ORIGINAL ARTICLE
DEVELOPMENT OF EXPERT CONSENSUS TO GUIDE PHYSICAL REHABILITATION IN CHILDREN AND ADOLESCENTS WITH ACQUIRED BRAIN INJURY DURING THE SUBACUTE PHASE
Christiaan GMELIG MEYLING, MSc1–3, Olaf VERSCHUREN, PhD1, Ingrid C. M. RENTINCK, PhD2, F. Virginia WRIGHT, PhD4,5, Jan WILLEM GORTER, MD, PhD1,6,7 and Raoul H. ENGELBERT, PhD8–10; on Behalf of the Pediatric Acquired Brain Injury (Abi) Collaborative
From the 1UMC Utrecht Brain Center and Center of Excellence for Rehabilitation Medicine, Utrecht University, 2De Hoogstraat Rehabilitation, Department of Pediatric Rehabilitation,Utrecht, 3HU University of Applied Sciences Utrecht, Institute of Human Movement Studies, Master Pediatric Physiotherapy, Utrecht, The Netherlands, 4Bloorview Research Institute, Toronto, 5Department of Physical Therapy, University of Toronto, Toronto, Ontario, Canada, 6Department of Rehabilitation, Physical Therapy Science and Sports, UMC Utrecht Brain Center, University Medical Center Utrecht, Utrecht, The Netherlands, 7CanChild Centre for Childhood Disability Research, Department of Pediatrics, McMaster University, Hamilton, Ontario, Canada, 8Amsterdam UMC, University of Amsterdam, Department of Rehabilitation, Amsterdam Movement Sciences, 9Centre of Expertise Urban Vitality, Faculty of Health, Amsterdam University of Applied Sciences and 10Amsterdam UMC, University of Amsterdam, Department of Pediatrics, Emma Children’s Hospital, Amsterdam, The Netherlands
Objective: To develop consensus among experts to guide physical rehabilitation in children and adolescents with acquired brain injury during the subacute phase.
Design: International Delphi study.
Methods: A 3-round online Delphi study was conducted with 11 international experts in rehabilitation for children and adolescents with acquired brain injury. The first round consisted of open-ended questions; the second and third round consisted of ranking 139 statements on a 5-point Likert scale.
Results: The panel reached consensus on 116/139 statements. Consensus was reached on the importance of age, pre-injury developmental stage and the clinical presentation of the child when determining content and focus of physical rehabilitation. In addition, consensus was reached on the importance of participation-focused interventions, and involvement of family members in goal-setting and therapeutic activities. Although dosage was deemed very important, no consensus was reached for determination of dose-response variables to suit and influence the child’s needs.
Conclusion: This study provides a framework for clinicians to design physical rehabilitation interventions in children with acquired brain injury in the sub-acute recovery phase. The promotion of physical activity in meaningful contexts and involvement of family members are considered as important components to optimize recovery.
LAY ABSTRACT
Children and adolescents with acquired brain injury are often admitted to rehabilitation services, which have great potential to improve their recovery. However, based on available research, it is unclear how an optimal rehabilitation programme should be created and offered. Therefore 139 statements were developed with an international expert-panel about physical rehabilitation in children with acquired brain injury, of which 116 statements reached consensus. The panel agreed on the importance of an early start of meaningful physical activities and the involvement of family members. Physical activity is seen as an important factor in recovery and the amount (frequency, intensity, time) of practice is suggested to have potential impact on the recovery of children with acquired brain injury. In addition, emphasis is given to the importance of an individualized approach. This research provides a framework for clinicians to design optimal physical rehabilitation interventions in children with acquired brain injury in the sub-acute recovery phase.
Key words: acquired brain injury; children and adolescents; Delphi study; occupational therapy; physical activity; physiotherapy; rehabilitation; traumatic brain injury.
Citation: J Rehabil Med 2023; 55: jrm12303. DOI: https://doi.org/10.2340/jrm.v55.12303
Copyright: © Published by Medical Journals Sweden, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Jul 5, 2023; Published: Aug 16, 2023
Correspondence address: Christiaan Gmelig Meyling, De Hoogstraat Rehabilitation, Rembrandtkade 10, NL-3583 TM Utrecht, The Netherlands. Email: c.g.meyling@dehoogstraat.nl
Competing interests and funding: Dr Stacy Suskauer reports her position on the scientific advisory board for Myomo, an upper extremity orthotics company. She has received stock options as part of this role. The other authors have stated that they had no interests that might be perceived as posing conflict or bias.
Christiaan Gmelig Meyling received a research stipend from De Hoogstraat Rehabilitation Scientific Research Fund.
Acquired brain injury (ABI) in children and adolescents is associated with acute and detrimental effects on physical, cognitive, social and emotional functioning (1, 2). To optimize recovery and the level of functioning and participation, children and adolescents with moderate to severe ABI are often admitted to multidisciplinary rehabilitation programmes in the subacute phase (1). Emphasis is initially given to physical rehabilitation, since deleterious changes in mobility post-injury are often most apparent and amenable to change during this subacute rehabilitation phase. In the absence of a generally accepted definition, we operationalize the subacute rehabilitation phase as “the period directly after the acute treatment phase in the hospital, when a child or adolescent is medically stable and admitted to an inpatient or outpatient rehabilitation programme”. The design of physical rehabilitation programmes for children and adolescents are often grounded in the framework of the International Classification of Functioning, Disability and Health: Children and Youth (ICF-CY) (3).
Physical rehabilitation interventions after ABI have great potential to improve recovery through experience-dependent neural plasticity and the development of compensatory strategies (4). Neural plasticity is believed to be the basis for relearning by the damaged brain. It occurs through physical rehabilitation in which the characteristics of physical intervention, including dosage (frequency, intensity, time and type), are essential (4, 5). In adults, systematic reviews have explored whether increased intensity of physical rehabilitation interventions improves the level of functioning and participation after stroke or traumatic brain injury (TBI) (6, 7). The available evidence indicates that more intensive rehabilitation in the adult population in the subacute phase is helpful to optimize recovery (8). However, evidence of the impact of physical rehabilitation overall and treatment intensity in particular is lacking in paediatric ABI. A recent scoping review (9) highlighted limited evidence as to the characteristics and effects of physical rehabilitation interventions in children and adolescents during the subacute rehabilitation phase. Due to the limited number of studies (n = 9) and their use of small and heterogeneous sample sizes (8/9 studies n ≤ 12), it remains unclear which children could benefit the most from subacute physical rehabilitation. In addition, large variation existed in the intervention characteristics in frequency (1–7 days per week), time (26–360 min per day) and type of exercise provided. The potential of intensive physical rehabilitation to improve functional physical recovery has been described in the literature with emphasis on developing an understanding of the factors needed for complex physical rehabilitation interventions (10). To understand the extent of the impact of physical rehabilitation interventions on recovery after ABI, it is important to find ways to gain insights into optimal intervention characteristics and their implementation in rehabilitation practice in children and adolescents with ABI.
In the absence of practical guidelines and high-quality studies, Delphi consensus statements can be created to unite researchers and clinicians in their ideas (11). Consensus recommendations achieved in a Delphi process can facilitate the development and implementation of evidence-based intervention programmes. Therefore, the aim of this study was to develop a set of consensus statements including recommendations on physical rehabilitation interventions in children and adolescents with ABI during the subacute phase. In alignment with the knowledge gaps identified in current literature (9), the following research questions were addressed:
- Which patient-related factors should we consider when designing intensive physical rehabilitation interventions for children and adolescents with ABI during the subacute phase?
- Which factors contribute to an optimal physical rehabilitation intervention programme during this phase?
METHODS
To ensure that the Delphi consensus process was adequately performed, all stages of the research were supervised by a 5-member independent steering group, consisting of experts in the field of paediatric physiotherapy (OV and RE), neuropsychology (IR) and paediatric rehabilitation medicine (JWG) who guided the principal investigator (CGM). An external researcher (FVW) with expertise in research methodology was involved to reflect on the structure of the Delphi surveys. Recommendations for the Conducting and Reporting of Delphi Studies (CREDES) were used to improve transparency of all aspects of this research (12).
Panel recruitment
As physical rehabilitation in ABI during the subacute recovery phase is mainly part of a multidisciplinary team effort, a broad range of experts was sought to ensure a multidisciplinary perspective during the Delphi rounds. To ensure diversity in clinical or research background and in international representation, experts were nominated using the authors’ names of published literature on the topic of rehabilitation in children with ABI and using a list of active participants in a relevant international network (International Pediatric Brain Injury Society). Given the small number of identified experts (n = 27), no exclusion criteria were applied for panel experts. The steering group invited all experts by email. Through a “snowball method” (13), all identified experts were asked to nominate other (clinical and/or scientific) experts for participation in this Delphi study, who all were then invited (n = 8) by the steering group to participate. The study aimed to include as many experts as possible, with a minimum target of 10, according to the recommendations in the literature (14). All experts were asked to commit to completing the 3 Delphi rounds. All participating experts were considered as members of the research group as an international collaborative. The anonymity and independence of all experts were assured throughout all Delphi rounds with sharing of names only after the entire Delphi process was completed.
Delphi methodology
Based on literature recommendations, the use of 3 online Delphi rounds was determined prior to the start (11, 15). In the first round, the experts shared their ideas and experiences related to subacute rehabilitation in paediatric ABI through a series of open-ended questions (Appendix SI), which were deliberately kept broad to ensure that all relevant information was collected (Fig. 1). Questions for round 1 were generated by the steering group based on the knowledge gaps that were identified in a scoping review (9) concerning the patient population and intervention characteristics. Due to the large number of questions, this first round was divided into 2 sub-rounds. Round 1a focused on establishing the definition of the ABI-population in the subacute phase and the influence of patient-related characteristics on physical rehabilitation interventions. Round 1b focused on the definition and theoretical framework of understanding physical rehabilitation and translation towards clinical practice. A fictitious case was provided in round 1b to facilitate the expert’s individual thinking process about the factors that could be related to the content and theoretical understanding of physical rehabilitation interventions in children and adolescents with ABI (Appendix SII). Conventional and summative content analysis (16) of the results of rounds 1a and 1b and plenary in-person discussions within the steering group resulted in the formation of 139 statements.

Fig. 1. Delphi consensus process.
In round 2, experts ranked each of the 139 statement using a 5-point Likert scale. This was applied as follows: 1 = not important, 2 = slightly important, 3 = moderately important, 4 = important, 5 = very important. The option “0= unable to score” was provided in case the topic or statement fell outside the expert’s scope of expertise. Experts had the opportunity to add comments to all statements. Two additional open questions were added to obtain more detailed information about the minimal cognitive requirements for active participation in physical rehabilitation interventions and the determination of dose-response variables in clinical practice.
In round 3, all experts received feedback consisting of their personal scores and the group scores (median and interquartile range (IQR)) for the statements that did not reach consensus in round 2. Experts were asked to re-consider their score and provide a final score with rationale for their decision. Finally, the entire set of 139 statements was sorted into categories by the first author using qualitative (inductive) content analysis approach and discussed and agreed upon by the steering committee (16, 17). This resulted in a deductive categorization according to ICF-CY (3), respectively health condition, body functions and structures, activity and participation, and contextual factors (personal and environmental) as well as into an additional category created by the steering committee on rehabilitation setting and content. A meeting with the steering committee was used to identify overarching key topics to aid in the translation of the results into the daily context of clinicians.
Statistical analysis and consensus
The median Likert score and IQR were calculated for each of the 139 statements rated in rounds 2 and 3 (18). The score “0 = unable to score” was not included in the analysis. Consensus was defined a priori as a median Likert-score ≥ 4 and IQR ≤ 1 (18). The answers to the open questions in round 2 and the comments related to the statements in rounds 2 and 3 were used to identify relevant themes.
RESULTS
Of the 35 invited experts, 11 agreed to participate in the Delphi panel, and of these 2 individuals were supported in their responses by their multidisciplinary teams (see characteristics of panellist Table I) (Fig. 2). These 2 participants reported that their mutual discussions with their teams led to in-depth discussions resulting in well-considered responses during the Delphi rounds. The demographic characteristics of the experts who were asked to participate but eventually did not accept the invitation were comparable with the participating panel (Table II). The response rates were 100% for round 1a, 91% for round 1b, 91% for round 2, and 100% for round 3. After round 2, consensus was reached on 73/139 statements (53%). After experts’ re-ranking of the remaining 66 statements in the third round, 43 (65%) additional statements reached consensus. Thus, overall, consensus was reached on 116/139 statements (83%). An overview of the statements and detailed ranking results is provided in Table III. The most important results are summarized below according to these categories.
| Number | Statement | Round 2 Median (IQR) | Round 3 Median (IQR) | Consensus |
| Health Condition (injury-related factors) | ||||
| 1 | Physical rehabilitation interventions need to be able to cope with rapidly changing clinical features that are common in children and young people with ABI | 5 (1) | ✔* | |
| 2 | Prognosis for recovery of function affects therapists’ decisions regarding type and dosage of physical rehabilitation interventions | 3.5 (1.25) | 4 (1) | ✔ |
| 3 | Nutritional status needs always to be monitored for its impact on effectiveness of physical rehabilitation | 4 (2) | 4 (1) | ✔ |
| Importance of variables related to injury related factors when determining the content and focus of physical rehabilitation interventions during subacute phase: | ||||
| 4 | - Stage of recovery | 4.5 (1) | ✔ | |
| 5 | - Severity of injury | 4 (1.25) | 4 (0) | ✔ |
| 6 | - Comorbidities | 4 (1.25) | 4 (0) | ✔ |
| 7 | - Time since injury | 3.5 (1.5) | 4 (1) | ✔ |
| 8 | - Etiology of injury | 3 (2) | 3 (1) | ×* |
| 9 | - Location of injury | 3.5 (2.25) | 3.5 (1) | × |
| Body Functions | ||||
| 10 | Level of consciousness determines to what extent the patient is indicated for active and intensive physical rehabilitation intervention | 5 (1) | ✔ | |
| 11 | Fatigue determines the dosage of physical rehabilitation interventions | 5 (1) | ✔ | |
| 12 | Fatigue determines the amount of environmental stimulation in the early phase of rehabilitation | 4.5 (1) | ✔ | |
| 13 | Medical and pharmacological management (e.g. pain, sleep, tone, attention) should be part of clinical decision making for the content of physical rehabilitation interventions | 4.5 (1) | ✔ | |
| 14 | Quality of sleep (including sleep hygiene) should be part of a physical rehabilitation program | 4.5 (1) | ✔ | |
| 15 | Impairments of cognitive functions (b1) determine motor learning strategies during physical rehabilitation intervention | 4.5 (1.25) | 4 (1) | ✔ |
| 16 | Attention deficits determine the amount of environmental stimulation in the early phase of rehabilitation | 4 (1.25) | 4 (0.5) | ✔ |
| 17 | Stimulus sensitivity determines the dosage of physical rehabilitation interventions | 3.5 (1.5) | 4 (1) | ✔ |
| Importance of variables related to body functions when determining the content and focus of physical rehabilitation interventions during the subacute phase: | ✔ | |||
| 18 | - Mental functions (e.g. cognitive, behavioral and emotional functions) (b1) | 5 (1) | ✔ | |
| 19 | - Pain management | 5 (1) | ✔ | |
| 20 | - Adequate sleep | 4 (1) | ✔ | |
| 21 | - Sensory functions (e.g. sensory loss, pain) (b2) | 4 (1) | ✔ | |
| 22 | - Neuromusculoskeletal and movement-related functions (e.g. range of motion, muscle power, muscle tone, motor control) (b7) | 5 (2) | 5 (1) | ✔ |
| 23 | - Cardiovascular functions (b410–429) | 4 (1.5) | 4 (1) | ✔ |
| 24 | - Respiratory functions (b440–449) | 4 (2.25) | 4 (0.5) | ✔ |
| 25 | - Nutritional status | 4 (1.25) | 4 (1) | ✔ |
| 26 | - Voice and speech functions (b3) | 3.5 (2.25) | 4 (2) | × |
| 27 | - Hematological and immunological functions (b430–439) | 3 (1.25) | 3 (0) | × |
| 28 | - Swallowing functions (b5) | 3 (2.25) | 3 (1) | × |
| 29 | - Medical and medication management | 4 (2) | 4 (2) | × |
| 30 | Hemodynamic and cardiovascular stability is required before attending a physical rehabilitation program | 3.5 (1.5) | 3 (1) | × |
| 31 | Physical rehabilitation interventions need to be focused on recovery at the level of body functions and structures, based on experience-dependent neuroplasticity | 3.5 (1.25) | 3.5 (1) | × |
| Activity and Participation | ||||
| 32 | Physical rehabilitation interventions should be focused on a broader context than body functions and structures alone | 5 (0.25) | ✔ | |
| 33 | Activities related to community and daily life (d9) determine priorities for a child or young person to work on during physical rehabilitation interventions | 5 (1) | ✔ | |
| 34 | Rehabilitation is a process of creating an environment that facilitates participation, encouraging activity and thus associated improvements in body structure and function | 4.5 (1) | ✔ | |
| 35 | The way a physical intervention is delivered depends on the child’s cognitive and communication abilities | 5 (1) | ✔ | |
| 36 | If a child or young person has the ability to learn and apply knowledge (d1), the clinician should provide an active approach in physical rehabilitation | 5 (0) | ✔ | |
| 37 | If a child or young person is not able to learn and apply knowledge (d1), the intervention should focus on context (e.g. training of caregivers) in physical rehabilitation interventions | 4 (1.25) | 4 (0) | ✔ |
| 38 | Communication abilities of the child and young person (d3) guide the level of support and education provided by the team to others | 4 (1.25) | 4 (0.5) | ✔ |
| 39 | Physical rehabilitation interventions need to be focused on participation (d9) | 4 (1.25) | 4 (0) | ✔ |
| 40 | Participation is not a major direct focus in subacute rehabilitation, but all interventions are done with future participation in mind | 4 (1.5) | 4 (1) | ✔ |
| 41 | Physical rehabilitation primarily focuses on (re)gaining the ability to interact with the environment | 4 (1.25) | 4 (1) | ✔ |
| 42 | Activities related to general tasks and demands (d2) should always be analyzed to identify the underlying features of the execution of tasks under different circumstances | 4 (2) | 4 (0.5) | ✔ |
| Importance of variables related to activities and participation when determining the content and focus of physical rehabilitation interventions during subacute phase: | ✔ | |||
| 43 | - Ability to learn and apply knowledge (d1) | 5 (1) | ✔ | |
| 44 | - Communication ability (d3) | 4 (1.25) | 4 (1) | ✔ |
| 45 | - Motor ability (d4) | 4 (2.25) | 4 (1) | ✔ |
| 46 | - Ability to interact with people (d7) | 4 (2) | 4 (1) | ✔ |
| Importance of variables related to activities and participation when determining the content and focus of physical rehabilitation interventions during subacute phase: | ||||
| 47 | - General tasks and demands (e.g. single-multi tasks, routines) (d2) | 3.5 (3) | 3 (1) | × |
| 48 | - Ability related to self-care (d5) | 2.5 (3) | 3 (2) | × |
| 49 | - Ability to engage in community and social life (d9) | 2.5 (2) | 3 (2) | × |
| 50 | Physical rehabilitation interventions primarily focus on mobility related activities (d4) (e.g. walking, moving, handling objects) | 3.5 (1.25) | 3 (1) | × |
| 51 | The basic principle is to elicit as much physical activity as possible based on neuroplasticity | 4 (2.5) | 4 (2) | × |
| 52 | Well practiced-activities will only induce neural plasticity if the child or young person perceives it to be as meaningful and important | 2.5 (4.25) | 3 (2) | × |
| Contextual factors (environmental and personal) | ||||
| 53 | Understanding of environmental (context) and personal factors helps the rehabilitation team to know the facilitators and barriers during subacute rehabilitation | 5 (0) | ✔ | |
| 54 | The family situation (e.g. level of understanding, psychosocial situation) (e3) influences the way parents are involved during the rehabilitation process | 5 (0.25) | ✔ | |
| 55 | Family involvement allows therapy to be extended to daily activities | 5 (1) | ✔ | |
| 56 | Family involvement increases the dosage of physical rehabilitation interventions | 5 (1) | ✔ | |
| 57 | Parents and children and young people should be involved in goal setting | 5 (1) | ✔ | |
| 58 | Collaborative goal setting with parents promotes coherence within the process | 5 (1) | ✔ | |
| 59 | Families need education to generalize and transfer skills to a variety of contexts | 5 (0) | ✔ | |
| 60 | Education and instruction to family and friends is a key component of physical rehabilitation interventions | 5 (0.25) | ✔ | |
| 61 | Knowledge of a child or young person’s interest is necessary to keep them engaged during physical rehabilitation interventions (d9) | 5 (0.25) | ✔ | |
| 62 | Fun is a key to increase engagement during physical rehabilitation | 5 (1) | ✔ | |
| 63 | Motivation, attention and engagement are influenced by the relevance and perception of potential rewards associated with a movement task | 5 (1.25) | 5 (0.5) | ✔ |
| 64 | Motivation (b1) is a key factor for the degree of success achieved by the child or young person in physical rehabilitation interventions | 4.5 (1.25) | 4 (1) | ✔ |
| 65 | To increase motivation, interventions should always be in line with the child and young person’s own identified goals | 4 (2) | 4 (1) | ✔ |
| 66 | Positive peer-interaction (d7) should be elicited during physical rehabilitation interventions | 5 (2) | 5 (1) | ✔ |
| 67 | Housing adaptations (structural modifications of physical home environment) (e1) are a priority in physical rehabilitation interventions as they reflect what a child will need for discharge | 4.5 (1.25) | 4 (1) | ✔ |
| Importance of variables related to environmental factors (child-context) when determining the content and focus of physical rehabilitation interventions during subacute phase: | ✔ | |||
| 68 | - Involvement of family | 5 (0.25) | ✔ | |
| 69 | - The family situation (e3) (e.g. level of understanding, psychosocial situation) | 5 (1) | ✔ | |
| 70 | - Availability of resources (e5) | 4.5 (2) | 5 (1) | ✔ |
| 71 | - Factors related to the home environment (e2) | 4.5 (1.25) | 4.5 (1) | ✔ |
| 72 | - Housing adaptations (e1) | 4 (1.25) | 4 (0) | ✔ |
| 73 | - Activities related to community and daily life (d9) | 4 (1.25) | 4 (1) | ✔ |
| 74 | - Factors related to support and relationship (e.g. family, friends) (e3) | 4 (1.25) | 4 (0.5) | ✔ |
| 75 | - Attitudes and norms held by family and friends (e4) | 4 (1.25) | 4 (0.5) | ✔ |
| 76 | - Availability of equipment (e1) | 4 (2) | 4 (1) | ✔ |
| Importance of variables related to personal factors when determining the content and focus of physical rehabilitation interventions during subacute phase: | ||||
| 77 | - Pre-injury developmental stage | 4.5 (1) | ✔ | |
| 78 | - Personality | 4 (1) | ✔ | |
| 79 | - Internal motivation | 4 (1) | ✔ | |
| 80 | - Personal perseverance and resilience | 4 (1) | ✔ | |
| 81 | - Age at injury | 4 (1.25) | 4 (1) | ✔ |
| Importance of environmental variables when determining the content and focus of physical rehabilitation interventions during subacute phase: | ||||
| 82 | - Involvement of friends/peers | 4 (1.5) | 4 (2) | × |
| 83 | - Services, systems and policies (e.g. insurance, school, leisure activities) (e5) | 4 (1.25) | 4 (2) | × |
| Rehabilitation setting and content | ||||
| 84 | The rehabilitation setting environment should be inviting and able to adapt to the individual needs of the child and young person | 5 (1) | ✔ | |
| 85 | Physical rehabilitation for children and young people needs a pediatric appropriate environment, and therefore should not take place in an adult rehabilitation environment | 4.5 (1) | ✔ | |
| 86 | Meaningful context increases motivation and engagement in the rehabilitation process | 4.5 (1) | ✔ | |
| 87 | Enriched environment supports neuroplasticity and recovery in the subacute phase | 4 (1.25) | 5 (1) | ✔ |
| 88 | Meaningful context reduces cognitive and emotional load | 4 (1.5) | 4 (1) | ✔ |
| 89 | External support/personnel (e5) available throughout the day promotes carryover of treatment goals | 4.5 (1) | ✔ | |
| 90 | Promotion of activities should be encouraged as soon as possible | 4.5 (1) | ✔ | |
| 91 | Physical rehabilitation interventions should be as functional as possible | 4 (1.25) | 4 (1) | ✔ |
| 92 | The amount of (environmental) stimulation needs to be adjusted to the individual needs of the patient | 5 (0) | ✔ | |
| 93 | Physical rehabilitation interventions should focus on the developmental needs of the child or young people | 5 (1) | ✔ | |
| 94 | Physical rehabilitation interventions need to be aligned with the child and young person’s individual needs (personalized care) | 5 (1) | ✔ | |
| 95 | Dosage of physical rehabilitation interventions need to be tailored to the child and young person’s condition | 5 (1) | ✔ | |
| 96 | Equipment (products and technology) (e1) should be personalized, comfortable and age appropriate. | 5 (0) | ✔ | |
| 97 | Equipment (e1; products and technology) can be applied in physical rehabilitation interventions to modify physical environment (home/school) to permit participation | 5 (0) | ✔ | |
| 98 | Equipment (e1) can be applied to promote independence and interaction with environment. | 5 (0.25) | ✔ | |
| 99 | Devices are resources, but not ends in themselves | 5 (1) | ✔ | |
| 100 | Equipment (e1) can be applied to increase frequency and intensity of practice in physical rehabilitation interventions | 4.5 (1.25) | 4 (1) | ✔ |
| 101 | Each practitioner should be aware of the resources (e.g. products and technology (e1), services (e5)) available to maximize their support in subacute physical rehabilitation and to promote recovery | 5 (1) | ✔ | |
| 102 | Multidisciplinary collaboration and coordination are more beneficial than a monodisciplinary approach | 5 (0) | ✔ | |
| 103 | Multidisciplinary collaboration should be extended to family and friends where possible | 5 (1) | ✔ | |
| 104 | Success of rehabilitation depends on a three-way connection among child, parents and therapist(s) | 5 (0) | ✔ | |
| 105 | Safety and trust are fundamentals in therapist-child and young person relationship | 5 (0.25) | ✔ | |
| 106 | Therapeutic alliance (personal connection, professional collaboration and family collaboration) is the basis for physical rehabilitation intervention | 5 (1) | ✔ | |
| 107 | A therapist must be able to modify the intervention to the child and young person’s circumstances | 5 (0) | ✔ | |
| 108 | A therapist must have an open mind related to recovery where realism and hope can coexist | 5 (0.25) | ✔ | |
| 109 | A therapist must have sufficient knowledge about the injury, recovery mechanisms and relation to typical development | 5 (1) | ✔ | |
| Importance of environmental variables when determining the content and focus of physical rehabilitation interventions during subacute phase: | ✔ | |||
| 110 | - Multidisciplinary collaboration | 5 (0) | ✔ | |
| 111 | - Therapist-patient relationship | 5 (0) | ✔ | |
| 112 | - Therapist’s general attitude | 5 (0.25) | ✔ | |
| 113 | - Therapist-parent relationship | 5 (1) | ✔ | |
| 114 | - ABI-related knowledge base of the therapist | 5 (1) | ✔ | |
| 115 | - Stimulating environment | 5 (1) | ✔ | |
| 116 | - Adequate rehabilitation facilities | 5 (1.25) | 5 (1) | ✔ |
| The qualities of a good therapist are: | ✔ | |||
| 117 | - Sensitive | 5 (1) | ✔ | |
| 118 | - Responsive | 5 (0) | ✔ | |
| 119 | - Respectful | 5 (0) | ✔ | |
| 120 | - Humorous (fun) | 4 (0.25) | ✔ | |
| 121 | - Positive attitude | 5 (0.25) | ✔ | |
| 122 | - Empathetic | 5 (0.25) | ✔ | |
| 123 | - Good communication | 5 (0) | ✔ | |
| 124 | - Flexible | 5 (0) | ✔ | |
| 125 | - Ability to listen | 5 (0) | ✔ | |
| 126 | - Focus on capacities rather than deficiencies | 5 (1) | ✔ | |
| Importance of physical rehabilitation content variables during subacute phase: | ||||
| 127 | - Meaningful context of practice | 5 (1) | ✔ | |
| 128 | - Fun | 4.5 (1) | ✔ | |
| 129 | - Dosage of practice (FITT) | 5 (2) | 5 (1) | ✔ |
| 130 | - Devices | 3.5 (1) | 4 (1) | ✔ |
| 131 | - Multisensory stimulation | 3.5 (2.25) | 4 (1) | ✔ |
| 132 | Therapists’ expectations of change and recovery influence therapy content and ambitions of rehabilitation goals | 4 (2) | 4 (1.5) | × |
| 133 | Continuity of care by the same team increases quality of care | 4 (2) | 4 (2) | × |
| 134 | Devices for early verticalization should be encouraged in physical rehabilitation intervention | 3.5 (2.75) | 4 (2) | × |
| 135 | Alternative therapies (e.g. art, music, massage, acupuncture, hospital animals) should be considered during the subacute rehabilitation phase | 4 (2.25) | 4 (2) | × |
| 136 | Interventions using virtual/mixed reality increase engagement and motivation | 3 (1.25) | 3 (0) | × |
| 137 | Physical rehabilitation interventions should be offered in peer groups when possible (d7) | 3.5 (1.5) | 3 (1) | × |
| 138 | Multisensory stimulation promotes the engagement of all systems required for optimal task performance | 3.5 (2.25) | 3 (1) | × |
| 139 | Multidisciplinary meetings must take place at least weekly | 3 (3) | 3 (3) | × |
| (b1), (d7) etc. refers to the chapter of the ICF-CY (3). | ||||
| ABI: acquired brain injury; FITT: frequency, intensity, time, type | ||||
| ✔: consensus (median Likert score ≥ 4 and IQR ≤ 1), ×: no consensus (median Likert score < 4 or IQR > 1). | ||||
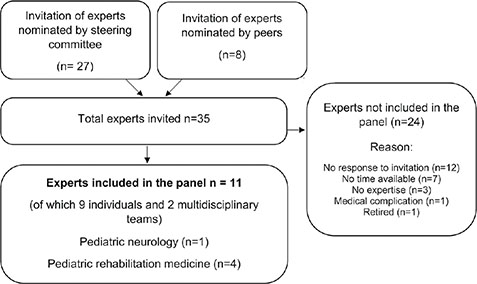
Fig. 2. Selection procedure expert Delphi panel.
Category 1: Health condition (injury-related factors)
Consensus was reached on 7 of 9 statements (78%). The expert panel agreed that the stage of recovery, severity of injury, time since injury and comorbidities are important variables when determining content and focus of physical rehabilitation (statements 4–7). In addition, the child’s clinical presentation, prognosis and rate of progress will affect the therapists’ decisions regarding therapy content. It is important that therapists can cope with rapidly changing clinical features (e.g. progression or decline in motor abilities) that are common in this population (statements 1–2).
Category 2: Body Functions
Consensus was reached on 16 of 22 statements (73%). In addition to physical variables related to neuromusculoskeletal, cardiovascular and respiratory functions (statements 22–24), mental functions (including cognitive functions, such as consciousness, attention and stimulus sensitivity) were key considerations in the selection of physical rehabilitation interventions (statements 10, 15–18). Furthermore, fatigue and adequate sleep were seen to play an important role in determining dosage of physical rehabilitation interventions (statements 11, 12, 14, 20).
Category 3: Activity and Participation
Consensus was reached on 15 of 21 statements (71%). The expert panel reached consensus on the importance of participation-focused interventions (statement 32, 39) and agreed that physical rehabilitation should be executed in a functional context with encouragement of meaningful activities related to community and daily life activities with future participation in mind (statement 33, 34, 40, 41). They agreed that the child’s ability to learn determines whether the intervention focuses on active involvement of the child in the programme, or focuses on context (e.g. training of caregivers) (statements 35–37, 43). The experts indicated that the ability to follow simple commands is a key criterion for minimal cognitive requirement for a child or adolescent to actively participate in a rehabilitation programme. This includes periods of alertness where the child or adolescent is at least partially oriented.
Category 4: Contextual factors (environmental and personal factors)
Consensus was reached on 29 of 31 statements (94%). The experts consensually ranked family involvement as very important (statement 68), both in goalsetting (statements 57, 58) and in therapeutic activities to stimulate transfers of skills to a variety of contexts and to increase dosage of physical rehabilitation interventions (statements 55, 56). To ensure family involvement, education and instruction to family members was seen as very important (statements 59, 60). With respect to personal factors, the experts agreed on the importance of aligning with the interest of the child or adolescent to increase motivation and engagement during therapeutic meaningful activities (statements 61–65). Finally, the experts stressed the importance of the child’s age and pre-injury developmental stage as it highly influences decision-making about content and focus of physical rehabilitation interventions.
Category 5: Rehabilitation setting and content
Consensus was reached on 48 of 56 statements (86%). The expert panel consensually ranked a paediatric appropriate rehabilitation setting as very important (statements 84, 85, 116), including meaningful context and enriched environment to support neural plasticity and recovery (statements 86–88, 115, 127). Equipment could be used as resources to increase dosage of clinical practice, promote independence of interaction with environment, as long as it is personalized, comfortable and age appropriate (statements 96–100, 130). The panel agreed unanimously on the added value of multidisciplinary collaboration over monodisciplinary approach with an essential role for the 3-way connection among child, parents and therapists (statements 102–106, 110, 111, 113). The therapist’s contingent attitude and qualities were endorsed as important (statements 107–109, 112, 114, 117–126). With respect to physical rehabilitation intervention characteristics, dosage of practice (FITT: frequency, intensity, time and type) was scored as very important (statement 129). However, no consensus was reached on statements on specific content relating to the FITT factors. The expert panel stressed the importance of tailored physical interventions, aligned with the child and adolescent’s individual and developmental needs (statements 92–95, 107).
DISCUSSION
This Delphi study resulted in consensus rankings of statements regarding physical rehabilitation interventions in children and adolescents with ABI during the subacute phase. Clinically relevant translation of the results led to 3 important topics to discuss: (i) the majority of the statements’ content are related to general principles of paediatric rehabilitation (19) and to a limited extent specific to children and adolescents with ABI, (ii) active participation in a rehabilitation programme should start as soon as the child or adolescent has the ability to follow simple commands, and (iii) the principles of physical activity (4) and motor learning (20) are recommended as a foundation for the determination of intervention characteristics in clinical practice.
The findings of this study align with current paediatric neurorehabilitation trends, from trying to fix the underlying biomedical impairments to promoting activities and participation meaningful to the child and their family, an idea which comes together in the “F-words of child development” (19). The 6 F-words are reflected in our findings: function, friends and fun (promoting activities in meaningful activities to increase motivation during physical rehabilitation), family (involvement and engagement of parents and siblings), fitness (physical activities during subacute phase) and future (alignment of activities with future participation in the natural environment of the child). The underlying general principles of physical activity, participation-focused interventions and family-centred care are widely supported in paediatric neurorehabilitation (21–24). In conjunction with the consensus statements found in the current study, we recommend that these generic principles form the basis for subacute physical rehabilitation practices. The expert panel highlighted the importance of the individual child’s clinical presentation. Therefore, physical rehabilitation should include a participation-focused and family-centred approach that is tailored to the individual needs of the child and their family. Partnership with families that promote a 3-way relationship among the child, families and therapists is essential in securing a personalized health approach (25).
According to the panel, active participation in a rehabilitation programme has a number of caveats, such as fatigue and the child’s own ability to follow simple commands. These were seen as the minimal cognitive key criteria. Several assessment tools (Rancho Los Amigos Scale (26), Post-Acute Level of Consciousness Scale (27) and WeeFIM (28)) were mentioned as measures that may be appropriate to assess which child can actively participate in a rehabilitation programme. Yet, future research is needed to determine more sensitive and specific cut-off points that can guide clinical decision-making.
The current study found that the content of physical rehabilitation interventions, such as dosage of practice was scored as very important. However, no consensus was reached as to the determination of dose-response variables in clinical practice. This may be due to the lack of a definition of dosage, leading to the term dosage being operationalized in different ways which makes the quantification of dosage complex (5, 10). In their remarks during the Delphi rounds, the panel referred multiple times to principles of motor learning to inform clinical practice in the ABI-population (20). These principles once again highlight relevant factors, such as specificity and dosage of practice, including repetition, intensity and time to enhance experience-dependent neuroplasticity in models of learning and brain damage (4, 5). These concepts align with the underlying principle that greater amounts of practice increase learning, which could have a positive effect during the subacute phase after ABI (29, 30). These principles are supported in animal and adult populations studies (7, 8, 30), and because of the similarities in pathophysiology and recovery mechanisms in children and adolescents with ABI (4, 7), we hypothesize that similar principles could be applied to them (9, 29). Although there are no specific guidelines, the determination for intervention characteristics should be based on the clinical reasoning process of the therapist in which knowledge of pathophysiology, recovery mechanisms, and prognosis in paediatric ABI should be aligned with clinical presentation, patient goals and outcome measurements.
Study strengths and limitations
The strengths of this study were the international panel with large experience in rehabilitation in children and adolescents with ABI, the high response rates during the Delphi rounds and the structured methodology. In addition, this study is complementary to the expanding research in adult ABI-population and associated initiatives to optimize and intensify physical rehabilitation. The study also had some limitations. The study specifically focused on the subacute phase, and therefore the results cannot simply be generalized to other stages of recovery. While the fictitious case (provided in round 1b to facilitate the expert’s individual thinking process) was of a child with TBI, it should be stressed that we did not find any results during the Delphi rounds that indicated a differentiation between ABI or TBI. This is supported by statement 8, where no consensus was reached on the importance of aetiology of injury when determining content and focus of physical rehabilitation interventions during the subacute phase. Moreover, the scope of the current study did not include rehabilitation programmes for children and adolescents with (prolonged) disorders of consciousness for whom natural history of recovery, prognosis, and treatment has yet to be established (31). For the latter population, various special treatment programmes have been developed and recommended (31, 32). Although eligible panellists were carefully recruited, selection bias could not be avoided. We are aware that all panellists are located in Western countries and that no experts from developing countries participated in this study. Due to the relatively small number of experts within the panel it is emphasized that the results of this study should not be seen as a definitive guideline. Although 2 panellists were supported by their multidisciplinary team, which probably resulted in broadly-based well-considered responses, the occurrence of group conformity (groupthink) may have negated the benefits of the anonymous nature of a Delphi process in their cases (33). The panel mentioned that the impact of a child’s developmental stage influenced their ranking of the statements, since no distinction had been made between age groups. This may have affected the outcome of the second and third Delphi rounds. The Delphi study was conducted online with panellists only given the opportunity to add written comments. Thus, it was not possible for the panellists to discuss the comments and expand on their thoughts. Future Delphi projects should consider a joint meeting with all panellists for in-depth discussions.
Recommendations for future research
The efforts to develop an evidence-based physical rehabilitation intervention programme for children and adolescents with ABI remain a research priority. Given the potential for intensive physical rehabilitation in the subacute phase, future studies should carefully determine intervention characteristics building from structured clinical assessment (34). We stress the importance of including an adequate description of rehabilitation content across all ICF-CY domains in future publications in order to improve both the interpretability of the results for clinician users and the replicability of future effectiveness studies. The Pediatric Rehabilitation Ingredients Measure (PRISM) is a promising tool to describe paediatric rehabilitation content and effort, and may contribute to a better understanding of the active ingredients of rehabilitation interventions (35). Together with systematic multicentre data collection to obtain broad (large sample sizes) and deep (multiple measures across multiple domains) datasets, the inherent heterogeneity of the population can then be used to better understand and predict outcomes and rehabilitation potential, which could facilitate a step towards data-driven precision rehabilitation medicine (36).
CONCLUSION
This Delphi study emphasizes the careful consideration of injury-related factors, and physical and cognitive functions when designing intensive physical rehabilitation interventions for children and adolescents with ABI during the subacute phase. In addition, early promotion of physical activities, participation-focused interventions, and family-centred care are basic ingredients of physical rehabilitation in children and adolescents with ABI. Although no consensus was reached on the optimal dosing of physical interventions, principles of motor learning and neural plasticity indicate that the amount of physical practice is suggested to have potential impact on children and adolescents with ABI. The translation of these principles into a rehabilitation programme requires tailoring by the clinician to the clinical presentation and developmental needs of the child or adolescent.
ACKNOWLEDGEMENTS
We thank the multidisciplinary rehabilitation team from The Children’s Trust (UK) including Gemma Kelly, Jo Harbinson, Sharon Tuppeny, Krishna Patel, Sammy Randall, Ruth Moys, Amy Wright, Anu Chatterjee, Becky Micklethwaite, Savannah Salsone, Kylie Langridge and Rachel Garrod, headed by Dr Lorna Wales and the multidisciplinary rehabilitation team of Saint Maurice Hospitals (France) including Geneviève Abada, Céline Chavanne, Amaia Mintegui, Vanessa Druet, Pascaline Kehlhoffner, Marion Travers, Caroline Hermet and Carmen Arteaga Sanchez, headed by Dr Mathilde Chevignard. Christiaan Gmelig Meyling received an educational grant from De Hoogstraat Rehabilitation Scientific Research Fund.
Contributors: Pediatric ABI Collaborative (collaborators). Mathilde Chevignarda,b,c, Carol DeMatteod, Rob Forsythe, Sarah J Knightf,g,h, Andreas Meyer-Heimi, Karin Reuter-Ricej, Peter Rumneyk Jennifer L Ryanl,m, Stacy J. Suskauern, Ruud van der Veeno,p and Lorna Walesq
aRehabilitation Department for Children with Acquired Neurological Injury, Saint Maurice Hospitals, Saint Maurice, France; bSorbonne Université, Laboratoire d’Imagerie Biomédicale, LIB, CNRS, INSERM, F-75006, Paris, France; cSorbonne Université, GRC 24 Handicap Moteur et Cognitif et Réadaptation (HaMCRe), Paris, France; dCanChild Centre for Childhood Disability Research, McMaster University, Hamilton, Ontario, Canada; eTranslational Clinical Research Institute, Newcastle University, UK; fDepartment of Neurodisability and Rehabilitation, Murdoch Children’s Research Institute, Melbourne, Australia; gVictorian Paediatric Rehabilitation Service, The Royal Children’s Hospital, Melbourne, Australia; hDepartment of Paediatrics and School of Psychological Sciences, The University of Melbourne, Melbourne, Australia; iSwiss Children’s Rehab, University Children’s Hospital Zurich, Switzerland; jSchool of Nursing/School of Medicine, Department of Pediatrics, Division of Pediatric Critical Care Medicine, Duke University, Durham, NC, USA; kUniversity of Toronto, Division of Paediatrics, Toronto, Canada; lBloorview Research Institute, Holland Bloorview Kids Rehabilitation Hospital, Toronto, Canada; mRehabilitation Sciences Institute, University of Toronto, Toronto, Canada; nKennedy Krieger Institute, Departments of Physical Medicine & Rehabilitation and Pediatrics, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA; oAmsterdam UMC, University of Amsterdam, Department of Pediatrics, Follow-Me program and Emma Neuroscience Group, Emma Children’s Hospital, Meibergdreef 9, Amsterdam, The Netherlands; pDaan Theeuwes Center for Intensive Neurorehabilitation, Woerden, The Netherlands; qThe Children’s Trust, Tadworth, UK.
REFERENCES
- Bedell GM. Functional outcomes of school-age children with acquired brain injuries at discharge from inpatient rehabilitation. Brain Inj 2008; 22: 313–324. DOI: 10.1080/02699050801978948.
- Anderson V, Catroppa C, Morse S, Haritou F, Rosenfeld J. Functional plasticity or vulnerability after early brain injury? Pediatrics 2005; 116: 1374–1382. DOI: 10.1542/peds.2004-1728.
- WHO. International Classification of Functioning, Disability, and Health: Children & Youth Version: ICF-CY. Geneva: World Health Organization; 2007.
- Kleim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J Speech Lang Hear Res 2008; 51: S225–239. DOI: 10.1044/1092-4388(2008/018).
- Maier M, Ballester BR, Verschure P. Principles of neurorehabilitation after stroke based on motor learning and brain plasticity mechanisms. Front Syst Neurosci 2019; 13: 74. DOI: 10.3389/fnsys.2019.00074.
- French B, Thomas LH, Coupe J, McMahon NE, Connell L, Harrison J, et al. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst Rev 2016; 11: Cd006073. DOI: 10.1002/14651858.CD006073.pub3.
- Konigs M, Beurskens EA, Snoep L, Scherder EJ, Oosterlaan J. Effects of timing and intensity of neurorehabilitation on functional outcome after traumatic brain injury: a systematic review and meta-analysis. Arch Phys Med Rehabil 2018; 99: 1149–1159 e1141. DOI: 10.1016/j.apmr.2018.01.013.
- Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. Lancet 2011; 377: 1693–1702. DOI: 10.1016/S0140-6736(11)60325-5.
- Gmelig Meyling C, Verschuren O, Rentinck IR, Engelbert RHH, Gorter JW. Physical rehabilitation interventions in children with acquired brain injury: a scoping review. Dev Med Child Neurol 2022; 64: 40–48. DOI: 10.1111/dmcn.14997.
- Forsyth R. The difference rehabilitation can make after acquired brain injury. Dev Med Child Neurol 2022; 64: 7. DOI: 10.1111/dmcn.15007.
- Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol 2014; 67: 401–409. DOI: 10.1016/j.jclinepi.2013.12.002.
- Jünger S, Payne SA, Brine J, Radbruch L, Brearley SG. Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliative Medicine 2017; 31: 684–706. doi:10.1177/0269216317690685
- Habibi A, Sarafrazi A, Izadyar S. Delphi Technique Theoretical Framework in Qualitative. Int J Eng Sci 2014; 3: 8–13.
- Okoli C, Pawlowski SD. The Delphi method as a research tool: an example, design considerations and applications. Informat Manag 2004; 42: 15–29. DOI: https://doi.org/10.1016/j.im.2003.11.002.
- Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS One 2011; 6: e20476. DOI: 10.1371/journal.pone.0020476.
- Hsieh H-F, Shannon S. Three approaches to qualitative content analysis. Qualitative health research 2005; 15: 1277–1288. DOI: 10.1177/1049732305276687.
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs 2008; 62: 107–115. DOI: https://doi.org/10.1111/j.1365-2648.2007.04569.x.
- von der Gracht HA. Consensus measurement in Delphi studies: review and implications for future quality assurance. Technolog Forecast Social Change 2012; 79: 1525–1536. DOI: https://doi.org/10.1016/j.techfore.2012.04.013.
- Rosenbaum P, Gorter JW. The ‘F-words’ in childhood disability: I swear this is how we should think! Child Care Health Dev 2012; 38: 457–463. DOI: 10.1111/j.1365-2214.2011.01338.x.
- Kitago T, Krakauer JW. Motor learning principles for neurorehabilitation. Handb Clin Neurol 2013; 110: 93–103. DOI: 10.1016/B978-0-444-52901-5.00008-3.
- Novak I, Morgan C, Fahey M, Finch-Edmondson M, Galea C, Hines A, et al. State of the Evidence Traffic Lights 2019: systematic review of interventions for preventing and treating children with cerebral palsy. Curr Neurol Neurosci Rep 2020; 20: 3. DOI: 10.1007/s11910-020-1022-z.
- Verschuren O, Hulst RY, Voorman J, Pillen S, Luitwieler N, Dudink J, et al. 24-hour activity for children with cerebral palsy: a clinical practice guide. Dev Med Child Neurol 2021; 63: 54–59. DOI: 10.1111/dmcn.14654.
- Miutz LN, Burma JS, Lapointe AP, Newel KT, Emery CA, Smirl JD. Physical activity following sport-related concussion in adolescents: a systematic review. J Appl Physiol (1985) 2022; 132: 1250–1266. DOI: 10.1152/japplphysiol.00691.2021.
- Rivara FP, Ennis SK, Mangione-Smith R, MacKenzie EJ, Jaffe KM, National Expert Panel for the Development of Pediatric Rehabilitation Quality Care I. Quality of care indicators for the rehabilitation of children with traumatic brain injury. Arch Phys Med Rehabil 2012; 93: 381–385 e389. DOI: 10.1016/j.apmr.2011.08.015.
- Jenkin T, Anderson V, D’Cruz K, Collins A, Muscara F, Scheinberg A, et al. Engaging children and adolescents with acquired brain injury and their families in goal setting: the clinician perspective. Neuropsychol Rehabil 2022; 32: 104–130. DOI: 10.1080/09602011.2020.1801470.
- Lin K, Wroten M. Ranchos Los Amigos. StatPearls. Treasure Island (FL); 2022.
- Eilander HJ, van de Wiel M, Wijers M, van Heugten CM, Buljevac D, Lavrijsen JC, et al. The reliability and validity of the PALOC-s: a post-acute level of consciousness scale for assessment of young patients with prolonged disturbed consciousness after brain injury. Neuropsychol Rehabil 2009; 19: 1–27. DOI: 10.1080/09602010701694822.
- Rehabilitation UDSfM. The WeeFIM II clinical guide, Version 6.0. 2006: UDSMR Buffalo, NY; 2006.
- Levac D, Missiuna C, Wishart L, Dematteo C, Wright V. Documenting the content of physical therapy for children with acquired brain injury: development and validation of the motor learning strategy rating instrument. Phys Ther 2011; 91: 689–699. DOI: 10.2522/ptj.20100415.
- Krakauer JW. Motor learning: its relevance to stroke recovery and neurorehabilitation. Curr Opin Neurol 2006; 19: 84–90. DOI: 10.1097/01.wco.0000200544.29915.cc.
- Giacino JT, Katz DI, Schiff ND, Whyte J, Ashman EJ, Ashwal S, et al. Practice Guideline Update recommendations summary: disorders of consciousness: report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Arch Phys Med Rehabil 2018; 99: 1699–1709. DOI: 10.1016/j.apmr.2018.07.001.
- Yeh N, Slomine BS, Paasch V, McLean HB, Suskauer SJ. Rehabilitation in children with disorder of consciousness. Curr Phys Med Rehabil Rep 2019; 7: 94–103. DOI: 10.1007/s40141-019-0214-4.
- Nasa P, Jain R, Juneja D. Delphi methodology in healthcare research: how to decide its appropriateness. World J Methodol 2021; 11: 116–129. DOI: 10.5662/wjm.v11.i4.116.
- Ryan JL, Zhou C, Levac DE, Fehlings DL, Beal DS, Hung R, et al. Gross mostor change after inpatient rehabilitation for children with acquired brain injury: a 10-year retrospective review. Dev Med Child Neurol 2022. DOI: 10.1111/dmcn.15471.
- Forsyth R, Young D, Kelly G, Davis K, Dunford C, Golightly A, et al. Paediatric Rehabilitation Ingredients Measure: a new tool for identifying paediatric neurorehabilitation content. Dev Med Child Neurol 2018; 60: 299–305. DOI: 10.1111/dmcn.13648.
- Covington NV, Duff MC. Heterogeneity is a hallmark of traumatic brain injury, not a limitation: a new perspective on study design in rehabilitation research. Am J Speech Lang Pathol 2021; 30: 974–985. DOI: 10.1044/2020_AJSLP-20-00081.