LETTER TO THE EDITOR
Multidisciplinary team meetings for lung cancer in the Nordic countries: results from a Nordic survey
Anja Gouliaeva,b  , Janna Bergc , Johan Isakssond , Heidi Anderséne,f,g and Torben Riis Rasmussena,b
, Janna Bergc , Johan Isakssond , Heidi Anderséne,f,g and Torben Riis Rasmussena,b
aDepartment of Respiratory Diseases and Allergy, Aarhus University Hospital, Aarhus N, Denmark; bDepartment of Clinical Medicine, Aarhus University, Aarhus N, Denmark; cDepartment of Pulmonology, Vestfold Hospital Trust, Tønsberg, Norway; dCentre for Research and Development, Region Gävleborg, Uppsala University, Uppsala, Sweden; eCancer Center, Vaasa Central Hospital, Vaasa, Finland; fDepartment of Clinical Oncology, University of Turku, Turku, Finland; gFaculty of Medicine and Health Technology, Tampere University, Tampere, Finland
KEYWORDS: Lung cancer; Scandinavian and Nordic countries; multidisciplinary team conference; tumor board; healthcare survey
Citation: ACTA ONCOLOGICA 2026, VOL. 65, 301–305. https://doi.org/10.2340/ao.v65.45213.
Copyright: © 2026 The Author(s). Published by MJS Publishing on behalf of Acta Oncologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Received: 5 January 2026; Accepted: 1 April 2026; Published: 17 April 2026
CONTACT Anja Gouliaev a.gouliaev@rm.dk Department of Respiratory Diseases and Allergy, Aarhus University Hospital, 99 Palle Juul-Jensens Boulevard, 8200 Aarhus N, Denmark
Supplemental data for this article can be accessed online at https://doi.org/10.2340/ao.v65.45213
Competing interests and funding: The project was funded by AstraZeneca. The authors report that there are no competing interests to declare.
Introduction
The management of lung cancer is complex and requires coordinated input from multiple specialties. Multidisciplinary team (MDT) meetings provide a structured forum in which respiratory physicians, oncologists, thoracic surgeons, radiologists, pathologists, and specialist nurses review diagnostic findings and formulate treatment strategies [1–3]. MDT-based care has been associated with improved staging accuracy and guideline adherence in lung cancer [4–6]. Effective MDT decision-making relies on access to relevant information, structured case presentations, clear leadership, and an infrastructure that supports balanced participation among team members. While MDT meetings are widely implemented across Europe, there is no international consensus defining how they should be organized, which patients should be discussed, or how meeting processes should be structured. The Nordic countries share publicly financed healthcare systems with universal access and established lung cancer registries, yet operational organization of MDT meetings may vary across settings [7].
We therefore conducted a cross-national survey to describe and compare lung cancer MDT meetings in Denmark, Finland, Norway, and Sweden, with particular focus on governance, meeting frequency, patient selection, and perceived barriers and drivers. Identifying structural similarities and differences may inform future operational guidance at national or Nordic level.
Patients/material and methods
After the turn of the century, MDT meetings have been implemented in all four Nordic countries. A lung cancer MDT meeting was defined as a formal multidisciplinary forum in which diagnostic and treatment decisions for lung cancer patients are discussed.
This was a non-interventional cross-sectional survey conducted between June and September 2025.
A senior respiratory physician functioning as a leader of lung cancer MDT meetings from each of the four participating countries, were invited to participate in the development of the survey questions and to distribute the survey nationally. All lung cancer MDT meetings in Denmark (n = 7), regional MDT meetings in Norway (n = 7), and treating hospitals in Finland (n = 20) and Sweden (n = 21) were invited to participate. In Norway, only regional MDT meetings were included to ensure comparable case complexity and access to thoracic surgery. One reminder was sent after 2 weeks.
Survey instrument
The questionnaire comprised 53 items addressing:
- - MDT composition and leadership
- - Governance and guideline support
- - Meeting frequency and duration
- - Case volume and patient selection
- - Infrastructure and remote participation
- - Biomarker testing
- - Perceived barriers and drivers
Full questionnaire details are provided in Supplementary Material.
Statistical approach
Quantitative responses were summarized using descriptive statistics.
Results
Response rate and MDT characteristics
Thirty of the 55 (55%) invited centers responded: Denmark 7/7 (100%), Finland 6/20 (30%), Norway 6/7 regional MDTs (86%), and Sweden 11/21 (52%).
Respiratory physicians chaired 90% of MDT meetings. Ninety-three percent reported local or national MDT guidelines. Sixty percent used structured templates for case presentation, and 62% reported access to second-opinion MDT meetings (Table 1).
Meeting frequency and workload
Meeting frequency ranged from weekly to multiple times per week (Table 1). Danish centers reported multiple weekly meetings, whereas most Finnish and Norwegian centers met weekly. The number of cases per meeting ranged from 1 to more than 25. Meeting duration ranged from 30 min to more than 2 h with average case numbers between one to 25 patient cases. Most centers use a standard template for case presentation and some have the option to refer for a second opinion MDT. Most respondents reported that both the number of cases discussed and total time spent in MDT meetings had increased over the past 3–5 years. Remote or hybrid participation was reported in all countries but varied considerably between centers.
Patient selection
Patient information required to be assessed at lung cancer MDT meeting is shown in Figure 1A. Variation in patient selection was observed (Figure 1B). All Danish centers and most Swedish centers reported discussing lung cancer patients across all disease stages. In contrast, several Finnish and Norwegian centers reported more selective discussion, particularly focusing on patients eligible for surgery or curative treatment.
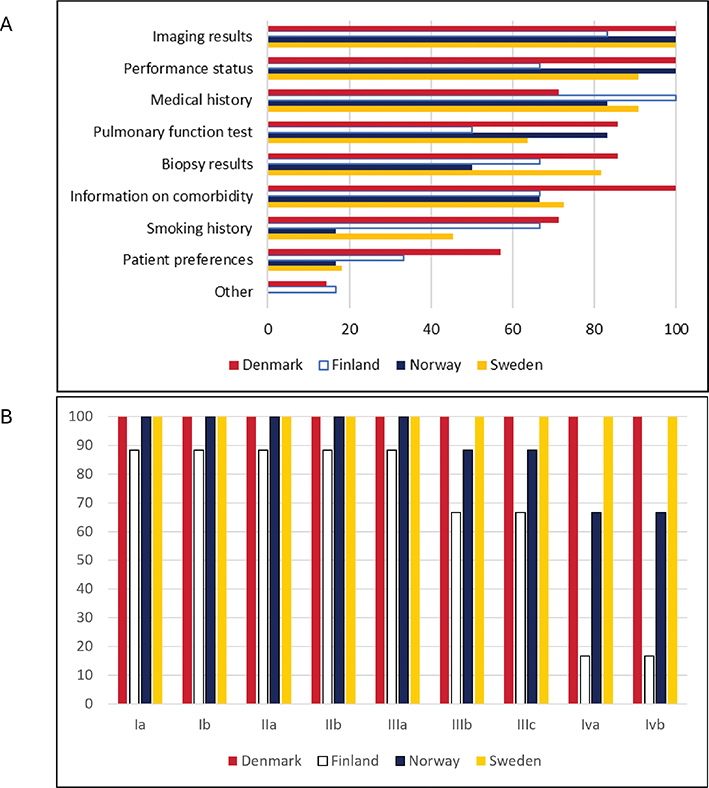
Figure 1. (A) Information required for the case to be presented at the lung cancer MDT in percent, by country (30 answers) (B) Stages of NSCLC included in discussions at MDT in percent, by country (30 answers).
The proportion of patients not discussed at MDT meetings ranged from < 10% to up to 69% across centers.
Perceived barriers and drivers
The most frequently reported driver for MDT meetings was the need for multidisciplinary input (96%), followed by case complexity (79%) and national guideline requirements (75%). Insufficient available time was identified as a barrier by 54% of respondents across all countries. Additional barriers included IT limitations (17%) and incomplete team participation (17%). Most lung cancer MDT centers have national or local guidelines, which to some extent support the MDTs’ role in decision-making (Table 1).
Discussion and conclusion
This study provides a contemporary overview of lung cancer MDT meetings in four Nordic countries. Despite broadly similar healthcare systems and guideline frameworks, we identified considerable variation in meeting frequency, case volume, and patient selection. Professional composition and leadership were largely consistent, with respiratory physicians chairing most meetings. The widespread presence of local or national guidelines suggests institutionalized MDT practice.
Meeting frequency and case volume varied substantially. Danish centers reported more frequent meetings and higher case numbers, whereas other countries more often conducted weekly meetings. Prior research suggests that effective MDT performance depends on regular meetings, manageable caseloads, and structured presentation formats [1–3, 8]. The relatively low number of cases discussed per MDT meeting in the Nordic countries aligns with previous studies on lung cancer MDTs [7] and MDTs for other cancers [8] in a Nordic setting. In contrast, MDTs in the United Kingdom often review more than 20 patients per meeting [9, 10], a volume associated with decision making fatigue [11]. Given that most Nordic lung cancer MDTs discuss fewer than 20 cases, this is unlikely to be a concern.
Prolonged diagnostic interval, exceeding 2 months in one Finnish center, highlights a challenge in delayed treatment. Another challenge in Finland is the limited access to computed tomography scans at primary care centers, which are often the first point of contact for patients who exhibit symptoms [12].
Variation in patient selection was notable. While some centers discussed all disease stages, others focused on potentially curative cases. Stage III non-small cell lung cancer (NSCLC), representing locally advanced disease, frequently presents diagnostic and therapeutic challenges [13–15]. Treatment intent for stage III NSCLC patients can be either curative or palliative depending on minor differences. In two Finnish and one regional Norwegian lung cancer centers, stage IIIB and IIIC patients were not routinely presented at MDT meetings. Registry data show that 91% of all Danish lung cancer patients and 93% of curatively treated lung cancer patients in Norway were discussed at local and regional MDT meeting in 2024 [16, 17] and 83% of all Swedish lung cancer patients in 2023 [18]. Finland lacks comparable national registry data [19]. By comparison, the United Kingdom has shifted toward more selective MDT discussion to streamline workflow [20, 21]. Whether all lung cancer patients should be routinely discussed remains debated. Selective discussion may improve efficiency but risk variation in care pathways. Clearer operational guidance may help to balance comprehensiveness and feasibility.
Although several benefits of MDT-based lung cancer care were highlighted, our findings also suggest barriers to optimal MDT function in the Nordic countries. National or local guidelines typically define roles, responsibilities, and eligibility, but often lack operational structure such as meeting workflow, documentation standards, or leadership responsibilities. In some centers, MDT structures were established before national guidelines, limiting the impact of later recommendations. To improve lung cancer MDTs in the Nordic countries, we propose developing national or Nordic-level operational guidelines and implementing routine MDT audits.
Strengths and limitations
To our knowledge, this is the first cross-national survey describing lung cancer MDT meetings across the Nordic countries. However, uneven response rates and differences in inclusion criteria, such as inclusion of only regional MDT meetings in Norway, limit cross-country comparability. The Finnish response rate was low. Data were self-reported and not validated against registry data or direct observation. Furthermore, we did not assess clinical outcomes, consensus rates, or documentation of staging decisions.
Conclusion
Nordic lung cancer MDT meetings share a similar multidisciplinary composition, but differ in meeting frequency, workload, and patient selection. Increasing demands and variation in operational structure highlight the need for clearer organizational guidelines to support sustainable and consistent MDT-based lung cancer care.
Acknowledgments
The authors would like to thank all respondents of the Nordic surveys.
Data availability statement
Data are available on request from the corresponding author.
Ethics declarations & trial registry information
Participants were informed of the study objectives and data handling. No personal or patient-identifiable information was collected; therefore, ethical approval and informed consent were not required.
Authors’ contributions
AG: conceptualization, data curation, formal analysis, methodology, writing original draft, writing reviewing and editing. JB, JI, HA: conceptualization, writing reviewing and editing. TRR: conceptualization, methodology, writing reviewing and editing. All authors reviewed, edited and approved the final manuscript.
References
[1] Rankin NM, Fradgley EA, Barnes DJ. Implementation of lung cancer multidisciplinary teams: a review of evidence-practice gaps. Transl Lung Cancer Res. 2020;9:1667–79. https://doi.org/10.21037/tlcr.2019.11.32
[2] Lamb BW, Sevdalis N, Benn J, Vincent C, Green JSA. Multidisciplinary cancer team meeting structure and treatment decisions: a prospective correlational study. Ann Surg Oncol. 2013;20:715–22. https://doi.org/10.1245/s10434-012-2691-x
[3] Soukup T, Lamb BW, Arora S, Darzi A, Sevdalis N, Green JSA. Successful strategies in implementing a multidisciplinary team working in the care of patients with cancer: an overview and synthesis of the available literature. J Multidiscip Healthc. 2018;11:49–61. https://doi.org/10.2147/JMDH.S117945
[4] Fehervari M, Hamrang-Yousefi S, Fadel MG, Mills SC, Warren OJ, Tekkis PP, et al. A systematic review of colorectal multidisciplinary team meetings: an international comparison. BJS Open. 2021;5(3):zrab044. https://doi.org/10.1093/bjsopen/zrab044
[5] Forrest LM, McMillan DC, McArdle CS, Dunlop DJ. An evaluation of the impact of a multidisciplinary team, in a single centre, on treatment and survival in patients with inoperable non-small-cell lung cancer. Br J Cancer. 2005;93(9):977–8. https://doi.org/10.1038/sj.bjc.6602825
[6] Heinke MY, Vinod SK. The impact of lung cancer multidisciplinary care on patient outcomes. Transl Lung Cancer Res. 2020;9(4): 1639–53. https://doi.org/10.21037/tlcr.2019.11.03
[7] Gouliaev A, Berg J, Bibi R, Arshad A, Leira HO, Neumann K, et al. Multi-disciplinary team meetings for lung cancer in Norway and Denmark: results from national surveys and observations with MDT-MODe. Acta Oncol (Madr). 2024;63:678–84. https://doi.org/10.2340/1651-226X.2024.40777
[8] Wihl J, Rosell L, Frederiksen K, Kinhult S, Lindell G, Nilbert M. Contributions to multidisciplinary team meetings in cancer care: predictors of complete case information and comprehensive case discussions. J Multidiscip Healthc. 2021;14:2445–52. https://doi.org/10.2147/JMDH.S309162
[9] Soukup T, Lamb BW, Morbi A, Shah NJ, Bali A, Asher V, et al. A multicentre cross-sectional observational study of cancer multidisciplinary teams: analysis of team decision making. Cancer Med. 2020;9(19):7083–99. https://doi.org/10.1002/cam4.3366
[10] Lamb BW, Wong HWL, Vincent C, Green JSA, Sevdalis N. Teamwork and team performance in multidisciplinary cancer teams: development and evaluation of an observational assessment tool. BMJ Qual Saf. 2011;20(10):849–56. https://doi.org/10.1136/bmjqs.2010.048660
[11] Soukup T, Gandamihardja TAK, McInerney S, Green JSA, Sevdalis N. Do multidisciplinary cancer care teams suffer decision-making fatigue: an observational, longitudinal team improvement study. BMJ Open. 2019;9(5):e027303. https://doi.org/10.1136/bmjopen-2018-027303
[12] Andersén H, Aro M, Kaarteenaho R, Koivunen J, Mäyränpää MI, Sihvo E, et al. Lung cancer in Finland. J Thorac Oncol. 2024;19(9):1265–71. https://doi.org/10.1016/j.jtho.2024.06.005
[13] Tanner NT, Gomez M, Rainwater C, Nietert PJ, Simon GR, Green MR, et al. Physician preferences for management of patients with stage IIIA NSCLC impact of bulk of nodal disease on therapy selection. J Thorac Oncol. 2012;7(2):365–9. https://doi.org/10.1097/JTO.0b013e31823a385f
[14] Hoeijmakers F, Heineman DJ, Daniels JM, Beck N, Tollenaar RAEM, Wouters MWJM, et al. Variation between multidisciplinary tumor boards in clinical staging and treatment recommendations for patients with locally advanced non-small cell lung cancer. Chest. 2020;158:2675–87. https://doi.org/10.1016/j.chest.2020.07.054
[15] Rasmussen TR, Gouliaev A, Jakobsen E, Hjorthaug K, Larsen LU, Meldgaard P, et al. Impact of multidisciplinary team discrepancies on comparative lung cancer outcome analyses and treatment equality. BMC Cancer. 2024;24(1):1423. https://doi.org/10.1186/s12885-024-13188-4
[16] The Danish Lung Cancer Registry. 2024 [cited 2025 Nov 21]. Available from: https://www.lungecancer.dk/wp-content/uploads/2025/08/DLCR-%C3%85rsrapport-2024_rev-07.08.24.pdf
[17] The Norwegian National Quality Registry of Lung Cancer (Nasjonalt Kvalitetsregister for Lungekreft) annual report. 2024 [cited 2025 Nov 21]. Available from: https://www.fhi.no/publ/2025/nasjonalt-kvalitetsregister-for-lungekreft-2024/
[18] The Swedish National Lung Cancer Register. 2023 [cited 2025 Nov 21]. Available from: https://www.lungecancer.dk/wp-content/uploads/2025/08/DLCR-%C3%85rsrapport-2024_rev-07.08.24.pdf
[19] Gouliaev A, Rasmussen TR, Malila N, Fjellbirkeland L, Löfling EL, Jakobsen E, et al. Lung cancer registries in Denmark, Finland, Norway and Sweden: a comparison and proposal for harmonization. Acta Oncol. 2023;62(1):1–7. https://doi.org/10.1080/0284186X.2023.2172687
[20] Al-Hammouri T, Almeida-Magana R, Soukup T, Lamb B. Implementation of streamlining measures in selecting and prioritising complex cases for the cancer multidisciplinary team meeting: a mini review of the recent developments. Front Health Serv. 2024;4:1340320. https://doi.org/10.3389/frhs.2024.1340320
[21] Winters DA, Soukup T, Sevdalis N, Green JSA, Lamb BW. The cancer multidisciplinary team meeting: in need of change? History, challenges and future perspectives. BJU Int. 2021;28:271–9. https://doi.org/10.1111/bju.15495