SHORT REPORT
Predictive factors of oral mucositis in patients with locally recurrent inoperable head and neck cancer treated with boron neutron capture therapy
Tanja Mälkiäa  , Hanna Koivunoroa,b , Tiina Seppäläa , Leena Kankaanrantaa , Liisa Porraa , Anu Anttonena , Mikko Tenhunena and Heikki Joensuua
, Hanna Koivunoroa,b , Tiina Seppäläa , Leena Kankaanrantaa , Liisa Porraa , Anu Anttonena , Mikko Tenhunena and Heikki Joensuua
aDepartment of Radiation Oncology, Helsinki University Hospital Comprehensive Cancer Center and University of Helsinki, Helsinki, Finland; bNeutron Therapeutics Finland Oy, Helsinki, Finland
ABSTRACT
Background and purpose: The prognosis of recurrent head and neck (HN) cancer is poor. High response rates have been achieved with boron neutron capture therapy (BNCT) in the treatment of locally recurrent HN cancer. Radiation-induced oral mucositis (OM) is a common adverse effect of BNCT. We evaluated the factors associated with severe OM in patients treated with BNCT.
Patient/material and methods: Ninety two patients with locally recurrent inoperable HN cancer were treated with nuclear reactor-based BNCT in 1–2 fractions. The association between grade 3 OM, patient clinical parameters and maximum weighted oral mucosa dose was evaluated. Mucosal dose was calculated using the skin nitrogen concentration of 4.2%. A sigmoidal normal tissue complication probability (NTCP) model was created by dividing patients into four equal sized groups based on increasing dose levels.
Results: Grade 3 OM was observed in 42% of patients after the first BNCT treatment. The prevalence of OM increased with higher maximum oral mucosa doses. From the NTCP curve, we estimated the dose corresponding to a 50% probability (D50) for grade 3 OM to be 13.5 Gy(W). Older age was the only patient- related factor significantly associated with increased grade 3 OM risk.
Interpretation: Higher maximum oral mucosa doses increased the risk of grade 3 OM. Older age was the only other factor related to severe OM.
KEYWORDS: Boron neutron capture therapy; oral mucositis; head and neck cancer; radiation therapy
Citation: ACTA ONCOLOGICA 2025, VOL. 64, 1307–1311. https://doi.org/10.2340/1651-226X.2025.44039.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Oncologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Received: 1 June 2025; Accepted: 3 September 2025; Published: 23 September 2025
CONTACT: Mälkiä Tanja tanja.malkia@hus.fi Comprehensive Cancer Center, Helsinki University Hospital, P.O. Box 180, FIN-00029 HUS, Helsinki, Finland
Competing interests and funding: Hanna Koivunoro is employed by Neutron Therapeutics Inc. Heikki Joensuu is the Chairman of the Scientific Advisory Board of Neutron Therapeutics, Inc., the Chairman of the Scientific Advisory Board of Orion Corporation, Orion Pharma and the Chairman of the Scientific Committee of Maud Kuistila Foundation; he has received a honorarium for speaking from Deciphera Pharmaceuticals, has been a full time or part time employer or consultant of Orion Pharma and owns stocks of Orion Pharma and Sartar Therapeutics. No further potential conflict of interest was reported by the authors.
Introduction
The treatment of locally recurrent head and neck (HN) cancer remains challenging despite multimodal approaches. Approximately 2/3 of patients present with stage III or IV disease, and the locoregional recurrence rate in advanced cases varies 15–50%, typically occurring within 2 years of primary treatment [1, 2]. Patients with non-metastatic recurrent tumors are treated with curative intent if possible. Salvage surgery is a curative option for a few patients with resectable recurrence, achieving disease control in 15–30% of cases [3–5]. However, for most patients, surgery is not viable, and radiotherapy with or without chemotherapy is used with curative intent. Overall prognosis after recurrence remains poor [6, 7]. Therefore, new treatment modalities are needed.
Boron neutron capture therapy (BNCT) has shown high response rates (58–81%) in clinical studies of locally recurrent HN cancer [8–13]. BNCT is a cell-selective particle radiotherapy based on neutron capture reaction. When a non-radioactive isotope of boron (10B) is irradiated with thermal neutrons, it produces a high linear energy transfer (LET) α-particle (4He2+) and recoils lithium (7Li) nuclei [14]. Due to their short range (<10 µm) in tissue, the effect is primarily local and limited to boron-containing cells while preserving normal cells. Tumor-selective boron uptake is achieved using boron carriers such as L-boronphenylalanine (L-BPA). Oral mucosa is considered a highly sensitive organ-at-risk in BPA-mediated BNCT, due to rapidly dividing epithelial cells, and high boron uptake [15].
In a phase I/II trial at the Finnish FiR 1 research reactor, 76% of patients responded to BNCT and 54% developed grade 3 oral mucositis (OM) [9, 11, 16]. This study was designed to evaluate the reasons for the high prevalence of grade 3 OM within the HN patient cohort treated with the reactor to improve future treatments using an accelerator-based BNCT.
Patients/material and methods
Study design and objectives
This is a retrospective study of HN cancer patients treated at the FiR 1 reactor during years 2003–2012 [9, 11, 16]. The primary objective was to identify factors associated with grade 3 OM.
Patients
A total of 102 patients with histologically confirmed, locally recurrent, inoperable HN cancer, without distant metastases and no available effective standard treatment, were treated with BNCT with the intent of local control. Of these, 92 patients were included in the study, 10 were excluded due to early death (n = 4) or missing data (n = 6). A total of 30 patients were treated within phase I–II study, the rest outside the trial. Most patients had received extensive prior treatments (Table 1). The most common primary tumor site was oral cavity (37%). Median gross tumor volume (GTV) at the time of initial BNCT was 92 cm3 (range: 5–660 cm3).
Treatment planning
For contouring, planning computed tomography (CT) was co-registered with contrast-enhanced T1-weighted magnetic-resonance images (MRI) and optional 18F-BPA-positron emission tomography (PET). CT was used to construct the 3D-model. Treatment planning was performed using the Monte Carlo software SERA (Simulation Environment for Radiotherapy Applications; Idaho National Laboratory, Idaho Falls, ID). The SERA system is not compatible for re-segmentation or recalculations anymore, and the FiR 1 beam model is not available in current treatment planning systems (TPS).
The elemental compositions of tissues were defined according to the International Commission on Radiation Units & Measurements (ICRU) Report 46 [17]. The voxel size for dose calculation was 1 cm3.
The dose weighted with relative biological effectiveness (DW) of BNCT is expressed as the sum of the four dose components: boron, gamma, nitrogen capture and fast neutron dose. Each dose component is multiplied by a constant weighting factor (wi), except for the boron dose, which is multiplied with boron carrier and tissue-specific compound biological effectiveness (CBE) factor [18]. DW aims to describe the equivalent photon dose that causes the same effect as BNCT and is expressed in unit Gy(W).

where DB is boron dose, Dg gamma, DN nitrogen capture and Dfast_n fast neutron dose.
Weighting factors were 1 for gamma, 3.2 for nitrogen capture and fast neutrons and 3.8 and 2.5 for boron in tumor and mucosa, respectively [19]. Weighted doses to the tumor, target volume and sensitive tissues were calculated based on the average boron concentration in whole blood during irradiation. A boron concentration ratio of 3.5:1 was assumed for tumor-to-blood, and 2:1 for mucosal membrane-to-blood [16].
The dose to the mucosal membrane was one of the dose-limiting factors in BNCT, restricted to 6 Gy or less per treatment, corresponding to approximately 13.5 Gy(W). Tumor dose varied according to safety limits of normal tissues. Mucosal membrane was not contoured in the treatment planning process. Instead, the maximum dose was visually estimated based on the isodose contours calculated on CT images.
Additionally, the maximum weighted dose to the oral mucosa was calculated. As the elemental composition of oral mucosa is not well-established, the dose was estimated using the nitrogen concentration of skin tissue (N = 4.2%) [20].
Treatment
The patients were scheduled to receive two BNCT treatments at 3–5 weeks intervals, and 52% completed both. Irradiation was performed using the 250 kW FiR TRIGA Mark II reactor (General Atomics, San Diego, CA), located in Espoo, Finland. L-BPA was manufactured by Interpharma Praha (Prague, Czech Republic).
Patients received a 2-hour intravenous infusion of L-BPA at 400 mg/kg. Blood samples were taken before the start of L-BPA infusion, at approximately 20-minute intervals during and after the infusion, and after irradiation of each field. Blood boron concentration was analyzed using inductively coupled plasma atomic emission spectrometry (ICP-AES). Average boron concentration during irradiation was based on the estimation of pharmacokinetic models [21].
Irradiation began approximately 1.5 hours after completing the L-BPA infusion. It was delivered via one to three fields, typically two opposing lateral or anterior-lateral circularly collimated fields.
Patients received cetirizine hydrochloride 10 mg before L-BPA infusion. Dexamethasone 10–15 mg was administered daily after completion of the infusion to prevent radiation-associated edema and was tapered over 3–4 weeks.
Follow up and evaluation of OM
Trial patients had a follow-up visit 1 month after BNCT treatment, then every 12 weeks. Patients treated outside of the trial did not have a specific follow-up schedule. OM data in this study were obtained within 1 month after the first treatment. If the patients underwent two BNCT treatments, only the OM status after the initial treatment was evaluated.
OM is defined as inflammation and ulceration of oral mucosal membranes. OM was assessed using the National Cancer Institute Common Toxicity 3.0 criteria (NCICT 3.0), where grade 3 is defined as confluent ulcerations or pseudomembranes with bleeding with minor trauma.
Statistical analysis
Association between grade 3 OM and patient characteristics and treatment-related parameters was analyzed using binary logistic regression (IBM SPSS Statistics,Version: 29.0.0.0(241)). The relationship between grade 3 OM and age, and grade 3 OM and the maximum oral mucosa dose, were analyzed using the Kruskal–Wallis test. Statistical significance was set at p < 0.05.
A sigmoidal normal tissue complication probability (NTCP) model was created by dividing the patients into four groups (n = 23 each) based on the magnitude of the maximum mucosal dose (mean group doses: 9.9, 11.8, 12.8 and 13.9 Gy(W)). The probability of grade 3 OM was calculated for each dose group based on observed responses. As a simple theoretical approach, a sigmoid curve was fitted to the data.

where D is the maximum mucosal dose, D50 the dose causing 50% probability of grade 3 OM and k the curve steepness.
Results
Among 92 patients, 15% had no OM, 15% developed grade 1, 27% grade 2 and 42% grade 3 OM. No grade 4 or 5 events occurred. Among patients (Table 1), only older age was significantly associated with a higher prevalence of grade 3 OM (p < 0.032) (Figure 1A). Patients with grade 3 OM had a higher mean age of 63 years (range 39–80 years), compared to 58 years (range 17–81 years) in those with lower-grade OM. No other factors showed a significant correlation with grade 3 OM.
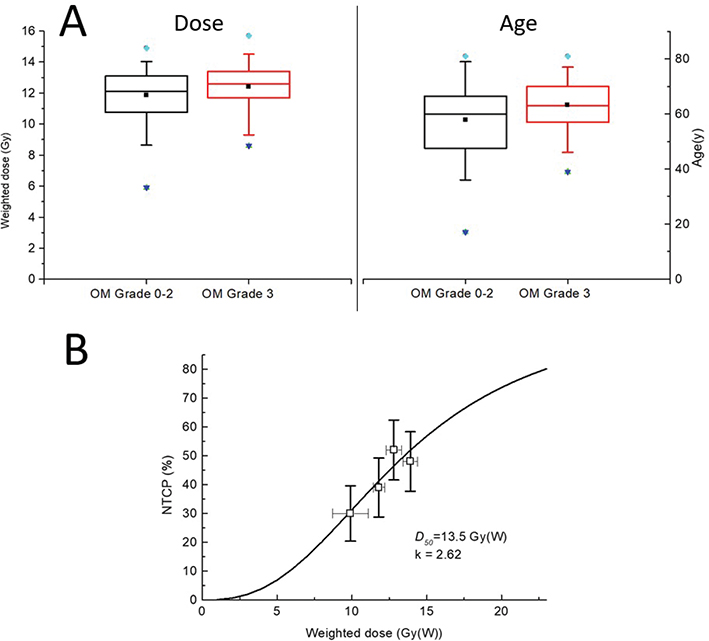
Figure 1. (A) Box plots of maximum oral mucosa dose and grade 3 oral mucositis, and between patient age and grade 3 oral mucositis. (B) Observed normal tissue complication probabilities (NTCP) of Grade 3 OM as mean (open squares) ± SD and the fitted sigmoidal model (solid line) where the 50% complication rate D50 = 13.5 Gy(W).
BNCT oral mucosa dose-response
Maximum oral mucosa doses varied considerably (Table 2). Patients with grade 3 OM had median maximum dose 12.6 Gy(W) (range: 8.6–15.7 Gy(W)). Although the difference in median dose between grade 3 and grade 0–2 OM groups was not statistically significant (p = 0.123), a trend toward higher doses was observed in the grade 3 group (Figure 1A). The NTCP curve estimated a D50 of 13.5 Gy(W), indicating a 50% probability of grade 3 OM, with a steepness factor k = 2.62 (Figure 1B).
Discussion and conclusion
To our knowledge, no previous clinical BNCT studies have reported NTCP-derived D50-values for predicting grade 3 OM. An NTCP model by González et al. [22], based on photon radiotherapy patient data from Strigari et al. [23], predicts a somewhat higher D50 of approximately 17 Gy.
The median tumor size in present study was 92 cm3, with the maximum oral mucosa limited to 13.5 Gy(W). In contrast, Wang et al. and Takeno et al. reported notably lower grade 3 OM rates (29 and 5%, respectively), but their median tumor sizes were substantially smaller – 15.6 and 6.9 cm3, respectively [10, 12]. Furthermore, Wang et al. limited the maximum oral mucosa dose to 10 Gy(W) and Takeno et al. to 12 Gy(W), assuming a boron concentration equal to that of blood and a boron dose weighting factor of 4.9. Both continued L-BPA infusion during irradiation, unlike our protocol.
In our study, tumor size and location did not correlate with grade 3 OM. This may be biased by a relatively large irradiated volume (2–3 fields with 11 or 14cm apertures), including nearly entire oral cavity in most cases to reach dose coverage within large GTVs [24].
The prevalence of grade 3 OM was higher among the elderly patients, although the difference was modest. There is no strong evidence in literature regarding the relationship between older age and radiation-induced OM. It is possible that aging can cause slower tissue healing [25, 26].
Severe OM is common in HN radiotherapy (up to 66%) [25]. After all, it is typically reversible and generally considered acceptable.
Study limitations
This retrospective study has several limitations. Patient heterogeneity and lack of detailed smoking and alcohol history limited risk factor analysis.
The SERA system is no longer available for resegmentation or calculations. The FiR 1 beam model is not available in the current TPS. Due to relatively large irradiation fields, the dose distribution across the mucosal surfaces was fairly homogeneous. Therefore, the primary source of uncertainty might not be the variability in physical dose, but rather the distribution of boron. Average boron concentrations were only available for dose estimation. Although detailed contouring of the mucosal structures was not performed, mucosal dose was evaluated following standard clinical practice.
Conclusions
Higher maximum oral mucosa doses were associated with an increased risk of grade 3 OM. Older age was the only other risk factor related to severe OM.
Acknowledgements
This work was supported by the Helsinki University Clinical Research Funding and by the Academy of Finland.
BIGART 2025 was financially supported by the Acta Oncologica Foundation.
Data availability statement
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data are not available.
Ethics declarations & trial registry information
According to the Finnish regulation for research, no ethics committee approval is needed in retrospective register-based studies. The authorities of HUCH gave permission for this retrospective registry-based study. All data are stored and handled according to General Data Protection Regulation (GDPR).
Author contributions
Study was designed by Tanja Mälkiä, Hanna Koivunoro, Liisa Porra, Anu Anttonen, Tiina Seppälä, Mikko Tenhunen and Heikki Joensuu. Tanja Mälkiä, Leena Kankaanranta, Tiina Seppälä and Hanna Koivunoro contributed to data acquisition. Mikko Tenhunen designed the NTCP model and sigmoidal curve. All authors contributed to the revision of the manuscript and had final approval of the submitted version.
References
[1] Argiris A, Karamouzis MV, Raben D, Ferris RL. Head and neck cancer. Lancet. 2008;371(9625):1695–709. https://doi.org/10.1016/S0140-6736(08)60728-X
[2] Rettig EM, D’Souza G. Epidemiology of head and neck cancer. Surg Oncol Clin N Am. 2015;24(3):379–96. https://doi.org/10.1016/j.soc.2015.03.001
[3] Wong LY, Wei WI, Lam LK, Yuen APW. Salvage of recurrent head and neck squamous cell carcinoma after primary curative surgery. Head Neck. 2003;25(11):953–9. https://doi.org/10.1002/hed.10310
[4] Gilbert H, Kagan AR. Recurrence patterns in squamous cell carcinoma of the oral cavity, pharynx, and larynx. J Surg Oncol. 1974;6(5):357–80. https://doi.org/10.1002/jso.2930060502
[5] Tan HK, Giger R, Auperin A, Bourhis J, Janot F, Temam S. Salvage surgery after concomitant chemoradiation in head and neck squamous cell carcinomas – stratification for postsalvage survival. Head Neck. 2010;32(2):139–47. https://doi.org/10.1002/hed.21159
[6] Vargo JA, Ward MC, Caudell JJ, Riaz N, Dunlap NE, Isrow D, et al. A multi-institutional comparison of SBRT and IMRT for definitive reirradiation of recurrent or second primary head and neck cancer. Int J Radiat Oncol Biol Phys. 2018;100(3):595–605. https://doi.org/10.1016/j.ijrobp.2017.04.017
[7] Ward MC, Riaz N, Caudell JJ, Dunlap NE, Isrow D, Zakem SJ, et al. Refining patient selection for reirradiation of head and neck squamous carcinoma in the IMRT era: a multi-institution cohort study by the MIRI collaborative. Int J Radiat Oncol Biol Phys. 2018;100(3):586–94. https://doi.org/10.1016/j.ijrobp.2017.06.012
[8] Suzuki M, Kato I, Aihara T, Hiratsuka J, Yoshimura K, Niimi M, et al. Boron neutron capture therapy outcomes for advanced or recurrent head and neck cancer. J Radiat Res. 2014;55(1):146–53. https://doi.org/10.1093/jrr/rrt098
[9] Kankaanranta L, Seppälä T, Koivunoro H, Saarilahti K, Atula T, Collan J, et al. Boron neutron capture therapy in the treatment of locally recurred head-and-neck cancer: final analysis of a phase I/II trial. Int J Radiat Oncol Biol Phys. 2012;82(1):e67–75. https://doi.org/10.1016/j.ijrobp.2010.09.057
[10] Wang L-W, Chen Y-W, Ho C-Y, Liu YH, Chou F, Liu Y, et al. Fractionated boron neutron capture therapy in locally recurrent head and neck cancer: a prospective phase I/II trial. Int J Radiat Oncol Biol Phys. 2016;95(1):396–403. https://doi.org/10.1016/j.ijrobp.2016.02.028
[11] Koivunoro H, Kankaanranta L, Seppälä T, Haapaniemi A, Mäkitie A, Joensuu H. Boron neutron capture therapy for locally recurrent head and neck squamous cell carcinoma: an analysis of dose response and survival. Radiother Oncol. 2019;137:153–8. https://doi.org/10.1016/j.radonc.2019.04.033
[12] Takeno S, Yoshino Y, Aihara T, Higashino M, Kanai Y, Hu N, et al. Preliminary outcomes of boron neutron capture therapy for head and neck cancers as a treatment covered by public health insurance system in Japan: real-world experiences over a 2-year period. Cancer Med. 2024;13(11):e7250. https://doi.org/10.1002/cam4.7250
[13] Sato M, Hirose K, Takeno S, Aihara T, Nihei K, Takai Y, et al. Safety of boron neutron capture therapy with Borofalan(10B) and its efficacy on recurrent head and neck cancer: real-world outcomes from nationwide post-marketing surveillance. Cancers (Basel). 2024;16(5):869. https://doi.org/10.3390/cancers16050869
[14] Barth RF, Coderre JA, Vicente MGH, Blue TE. Boron neutron capture therapy of cancer: current status and future prospect. Clin Cancer Res. 2005;11(11):3987–4002. https://doi.org/10.1158/1078-0432.CCR-05-0035
[15] Coderre JA, Morris GM, Kalef-Ezra J, Micca PL, Ma R, Youngs K, et al. The effects of boron neutron capture irradiation on oral mucosa: evaluation using a rat tongue model. Radiat Res. 1999;152(2):113–18. https://doi.org/10.2307/3580083
[16] Kankaanranta L, Seppälä T, Koivunoro H, Saarilahti K, Atula T, Collan J, et al. Boron neutron capture therapy in the treatment of locally recurred head and neck cancer. Int J Radiat Oncol Biol Phys. 2007;69(2):475–82. https://doi.org/10.1016/j.ijrobp.2007.03.039
[17] International Commission on Radiation Units & Measurements. ICRU report 46: photon, electron, proton, and neutron interaction data for body tissues. Bethesda, MD: International Commission on Radiation Units & Measurements; 1992.
[18] International Atomic Energy Agency. Current status of neutron capture therapy (IAEA-TECDOC-1223 report). Vienna: International Atomic Energy Agency; 2001.
[19] Coderre JA, Morris GM. The radiation biology of boron neutron capture therapy. Radiat Res. 1999;151(1):1–18. https://doi.org/10.2307/3579742
[20] International Commission on Radiation Units & Measurements. ICRU report 44: tissue substitutes in radiation dosimetry and measurement. Bethesda, MD: International Commission on Radiation Units & Measurements; 1989.
[21] Ryynänen PM, Kortesniemi M, Coderre JA, Diaz AZ, Hiismäki P, Savolainen SE. Models for estimation of the (10)B concentration after BPA-fructose complex infusion in patients during epithermal neutron irradiation in BNCT. Int J Radiat Oncol Biol Phys. 2000;48(4):1145–54. https://doi.org/10.1016/s0360-3016(00)00766-5
[22] González SJ, Pozzi ECC, Monti Hughes A, Provenzano L, Koivunoro H, Carando DG, et al. Photon iso-effective dose for cancer treatment with mixed field radiation based on dose-response assessment from human and an animal model: clinical application to boron neutron capture therapy for head and neck cancer. Phys Med Biol. 2017;62(20):7938–58. https://doi.org/10.1088/1361-6560/aa8986
[23] Strigari L, Pedicini P, D’Andrea M, Pinnarò P, Marucci L, Giordano C, et al. A new model for predicting acute mucosal toxicity in head-and-neck cancer patients undergoing radiotherapy with altered schedules. Int J Radiat Oncol Biol Phys. 2012;83(5):e697–702. https://doi.org/10.1016/j.ijrobp.2012.02.004
[24] Konijnenberg MW, Dewit LG, Mijnheer BJ, Raaijmakers CP, Watkins PR. Dose homogeneity in boron neutron capture therapy using an epithermal neutron beam. Radiat Res. 1995;142(3):327–39. https://doi.org/10.2307/3579142
[25] Elting LS, Cooksley CD, Chambers MS, Garden AS. Risk, outcomes, and costs of radiation-induced oral mucositis among patients with head-and-neck malignancies. Int J Radiat Oncol Biol Phys. 2007;68(4):1110–20. https://doi.org/10.1016/j.ijrobp.2007.01.053
[26] Goel G, Alice KP, Negi P, Aggarwal N. Factors influencing radiation induced oral mucositis in head and neck cancer. J Cancer Res Ther. 2024;20(5):1564–9. https://doi.org/10.4103/jcrt.jcrt_1200_23