioma (DMG) dominated (Table 2). After a median follow-up of 8.4 months (range 1.1–83.9 months), the median OS was 8.9 months (Figure 5). Four patients died within 30 days of starting RT. See supplementary material, Table S2 for details on fractionation.
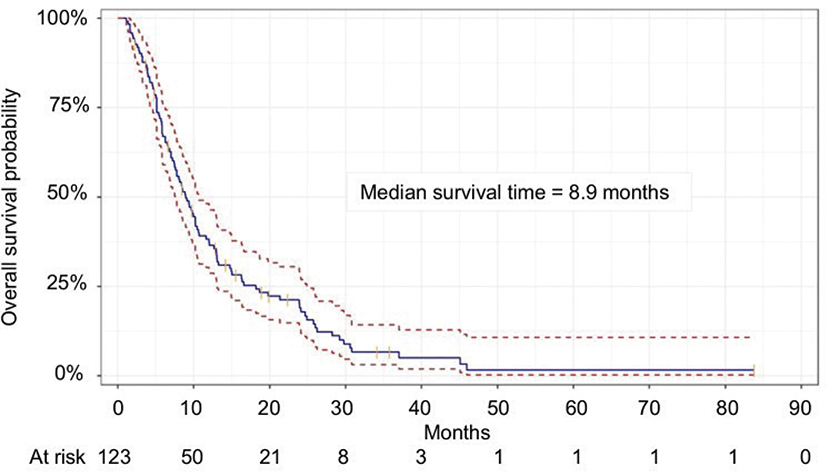
Figure 5. Kaplan–Meier estimate of overall survival in the non-curative intent group (n = 123). Solid blue curve is the Kaplan–Meier estimator. Red dashed curves show the 95% confidence interval. Orange vertical markers show censored patients. n: number of patients.
In 86% of EBRT courses, including all with reasons stated as non-curative intent, equal or superior expected outcome, TBI/TMI/TLI (considered not applicable) social and technical circumstances, no comparative proton–photon planning was performed (Table 1). For the remaining 14%, comparative planning was conducted, but PT was not selected for various reasons described further in the text. Use of comparative planning generally increased over time.
The second largest group, equal or superior expected outcome (n = 109), mainly included Wilms tumour or neuroblastoma with large-volume targets (e.g. whole abdomen, lung, flank) and low prescribed doses (10–25.2 Gy) (See supplementary material, Table S3). In 13 cases, comparative plans showed equivalency, typically in similar diagnoses and targets. Additionally, in some sarcomas located distally or superficially in extremities, photon plans offered no clear disadvantage. In some of these cases, additional social and practical considerations further contributed to selecting photon RT over PT.
Photon RT was preferred in 71 cases where uncertainties related to metal in field (e.g. bone sarcomas), tissue inhomogeneities, or internal organ movement (e.g. head and neck area, thorax, abdomen) posed challenges with PT (see supplementary material, Table S4). In another 22 cases, photon plans were favoured due to factors like better target coverage, robustness or reduced uncertainties associated with the wider proton penumbra near sensitive organs at risk (OARs), most commonly in targets with a large interface against the brainstem and high prescribed doses up to 59.4 Gy (see supplementary material, Table S5). Photon plans were also preferred for small orbital targets, to avoid hotspots more frequently observed in PT plans, and in one ocular case the photon plan achieved better coverage with bolus. Concerns about increased biological effect due to elevated linear energy transfer (LET) in the brainstem influenced decisions in a patient with central respiratory impairment. In another patient, type 1 reirradiation (i.e. a new course of RT with geometrical overlaps with a previously irradiated volume) in a region earlier treated with Gamma Knife also affected the clinical decision. Furthermore, in one extremity sarcoma, the photon plan offered better sparing of the limb circumference using tangential fields.
Social factors (n = 6) related to school/family context influenced decisions, particularly in centres far from the PT facility. Two of these cases involved CSI delivered with helical tomotherapy to minimise normal tissue exposure. Urgent symptoms (n = 9) further prompted initiation of RT at the home clinic faster than would have been possible with PT. Technical limitations (n = 3) included treatment volumes exceeding the capacity of the PT planning system.
Combined proton–photon courses
In 9% of courses, protons and photons were combined in the same course. One-third was mixed due to unplanned technical downtime at the proton facility, where at least one fraction was delivered with photons to avoid prolonged treatment interruption. Another third involved acute symptoms (mainly CNS-related) requiring urgent treatment start, before a start with PT could possibly be arranged. In the final third, a combined approach was deemed dosimetrically advantageous, mostly in whole lung RT cases treated with photons followed by a proton boost exploiting the strengths of both modalities (see supplementary material, Table S6). In some CNS-cases, a mixed plan was chosen as photons offered superior target coverage, while protons reduced the integral dose and OAR exposure. Finally, four patients treated in early 2016 still received CSI with photons but also the boost with protons prior to full implementation of PT-based CSI.
Discussion
This nationwide registry-based study provides a comprehensive overview of paediatric RT practice in Sweden from 2016 to 2023, offering real-world insights into clinical decision-making. Nationally, PT use has steadily increased, reaching 40–45% of all paediatric RT courses. However, this is still lower than the 60–80% initially projected before the centre opened [18]. The temporary dip in PT use observed in 2020 was likely due to the Covid-19 outbreak. A relatively even distribution of PT use across centres, regardless of distance from the proton facility, suggests that treatment decisions are primarily guided by clinical and dosimetric considerations, not geographic proximity.
The most common reason for selecting a non-PT approach was non-curative intent, reflecting prioritisation of symptom relief and quality of life over potential long-term benefits in patients with limited life expectancy. Palliative RT remains a valuable tool to alleviate or prevent symptoms in paediatric patients [3, 19]. Careful patient selection is essential to balance potential benefits against disadvantages such as toxicity or additional time spent in hospital near the end of life. While this study did not aim to assess treatment outcomes, the low 30-day mortality (3%) suggests appropriate patient selection, consistent with findings from other paediatric-focused studies but considerably lower than in the adult population [3, 20]. Social circumstances also influenced decision-making in a small subset of cases, emphasising the need for patient-centred, individualised care.
Several reasons for selecting non-PT treatment were described even in curative settings, despite the availability and full subsidisation of PT. While clinical outcomes with PT are encouraging and its use is expected to increase [21], other RT modalities will remain necessary. Photon RT for instance, continues to be standard of care for TBI [22], and in line with international guidelines we also observed a trend towards increased use of rotational techniques such as VMAT and helical tomotherapy in our TBI treatments over the years [22, 23].
Another frequent rationale for selecting photon RT was the anticipated equivalence in clinical outcome of photon and proton treatment without comparative planning being performed. This was particularly noted in treatments involving large target volumes, such as whole lung, whole abdomen, or flank irradiation in Wilms tumours or neuroblastomas. One explanation may be the relatively low prescribed doses (10–25.2 Gy) and the fact that photon RT has been the standard treatment in many historical paediatric study protocols. However, this represents an area for potential improvement, as PT can reduce low-dose exposure and spare OARs, thereby mitigating acute toxicity and potentially long-term effects even at lower radiation doses [24, 25]. Notably, the use of PT for neuroblastoma increased towards the end of the study period and our recently published data on comparative proton and photon treatment planning in this patient group further support the benefits of PT in selected cases by lower doses to OARs and reduced low-dose exposure to surrounding healthy tissue [26].
Mixed proton–photon treatments were used to a lesser extent, reflecting a hybrid approach, with potential to combine strengths of both modalities [27, 28]. In some cases, this approach was necessitated by technical downtime, urgent treatment needs, or other clinical considerations that favoured one modality for at least part of the course. This demonstrates opportunities to balance dosimetric advantages with logistical realities and further illustrates the complexity of paediatric RT.
Uncertainties related to air interfaces and internal organ motion contributed to the choice of photon therapy in a substantial number of courses. This may partly reflect limited experience with motion management techniques at the PT centre, especially in the beginning of the study period. Over time, an increasing trend in comparative dose planning was shown, probably mirroring implementation of motion management strategies (e.g. 4DCT and breath hold techniques), even for children and adolescents. Improved strategies to address technical challenges together with streamline PT logistics, and preparing children as much as possible before starting RT to reduce the need of anaesthesia, could enhance feasibility for a broader group of paediatric patients [29, 30].
Photon RT was sometimes preferred or considered equivalent to PT in terms of target coverage, robustness, and the ability to create steep dose gradients – particularly near critical structures like the brainstem, where the wider lateral penumbra of protons might pose challenges [6, 31]. In cases of type 1 reirradiation [32] and concerns of increased LET, advanced photon techniques (e.g. IMRT, VMAT) may represent a reasonable alternative [33, 34]. In our cohort, this rationale applied in selected ependymoma cases with a large interface against the brainstem, probably reflecting previously raised concerns about PT-related brainstem toxicity. Limitations in technical infrastructure, such as the absence of more advanced and accurate dose calculation algorithms and LET evaluation tools in daily clinic, may also have influenced the decision-making, especially in anatomically complex cases. While large prospective randomised trials are unlikely due to practical and ethical reasons, PT is increasingly used for these challenging targets and growing outcome data suggest no clear correlation between brainstem toxicity and RT modality [35] and PT should always be considered in multidisciplinary discussions for all children with CNS tumours [36, 37]. Reporting of outcome data is furthermore strongly encouraged, alongside continuous improvements in PT technology, access to advanced treatment planning systems to address dose-deposition uncertainties, developments that may support and aid clinical decision-making and broaden the applicability of PT to more paediatric patients.
Other techniques limiting radiation exposure to surrounding healthy tissues, such as brachytherapy and SRT, remained infrequently used throughout the study period. Their limited application likely reflects both narrow clinical indications and high demands in terms of equipment, expertise, and treatment planning [4]. Nevertheless, these techniques remain valuable in selected cases, for example localised rhabdomyosarcoma, where preserving organ and function can be very important for quality of life, offering clinicians additional opportunities to individualise care [38, 39].
RT decisions in the paediatric population require multidisciplinary discussions to weigh the benefits and limitations of each modality. Over time, a distinct increase in the utilisation of comparative proton-photon planning was observed and this upward trend may reflect growing awareness of the benefits of plan comparison to guide modality selection. Sweden’s model of distributed competence – where RT planning is conducted at six regional centres, while PT delivery is centralised – may contribute to variability in local experience [40]. In the initial years of PT use, some referring centres may have had limited hands-on experience with proton planning, possibly leading to more cautious or conservative modality choices in ambiguous cases. However, regular and close collaboration between clinicians and physicists in daily practice, along with continuous national coordination within SBRTG has facilitated shared expertise as all paediatric patients planned for RT, regardless of modality, are presented at SBRTG meetings.
Our study’s strengths lie in its comprehensive national cohort, ensuring representativeness and minimal selection bias. The inclusion of all paediatric RT patients treated with modalities other than PT over an extended period provides valuable insights into the decision-making processes. Limitations include the retrospective nature and the registry-based approach with inherent weaknesses such as potential underreporting of nuanced factors influencing treatment decisions. The absence of consistent comparative dose plans restricts the ability to fully assess the theoretical benefits of PT as well as the lack of information on side-effects. Although this was outside the scope of this study, it might add an important dimension in further studies. Our findings may also have limited generalisability to other healthcare systems due to differences in infrastructure and access to PT.
Conclusion
This study provides a comprehensive overview of paediatric RT in clinical routine care with a particular focus on the rationale behind the decision-making for selecting alternative modalities than PT. Despite full subsidisation and availability, PT was used in only one third of all courses. Our findings indicate that while PT is gaining ground, photon RT – particularly with advanced rotational techniques and broad clinical indications – continues to play a major role in paediatric RT. Individualised treatment selection is especially critical in paediatric cases, where the balance between effective tumour control and sparing of normal tissue is paramount. This study contributes to support the difficult decision-making in a complex clinical setting and underscores the vital role of paediatric radiation oncologists in multidisciplinary teams. It also highlights the importance of continued close collaboration between physicians, physicists, and dosimetrists as well as within the broader RT community, both nationally and internationally, to ensure the most appropriate treatment for each child.
Author contributions
AA, AE, UM, IK, JE, MN, MB, CF, AF, MA, AMS were involved in the planning of the study, data collection, and data analysis. AA, AE, UM, and IK prepared the manuscript. AA and AE were responsible for the literature research. AA, AE, and EA performed the statistical analyses. All authors reviewed, edited, and approved the final manuscript.
Acknowledgements
This work was partly funded by the Skandion Clinic Research Council, Uppsala and the Swedish Childhood Cancer Foundation.
Data availability statement
Raw data are available from the corresponding author on request.
Supplementary material
See supplementary material for STROBE Statement-Checklist and for supplementary tables and figures.
References
[1] Jairam V, Roberts KB, Yu JB. Historical trends in the use of radiation therapy for pediatric cancers: 1973–2008. Int J Radiat Oncol Biol Phys. 2013;85(3):e151–5. https://doi.org/10.1016/j.ijrobp.2012.10.007
[2] Steinmeier T, Schulze Schleithoff S, Timmermann B. Evolving radiotherapy techniques in paediatric oncology. Clin Oncol (R Coll Radiol). 2019;31(3):142–50. https://doi.org/10.1016/j.clon.2018.12.005
[3] Tsang DS, Vargo JA, Goddard K, Breneman JC, Kalapurakal JA, Marcus KJ. Palliative radiation therapy for children with cancer. Pediatr Blood Cancer. 2021;68(Suppl 2):e28292. https://doi.org/10.1002/pbc.28292
[4] Boterberg T, Dunlea C, Harrabi S, Janssens G, Laprie A, Whitfield G, et al. Contemporary paediatric radiation oncology. Arch Dis Child. 2023;108(5):332–7. https://doi.org/10.1136/archdischild-2021-323059
[5] Årsrapport 2023 Svenska Barncancerregistret [Internet]. [cited 2024 Dec 11]. Available from: https://cceg.ki.se/documents/Arsrapport_SBCR_2023.pdf
[6] Patyal B. Dosimetry aspects of proton therapy. Technol Cancer Res Treat. 2007;6(4 Suppl):17–23. https://doi.org/10.1177/15330346070060S403
[7] Greenberger BA, Yock TI. The role of proton therapy in pediatric malignancies: recent advances and future directions. Semin Oncol. 2020;47(1):8–22. https://doi.org/10.1053/j.seminoncol.2020.02.002
[8] Ho ESQ, Barrett SA, Mullaney LM. A review of dosimetric and toxicity modeling of proton versus photon craniospinal irradiation for pediatrics medulloblastoma. Acta Oncol. 2017;56(8):1031–42. https://doi.org/10.1080/0284186X.2017.1324207
[9] Eaton BR, MacDonald SM, Yock TI, Tarbell NJ. Secondary malignancy risk following proton radiation therapy. Front Oncol. 2015;5:261. https://doi.org/10.3389/fonc.2015.00261
[10] Brandal P, Bergfeldt K, Aggerholm-Pedersen N, Backstrom G, Kerna I, Gubanski M, et al. A Nordic-Baltic perspective on indications for proton therapy with strategies for identification of proper patients. Acta Oncol. 2020;59(10):1157–63. https://doi.org/10.1080/0284186X.2020.1817977
[11] Kristensen I, Nilsson K, Nilsson P. Comparative proton and photon treatment planning in pediatric patients with various diagnoses. Int J Partic Ther. 2015;2(2):367–75. https://doi.org/10.14338/IJPT-14-00026.1
[12] Journy N, Indelicato DJ, Withrow DR, Akimoto T, Alapetite C, Araya M, et al. Patterns of proton therapy use in pediatric cancer management in 2016: an international survey. Radiother Oncol. 2019;132:155–61. https://doi.org/10.1016/j.radonc.2018.10.022
[13] Martinsson U, Svard AM, Witt Nystrom P, Embring A, Asklid A, Agrup M, et al. Complications after proton radiotherapy in children, focusing on severe late complications. A complete Swedish cohort 2008–2019. Acta Oncol. 2023;62(10):1348–56. https://doi.org/10.1080/0284186X.2023.2260946
[14] Team RDC. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2024.
[15] Wilkinson L. ggplot2: elegant graphics for data analysis by WICKHAM, H. Biometrics. 2011;67(2):678–9. https://doi.org/10.1111/j.1541-0420.2011.01616.x
[16] Sjoberg DBM, Fruechtenicht C, Haesendonckx S, Treis T. ggsurvfit: flexible time-to-event figures. R package version 1.1.0. 2024. [Cited date: 2024 Dec 11] Available from: https://github.com/pharmaverse/ggsurvfit
[17] Steliarova-Foucher E, Stiller C, Lacour B, Kaatsch P. International classification of childhood cancer, third edition. Cancer. 2005;103(7):1457–67. https://doi.org/10.1002/cncr.20910
[18] Glimelius B, Ask A, Bjelkengren G, Bjork-Eriksson T, Blomquist E, Johansson B, et al. Number of patients potentially eligible for proton therapy. Acta Oncol. 2005;44(8):836–49. https://doi.org/10.1080/02841860500361049
[19] Salins N, Hughes S, Preston N. Palliative care in paediatric oncology: an update. Curr Oncol Rep. 2022;24(2):175–86. https://doi.org/10.1007/s11912-021-01170-3
[20] Kutzko JH, Dadwal P, Holt T, Rahman MA, Zahir SF, Hickey B. Defining the expected 30-day mortality for patients undergoing palliative radiotherapy: a meta-analysis. Radiother Oncol. 2022;168:147–210. https://doi.org/10.1016/j.radonc.2022.01.030
[21] Thomas H, Timmermann B. Paediatric proton therapy. Br J Radiol. 2020;93(1107):20190601. https://doi.org/10.1259/bjr.20190601
[22] Hoeben BAW, Pazos M, Seravalli E, Bosman ME, Losert C, Albert MH, et al. ESTRO ACROP and SIOPE recommendations for myeloablative total body irradiation in children. Radiother Oncol. 2022;173:119–33. https://doi.org/10.1016/j.radonc.2022.05.027
[23] Milgrom SA, Dandapani SV, Wong J, Kalapurakal J, Smith KS, Han C, et al. Incorporating intensity modulated total body irradiation into a Children’s Oncology Group trial: rationale, techniques, and safeguards. Pediatr Blood Cancer. 2024;71(11):e31185. https://doi.org/10.1002/pbc.31185
[24] Mirandola A, Colombo F, Cavagnetto F, Cavallo A, Gusinu M, Molinelli S, et al. Dosimetric comparison between proton and photon radiation therapies for pediatric neuroblastoma. Int J Part Ther. 2024;12:100100. https://doi.org/10.1016/j.ijpt.2024.100100
[25] Cunningham DA, Breen WG, Johnson JE, Mullikin TC, Bradley TB, Sorenson KL, et al. Proton whole-lung irradiation: initial report of outcomes. Int J Radiat Oncol Biol Phys. 2023;115(4):866–72. https://doi.org/10.1016/j.ijrobp.2022.10.001
[26] Embring A, Kristensen I, Nilsson MP, Engellau J, Blomstrand M, Frojd C, et al. Comparative proton and photon treatment plans in children treated for neuroblastoma. Acta Oncol. 2025;64:939–45. https://doi.org/10.2340/1651-226X.2025.43865
[27] Kiss-Miki R, Obeidat M, Mate V, Teutsch B, Agocs G, Kiss-Dala S, et al. Proton or photon? Comparison of survival and toxicity of two radiotherapy modalities among pediatric brain cancer patients: a systematic review and meta-analysis. PLoS One. 2025;20(2):e0318194. https://doi.org/10.1371/journal.pone.0318194
[28] Miao Y, Wu D, Li Y, Ji Y, Sang Y. Radiation therapy for childhood-onset craniopharyngioma: systematic review and meta-analysis. J Neurooncol. 2025;172(1):89–98. https://doi.org/10.1007/s11060-024-04914-w
[29] Pakela JM, Knopf A, Dong L, Rucinski A, Zou W. Management of motion and anatomical variations in charged particle therapy: past, present, and into the future. Front Oncol. 2022;12:806153. https://doi.org/10.3389/fonc.2022.806153
[30] Ritchie T, Awrey S, Maganti M, Chahin R, Velec M, Hodgson DC, et al. Paediatric radiation therapy without anaesthesia – are the children moving? Radiother Oncol. 2024;193:110120. https://doi.org/10.1016/j.radonc.2024.110120
[31] Vogel J, Grewal A, O’Reilly S, Lustig R, Kurtz G, Minturn JE, et al. Risk of brainstem necrosis in pediatric patients with central nervous system malignancies after pencil beam scanning proton therapy. Acta Oncol. 2019;58(12):1752–56. https://doi.org/10.1080/0284186X.2019.1659996
[32] Andratschke N, Willmann J, Appelt AL, Alyamani N, Balermpas P, Baumert BG, et al. European Society for Radiotherapy and Oncology and European Organisation for Research and Treatment of Cancer consensus on re-irradiation: definition, reporting, and clinical decision making. Lancet Oncol. 2022;23(10):e469–78. https://doi.org/10.1016/S1470-2045(22)00447-8
[33] Mohan R, Peeler CR, Guan F, Bronk L, Cao W, Grosshans DR. Radiobiological issues in proton therapy. Acta Oncol. 2017;56(11):1367–3. https://doi.org/10.1080/0284186X.2017.1348621
[34] Toma-Dasu I, Dasu A, Vestergaard A, Witt Nystrom P, Nystrom H. RBE for proton radiation therapy – a Nordic view in the international perspective. Acta Oncol. 2020;59(10):1151–6. https://doi.org/10.1080/0284186X.2020.1826573
[35] Dalmasso C, Alapetite C, Bolle S, Goudjil F, Lusque A, Desrousseaux J, et al. Brainstem toxicity after proton or photon therapy in children and young adults with localized intracranial ependymoma: a French retrospective study. Radiother Oncol. 2024;194:110157. https://doi.org/10.1016/j.radonc.2024.110157
[36] Indelicato DJ. No question: proton therapy is safe. Neuro Oncol. 2022;24(9):1582–3. https://doi.org/10.1093/neuonc/noac121
[37] Indelicato DJ, Ioakeim-Ioannidou M, Bradley JA, Mailhot-Vega RB, Morris CG, Tarbell NJ, et al. Proton therapy for pediatric ependymoma: mature results from a bicentric study. Int J Radiat Oncol Biol Phys. 2021;110(3):815–20. https://doi.org/10.1016/j.ijrobp.2021.01.027
[38] Davila Fajardo R, Scarzello G, Gaze MN, Boterberg T, Cameron A, Fuchs J, et al. Brachytherapy for rhabdomyosarcoma: survey of international clinical practice and development of guidelines. Radiother Oncol. 2024;195:110273. https://doi.org/10.1016/j.radonc.2024.110273
[39] Stenman J, Wickart-Johansson G, Sundquist F, Nilsson J, Ljungman G, Osterlundh G, et al. Five-year follow-up after multimodal treatment incorporating HDR brachytherapy for bladder prostate rhabdomyosarcoma in children. Int J Radiat Oncol Biol Phys. 2022;113(2):355–9. https://doi.org/10.1016/j.ijrobp.2022.01.034
[40] Karlsson M, Bjork-Eriksson T, Mattsson O, Mattsson S, Montelius A, Nilsson P, et al. “Distributed proton radiation therapy” – a new concept for advanced competence support. Acta Oncol. 2006;45(8):1094–101. https://doi.org/10.1080/02841860600897876