ORIGINAL REPORT
EFFECT OF VERY EARLY SUPPORTED DISCHARGE VERSUS USUAL CARE ON ACTIVITIES OF DAILY LIVING ABILITY AFTER MILD STROKE: A RANDOMIZED CONTROLLED TRIAL
Ann BJÖRKDAHL, PhD1,2, Lena RAFSTEN, PhD1,2, Cathrine PETERSON, BSc2, Katharina S. SUNNERHAGEN, MD, PhD1,3 and Anna DANIELSSON, PhD1,4
From the 1Institute of Neuroscience and Physiology, Department of Clinical Neuroscience/Rehabilitation Medicine, Sahlgrenska Academy, University of Gothenburg, 2Department of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital, 3Neurocare, Sahlgrenska University Hospital and 4Institute of Neuroscience and Physiology, Department of Health and Rehabilitation, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Objective: To examine the ability to perform basic and instrumental activities of daily life after very early supported discharge vs usual discharge and referral routine during the first year after mild stroke.
Design: A secondary analysis of data from the Gothenburg Very Early Supported Discharge randomized controlled trial.
Patients: A total of 104 patients (56% men; mean (standard deviation) age 75 (11) years) who had experienced a first stroke classified as mild.
Methods: The primary outcome was the Activities of Daily Living Taxonomy score. Stroke Impact Scale (activities of daily living, and mobility) scores was a secondary measure. Patients were randomized to either very early supported discharge with 4 weeks of home rehabilitation provided by a multidisciplinary stroke team, or a control group discharged according to usual routine (referral to primary care when needed). Assessments were performed at discharge, 4 weeks post-discharge, and 3 and 12 months post-stroke.
Results: Instrumental activities of the Activities of Daily Living Taxonomy scores (the lower the better) in the very early supported discharge and control groups were median 4 and 6 (p = 0.039) at 4 weeks post-discharge and 3 and 4.5 (p = 0.013 at 3 months post-stroke, respectively. Stroke Impact Scale (Mobility) median scores (the higher the better) in the very early supported discharge and control groups at 3 months were 97 and 86 (p = 0.040), respectively. There were no group differences in the 2 outcomes at 12 months post-stroke.
Conclusion: Compared with usual discharge routine, team-based rehabilitation during the first month at home is beneficial for instrumental activity in the subacute phase, in patients with mild stroke. One year post-stroke both groups show equal results.
LAY ABSTRACT
After stroke, even mild symptoms may impact ability to perform activities of daily living, such as household chores, outdoor walking and transport. It is necessary to understand more about the effects of different rehabilitation methods after mild stroke. The aim of this study was to investigate whether home-based rehabilitation provided by a stroke team during the first 4 weeks post-discharge after mild stroke is comparable to usual discharge routine implicating referral to primary care when needed, with respect to facilitating simple and complex everyday activities. The home-based rehabilitation programme was tailored to the patients’ own goals and problems. The group receiving supported training at home recovered faster, and was more able than controls to manage activities indoors and outdoors, at both 4 weeks post-discharge and at 3 months post-stroke. Twelve months post-stroke, the group that received usual care had also improved, so there was no longer a difference between the outcomes of the two approaches.
Key words: cerebrovascular disorders; rehabilitation; activities of daily living; hospital to home transition.
Citation: J Rehabil Med 2023; 55: jrm12363. DOI: https://doi.org/10.2340/jrm.v55.12363
Copyright: © Published by Medical Journals Sweden, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/)
Accepted: Jun 5, 2023; Published: Aug 24, 2023
Correspondence address: Anna Danielsson, Institute of Neuroscience and Physiology, Department of Clinical Neuroscience/Rehabilitation Medicine, Sahlgrenska Academy, University of Gothenburg, Box 455, SE-405 30 Gothenburg, Sweden. E-mail: anna.danielsson@neuro.gu.se
Competing interests and funding: The authors have no conflicts of interest to declare.
Medical advances mean that the sequelae of stroke are less severe than in the past; indeed, 66% of acute cases in Sweden in 2021, were classified as mild, this proportion has increased from 63% the last 5 years (1). However, little attention has been paid to how existing interventions meet the needs of today’s stroke population (2–5), particularly with respect to function during activities of daily living (ADL).
Despite the fact that muscle strength is often maintained after mild stroke, functional mobility (6), postural balance (7) and upper limb coordination (8) can still be affected. A study of 455 patients scoring 0, indicating no symptoms, on the initial National Institute of Health Stroke Scale (NIHSS) found cognitive impairment in 23% of patients, motor impairment in 30%, walking dependency in 21%, swallowing disability in 10% and aphasia in 29%; in 2–15% of these patients, deficits persisted at 6 months post-stroke (9). In a population of 97 patients with mean age 55 years, of whom the majority scored 0 on the NIHSS, spatial navigation was impaired in 32% and 25% of patients during the acute phase and at 12 months post-stroke, respectively, with a marked effect on mobility (10).
More complex ADL, which are significant with respect to community living, referred to as instrumental ADL (I-ADL), require higher levels of functional ability (11). An early study (12) conducted 6 months after a minor stroke found that 87% of the 219 patients reported persistent changes, despite being fully independent in terms of basic ADL (B-ADL). Patients reported difficulties with driving, work-related tasks, household management and recreation. Reduced life satisfaction, mainly due to reduced participation in meaningful activities, increased emotional stress, depressed mood (12) and anxiety, can affect real-life functioning (13, 14). Similarly, a narrative review including 34 papers (15) found that even minor stroke requires major life adjustments, both for patients and for their families, leading to a re-evaluation of life plans. Reduced participation in domestic chores, and even larger reductions in work and leisure activities, were reported 7 years post-stroke in 237 stroke survivors (mainly classified as mild) aged under 70 years (11).
Guidelines prioritize early supported discharge (ESD) for patients with mild to moderate symptoms (16). Two studies of ESD have described patients’ expectations after coming home after a stroke with the support of a rehabilitation team (17, 18). One study reported that the major themes were independence and feeling secure at home (18). An important aspect of supported discharge seems to be that patients can rely on the rehabilitation team, thereby ensuring their safety and providing help with person-centred adjustments to their new situation (17).
However, the literature suggests that there is an unmet need with respect to rehabilitation after mild stroke (5); indeed, follow-up studies of I-ADL are scarce in this population of stroke survivors (11). The objective of the current study was therefore to investigate whether very early supported discharge (VESD) delivered by a multidisciplinary stroke-specialized team would improve the ability of patients with mild stroke to perform B-ADL and I-ADL compared with usual care. Changes in ADL after VESD were compared with those after the usual discharge routine implicating referral to primary care when needed, during the first year after mild stroke.
MATERIAL AND METHODS
The current study is a secondary analysis of a prospective randomized controlled trial, the Gothenburg Very Early Supported Discharge (GOTVED) (clinicaltrials.gov: NCT01622205) (19), conducted at a stroke unit at Sahlgrenska University Hospital, Sahlgrenska, Sweden. The GOTVED study included 140 consecutive adult patients (20). The CONSORT checklist (21) was followed. All variables presented in the current study were collected in the GOTVED study.
Due to expected short hospital stays, patients were enrolled on day 2 post-stroke. The inclusion criteria in GOTVED were as follows: confirmed stroke according to World Health Organization (WHO) criteria; age > 18 years; living within 30 min of the stroke unit; 0–16 points on the NIHSS (0–42) (22), 50–100 points on the Barthel Index (BI 0–100) on day 2 post-stroke (23); and, in cases where the BI was 100, the Montreal Cognitive Assessment (MoCA, 0–30) (24) score had to be < 26 on day 2 post-stroke. In addition, for the current study, follow-up data from the ADL Taxonomy (25) and the Stroke Impact Scale (SIS) (26) must be available. The exclusion criteria in GOTVED were: life expectancy < 1 year and an inability to speak Swedish. The GOTVED study was approved by the Regional Ethical Review Board in Gothenburg (reference number 042-11), and all patients provided written informed consent.
Patients were randomized into 1 of 2 groups: an intervention group receiving supported discharge (VESD), or a control group receiving usual care implicating referral to primary care when needed. Randomization was performed by an external person using sealed envelopes. The time-point for discharge in both groups was determined according to the patient’s medical status. The median length of stay at the stroke unit was 9 days, which was much shorter than shown in earlier studies of ESD (27); therefore, the expression “very early supported discharge” was chosen in the GOTVED study. The VESD intervention was delivered 2–4 times/week (over 4 weeks) at the patient’s home by a team from the stroke unit (an occupational therapist, a physiotherapist, and a nurse). The intervention focused on the patient’s individual goals, which were set before discharge, and could include personal care, transfers, and household and/or leisure activities. If relevant, primary care rehabilitation was offered after the intervention period. The control group was discharged from the stroke unit according to the usual routine, which included referral to outpatient primary care, community rehabilitation at a nursing home or own home (with or without assistance), according to the patient’s needs.
Instruments
The assessment instruments and time-points are summarized in Table I.
Descriptive variables. Stroke severity was categorized using the NIHSS (22) on day 2 post-stroke. Overall disability on day 1 post-discharge, and at 3 and 12 months post-stroke, was categorized according to the modified Rankin Scale (mRS, 0–6) (28). Cognitive impairment on day 2 post-stroke, and at 3 and 12 months post-stroke, was assessed using the MoCA (24). Motor function on day 1 post-discharge, and 12 months post-stroke was assessed using the Fugl-Meyer Sensorimotor Assessment (FMA, 0–100) (29), with total scores for the upper and lower extremities. All assessments were performed by an external examiner who played no role in the patients’ treatment.
Primary outcome. For the current study, the ADL Taxonomy (25) was chosen to reflect a structured assessment of everyday function. The ADL Taxonomy includes 12 activities, each based on different hierarchically ordered tasks. The ADL activities are summed into 2 domains: B-ADL and I-ADL. The tasks included in B-ADL are eating, mobility, going to the toilet, dressing, personal hygiene and grooming. Included in I-ADL are transportation, cooking, shopping, cleaning and washing. An item regarding communication is included in the ADL Taxonomy, but was not analysed in the current study. If all tasks involved in a particular activity can be performed, then it is scored as A = 0. For each task that cannot be performed, the letter changes and the number increases by 1 (i.e. B = 1, C = 2, etc.). A score of zero indicates full ability, and a higher score indicates a higher level of difficulty, to perform the task. The summed scores for each domain (B-ADL maximum = 26; I-ADL maximum = 16) were calculated. Assessments were made on day 1 post-discharge (in the following expressed as “discharge”), at 4 weeks post-discharge, and at 3 and 12 months post-stroke.
Secondary outcome. To reflect the patient’s own perspective on ADL and mobility, the SIS 3.0 (26) was used in the current study. The SIS is a multi-dimensional, self-reported measure designed specifically for mild-to-moderate stroke (26). The SIS has 8 domains, divided into several items. Each item is rated based on 5 categories (e.g. from 5 = “not difficult at all” to 1 = “could not do at all”). The SIS is based on activities carried out in the past 2 weeks. An algorithm converts each summed domain score into a score between 0 and 100, with a higher score indicating better self-perceived function. Two domains (domain 5, ADL (comprising 10 items); and domain 6, Mobility (comprising 9 items)) were analysed in the current study. The SIS domains ADL and Mobility both include a combination of B-ADL and I-ADL items; therefore, a sub-analysis of the I-ADL-related items within each of these domains was also carried out. Sub-analysis of the ADL domain was based on 3 items: light household tasks, shopping and heavy household chores. In the Mobility domain, 5 items were selected: walk 1 block, walk fast, climb 1 flight of stairs, climb several flights of stairs, and get in and out of a car. The SIS was administered via an interview conducted at time for discharge, and again at 3 and 12 months post-stroke.
Statistical analysis
The power calculation in GOTVED was based on the primary outcome of the main GOTVED study: the level of anxiety on the Hospital Anxiety and Depression Scale (HADS). For a power of 80% and a p-value of 0.05 (2-sided test), 44 patients per group were required in GOTVED.
Data were analysed using IBM SPSS statistics for Windows, version 28.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used for demographic and clinical background data. Since most data were ordinal, median values with 25% and 75% percentiles (interquartile range, IQR) were calculated. The distribution of scores for each item of the ADL Taxonomy was visualized using boxplots. Inter-group differences were analysed using the Mann–Whitney U test. Scores of the primary and secondary outcome measures were analysed to identify group differences at each assessment time-point, and visualized as scatter plots. Sub-analyses of the I-ADL-related items of the SIS were also examined to identify inter-group differences. Changes in total scores for the primary and secondary outcome measures between discharge and follow-up were calculated, expressed as change scores and analysed for inter-group differences.
RESULTS
The following presentation of results is based on analyses of the material included in the current study. Overall, 104 patients met the inclusion criteria for the current study. The VESD and control groups comprised 58% and 56% males (mean ages, 74.8 and 74.1 years), respectively. A flow chart of the current study is shown in Fig. S1. There were no significant differences between the groups with respect to demographic or clinical data on day 2 post-stroke and at discharge (Table II). At day 2 post-stroke, the median NIHSS score for all enrolled patients was ≤ 5, with 95% categorized as having mild stroke symptoms. The mRS was ≤ 2, meaning no or slight disability, for 64% of patients. Most patients were independent in terms of basic ADL when assessed using the BI. Overall, 12% of the sample had the maximum BI score, and were therefore included based on their MoCA score (< 26). Day 2 post-stroke, there was no significant difference in MoCA score between the VESD and control groups, although the proportion that fell below the cut-off score was higher in the control group (71%) than in the VESD group (46%). The high FMA scores in almost all participants indicated good motor function. Most patients had had a cerebral infarct, and the distribution of infarcts and haemorrhages was similar between the groups. Approximately 20% of participants in both groups underwent reperfusion therapy.
| Characteristics | VESD N = 52 | Control N = 52 | ||||||
| 2 days post-stroke/discharge | 4 weeks post-discharge | 3 months post-stroke | 12 months post-stroke | 2 days post-stroke/discharge | 4 weeks post-discharge | 3 months post-stroke | 12 months post-stroke | |
| Age, years; mean (SD) | 74.8 (11.2) | 74.1 (12.8) | ||||||
| Men/women, n | 30/22 | 29/23 | ||||||
| Cerebral infarct, n | 51 | 47 | ||||||
| Cerebral haemorrhage, n | 1 | 5 | ||||||
| Thrombolysis, n | 5 | 8 | ||||||
| Thrombectomy, n | 3 | 3 | ||||||
| NIHSS, median (IQR) | 1 (0–2.5)a | 1 (0–2)a | ||||||
| BI, median (IQR) | 80 (65-90)a | 80 (66-94)a | ||||||
| mRS, median (IQR) | 2 (2-3)b | 2 (1-2) | 1 (1-2) | 1.5 (1-2) | 2 (2-3)b | 2(1-3) | 2 (1-3) | 1 (1-3) |
| MoCA, median (IQR) | 24 (20-26)a | 26 (22-27) | 25 (23-27) | 21 (17-25)a | 24 (19-26) | 24 (18-26) | ||
| FMA, median (IQR) | 95 (85–98)b | 98 (93–99) | 97 (87–99)b | 99 (95–100) | ||||
| a2 days post-stroke, bat discharge. | ||||||||
| VESD: very early supported discharge; mRS: modified Rankin Scale; BI: Barthel Index; MoCA: Montreal Cognitive Assessment; FMA: Fugl-Meyer Sensorimotor Assessment; IQR: interquartile range. | ||||||||
The VESD comprised home visits from the rehabilitation team, who provided training to allow achievement of individual goals. The most common goals were improvements in B-ADL and in I-ADL, such as management of home activities, safe outdoor mobility and use of public transport. The VESD group received a median (IQR) of 11 (8–14) home visits during the 4 weeks. In addition, after the 4-week intervention, 45 of the 52 patients in the VESD group received some form of outpatient rehabilitation on a median (IQR) of 14 (7–22) occasions during the remaining 12-month follow-up period. In the control group, 35 of the 52 patients had a median (IQR) of 5 (2–22) outpatient visits post-discharge up until 12 months post-stroke.
When comparing the total scores for the primary and secondary outcomes (ADL Taxonomy and SIS, respectively) at time-point for discharge, no significant differences were found (Table III). However, at 4 weeks post-discharge, the VESD group had significantly fewer difficulties in I-ADL than the control group. At the follow-up 3 months post-stroke, the total scores for the ADL Taxonomy I-ADL domain and SIS Mobility domain showed better function in the VESD group than the control group (Table III). Fig. 1 shows box plots of data at discharge and the 3-month follow-up for the 5 tasks included in the ADL Taxonomy I-ADL. The tasks that were most problematic for both groups were transport, shopping and washing; the figures show how the scores for the 2 groups changed between the 2 assessments. Sub-analysis of the SIS I-ADL-related items showed a significant difference between the groups with respect to ADL (p = 0.011) and Mobility (p = 0.027) scores at 3 months post-stroke, which favoured the VESD group.
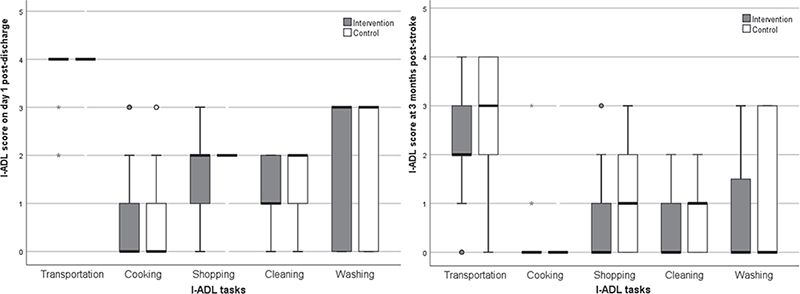
Fig. 1. Boxplots of changes in the scores for instrumental activities of daily living (I-ADL) items in the ADL Taxonomy from discharge to the follow-up 3-months post-stroke. Boxes represent 50% of the material, and top and bottom edges denote the upper and lower quartiles. Black line in the box denotes median value, and whiskers represent minimum and maximum values. The lower the score the better the performance in I-ADL. Zero indicates an ability to perform all actions included within an item, and higher scores denote that 1 or more actions cannot be performed.
Changes in the ADL Taxonomy total scores between discharge and subsequent time-points are shown in Fig. 2. Analysis of changes in the B-ADL scores showed that the VESD group improved significantly faster than the control group (p = 0.048) from discharge to the assessment at 4 weeks post-discharge, which took place directly after the intervention. The median B-ADL score of 1.5 in the VESD group was somewhat higher than that in the control group (i.e. 0) at discharge, although not statistically significant (Table III). With respect to changes in the I-ADL between discharge and 4 weeks post-discharge, there was a tendency toward a greater improvement in the VESD than the control group (p = 0.083), which became significant from discharge to the follow-up at 3 months post-stroke (p = 0.012). As expected, both groups showed marked improvements in the ADL Taxonomy at 12 months post-stroke; consistent with this, group differences in I-ADL evened out and were no longer significant at 12 months post-stroke (p = 0.138). Due to new onset of stroke in 1 case, and cardiorespiratory problems in another, these 2 participants showed a deterioration in ADL Taxonomy from discharge to the 4-week post-discharge assessment; therefore, they were not included in the subsequent analyses. In this subsequent analysis of changes in scores, significant group differences in the B-ADL domain scores between discharge and 4 weeks post-discharge disappeared (p = 0.105), whereas group differences in the I-ADL scores remained about the same at 4 weeks post-discharge (p = 0.062) and at 3 months post-stroke (p = 0.016).
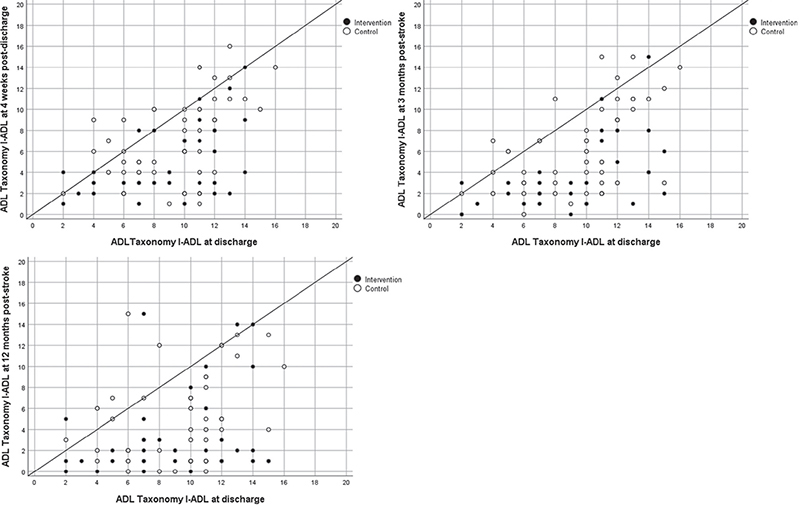
Fig. 2. Total instrumental activities of daily living (I-ADL) score for each patient within the ADL Taxonomy (where a lower value denotes a better outcome). The 3 figures illustrate changes from discharge to each of the assessments (at 4 weeks post-discharge, and at 3 and 12 months post-stroke). Dots below the reference line indicate improvement. Between discharge to 3 months post-stroke, the intervention group improved significantly more than the control group (p = 0.012).
Regarding the total scores for the self-reported outcomes on the SIS domains ADL and Mobility, changes over time are shown in Fig. 3. The change in the score for the ADL domain from discharge to the follow-up 3 months post-stroke was significantly larger for the VESD group than for the control group (p = 0.049), but there was no difference between discharge and the follow-up 12 months post-stroke. The same trend was seen for the Mobility domain, in which the change in the score between discharge and 3 months post-stroke differed significantly in favour of the VESD group (p = 0.038); however, the difference disappeared by the follow-up 12 months post-stroke. The patient who had a second stroke showed a large decrease in the scores at the 3-month follow-up. Excluding this patient from the analysis did not change the significance level substantially (p = 0.042).
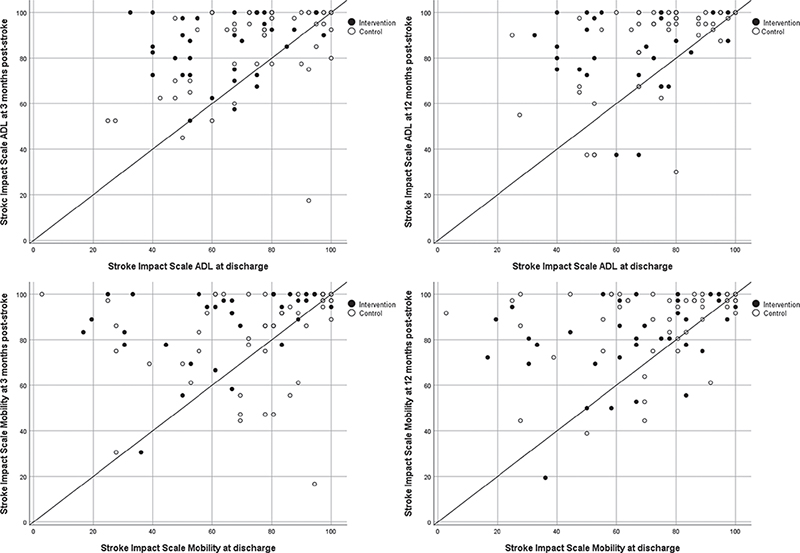
Fig. 3. Stroke Impact Scale (Domain activities of daily living (ADL) and Domain Mobility) scores for each patient (higher values denote better function) at discharge and at 3 months (left panel), and at discharge and 12 months (right panel), post-stroke. Dots above the reference line show a change towards a higher score, indicating improvement over time. At 3 months post-stroke, the very early supported discharge (VESD) intervention group improved more than the control group (p< 0.05).
Although MoCA was an instrument chosen to describe the sample, it may also serve as an explanatory variable. Comparison of the MoCA total score between the groups at 3 months and 12 months post-stroke revealed significant differences at both time-points (p = 0.010 and p = 0.034) in favour of the VESD group.
DISCUSSION
This study found that even though initial stroke severity and general disability were mild, patients still experienced limitations in activity during the first year. These limitations were particularly noticeable for I-ADL. The main finding was that ability to perform daily activities improved faster in the VESD group than in the control group. These inter-group differences in ability were significant at 3 months post-stroke, but disappeared after 1 year post-stroke.
This study showed that, at discharge, most patients were independent in B-ADL. However, the faster improvement seen in the VESD group could be explained by a somewhat higher median B-ADL score at discharge, compared with the control group, which left more room for improvement. Most patients had some difficulties with I-ADL; the most problematic items were transport, shopping and washing. Most patients in the VESD group could already manage shopping and cleaning at 4 weeks post-discharge, but it took longer (up to 12 months) for the control group to manage these items. The more rapid recovery observed in the VESD group is probably due to interventions that focused directly on the patients’ own activity-based goals, which were set before discharge (32). Finch et al. (5) reported unmet needs of patients at 2 weeks, and several remaining limitations at 2 months post hospital-discharge, despite the stroke being classed as minor. The problems were similar to those reported herein; indeed, travelling in the community was the top-rated area requiring help. Other areas of unmet need were dependence in walking, lifting and balancing, as well as difficulties with housekeeping, cooking and shopping. Similarly, Faux et al. (4) found that 1 in 3 patients who had had a transient ischaemic attack or mild stroke experienced difficulty fully re-integrating into the community; hence early and accessible programmes targeted to each patient’s needs and personal situation are warranted.
Life changes significantly after stroke, not only with respect to impairment and increased dependency, but also existentially. People describe a feeling of incomprehensibility and unfamiliarity with the new situation, despite only having had a mild stroke (33). When interviewed at time of discharge according to VESD, patients cited fear and insecurity with respect to their expectations regarding support from the stroke team (18). An important short-term goal of neurorehabilitation is to alleviate emotional distress to improve functioning in daily life (13). After a stroke, there is a need for a fresh perspective when engaging in familiar activities, which could mean reluctance to go out due to a feeling of uncertainty (33). Confidence and satisfaction with function are important factors when appraising one’s own functional competence after brain injury (13). A primary outcome of the main GOTVED study was anxiety, and the hypothesis was that supported discharge may reduce apprehension. The 4 weeks of VESD focused on the patient’s needs, with support and proposals for alternative solutions where needed; this may have increased self-confidence and reduced uncertainty. Although the primary report regarding anxiety (31) was neutral, a secondary analysis from the GOTVED study demonstrates small-to-moderate negative correlations between confidence in postural balance and anxiety (20). In the current study, the VESD group improved their I-ADL scores directly after the 4-week intervention, but significant differences between that group and the controls did not appear until the follow-up 3 months post-stroke. This might be explained by the positive effect of improved performance on self-esteem, which made it possible for patients in the VESD group to resume their pre-stroke roles and activities (33).
For inclusion in the current study, the patients had to score 50–100 points on the BI on day 2; in cases where the BI was 100, the MoCA had to be < 26 on day 2. In this sample of patients with mild stroke, the median BI was 80 on day 2 post-stroke, indicating that the cohort recovered physically relatively well. On the MoCA, the median for both groups was below the cut-off of < 26; therefore, much of the disability could be due to fatigue and cognitive impairment. Cognitive deficits are a main cause of long-term functional impairment and reduced quality of life after acquired brain injury (13). Interventions that teach individuals to use cognitive strategies during daily activities increase the ability to perform those; also, the use of positive feedback may raise awareness and promote generalization to different activities (34). The VESD support included both feedback and training in the use of such strategies, which may explain the observed greater improvement in the VESD group than in the control group with respect to I-ADL.
A recent review of multiple component interventions, such as cognitive rehabilitation training combined with physiotherapy or occupational therapy, demonstrated a significant effect on cognitive function at < 3 months post-stroke (35), which is in line with the findings of the current study. The MoCA results for the VESD group at 4 weeks post-discharge and 3 months post-stroke were significantly better than those of the controls, which may indicate that the intervention contributed to better awareness and alertness, leading to improved cognitive functioning. Despite having statistically similar cognitive function at discharge, a larger proportion of patients in the control group scored below the cut-off on the MoCA, which may have had an impact on the results.
Since there may be a discrepancy between professionals’ focus on function/rehabilitation goals and the patients’ actual experience of the impact of stroke (33, 36), the current study used 2 different instruments to measure ADL. The primary outcome; the ADL Taxonomy, assessed by a health professional, was supplemented by a secondary outcome; the SIS, a self-report measure, with the aim to capture the patient’s own experience of ability to perform different activities (26). However, both instruments showed a significant difference in I-ADL in favour of VESD at the 3-month follow-up. Since both B-ADL and I-ADL items are included in the SIS domains ADL and Mobility, a sub-analysis was conducted of specific I-ADL items included in both domains, which further confirmed the results.
As in the ADL Taxonomy, only the more demanding tasks in the SIS ADL and Mobility domains challenged the patients in the current study. Perceived disability included stair climbing, outdoor walking, and getting in and out of a car. In the VESD, frequent training during the intervention focused on shopping or doing the laundry (which could involve moving to another floor), and subsequently targeted items in the SIS Mobility domain; this ultimately improved the I-ADL, as well as mobility, in the VESD group. The SIS is a suitable instrument for tracking patient progress, and can be useful for tailoring rehabilitation interventions to target the dimensions of health that are most important to a patient’s overall health and perceived quality of life (37). Changes in scores recorded for both SIS domains in the current study exceeded those reported as clinically important in a previous study (38).
Information provided in the VESD, and the possibility of testing different solutions, makes the situation more understandable and may have reduced the feeling of unfamiliarity with the new life condition. After stroke patients experience an altered capacity to cope, which impacts their life (39); an increased capacity to cope leads to better functioning during B-ADL and I-ADL (33). The supportive intervention provided in the current study may equip individuals with the tools to cope.
The focus of the current study was ADL outcome in patients with mild stroke, therefore resource outcomes, e.g. analysis of length of stay (LOS), were not included. It may be hypothesized that a faster recovery of ability to perform daily activities would reduce care costs, but whether home rehabilitation provided by staff from the stroke unit is cost effective compared with usual outpatient rehabilitation services is yet to be determined. In the main GOTVED study, the median (IQR) LOS of 10 (8-15.5) and 12 (8-16) days in the VESD and control groups, respectively, did not differ statistically significantly (31). Analyses of cost benefits in the main GOTVED study are ongoing in a separate study.
The definition of “early” vs “very early” supported discharge is not clear. Previous publications on ESD report mean LOS between 10 and 50 days for control groups, and 3–5 days shorter for intervention groups (27). At the time of starting data collection in the main GOTVED study, the median LOS of patients with stroke of all severities at the study unit, was 9 days (1). Therefore, based on the actual LOS at the stroke unit the term “very early” was used in the GOTVED study. Since LOS has been successively shortened in past years, the main GOTVED study aimed to study the effects of home rehabilitation delivered during a short period. The goal was not to shorten LOS even more.
A limitation of the current study is that both the primary and secondary measures are subjective. Although the ADL Taxonomy is classified as an observer-based instrument, it still relies on the patient’s report of their ability. The reliability of self-report measures acquired from people with cognitive deficits may be questioned; however, patient-reported outcome measures are, by definition, a direct reflection of the patient’s experience, without interpretation by another person. Therefore, inclusion of this perspective is considered highly important for clinical practice as well as for research (30). The range of interventions delivered to the VESD group have been described in previous publications (31), but the content and intensity of the “usual” rehabilitation programmes offered to the control group is not well documented. Comparing 2 groups that may not have received the same intensity of intervention may therefore be a limitation of the current study.
The strengths of the current study are the randomized design and a relatively large cohort of patients with similar stroke severity. The results of the current analysis may be generalizable to patients with mild stroke symptoms, including cognitive impairment, within the age range at which most stroke cases occur.
Another strength of the current study is that patients with cognitive impairment were included, which is not the case in many studies. The combination of both observer-based and self-report instruments, and the finding that the results from both of these types of instruments moved in the same direction, are also strengths of the current study.
Recommendations for rehabilitation after stroke focus less on full recovery and more on adjustment and adaptation (40). Taule & Råheim (33) studied the experiences of survivors of mild stroke in the context of ESD; they concluded that many patients with mild stroke might not recover fully, despite home rehabilitation; however, support provided by the rehabilitation team may speed up the process of adaptation.
CONCLUSION
These results suggest that supported discharge is beneficial and may enhance the speed of recovery of ADL in the subacute phase for patients with mild stroke. Immediately after the 4-week intervention, the VESD group improved more with respect to I-ADL performance (measured by the ADL Taxonomy) than the control group, and at 3 months post-stroke the difference was significant. The difference in ADL ability, as perceived by the participants according to the SIS ADL and Mobility scores, was also significantly different at 3 months (in favour of the VESD group). The improvements in the control group, referred to primary care according to usual routine, took longer to achieve and at 12 months post-stroke the previous group differences had evened out. The results of the current study suggest that, from a rehabilitation perspective, the recommendation to offer stroke specialized multidisciplinary goal-based rehabilitation in the home setting, after mild stroke, should be maintained.
ACKNOWLEDGEMENTS
This study was funded by grants from the Swedish Science Council (VR2012-3523), the Gothenburg Centre for Person-Centered Care, the Health & Medical Care Committee of the Regional Executive Board Region Västra Götaland, the Axel Linder Foundation, the Foundation of the Swedish Stroke Association, the Local Research and Development Board for Gothenburg and Södra Bohuslän, the Hjalmar Svensson Research Foundation, the Greta and Einar Asker Foundation, the Rune and Ulla Amlöv Foundation, the John and Brit Wennerström Foundation and the Swedish State under an agreement between the Swedish government and county councils (ALF agreement ALFGBG-965653).
REFERENCES
- Riksstroke. The Swedish Stroke Register. Stroke and TIA. Annual reports of data from Riksstroke. [accessed 2023 Aug 4]. Available from: https://www.riksstroke.org/sve/forskning-statistik-och-verksamhetsutveckling/rapporter/arsrapporter/
- Roberts PS, Krishnan S, Burns SP, Ouellette D, Pappadis MR. Inconsistent classification of mild stroke and implications on health services delivery. Arch Phys Med Rehabil 2020; 101: 1243–1259. DOI: 10.1016/j.apmr.2019.12.013
- Abzhandadze T, Buvarp D, Lundgren-Nilsson Å, Sunnerhagen KS. Barriers to cognitive screening in acute stroke units. Sci Rep 2021; 11: 19621. DOI: 10.1038/s41598-021-98853-5
- Faux SG, Arora P, Shiner CT, Thompson-Butel AG, Klein LA. Rehabilitation and education are underutilized for mild stroke and TIA sufferers. Disabil Rehabil 2018; 40: 1480–1484. DOI: 10.1080/09638288.2017.1295473
- Finch E, Foster M, Fleming J, Cruwys T, Williams I, Shah D, et al. Exploring changing needs following minor stroke. Health Soc Care Comm 2020; 28: 347–356. DOI: 10.1111/hsc.12866
- Lodha N, Patel P, Casamento-Moran A, Hays E, Poisson SN, Christou EA. Strength or motor control: what matters in high-functioning stroke? Front Neurol 2019; 9: 1160. DOI: 10.3389/fneur.2018.01160
- Li N, Li J, Gao T, Wang D, Du Y, Zhao X. Gait and balance disorder in patients with transient ischemic attack or minor stroke. Neuropsychiatr Dis Treat 2021; 17: 305–314. DOI: 10.2147/ndt.S289158
- Hasanbarani F, Batalla MAP, Feldman AG, Levin MF. Mild stroke affects pointing movements made in different frames of reference. Neurorehabil Neural Repair 2021; 35: 207–219. DOI: 10.1177/1545968321989348
- Chang WH, Sohn MK, Lee J, Kim DY, Lee SG, Shin YI, et al. Long-term functional outcomes of patients with very mild stroke: does a NIHSS score of 0 mean no disability? An interim analysis of the KOSCO study. Disabil Rehabil 2017; 39: 904–910. DOI: 10.3109/09638288.2016.1170214
- Hamre C, Fure B, Helbostad JL, Wyller TB, Ihle-Hansen H, Vlachos G, et al. Impairments in spatial navigation during walking in patients 70 years or younger with mild stroke. Top Stroke Rehabil 2020; 27: 601–609. DOI: 10.1080/10749357.2020.1755814
- Blomgren C, Jood K, Jern C, Holmegaard L, Redfors P, Blomstrand C, et al. Long-term performance of instrumental activities of daily living (IADL) in young and middle-aged stroke survivors: results from SAHLSIS outcome. Scand J Occup Ther 2018; 25: 119–126. DOI: 10.1080/11038128.2017.1329343
- Edwards DF, Hahn M, Baum C, Dromerick AW. The impact of mild stroke on meaningful activity and life satisfaction. J Stroke Cerebrovasc Dis 2006; 15: 151–157. DOI: 10.1016/j.jstrokecerebrovasdis.2006.04.001
- Bertisch HC, Long C, Langenbahn DM, Rath JF, Diller L, Ashman T. Anxiety as a primary predictor of functional impairment after acquired brain injury: a brief report. Rehabil Psychol 2013; 58: 429–435. DOI: 10.1037/a0034554
- Rafsten L, Danielsson A, Sunnerhagen KS. Anxiety after stroke: a systematic review and meta-analysis. J Rehabil Med 2018; 50: 769–778. DOI: 10.2340/16501977-2384
- Green TL, King KM. The trajectory of minor stroke recovery for men and their female spousal caregivers: literature review. J Adv Nurs 2007; 58: 517–531. DOI: 10.1111/j.1365-2648.2007.04321.x
- Swedish National Board of Health and Welfare. National Guidelines of Stroke Care 2020 [cited 2023 June 16]. Available from: https://www.socialstyrelsen.se/kunskapsstod-och-regler/regler-och-riktlinjer/nationella-riktlinjer/riktlinjer-och-utvarderingar/stroke/
- Lou S, Carstensen K, Møldrup M, Shahla S, Zakharia E, Nielsen CP. Early supported discharge following mild stroke: a qualitative study of patients’ and their partners’ experiences of rehabilitation at home. Scand J Caring Sci 2017; 31: 302–311. DOI: 10.1111/scs.12347
- Nordin Å, Sunnerhagen KS, Axelsson ÅB. Patients’ expectations of coming home with Very Early Supported Discharge and home rehabilitation after stroke – an interview study. BMC Neurol 2015; 15: 235. DOI:10.1186/s12883-015-0492-0
- Sunnerhagen KS, Danielsson A, Rafsten L, Björkdahl A, Axelsson ÅB, Nordin Å, et al. Gothenburg very early supported discharge study (GOTVED) NCT01622205: a block randomized trial with superiority design of very early supported discharge for patients with stroke. BMC Neurol 2013; 13: 66. DOI: 10.1186/1471-2377-13-66
- Rafsten L, Danielsson A, Sunnerhagen KS. Self-perceived postural balance correlates with postural balance and anxiety during the first year after stroke: a part of the randomized controlled GOTVED study. BMC Neurol 2020; 20: 410. DOI: 10.1186/s12883-020-01982-z
- Schulz K, Altman D, Mohed D; CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. Ann Intern Med 2010; 152: 726-732. DOI: 10.7326/0003-4819-152-11-201006010-00232
- Goldstein LB, Bertels C, Davis JN. Interrater reliability of the NIH stroke scale. Arch Neurol 1989; 46: 660–662. DOI: 10.1001/archneur.1989.00520420080026
- Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J 1965; 14: 61–65.
- Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005; 53: 695–699. DOI: 10.1111/j.1532-5415.2005.53221.x
- Sonn U, Törnquist K, Svensson E. The ADL Taxonomy – from individual categorical data to ordinal categorical data. Scand J Occup Ther 1999; 6: 11–20. DOI: 10.1080/110381299443807
- Duncan PW, Wallace D, Lai SM, Johnson D, Embretson S, Laster LJ. The Stroke Impact Scale Version 2.0. Stroke 1999; 30: 2131–2140. DOI: 10.1161/01.STR.30.10.2131
- Langhorne P, Baylan S. Early supported discharge services for people with acute stroke. Cochrane DB Syst Rev 2017; 7: CD000443. DOI: 10.1002/14651858.CD000443.pub4
- Bonita R, Beaglehole R. Recovery of motor function after stroke. Stroke 1988; 19: 1497–1500. DOI: 10.1161/01.str.19.12.1497
- Fugl-Meyer AR, Jääskö L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand J Rehabil Med 1975; 7: 13–31.
- Reeves M, Lisabeth L, Williams L, Katzan I, Kapral M, Deutsch A, et al. Patient-Reported Outcome Measures (PROMs) for acute stroke: rationale, methods and future directions. Stroke 2018; 49: 1549–1556. DOI: 10.1161/STROKEAHA.117.018The912
- Rafsten L, Danielsson A, Nordin Å, Björkdahl A, Lundgren Nilsson Å, Larsson M, et al. Gothenburg Very Early Supported Discharge study (GOTVED): a randomised controlled trial investigating anxiety and overall disability in the first year after stroke. BMC Neurol 2019; 19: 277. DOI: 10.1186/s12883-019-1503-3
- Rafsten L, Sunnerhagen KS. Patient-centered goal setting in very early supported discharge with continued rehabilitation after stroke. Disabil Rehabil 2022: Nov 8; 1–6. [Online ahead of print] DOI: 10.1080/09638288.2022.2141357
- Taule T, Råheim M. Life changed existentially: a qualitative study of experiences at 6–8 months after mild stroke. Disabil Rehabil 2014; 36: 2107–2119. DOI: 10.3109/09638288.2014.904448
- Adamit T, Shames J, Rand D. Effectiveness of the Functional and Cognitive Occupational Therapy (FaCoT) intervention for improving daily functioning and participation of individuals with mild stroke: a randomized controlled trial. Int J Environ Res Public Health 2021; 18: 7988. DOI: 10.3390/ijerph18157988
- O’Donoghue M, Leahy S, Boland P, Galvin R, McManus J, Hayes S. Rehabilitation of cognitive deficits poststroke: systematic review and meta-analysis of randomized controlled trials. Stroke 2022; 53: 1700–1710. DOI: 10.1161/STROKEAHA.121.034218
- Tistad M, Ytterberg C, Tham K, von Koch L. Poor concurrence between disabilities as described by patients and established assessment tools three months after stroke: a mixed methods approach. J Neurol Sci 2012; 313: 160–166. DOI: 10.1016/j.jns.2011.08.038
- Richardson M, Campbell N, Allen L, Meyer M, Teasell R. The stroke impact scale: performance as a quality of life measure in a community-based stroke rehabilitation setting. Disabil Rehabil 2016; 38: 1425–1430. DOI: 10.3109/09638288.2015.1102337
- Lin KC, Fu T, Wu CY, Wang YH, Liu JS, Hsieh CJ, et al. Minimal detectable change and clinically important difference of the Stroke Impact Scale in stroke patients. Neurorehabil Neural Repair 2010; 24: 486–492. DOI: 10.1177/1545968309356295
- Winkel A, Ekdahl C, Gard G. Early discharge to therapy-based rehabilitation at home in patients with stroke: a systematic review. Phys Ther Rev 2008; 13: 167–187. DOI: 10.1179/174328808X252091
- Donnellan C, Martins A, Conlon A, Coughlan T, O’Neill D, Collins DR. Mapping patients’ experiences after stroke onto a patient-focused intervention framework. Disabil Rehabil 2013; 35: 483–491. DOI: 10.3109/09638288.2012.702844