ORIGINAL ARTICLE
Predicting neoadjuvant chemotherapy treatment response in hormone-receptor-positive/HER2-negative breast cancer – results from the Swedish SCAN-B population-based cohort
Niklas Lomana,b,c  , Hani Saghira,c,d and Siker Kimbunga,c
, Hani Saghira,c,d and Siker Kimbunga,c
aDivision of Oncology, Department of Clinical Sciences, Lund University, Lund, Sweden; bDepartment of Hematology, Oncology and Radiation Physics, Lund University Hospital, Malmö/Lund, Sweden; cLund University Cancer Center, Lund, Sweden; dDepartment of Hematology, Sahlgrenska University Hospital, Gothenburg, Sweden
ABSTRACT
Background and purpose: Hormone-receptor-positive/HER2-negative (HR+/HER2-) early-stage breast cancers (EBCs) display heterogenous responses to neoadjuvant chemotherapy (NACT) warranting biomarkers to tailor optimal treatment for individual patients.
Patients/material and methods: Women with HR+/HER2- EBC (N = 178) included in the Swedish Sweden Cancerome Analysis Network-Breast (SCAN-B) population-based cohort (2010–2019) treated with NACT were included. We analyzed rates of pathologic complete response (pCR), objective response (OR), breast conserving surgery (BCS), and recurrence-free interval (RFI) in subgroups defined by baseline clinicopathological and molecular characteristics.
Results: The pCR rate was low (6%); nonetheless, after a median follow-up of 5.41 years, all patients who achieved pCR remained recurrence-free despite uniform baseline predicted high PAM50 risk of recurrence (ROR). Younger age (≤ 40 years), cT1, ER% positivity (≤ 66%), and negative PR (≤ 10%) were conventional clinicopathological factors positively associated with increased pCR. Molecular predictors of pCR included negative HR status by gene-expression signatures and non-luminal PAM50 subtypes. Tumor shrinkage ≥ 30%, i.e., OR and BCS, was achieved in 59% and 34%, respectively. No factor was significantly associated with ORR, whereas non-lobular histology and cT1 were positively associated with BCS. In addition, only 1/49 patients who underwent BCS experienced a recurrence during follow-up. Low/intermediate ER% positivity, PR negativity, and non-luminal PAM50 subtype were baseline factors univariately prognostic for inferior long-term outcome in case of residual disease.
Interpretation: Baseline characteristics indicative of reduced hormonal signaling and non-luminal tumor biology assessed more precisely using mRNA profiling can guide optimal tailoring of NACT for patients with high-risk HR+/HER2-tumors. Baseline molecular biology did not predict surgical outcomes following NACT.
KEYWORDS: Neoadjuvant chemotherapy; hormone-receptor-positive; optimal response; endocrine responsiveness; personalized treatment
Citation: ACTA ONCOLOGICA 2025, VOL. 64, 1577–1589. https://doi.org/10.2340/1651-226X.2025.44201.
Copyright: © 2025 The Author(s). Published by MJS Publishing on behalf of Acta Oncologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Received: 22 June 2025; Accepted: 3 November 2025; Published: 19 November 2025
CONTACT: Niklas Loman Niklas.loman@med.lu.se Division of Oncology, Department of Clinical Sciences, Lund University, Medicon Village Building 404, SE-22381 Lund, Sweden
Supplemental data for this article can be accessed online at https://doi.org/10.2340/1651-226X.2025.44201
Competing interests and funding: The authors report there are no competing interests to declare.
Introduction
Hormone-receptor-positive (HR+) and human epidermal growth factor receptor 2-negative (HER2-) breast cancer (BC) constitute ~70% of all breast malignancies and display substantial pathological and molecular heterogeneity, which impact treatment response and prognosis [1–3]. HR+/HER2- BC is often detected as a surgically resectable tumor allowing for upfront surgery followed by molecularly driven adjuvant treatment choices, as accessible. For patients presenting with larger tumors, a substantial lymph nodal burden, or those who may favor the less radical breast conservating surgery (BCS) as opposed to mastectomy, neoadjuvant therapy may be offered [4]. The decision to provide neoadjuvant chemotherapy (NACT) for patients with HR+/ HER2-tumors is still based on conventional clinical and pathological features rather than molecular/genomic biomarkers, in stark contrasts with the adjuvant setting where various gene-expression signatures have been widely adopted to support decision-making about chemotherapy use [5–7]. Without robust molecular biomarker-driven strategies, treatment selection based solely on the tumor staging is limited by the risk for exposing and/or overtreating patients with highly toxic drugs without guarantees of a meaningful clinical benefit.
Multiple randomized clinical trials have demonstrated that administering chemotherapy before surgery does not compromise long-term survival [8, 9] in spite of delaying the time to removal of the tumor, expanding clinical adoption of NACT. Moreover, providing chemotherapy treatment preoperatively allows for in vivo assessment of treatment response, opening avenues for tailoring adjuvant treatment according to response [4]. Pathologic complete response (pCR) following NACT is a robust prognostic biomarker for excellent long-term outcomes at the individual patient level, but pCR rates are substantially low (~5–15%) among patients with HR+/HER2- BC [10, 11]. Nonetheless, adjuvant endocrine therapy significantly improves long-term prognosis for patients with HR+/HER2- BC [12–14].
Although achieving a pCR is most desirable, the possibility for surgical down-staging remains a key outcome after NACT, especially in patients with large HR+/HER2- early-stage breast cancer (EBC). BCS rates up to 50% have been reported after NACT for such patients [15–17], indicating many patients do not achieve this clinical benefit. Response predictive markers are therefore needed to optimize NACT usage in this diverse clinical subtype of BC. Herein, we explore clinical, pathological, and molecular features associated with pCR, objective response (OR), BCS, and prognosis after NACT among patients with HR+/HER2- early BC included in the Sweden Cancerome Analysis Network-Breast (SCAN-B) cohort between 2010 and 2019.
Patients/material and methods
Patients
SCAN-B comprises a population-based consecutively enrolled series of BC patients accrued at nine hospitals in the Skåne, Uppland, and Småland healthcare regions in Sweden for the purpose of analyzing breast tumors using whole-genome RNA sequencing (RNAseq) technology [18–20]. The SCAN-B research database (inclusion period 2010–2019) was reviewed to identify women treated with NACT. The availability of relevant biomarker information assessed on the preoperative core needle biopsy (CNB) was necessary. Refer to the consort diagram (Figure 1) for details about subcohort selection for the current analyses.

Figure 1. Consort diagram showing patient and tumor selection for inclusion in the analyses reported in the current study.
Patient and tumor characteristics
Information about patient demographics, conventional tumor histo-pathology characteristics, medical treatments, and pathological and surgical outcome after NACT were retrieved from the Swedish national quality register for BC (NKBC) [21] and complemented with review of patient medical records wherever possible. Preoperative anthracycline- and taxane-based chemotherapy regimens followed by postoperative endocrine therapy were the standard treatment regimen for patients with locally advanced inoperable HR+/HER2- tumors during the inclusion period. Neither neo-adjuvant endocrine treatment (NET), post-NACT nor adjuvant CDK 4/6 inhibitor was the standard treatment in Sweden between 2010 and 2019. Central reevaluation of biomarkers was not performed; hence, our results capture real-world experiences. Biomarkers were assessed on pre-treatment core biopsies only. Protocols and cutoffs for routine evaluation of tumor histology and hallmark biomarkers (ER, PR, HER2, and Ki67) status are described in guidelines published by the Swedish society of pathologists (KVAST) [22]. To explore the diverse expression of ER between tumors, we split the percentage ER positivity into three categories: low (≤ 10%), intermediate (11%–66%), and high (> 66%). The threshold for the low ER group was set at the ≤ 10% to reflect the recognized differential biology of ‘ER-low; 1–10%’ tumors [23–25]. HR+ tumors with low/intermediate ER positivity not only are more likely to be sensitive to NACT [25] but also represent a group where additional measures are needed in case of residual cancer at surgery. A threshold of 20% immunohistochemical staining was applied in the material description to discriminate between high vs. low proliferative disease. Although imperfect, this is a threshold generally utilized in clinical practice, e.g., in the monarchE study to identify patients eligible for the addition of adjuvant CDK 4/6 inhibitor treatment [26].
RNA sequencing-derived hallmark features
The description of SCAN-B procedures for tissue collection, RNA sequencing, data cleaning, and the development of RNAseq-derived single sample predictor (SSP) models for annotating ER, PR, and Ki67 status and the PAM50 molecular subtypes and PAM50 genomic risk of recurrence (ROR) scores and risk category class have been published [18–20].
Statistical analysis
Analyses in this study are restricted to patients with HR+/HER2- tumors, unless otherwise stated. The association of clinical pathological and molecular factors with time independent outcomes (pCR, OR, and surgical procedure) was evaluated using Fisher’s exact tests and logistic regression models outputting odds ratios (ORs) and 95% confidence interval (CI). Kaplan-Meier plots and Log-rank tests were used to analyze associations of pathological and surgical outcomes with recurrence-free survival (RFI) as defined by the Standardized Definitions for Efficacy End Points (STEEP) criteria [27]. RFI was defined as the time from BC diagnosis until any recurrence (local, regional, or distant) with death being a censoring event. All statistical tests were two-sided, and p-values < 0.05 were considered significant. Analyses were performed using SPSS v29 (IBM Corporation, Armonk, NY, USA).
Results
Patient and tumor characteristics at baseline
In this SCAN-B cohort of N = 424 patients who received NACT, 178 (42%) patients presented with clinical HR+/HER2- tumors (Figure 1) and are the focus of this study. Using the Swedish immunohistochemical (IHC) cut-off (≤ 10%) for HR positivity, 80% versus 18% versus 2% were ER+/PR+ versus ER+/PR- versus ER-/PR+, respectively. The median age at diagnosis was 55 years (range 25–75 years), median radiological tumor size was 30 mm (range 9–120 mm), 87% had positive nodal involvement, 88% had clinical stage I&II disease (AJCC 8th edition), and 78% of tumors were invasive ductal carcinomas. Most (89%) showed high ER% positivity (> 66%) by IHC, and 82% were considered highly proliferative (Ki67 > 20%) (Table 1), reflecting common characteristics for selecting patients for preoperative chemotherapy. Similarly using RNAseq-derived SSPs, 91% were ER positive, 67% were PR-positive, 70% were highly proliferative (Ki67), 79% were assigned a PAM50 luminal subtype, and 81% were classified as genomic high-risk category by SSP-ROR (Table 1). Notably, all (100%) combined HR-negative cases by SSP were classified non-luminal by PAM50, and most (75%) had a predicted high genomic ROR. Prevalent clinicopathological characteristics among patients with non-luminal tumors included older age (74%), larger tumors (81%), nodal positivity (84%), high proliferation (91%), and invasive ductal histology (79%).
Concordance between IHC and molecular biomarkers
The agreement between the IHC versus SSP status for ER and PR was 93% (kappa 0.33) and 79% (kappa 0.44), respectively. Discordant cases mainly switched from IHC-positive to SSP-negative; 100% and 83% for ER and PR status, respectively. Most IHC low/intermediate (≤ 66%) ER% positive and PR-negative tumors were non-luminal by PAM50 and had high genomic ROR (Supplementary Figure 1).
Association of pCR with conventional clinicopathological characteristics among patients with clinical HR+/HER2– tumors
pCR was defined as the disappearance of all signs of invasive cancer in the breast and axillary nodes (ypT0 ypN0). Only 6% (11/178) of patients with clinical HR+/HER- BC achieved a pCR (Figure 2a). Younger age at diagnosis (≤ 40 years) was associated with higher odds for pCR (OR = 4.7, 95% CI 1.3–16.7, Figure 2b). Age cut-off of 40 years is supported by results from the SOFT/TEXT trials, suggesting that patients with younger age have more aggressive tumors and worse 12-year overall survival [28, 29]. Patients with cT1 tumors were more likely to achieve a pCR compared to cT2-T3 tumors (13% vs. 9%, p = 0.038, Figure 2c), but histological subtype (p = 0.269; Figure 2d) and clinical stage (p = 1.0, Figure 2e) did not impact the rate of pCR. To further evaluate the pathological response to NACT, we explored the objective response rate (ORR) in relation to baseline characteristics. OR was calculated as > 30% percent reduction in tumor size when comparing preoperative ultrasound to the pathological size of the residual cancer (pre-surgical radiological size was not available), to mimic the RECIST 1.1 criteria for treatment response [30]. Optimally, the same imaging modality should be used to determine ORR. ORR for the clinical HR+/HER2- subtype was 59%; however, no baseline clinicopathological or molecular factor significantly associated with OR in our cohort (Table 2).
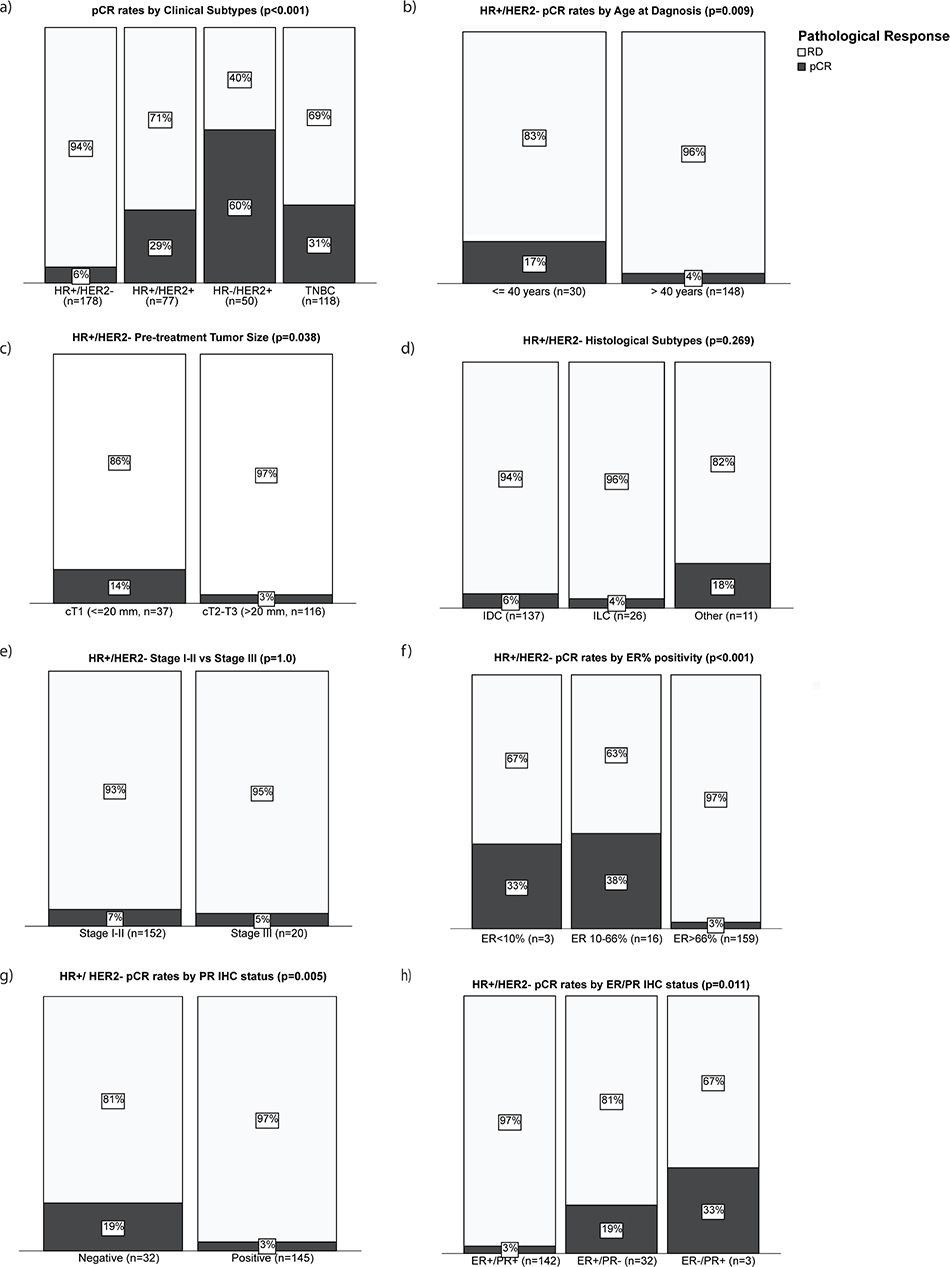
Figure 2. pCR rates by conventional clinicopathological features. Bar plots showing percentage of patients who achieved pCR (black) versus patients with residual cancer (white) by (a) clinical subtypes in all SCAN-B NACT cohort (n = 424), (b) age at diagnosis in HR+/HER2- disease, (c) pre-treatment tumor size in HR+/HER2- disease, (d) tumor histological subtypes in HR+/HER2- disease, (e) clinical disease stage in HR+/HER2- disease, (f) ER% positivity by IHC in HR+/HER2- disease, (g) PR status by IHC in HR+/HER2- disease, and (h) combined ER/PR status in HR+/HER2- disease. P-values are from Fisher’s exact 2-sided tests. Abbreviations: RD: residual disease; pCR: pathological complete response; IHC: immunohistochemistry.
The impact of the IHC quantitative HR% positivity on the pCR rate was next explored. Tumors with low (≤ 10%) and intermediate (11–66%) ER% positivity had higher pCR rates compared to high (> 66%) ER% positive tumors (33% vs. 38% vs. 3%, respectively; p < 0.001; Figure 2f). Similarly, pCR was more frequent among PR-negative (≤ 10%) compared to PR-positive (> 10%) tumors (19% vs. 3%, respectively; p = 0.005; Figure 2g). Furthermore, combined ER+/PR+ (> 10% cutoff for both receptors) was associated with the lowest pCR rate; 3% vs. 19% vs. 33% for ER+/PR+, ER+/PR-, and ER-/PR+, respectively (p = 0.011; Figure 2h).
Association of pCR with baseline molecular biomarkers among patients with clinical HR+/HER2– tumors
The odds for achieving a pCR was higher among clinical HR+ tumors classified by SSP to be ER-negative (OR = 4.5, 95% CI 1.1–19.5, Figure 3a) or PR-negative (OR = 11, 95% CI 2.3–52.7, Figure 3b). Moreover, combined ER-/PR- by SSPs was associated with a higher pCR rate (20%) compared to ER+/PR- (15%) or ER+/PR+ (2%), respectively (p = 0.002; Figure 3c). Note that no tumor was classified as ER-/PR+ by SSPs. Rates of pCR also varied significantly by PAM50 subtypes as follows: HER2-enriched (28%) versus basal (18%) versus LumB (4%) versus LumA (0%) [p < 0.001; Figure 3d]. Precisely, 8/11 (72%) patients who achieved a pCR had a non-luminal tumor by PAM50 classification, and all (11/11, 100%) were predicted to have a high genomic ROR (Figure 3e and f).
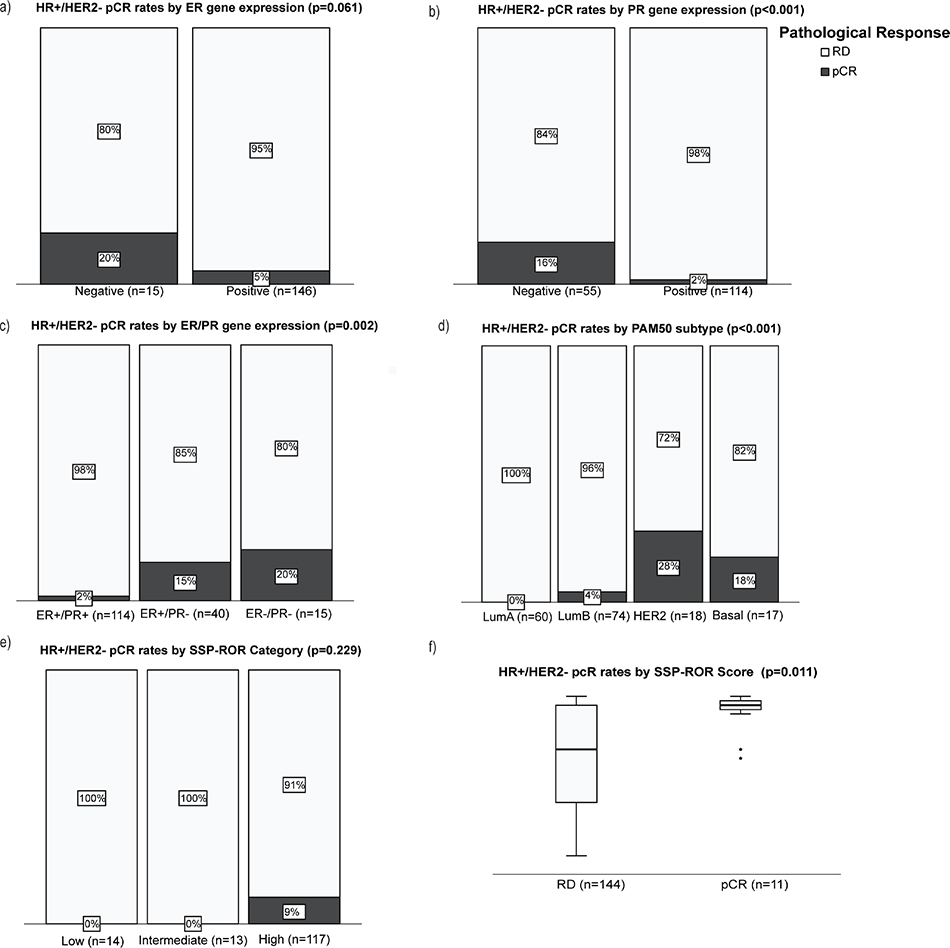
Figure 3. pCR rates by molecular (mRNA-based) biomarkers in HR+/HER2- disease. Bar plots showing percentages of patients who achieved pCR (black) versus patients with residual cancer (white) by (a) ER gene signature status, (b) PR gene signature status, (c) combined HR gene signature status, (d) PAM50 molecular subtype, and (e) genomic risk of recurrence (SSP-ROR) category. Continuous SSP-ROR scores between cases with pCR and residual disease (f). P-values are from Fisher’s exact 2-sided tests (a–e) and Mann-Whitney test (f).
Multivariable logistic regression analyses
Logistic regression analyses adjusted pairwise for covariates (pCR ~ biomarker + covariate) were performed to further understand the association between pCR and the biomarkers age at diagnosis (≤ 40 years vs. > 40 years), IHC ER% positivity (≤ 66% vs. > 66%), and PAM50 subtype (non-luminal vs. luminal A/B); Supplementary Table 1. Covariates included pre-treatment tumor size (≤ 20 mm vs. > 20 mm), clinical stage (I&II vs. III), IHC PR status (positive vs. negative), and histology subtype. Low/intermediate ER% positivity (≤ 66%) remained independently associated with higher odds for pCR in all pairwise adjusted models. Younger age at diagnosis was significantly associated with higher odds for pCR in all pairwise models except when adjusting for PAM50 subtype (p = 0.057). Likewise, non-luminal PAM50 subtype was significantly associated with higher odds for pCR in all pairwise except when adjusting for ER% positivity (p = 0.271). In a multivariable model that combined age, tumor size, ER% positivity, and PR status by SSP and PAM50 subtype, only ER% positivity and tumor size emerged as independent positive predictive factors for pCR after NACT (p = 0.012. and p = 0.008, respectively). Note that the PAM50 ROR category was exempted from these exploratory logistic regression analyses because all pCR cases converged within the high-risk category, making odds-ratio calculation unreliable due to the statistical problem of ‘complete separation’.
Association of surgical outcomes with baseline clinical and molecular factors and pathological response
The rate of BCS after NACT among patients with clinical HR+/HER2- subtypes was 34%. Smaller tumor size (cT1) and non-lobular histology were the only pathological factors positively associated with BCS over mastectomy in this cohort. Notably, neither baseline molecular characteristics nor ORR after NACT was associated with BCS versus mastectomy (Table 3).
Associations of recurrence-free interval (RFI) by baseline clinic-pathological and molecular biomarkers and post-NACT outcomes
RFI data were available for 172/178 patients with HR+/HER-, of which 24 registered an event during a median follow-up for RFI of 5.41 years (range 0.5–10.4 years). Despite the general high genomic ROR predicted at baseline, all patients who achieved a pCR remained disease-free during follow-up [HR = 0.05, 95% CI 0.00–59, Figure 4a]. Among patients with residual disease, younger age [≤ 40 years old; HR 2.1 (95% CI 0.82–5.3), Figure 4b] and larger tumor size [> 20 mm; HR = 5.6, 95% CI 0.74–41.6, Figure 4c] trended toward shorter RFI, while low/intermediate ER% positivity (≤ 66%) [HR = 3.9, 95% CI 1.3–11.5, Figure 4d], IHC PR negativity [HR = 3.3, 95% CI 1.4–7.8, Figure 4e], SSP PR-negative status (HR = 2.7, 95% CI 1.2–6.8, Figure 4f), and non-luminal PAM50 subtype [HR = 2.9, 95% CI 1.2–6.8, Figure 4g] were significant univariate predictors of inferior RFI. Likewise, patients with predicted high PAM50 ROR displayed a non-significant trend for worse prognosis relative to low/intermediate ROR categories (HR = 1.98, 95% CI 0.46–8.6, Figure 4h). Interestingly, BCS was associated with significantly fewer RFI events compared to mastectomy [HR = 0.09, 95% CI 0.01–0.7, Figure 4i]. Nevertheless, no factor was independently prognostic for RFI in multivariable analyses (Supplementary Table 2).
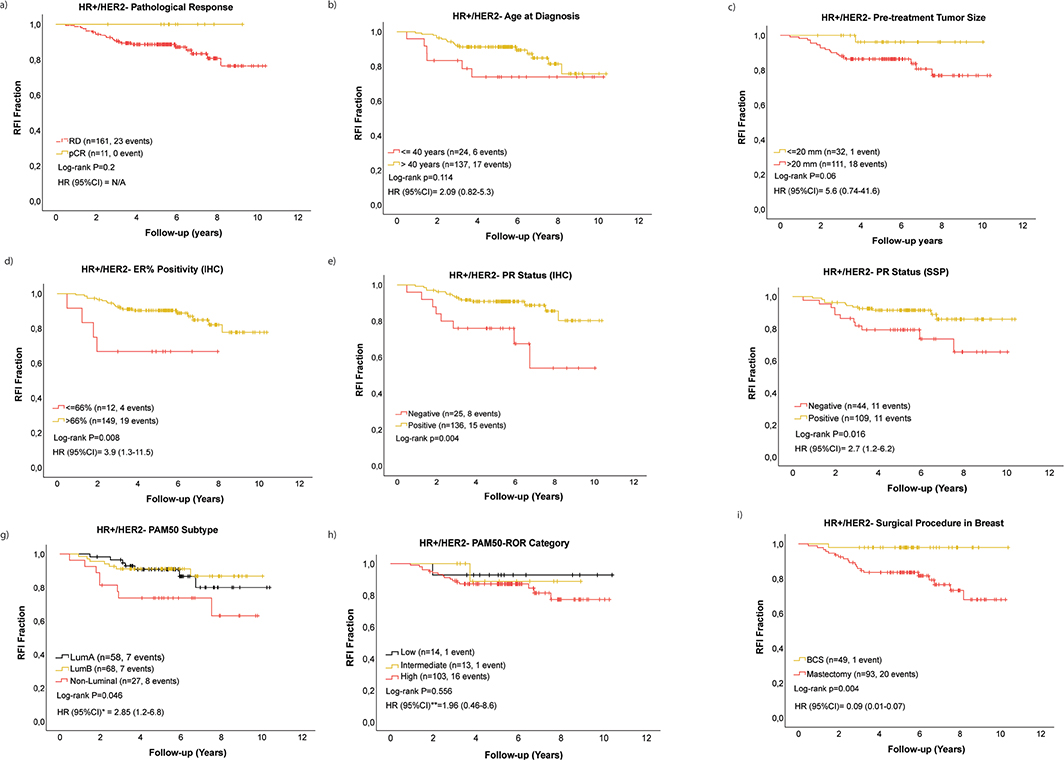
Figure 4. Recurrence-free interval (RFI) stratified by pCR status among all patients with HR+/HER2- tumors (a). RFI among patients with HR+/HER2- with residual disease stratified by age at diagnosis (b), pre-treatment tumor size (c), ER% positivity IHC (d), PR status IHC (e), PR status SSP (f), PAM50 subtype (g), PAM50-ROR category class (h), and breast surgery procedure (i).
*represents HR (95% CI) for Non-luminal versus Lum A/B.
**represents HR (95% CI) for PAM50-ROR category class high versus low/intermediate.
N/A because hazard ratio and confidence intervals cannot be computed due to no pCR event in the pCR group.
Discussion and conclusion
NACT is still used in the clinical management of early HR+/HER2-, despite the low likelihood for pCR, a less pronounced prognostic value, and the effect on adjuvant treatment. In this Swedish population-based SCAN-B cohort, over 40% of the women who received NACT as part of their oncological treatment between 2010 and 2019 presented with HR+/HER2- tumors, with only 6% achieving a pCR after NACT. The observed low pCR rate is consistent with previous studies [25, 31–33] and reinforces the necessity for optimal tailoring of chemotherapy treatment preoperatively in high-risk HR+/HER2- EBC. Standard clinicopathological biomarkers including younger age at diagnosis (≤ 40 years), cT1, low/intermediate ER% score (≤ 66%), and PR negativity (≤ 10%) univariately predicted higher pCR potential in our cohort. The association of cT1 with pCR (5 of 11 pCR cases were cT1) is surprising, but we noted that the responding cT1 tumors were biologically non-luminal (4/5 were non-luminal subtype). Huppert et al. [25] also found a positive association between pCR and low/intermediate ER% positivity (≤ 66), whereas another study including 10 neoadjuvant trials from the German Breast Group reported double pCR rates among ER+/PR- compared to ER+/PR+ tumors [33]. Claims of higher benefits of chemotherapy in premenopausal patients are however well documented in literature [6]. However, no factor was independently prognostic of pCR in our cohort, likely due to small subgroup sizes, which underpowered statistical analyses.
The biological and prognostic diversity within clinical HR+/HER2- EBC is well captured by gene-signatures and genomic prognostic scores, which are mostly clinically implemented in guiding adjuvant treatment decisions. The value of mRNA assays is not firmly established in preoperative treatment in HR+/HER2- EBC, where biomarkers for tailoring optimal treatment are needed. We explored the predictive and prognostic value of our SCAN-B developed RNAseq SSPs [19] for response to NACT in HR+/HER2- EBC. The HR SSPs assigned a ‘negative’ expression label to a substantial fraction of clinical HR+/HER2- tumors in our cohort, and one fifth was assigned a non-luminal PAM50 subtype, confirming that significant heterogeneity related to HR signaling persists within this clinical subgroup [7, 34]. Importantly, decreased hormonal signaling and non-luminal traits were predictive of higher pCR rates, underscoring the proven benefit of chemotherapy for typical endocrine non-responsive tumors [35]. In line with our results, Ohara et al. [36] reported a higher pCR rate among non-luminal PAM50 intrinsic subtypes while Whitworth et al. [34] and Huppert et al. [25] reported higher pCR rates for Blueprint-Basal-type subtype within clinical HR+/HER2- EBC. We observe that no LumA tumor in our series achieved a pCR, highlighting their intrinsic resistance to chemotherapy and projecting LumA subtype as a biomarker for non-pCR. Luminal A-like tumors (IHC-based) also presented with very low pCR rate in the large meta-analysis by Cortazar et al. [35]. Nonetheless, a few patients with low-grade luminal EBC still experience significant long-term benefits from (neo)adjuvant chemotherapy despite not achieving a pCR [37], thanks to adjuvant endocrine therapies.
Our SCAN-B developed PAM50 ROR score, and risk category class [19] assigned 81% of our cohort into the high-risk category at baseline. Notably, all patients with pCR were also predicted to have high genomic ROR. Though exploratory, our results align with previous studies reporting higher pCR rates among genomic high-risk categories assigned by signatures such as PAM50-ROR, OncotypeDX, Mammaprint, Blueprint, and EndoPredict [14, 25]. Larger and prospective studies are required to firmly establish the role of these molecular signatures in preoperative HR+/HER2- EBC. NET alone is nowadays recommended for strongly HR+ tumors, based on comorbidities or low-risk luminal biology based on clinical characteristics and/or genomic signatures, but NACT remains a therapeutic contender for a selected few. Adjuvant CDK 4/6-based treatment today is offered to patients with intermediate or high risk. Although the treatment may be well tolerated, it is obvious that it leads to a prolonged treatment period (an additional 2–3 years of treatment), and potentially complicating rehabilitation and thereby delaying reentry to the patients ‘healthy life’. Adjuvant CDK-inhibitor treatment also comes with a high cost both for the drug itself and most likely also associated with a prolonged period on sick-leave. Additional prognostic information acquired as a consequence of preoperative treatment potentially could be helpful in selecting patients who could potentially omit such additional treatment modalities.
Although an OR (≥ 30% tumor shrinkage) was achieved in 59% of HR+/HER2- tumors after NACT in our cohort, no baseline patient or tumor characteristic was significantly associated with tumor shrinkage besides the unexpected link between cT1 and pCR. Predicting the potential for BCS upfront NACT treatment remains a clinical challenge. The rate of BCS after NACT in our cohort was 34% similar to rates reported for HR+/HER2- tumors in the ACOSOG Z1701 Alliance trial from 2009 to 2011 [15]. Rates of BCS up to 50% were reported in another large cohort of HR+/HER2- tumors (2011–2016; n = 2,237), although this high BCS rate was associated with a higher rate of involved margins [16]. Interestingly, ORR was not associated with BCS. In fact, 80% of the patients who achieved a pCR had a mastectomy compared to 66% mastectomy rate among cases with residual disease. Small tumor size and non-lobular histology were the only baseline factors univariately associated with lumpectomy versus mastectomy in our cohort. A previous publication including a subset preoperative SCAN-B patients of all clinical subtypes (2014–2019) suggested that the strongest predictors of BCS after preoperative chemotherapy are clinical stage at diagnosis and a low mammographic density [17]. Lobular histology was also identified as an independent predictor of mastectomy but not pCR after NACT previously [38, 39] and represents the most established negative-predictive factor for achieving BCS after NACT. Importantly, the choice for BCS after NACT can be influenced by other clinical factors and might affect surgical preferences, such as occurrence of extensive microcalcifications, unfavorable breast/tumor ratio, surgeon’s experience and attitude, BRCA mutation carrier status, and non-clinical factors like patient preference, regardless of OR to NACT.
The validity of pCR for predicting favorable long-term prognosis among patients with HR+/HER2- EBC [35, 40, 41] was supported by our results. Despite uniform molecular predicted high ROR scores at baseline, no patient who achieved a pCR experienced disease recurrence after a median follow-up of 5.41 years, although statistically non-significant, limited by the small numbers of patients and events included in the analysis. We noted that BCS correlated with excellent RFI probably associated with the high adjuvant radiotherapy rate (95%) in our cohort, and the enrichment for smaller tumors within the BCS group. Prognostic biomarkers for inferior RFI among patients with residual disease included tumor characteristics suggestive of non-luminal biology and endocrine non-responsiveness. Younger-age, larger tumor size, and high PAM50 ROR category class showed trends for inferior outcome. The fact that the biomarkers predictive for pCR adversely impact prognosis when treatment did not result in pCR stresses the context-dependency when utilizing biomarkers. How residual disease biology impacts prognosis remains an unsettled research question. In the study, we identify a group of ER+/HER2- tumors with an intermediate ER-expression (IHC 10–66%) with a higher likelihood of pCR following NACT, but at higher ROR in case of residual invasive cancer at surgery. In this prognostically adverse subset, characterized by an over representation of a non-luminal subtype by with gene expression profiling, there is a clinical need to evaluate the optimal post-neoadjuvant therapeutic approach.
Understanding biological heterogeneity is key to tailoring treatment. Our study is limited by the relatively small number of cases, exemplifying the limited use of NACT within this sub-population. The median follow-up for adverse events was only 5.41 years, which is not sufficiently long for HR+/HER2- BC, as late events occurring after 10 years follow-up are typically expected. Furthermore, NET and postoperative CDK4/6 inhibitors are nowadays included in the arsenal of therapies for early HR+/HER2- BC with significant improvements in prognosis. Nottingham hostologic grade (NHG) was mostly performed post-operatively (only 9% at baseline) during the treatment period; hence, it was not adjusted for in our analyses. Technical variability associated with tissue collection methods, processing, and interpretation of IHC stains is other limitations when data are collected from multiple laboratories. Nevertheless, our study uniquely describes Swedish population-based real-world outcomes of a decade of anthracycline and taxane-based NACT in HR+/HER2- EBC, a subgroup where the use of NACT is somewhat controversial. Our results are mostly consistent with independent and larger international cohorts of similarly treated patients, indicating that optimal tailoring of NACT in high-risk HR+/HER2- EBC is feasible using conventional IHC biomarkers and more precisely gene-signatures that capture non-luminal biology within clinical HR+ BCs. Future investigations are warranted in larger and prospective cohorts of patients exposed to relevant therapies and where tumor biomarkers are centrally evaluated.
Acknowledgments
The authors would like to thank all patients, clinicians, hospital staff participating in the SCAN-B study, and the staff at the central SCAN-B laboratory for their contributions toward collecting and processing biomaterials and building the SCAN-B database. We also acknowledge the Swedish National Quality Register for Breast Cancer (NKBC) for collecting clinical, tumor pathological, and outcome data.
This work was supported by the Mrs Berta Kamprad Foundation (FBKS 2022-35 and FBKS-2020-9), the Gunnar Nilsson’s Foundation (GN-2022-7-283), the Swedish Research Council (2018-00522), and Swedish governmental funding (ALF, grant to N.L.). Funding organizations did not participate in the actual research activities.
Data availability statement
RNA-sequencing-based gene-expression data, clinicopathological data, and SSP classifications for SCAN-B cohort were made publicly available and are retrievable at https://github.com/StaafLab/sspbc. However, information and mechanisms for accessing the specific subset of gene-expression and clinical data associated with the findings in this study can be obtained from the corresponding author upon reasonable request.
Ethics declarations & trial registry information
Enrollment into SCAN-B opened in September 2010 and is ongoing. Refer to clinicaltrials.gov/study/NCT02306096 and https://www.scan-b.lu.se/ for the complete inclusion and exclusion criteria. Written informed consent was collected from all patients before enrolment into SCAN-B. Inclusion of patients into SCAN-B and translational research projects based on biomaterials collected within SCAN-B is conducted in accordance to the declaration of Helsinki and approved by the Regional Ethical Review Board of Lund (registration numbers 2009/658, 2010/383, 2012/58, 2013/459 2014/521, 2015/277, 2016/944, and 2018/267), the Swedish Ethical Review Authority (registration numbers 2019-01252, 2019-01252, and 2024-02040-02), the county governmental biobank center, and the Swedish Authority for Privacy Protection (registration number 364-2010).
Author contributions
Conceptualization and design: N.L and S.K. Collection and assembly of data: H.S., N.L., and S.K. Data interpretation: all authors. Manuscript writing and review: drafted by S.K. and reviewed by all authors. Funding acquisition: N.L. and S.K. All authors have read and approved the final manuscript.
References
[1] Asselain B, Barlow W, Bartlett J, Bergh J, Bergsten-Nordström E, Bliss J, et al. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018;19(1): 27–39. https://doi.org/10.1016/S1470-2045(17)30777-5
[2] Buus R, Sestak I, Kronenwett R, Ferree S, Schnabel CA, Baehner FL, et al. Molecular drivers of oncotype DX, prosigna, endopredict, and the breast cancer index: a TransATAC study. J Clin Oncol. 2020;39(2): 126–35. https://doi.org/10.1200/JCO.20.00853
[3] Falato C, Schettini F, Pascual T, Brasó-Maristany F, Prat A. Clinical implications of the intrinsic molecular subtypes in hormone receptor-positive and HER2-negative metastatic breast cancer. Cancer Treat Rev. 2023;112:102496. https://doi.org/10.1016/j.ctrv.2022.102496
[4] Burstein HJ, Curigliano G, Thürlimann B, Weber WP, Poortmans P, Regan MM, et al. Customizing local and systemic therapies for women with early breast cancer: the St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann Oncol. 2021;32(10):1216–35. https://doi.org/10.1016/j.annonc.2021.06.023
[5] Andre F, Ismaila N, Allison KH, Barlow WE, Collyar DE, Damodaran S, et al. Biomarkers for adjuvant endocrine and chemotherapy in early-stage breast cancer: ASCO guideline update. J Clin Oncol. 2022;40(16):1816–37. https://doi.org/10.1200/JCO.22.00069
[6] Kalinsky K, Barlow William E, Gralow Julie R, Meric-Bernstam F, Albain Kathy S, Hayes Daniel F, et al. 21-gene assay to inform chemotherapy benefit in node-positive breast cancer. New Engl J Med. 2021;385(25):2336–47. https://doi.org/10.1056/NEJMoa2108873
[7] Cantini L, Trapani D, Guidi L, Boscolo Bielo L, Scafetta R, Koziej M, et al. Neoadjuvant therapy in hormone Receptor-Positive/HER2-Negative breast cancer. Cancer Treat Rev. 2024;123:102669. https://doi.org/10.1016/j.ctrv.2023.102669
[8] Kaufmann M, von Minckwitz G, Mamounas EP, Cameron D, Carey LA, Cristofanilli M, et al. Recommendations from an international consensus conference on the current status and future of neoadjuvant systemic therapy in primary breast cancer. Ann Surgical Oncol. 2012;19(5):1508–16. https://doi.org/10.1245/s10434-011-2108-2
[9] Schettini F, Martínez-Sáez O, Falato C, De Santo I, Conte B, Garcia-Fructuoso I, et al. Prognostic value of intrinsic subtypes in hormone-receptor-positive metastatic breast cancer: systematic review and meta-analysis. ESMO Open. 2023;8(3):101214. https://doi.org/10.1016/j.esmoop.2023.101214
[10] Yau C, Osdoit M, van der Noordaa M, Shad S, Wei J, de Croze D, et al. Residual cancer burden after neoadjuvant chemotherapy and long-term survival outcomes in breast cancer: a multicentre pooled analysis of 5161 patients. Lancet Oncol. 2022;23(1):149–60. https://doi.org/10.1016/S1470-2045(21)00589-1
[11] Consortium IST. Association of event-free and distant recurrence–free survival with individual-level pathologic complete response in neoadjuvant treatment of stages 2 and 3 breast cancer: three-year follow-up analysis for the I-SPY2 adaptively randomized clinical trial. JAMA Oncol. 2020;6(9):1355–62. https://doi.org/10.1001/jamaoncol.2020.2535
[12] Ma CX, Suman VJ, Sanati S, Vij K, Anurag M, Leitch AM, et al. Endocrine-sensitive disease rate in postmenopausal patients with estrogen receptor-rich/ERBB2-negative breast cancer receiving neoadjuvant anastrozole, fulvestrant, or their combination: a phase 3 randomized clinical trial. JAMA Oncol. 2024;10(3):362–71. https://doi.org/10.1001/jamaoncol.2023.6038
[13] Ellis MJ, Suman VJ, Hoog J, Lin L, Snider J, Prat A, et al. Randomized phase II neoadjuvant comparison between letrozole, anastrozole, and exemestane for postmenopausal women with estrogen receptor–rich stage 2 to 3 breast cancer: clinical and biomarker outcomes and predictive value of the baseline PAM50-based intrinsic subtype – ACOSOG Z1031. J Clin Oncol. 2011;29(17):2342–9. https://doi.org/10.1200/JCO.2010.31.6950
[14] Torrisi R, Marrazzo E, Agostinetto E, De Sanctis R, Losurdo A, Masci G, et al. Neoadjuvant chemotherapy in hormone receptor-positive/HER2-negative early breast cancer: when, why and what? Crit Rev Oncol Hematol. 2021;160:103280. https://doi.org/10.1016/j.critrevonc.2021.103280
[15] Boughey JC, McCall LM, Ballman KV, Mittendorf EA, Ahrendt GM, Wilke LG, et al. Tumor biology correlates with rates of breast-conserving surgery and pathologic complete response after neoadjuvant chemotherapy for breast cancer: findings from the ACOSOG Z1071 (Alliance) Prospective Multicenter Clinical Trial. Ann Surg. 2014;260(4):608–14; discussion 14–6. https://doi.org/10.1097/SLA.0000000000000924
[16] Spronk PER, Volders JH, van den Tol P, Smorenburg CH, Vrancken Peeters M-JTFD. Breast conserving therapy after neoadjuvant chemotherapy; data from the Dutch Breast Cancer Audit. Eur J Surg Oncol. 2019;45(2):110–7. https://doi.org/10.1016/j.ejso.2018.09.027
[17] Gulis K, Ellbrant J, Svensjö T, Skarping I, Vallon-Christersson J, Loman N, et al. A prospective cohort study identifying radiologic and tumor related factors of importance for breast conserving surgery after neoadjuvant chemotherapy. Eur J Surg Oncol. 2023;49(7):1189–95. https://doi.org/10.1016/j.ejso.2023.03.225
[18] Saal LH, Vallon-Christersson J, Hakkinen J, Hegardt C, Grabau D, Winter C, et al. The Sweden Cancerome Analysis Network – Breast (SCAN-B) Initiative: a large-scale multicenter infrastructure towards implementation of breast cancer genomic analyses in the clinical routine. Genome Med. 2015;7(1):20. https://doi.org/10.1186/s13073-015-0131-9
[19] Staaf J, Häkkinen J, Hegardt C, Saal LH, Kimbung S, Hedenfalk I, et al. RNA sequencing-based single sample predictors of molecular subtype and risk of recurrence for clinical assessment of early-stage breast cancer. NPJ Breast Cancer. 2022;8(1):94. https://doi.org/10.1038/s41523-022-00465-3
[20] Ryden L, Loman N, Larsson C, Hegardt C, Vallon-Christersson J, Malmberg M, et al. Minimizing inequality in access to precision medicine in breast cancer by real-time population-based molecular analysis in the SCAN-B initiative. Br J Surg. 2018;105(2):e158–68. https://doi.org/10.1002/bjs.10741
[21] Center RC. Swedish national quality register for breast cancer. [22 June 2025] Available from: https://cancercentrum.se/samverkan/cancerdiagnoser/brost/kvalitetsregister/
[22] Pathology SSo. KVAST document. [22 June 2025] Available from: https://svfp.se/kvast/brostpatologi/kvast-dokument/
[23] Allison KH, Hammond MEH, Dowsett M, McKernin SE, Carey LA, Fitzgibbons PL, et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP guideline update. J Clin Oncol. 2020;38(12):1346–66. https://doi.org/10.1200/JCO.19.02309
[24] Kimbung S, Veerla S, Muhammad K, Ehinger A, Vallon-Christersson J, Malmberg M, et al. Global transcriptional complexity of estrogen receptor low positive breast cancers in a prospective swedish population-based SCAN-B cohort. Clin Cancer Res. 2025;31(13):2695-2709. https://doi.org/10.1158/1078-0432.c.7903433
[25] Huppert LA, Wolf D, Yau C, Brown-Swigart L, Hirst GL, Isaacs C, et al. Pathologic complete response (pCR) rates for patients with HR+/HER2− high-risk, early-stage breast cancer (EBC) by clinical and molecular features in the phase II I-SPY2 clinical trial. Ann Oncol. 2025;36(2):172–84. https://doi.org/10.1016/j.annonc.2024.10.018
[26] Johnston SRD, Harbeck N, Hegg R, Toi M, Martin M, Shao ZM, et al. Abemaciclib combined with endocrine therapy for the adjuvant treatment of HR+, HER2-, node-positive, high-risk, early breast cancer (monarchE). J Clin Oncol. 2020 Dec 1;38(34):3987–3998. https://doi.org/10.1200/JCO.20.02514
[27] Tolaney SM, Garrett-Mayer E, White J, Blinder VS, Foster JC, Amiri-Kordestani L, et al. Updated Standardized Definitions for Efficacy End Points (STEEP) in adjuvant breast cancer clinical trials: STEEP Version 2.0. J Clin Oncol. 2021;39(24):2720–31. https://doi.org/10.1200/JCO.20.03613
[28] Pagani O, Walley BA, Fleming GF, Colleoni M, Láng I, Gomez HL, et al. Adjuvant exemestane with ovarian suppression in premenopausal breast cancer: long-term follow-up of the combined TEXT and SOFT trials. J Clin Oncol. 2022;41(7):1376–82. https://doi.org/10.1200/JCO.22.01064
[29] Brown LC, Luen SJ, Molania R, Caramia F, Savas P, VanGeelen C, et al. Evaluation of PAM50 intrinsic subtypes and risk of recurrence (ROR) scores in premenopausal women with early-stage HR+ breast cancer: a secondary analysis of the SOFT trial. J Clin Oncol. 2023;41(16_suppl):504.
[30] Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47. https://doi.org/10.1016/j.ejca.2008.10.026
[31] Lips EH, Mulder L, de Ronde JJ, Mandjes IAM, Vincent A, Vrancken Peeters MTFD, et al. Neoadjuvant chemotherapy in ER+ HER2− breast cancer: response prediction based on immunohistochemical and molecular characteristics. Breast Cancer Res Treat. 2012;131(3):827–36.
[32] Raphael J, Kiss A, Nofech-Mozes S, Trudeau M. Clinical outcomes of single versus double hormone receptor-positive breast cancer patients treated with neoadjuvant chemotherapy. Clin Breast Cancer. 2018;18(6):e1381–7.
[33] van Mackelenbergh MT, Denkert C, Nekljudova V, Karn T, Schem C, Marmé F, et al. Outcome after neoadjuvant chemotherapy in estrogen receptor-positive and progesterone receptor-negative breast cancer patients: a pooled analysis of individual patient data from ten prospectively randomized controlled neoadjuvant trials. Breast Cancer Res Treat. 2018;167(1):59–71.
[34] Whitworth P, Beitsch P, Mislowsky A, Pellicane JV, Nash C, Murray M, et al. Chemosensitivity and endocrine sensitivity in clinical luminal breast cancer patients in the prospective Neoadjuvant Breast Registry Symphony Trial (NBRST) predicted by molecular subtyping. Ann Surg Oncol. 2017;24(3):669–75. https://doi.org/10.1245/s10434-016-5600-x
[35] Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–72.
[36] Ohara AM, Naoi Y, Shimazu K, Kagara N, Shimoda M, Tanei T, et al. PAM50 for prediction of response to neoadjuvant chemotherapy for ER-positive breast cancer. Breast Cancer Res Treat. 2019;173(3): 533–43. https://doi.org/10.1007/s10549-018-5020-7
[37] Braybrooke J, Bradley R, Gray R, Hills RK, Pan H, Peto R, et al. Anthracycline-containing and taxane-containing chemotherapy for early-stage operable breast cancer: a patient-level meta-analysis of 100 000 women from 86 randomised trials. Lancet. 2023;401(10384):1277–92. https://doi.org/10.1016/S0140-6736(23)00285-4
[38] Delpech Y, Coutant C, Hsu L, Barranger E, Iwamoto T, Barcenas CH, et al. Clinical benefit from neoadjuvant chemotherapy in oestrogen receptor-positive invasive ductal and lobular carcinomas. Br J Cancer. 2013;108(2):285–91. https://doi.org/10.1038/bjc.2012.557
[39] Loibl S, Volz C, Mau C, Blohmer J-U, Costa SD, Eidtmann H, et al. Response and prognosis after neoadjuvant chemotherapy in 1,051 patients with infiltrating lobular breast carcinoma. Breast Cancer Res Treat. 2014;144(1):153–62. https://doi.org/10.1007/s10549-014-2861-6
[40] Bonnefoi H, Litière S, Piccart M, MacGrogan G, Fumoleau P, Brain E, et al. Pathological complete response after neoadjuvant chemotherapy is an independent predictive factor irrespective of simplified breast cancer intrinsic subtypes: a landmark and two-step approach analyses from the EORTC 10994/BIG 1-00 phase III trial. Ann Oncol. 2014;25(6):1128–36. https://doi.org/10.1093/annonc/mdu118
[41] Haque W, Verma V, Hatch S, Suzanne Klimberg V, Brian Butler E, Teh BS. Response rates and pathologic complete response by breast cancer molecular subtype following neoadjuvant chemotherapy. Breast Cancer Res Treat. 2018;170(3):559–67. https://doi.org/10.1007/s10549-018-4801-3