Key words: physical activity; exercise; para-sport; sports for people with disabilities; cerebral palsy; physical fitness; surveys and questionnaires.
Accepted Dec 6, 2021; Epub ahead of print Jan 12, 2022
J Rehabil Med 2022; 54: jrm00273
DOI: 10.2340/jrm.v53.1393
Correspondence address: Marietta van der Linden, Centre for Health, Activity and Rehabilitation Research, Queen Margaret University Edinburgh, Musselburgh, EH21 6UU, UK. E-mail: mvanderlinden@qmu.ac.uk
LAY ABSTRACT
Frame Running (RaceRunning) allows people with moderate-to-severe walking difficulties to walk or run independently using a 3-wheeled frame with a saddle and handlebars. In this study 115 Frame Running athletes living in the UK, Sweden or the Netherlands and aged 5 years or over (or their parents) completed a survey about taking part in Frame Running. More than half used a wheelchair or walker for distances over 50 m. Most felt that Frame Running stretched their muscles and increased their self-confidence. Four athletes perceived extreme fatigue and 17 reported sore muscles after training. Approximately half of the athletes reported that they were less out of breath during mobility tasks (walking, standing) and two thirds reported better functional mobility since they had started Frame Running. Injuries lasting more than 4 weeks were reported by 4 athletes. We conclude that Frame Running is a safe activity with the potential to improve physical fitness, functional mobility, and self-confidence.
INTRODUCTION
It is well established that the majority of children and adults with long-term neurological conditions affecting mobility have lower levels of physical activity compared with the general population (e.g. 1–3). This is of concern, as there is evidence that people with a long-term neurological condition affecting mobility also have a higher risk of developing cardiometabolic and cardiovascular diseases (4–5), worse mental health (6–7) and increased fatigue (7) compared with the general population.
In the last decade there has been increasing evidence that exercise interventions positively impact people with disabilities in terms of mobility, cardiovascular endurance, muscular strength, balance and cognitive function (8). In addition, studies have highlighted the beneficial effects of exercise for people with disabilities on social interactions (9) and psychosocial outcomes (10–11).
However, a recent Cochrane systematic review (12) highlighted the lack of exercise intervention studies involving people who are more severely affected by cerebral palsy (CP) and studies investigating the long-term impact of these interventions. These activities need to be adapted to enable people with moderate-to-severe walking impairments to engage in a sustainable physical activity, and need to be safe, relatively easily accessible and enjoyable (10). Moreover, such activities should also be sufficiently demanding to promote improvements in physical fitness (13).
Frame Running, formerly known as RaceRunning, allows people with moderate-to-severe walking impairments to propel themselves using a 3-wheeled frame with a saddle, a chest plate for support, and handlebars for steering (https://cpisra.org/framerunning/). A study into the impact of impairments such as spasticity on Frame Running performance showed that even those with high levels of spasticity and severe knee contractures can compete internationally (14). This study with 31 athletes also reported that the majority of athletes had a diagnosis of CP and hypertonia, and that most were unable to walk independently (Gross Motor Function Classification System level III, n=10; level IV n = 11; level V, n = 2).
Evidence suggests that Frame Running can enable individuals with CP to engage in moderate-to-vigorous physical activity, with sufficient intensity to promote measurable training adaptations. Bolster et al. (15) found that adolescents who are moderately-to-severely affected by CP can reach a close-to-maximum heart rate (> 180 bpm) during the 6-min Frame Running test. Similar high-intensity exercise levels (mean heart rate > 65% of age-related maximum heart rate during training) in young people with CP were shown in a 12-week Frame Running training intervention by Hjalmarsson et al. (16). This study also demonstrated improved cardiorespiratory endurance and hypertrophy of the gastrocnemius.
These results show the potential for Frame Running training to impact positively on the physical fitness of individuals with moderate-to-severe walking impairment. However, more evidence is required to explore the factors that may influence the sustainability of Frame Running training, such as injury risk and the athlete-perceived impact of Frame Running participation on physical outcomes as well as psychosocial outcomes such as self-confidence and interpersonal relationships (17). Understanding of athlete-perceived benefits and adverse effects of Frame Running is crucial for those considering undertaking or promoting Frame Running. Finally, the knowledge of Frame Running athlete population demographics and their Frame Running participation characteristics can also inform future experimental research, such as randomized controlled trials or longitudinal cohort studies.
Therefore, this study used a survey design and had the following aims. The first was to describe the Frame Running athlete population demographics and participation characteristics. The second was to investigate the athlete-perceived adverse effects as well the impact of taking part in Frame Running on aspects of physical fitness, functional mobility and psychosocial outcomes. Finally, we aimed to investigate whether the athlete-perceived impact of Frame Running on these outcomes is associated with mobility level and age.
METHODS
Participants
In this cross-sectional study, athletes aged 5 years and over with any underlying health condition who participated in Frame Running as part of a club or their national sports organization were eligible to take part in the survey. Participants were recruited through Frame Running clubs or through their Frame Running organizations in the UK, Sweden and the Netherlands. A link to the online survey (www.onlinesurveys.ac.uk) in the participants’ native language was distributed to Frame Running athletes via their coaches. In the UK and Sweden paper copies were also distributed to coaches who preferred this.
This anonymous survey was completed by the athlete independently or, if necessary, with help from a parent/carer or by the parent/carer (proxy report). The completion of the survey implied consent. The study protocol was approved by the Research Ethics Committee of Queen Margaret University, Edinburgh, UK.
Survey
The questions in the survey were based on evidence from quantitative and qualitative studies on the impact of physical activity exercise for people with impaired balance and gait (12; 18–20). The constructs examined in the survey cover the main domains of the International Classification of Functioning, Disability and Health (ICF) (21): body function & structures (e.g. muscle tone), activity (e.g. functional mobility), participation (e.g. interpersonal relationships) and personal factors (e.g. self-confidence). The questionnaire consisted of 5 types of question (Appendix SI). Questions 1–5 aimed to collect demographic data, such as age, sex, country of residence, self-reported functional mobility using the Functional Mobility Scale over 50 m (FMS50) (22) and information on who completed the survey. Secondly, the questionnaire collected information on the athlete’s Frame Running participation characteristics, e.g. how often respondents took part in Frame Running, where they did this and whether they participate in competitions (Q6–9). The questionnaire also included a question (Q10) on whether athletes feel out breath when taking part in Frame Running as a proxy for training intensity. It was assumed that feeling out of breath indicates moderate-to-vigorous physical activity, which has the potential to improve cardiovascular endurance (13).
Athlete-perceived adverse effects were explored in questions 11 (pain), 18 (injuries) and 19 (fatigue). Finally, we included questions on the athlete-perceived impact of taking part in Frame Running, either immediately (Q20–24) or after participation over a period of 3 months or more (Q12–17). Based on evidence from quantitative and qualitative studies on the effects of physical activity and exercise for people with impaired balance and gait (12; 18–20), it was decided to include questions addressing the following constructs: physical fitness (endurance and flexibility), functional mobility, muscle tightness, interpersonal relationships, sleep quality, enjoyment, and self-confidence. These constructs cover the main domains of the ICF (21), namely body function & structures (e.g. muscle tightness), activity (e.g. functional mobility), participation (e.g. interpersonal relationships). A question on self-confidence (personal factors) was added to the surveys in Dutch and English.
The questionnaire consisted mostly of multiple-choice questions, with the possibility for the respondents to explain their answer further in free text. The survey questions were reviewed for relevance and clarity by 2 young adult Frame Running athletes and 1 parent of an athlete and recommended changes were made before the questionnaire was distributed.
Data analysis
Descriptive statistics, such as medians and interquartile (IQR) ranges, for age and measures of frequency for the other questions were used to report the results of the survey sample. Percentages were calculated from the number of respondents answering that question. Fisher’s exact tests were used to analyse the association between functional mobility and age and the athlete-perceived impact of Frame Running on physical fitness and psychosocial outcomes. To analyse the relationship between perceived impact and functional mobility, we grouped those with FMS50 scores 5 and 6 together to form a group of independent walkers and grouped those with FMS50 scores 1–4 to form a group of respondents who used walking aids or a wheelchair. Children and adolescents (<18 years) were also grouped together and compared with adults (18 years and over) to analyse the influence of age.
A p-value <0.05 was regarded as statistically significant. Statistical analysis was performed using MS Excel and IBM SPSS v23.
RESULTS
Demographics
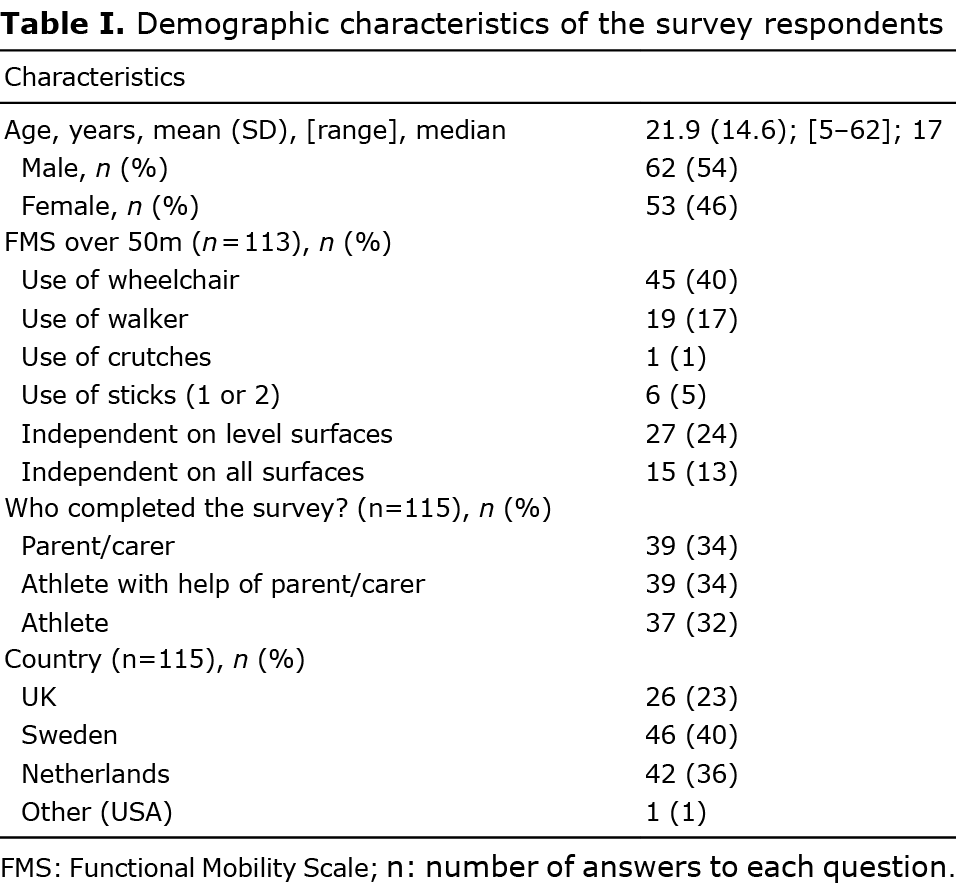
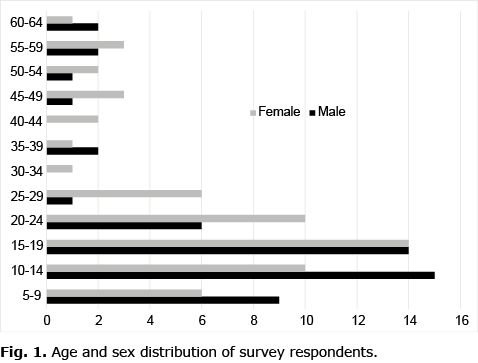
The demographics of the 115 participants are shown in Table I. Slightly more males than females took part (54% vs 46%) in the survey and the median age was 17 years (range 5–62) (Fig. 1). The majority of respondents lived in Sweden (40%) or the Netherlands (36%), and over half (57%) used a wheelchair or walker for distances of 50 m or more. The survey was open to all Frame Running athletes and we did not record the health condition of the respondents. The free-text answers showed that at least 12 participants did not have CP. Other conditions that were stated were: “progressive health condition” (n = 3), multiple sclerosis (MS) (n = 3), musculoskeletal condition (n = 2), neuromyelitis optica (n = 1), post-stroke (n = 1), bronchial asthma (n = 1) and autism (n = 1).
Participation characteristics
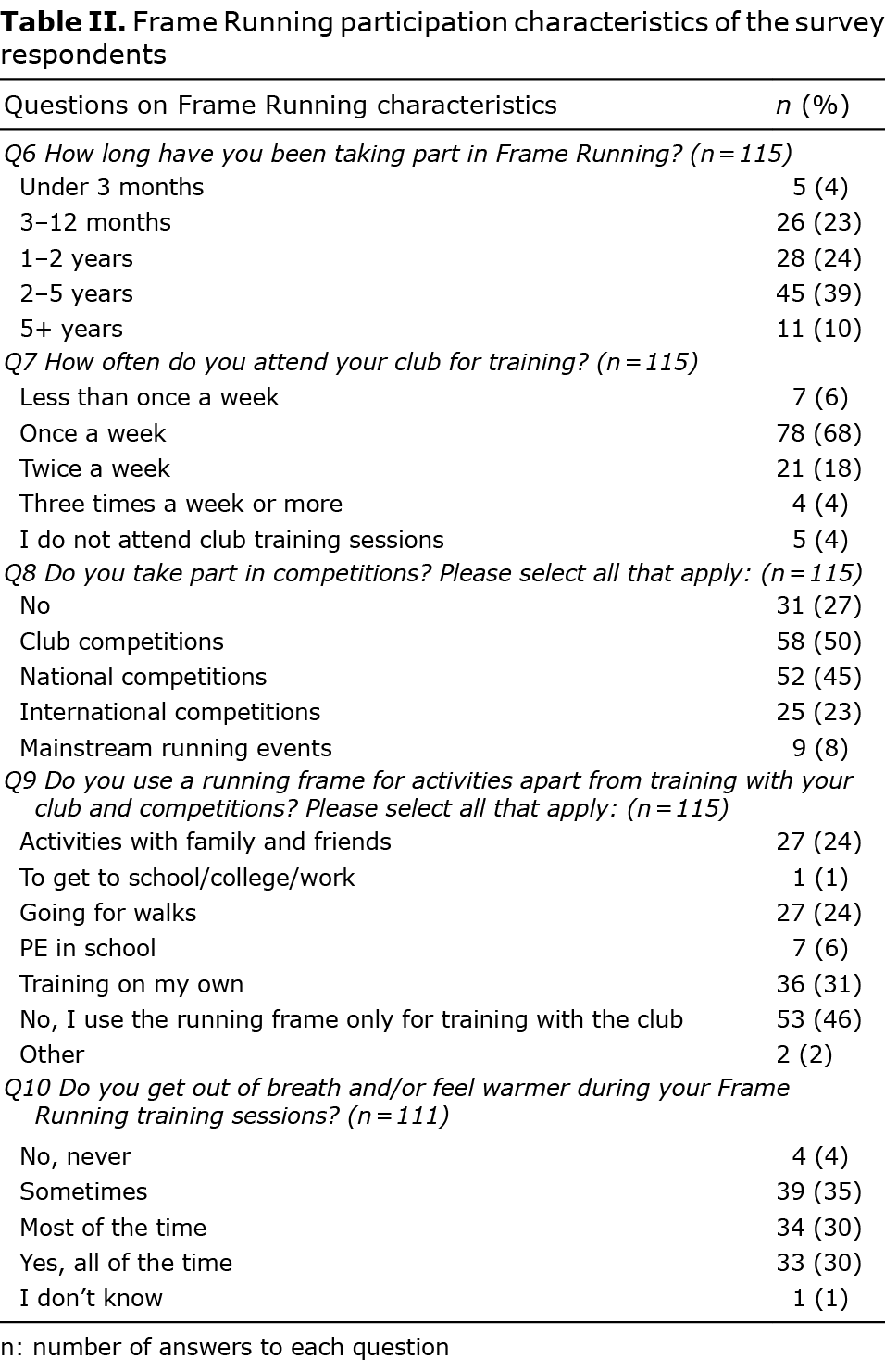
Table II shows the Frame Running participation characteristics. All except 5 respondents had been participating in Frame Running for more than 3 months and 11 respondents for more than 5 years at the time of the study. The most commonly reported Frame Running training frequency with a club was once a week (68%). However, respondents also reported that they used the running frame in other settings, such as walks with friends and family, and many (73%) stated they had taken part in at least 1 Frame Running competition or mainstream running event. With regard to the potential of Frame Running to improve cardiovascular fitness, nearly all respondents reported experiencing signs of physical exertion during a training session all the time (30%), most of the time (30%), or some of the time (35%).
Immediate impact of Frame Running participation
The perceived immediate effects of taking part in Frame Running are shown in Table III. The majority of respondents (87%) felt that Frame Running helped them to stretch their muscles. Other benefits noted by most were enjoyment (95%) and making friends (90%) and 93% reported increased self-confidence.
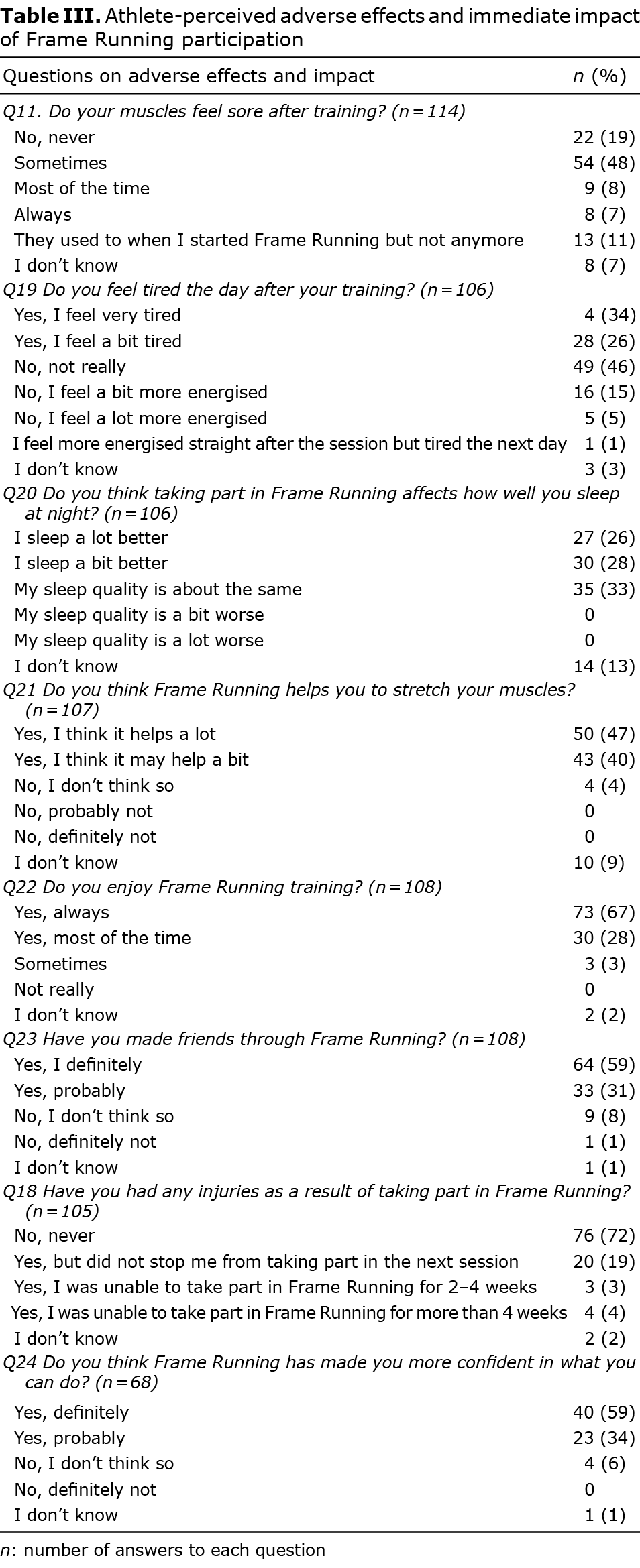
Fatigue the day after the session was not an issue for the majority of respondents and only 4 athletes perceived severe fatigue. Injuries were reported by approximately a quarter of the respondents, with only 4 reporting an injury that lasted more than 4 weeks. The free text showed among these 4 respondents, 2 reported a fracture (1 thumb and 1 clavicle) and 1 sprained an ankle, all as a result of a fall when using the running frame, whilst the fourth reported saddle soreness.
Table IV presents information on the perceived change in physical fitness and functional mobility after taking part in Frame Running sessions for 3 months or more. Compared with when they first started Frame Running, more than half of the respondents felt they were less out of breath when using the frame going at the same speed. However, just under half reported being less out of breath during their usual functional mobility-related activities. Nevertheless, the majority of respondents felt that their walking/standing/transferring ability was a bit or a lot better. Three respondents found it a bit more difficult to walk or transfer since they started participating in Frame Running, but all 3 commented that this was not likely due to taking part in Frame Running, but rather due to their underlying condition.
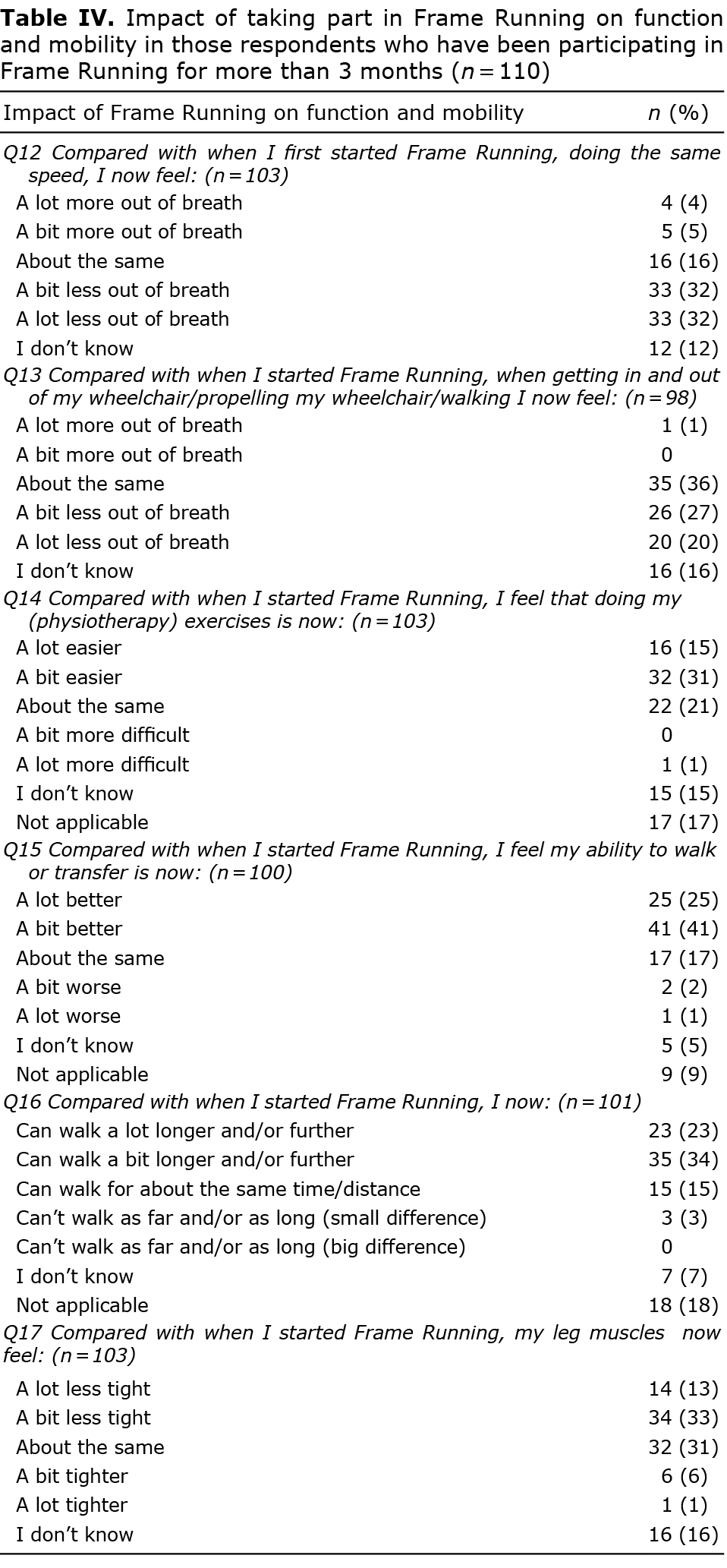
Muscle tightness since taking up Frame Running was perceived to be less by just under half of the respondents, but 7 perceived that this had increased either a bit or a lot. Of these 7, 1 individual reported that they had low muscle tone to start with, so an increase was regarded as positive, while another added: “A lot tighter/more tense, doesn’t only depend on the Frame Running, I’ve increased my training dose of other activities as well”.
Effect of age and mobility level on perceived impact of Frame Running participation
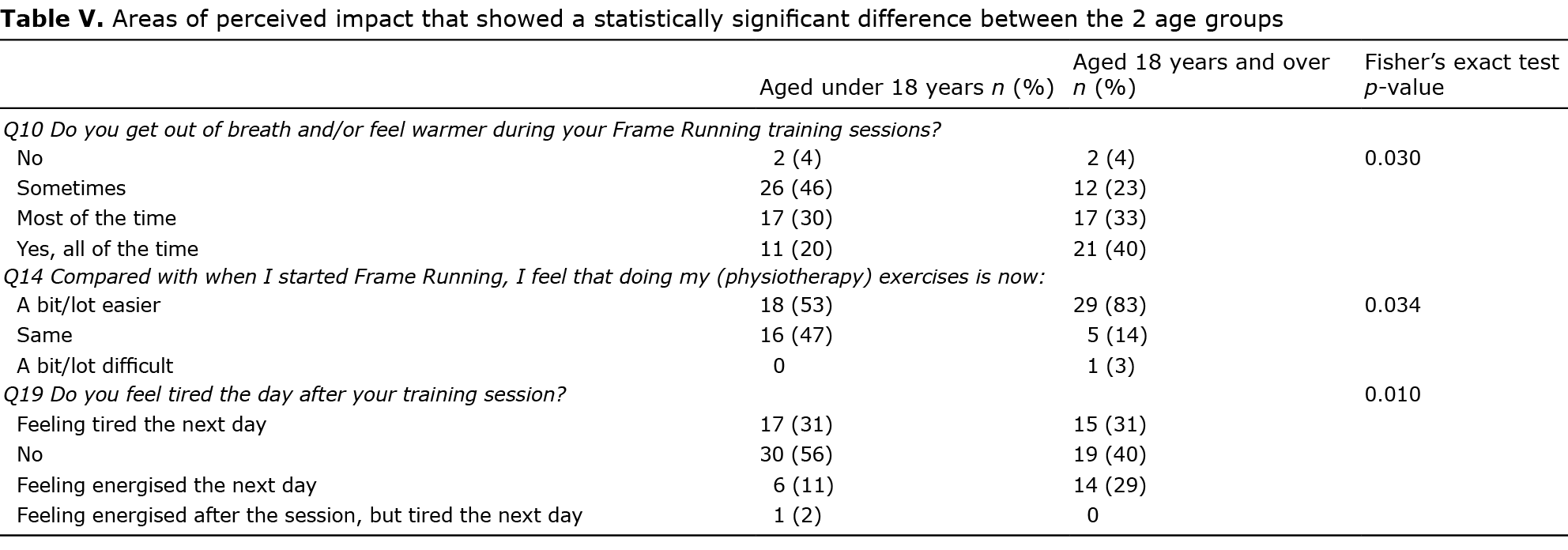
Most questions showed no difference in the answers between the 2 age groups or between the 2 mobility groups (Appendix SII). The areas of perceived impact that differed significantly between age groups and levels of mobility are presented in Tables V (age) and VI (functional mobility). Adults were significantly more likely to report feeling out of breath during a training session (p = 0.03) and feeling more energised the day after training (p = 0.01) compared to those under 18. Adults also responded more often that physiotherapy exercises felt easier since they had started taking part in Frame Running (p = 0.034) compared with the younger age group (Table V). Those using walking aids and/or a wheelchair were more likely to report experiencing muscle soreness (p = 0.007) and increased fatigue the day after the training session (p = 0.026) compared with those able to walk independently. However, they also reported more often that their muscles felt less tight since they started regular Frame Running compared with independent walkers (p = 0.013) (Table VI).

DISCUSSION
This study aimed to describe the Frame Running athlete population and participation characteristics in 3 European countries as well as the athlete-perceived impact of this activity on aspects of physical fitness, functional mobility and psychosocial outcomes. The results indicated most respondents perceived Frame Running to be enjoyable and safe and that their participation resulted in a variety of benefits.
The respondents in the survey included females and males in similar proportions, and children aged 5 years up to adults in their 60s. Although, currently, the majority of Frame Running athletes have CP, this survey’s inclusion criteria were deliberately broad to include anyone taking part in Frame Running as part of a club or national sports organization, in order to provide insight into the Frame Running athlete population in general. The free-text answers showed that the survey sample also included people recovering from a stroke and those with progressive conditions, such as multiple sclerosis. Both of these populations are known to have a high risk of falling (23, 24) and Frame Running thus allows a safe alternative to independent walking and running.
The results of the current survey showed that most participants thought that Frame Running enabled them to exert themselves physically, which supports observations from previous studies (15, 16). This potential of Frame Running to enable moderate-to-vigorous physical activity and thereby improve cardiovascular fitness is important, as this level of physical exertion is difficult to achieve during other sports for many individuals with severe mobility impairments. Indeed, approximately half of the respondents reported feeling less out breath during their functional mobility activities such as transfers, wheelchair propulsion and walking since they started Frame Running. Although this benefit of improved cardiorespiratory fitness was subjective and not confirmed by objective measurement of fitness in an experimental study, this result should be regarded as relevant. Firstly, as it is likely that the experience reflects an adequate improvement in fitness and, secondly, perceived fitness has been shown to have a strong connection to positive personality and mood variables (25). Similarly, the positive findings of the survey with regard to self-confidence, making friends and enjoyment are likely to increase the sustainability of this activity (26).
Another interesting finding is that many respondents perceived their muscles to be “less tight” both during Frame Running and since they started taking part in Frame Running. The phrase “less tight” was used to include restrictions in both passive and dynamic range of motion (spasticity). Traditionally, many clinicians were concerned that increased physical effort would increase spasticity in muscles and thereby exacerbate joint stiffness and contractures. Although more rigorous research is needed in this area, current evidence suggests that muscles can be strengthened effectively in people with CP without reducing range of motion or exacerbating spasticity (27). In a recent study on the impact of a 12-week Frame Running training programme, Hjalmarsson et al. (16) also reported no change in spasticity levels, but found a decreased dorsiflexion range of motion (ROM) in the most affected leg. Although this decrease was relatively small and may be linked to the muscle hypertrophy as a result of training, this result and our finding that 7 (7%) individuals reported an increase in muscle tightness indicate that passive range of motion needs to be monitored in athletes who may be prone to contractures (28). These results also advocate, as for most other physical activities, a role for stretching as part of the training session.
Regarding safety, the survey showed that, in this mostly recreational sample, injuries lasting more than 4 weeks were less common (4%) compared with those who took part in other para-sports at a recreational level (29).
The main limitation of this study is that the data were collected through a questionnaire with unknown validity and reliability, as opposed to an experimental design with objective measures of aerobic fitness, functional mobility, spasticity and range of motion or validated questionnaires for outcomes such as self-confidence, fatigue and interpersonal relationships. This, and the fact that we did not adopt a pre-post design or include a control group, may have resulted in an overestimation of the positive impact of Frame Running compared with an experimental design using standardized validated outcomes. Another limitation is that we did not record the health condition of the respondents. Although globally, the majority of those taking part in Frame Running are diagnosed with CP, it was evident from some of the free-text responses that several respondents had different health conditions. This mix of health conditions, which included progressive conditions, may have affected the responses to the questions regarding changes in functional mobility over time and those on fatigue. On the other hand, the broad inclusion criteria also increase the generalizability of our findings. Finally, we did not collect data from those athletes who stopped taking part in Frame Running. Nearly all respondents (95%) reported to have taken part in Frame Running for 3 months or more, indicating that this was a sample who had persisted with it and were thus more likely to report a positive impact from Frame Running.
However, we believe that the strengths of this study lie in its sample size, the range of athlete-perceived outcomes that were explored, and that people from 3 different countries completed the survey. The athlete-perceived impact of an adapted physical activity, as presented in this study, is rarely reported, but is of high importance for decision making by a wide variety of stakeholders, including potential Frame Running athletes and their families.
The focus of this survey was on one particular adapted physical activity, namely Frame Running. However, the design and results of this survey may also contribute to the understanding of athlete-perceived adverse effects and benefits of participation in other para-sports, especially those that promote inclusion of athletes with high support needs.
In conclusion, this survey has demonstrated, for the first time, that taking part in Frame Running is feasible, safe and enjoyable for individuals with a wide range of abilities and ages. People take part in Frame Running as part of a club with specified training sessions, but many also train on their own or join family walks using their frame. Many also take part in competitions including mainstream road running events, club championships and World Para Athletics events. Participation in Frame Running was perceived to lead to a variety of positive effects on physical fitness, functional mobility and psychosocial outcomes. A small number of athletes reported an increase in muscle tightness and this, although relatively rare, should be monitored carefully. Furthermore, it is recommended to include warming up exercises and stretching as part of Frame Running training sessions (30).
We believe that the findings of this study provide support for stakeholders, such as medical and allied health professionals, (para) athletics coaches, physical education teachers and potential athletes and their families who are considering undertaking or promoting Frame Running. Researchers designing studies investigating the impact of Frame Running participation with experimental designs and objective performance measures need to consider the findings of this survey, including that the majority of athletes are unable to walk independently and that most only train once a week.
The authors have no conflicts of interest to declare
REFERENCES
- English C, Manns PJ, Tucak C, Bernhardt J. Physical activity and sedentary behaviors in people with stroke living in the community: a systematic review. Phys Ther 2014; 94:185–196.
- Casey B, Coote S, Galvin R, Donnelly A. Objective physical activity levels in people with multiple sclerosis: meta-analysis. Scand J Med Sci Sports 2018; 28:1960–1969.
- Carlon SL, Taylor NF, Dodd KJ, Shields N. Differences in habitual physical activity levels of young people with cerebral palsy and their typically developing peers: a systematic review. Disabil Rehabil 2013; 35: 647–655.
- Ryan JM, Crowley VE, Hensey O, Broderick JM, McGahey A, Gormley J. Habitual physical activity and cardiometabolic risk factors in adults with cerebral palsy. Res Dev Disabil 2014; 35: 1995–2002.
- Ryan JM, Hensey O, McLoughlin B, Lyons A, Gormley J. Reduced moderate-to-vigorous physical activity and increased sedentary behavior are associated with elevated blood pressure values in children with cerebral palsy. Phys Ther 2014; 94: 1144–1153.
- Marrie RA, Reingold S, Cohen J, Stuve O, Trojano M, Soelberg Sorensen P, et al. The incidence and prevalence of psychiatric disorders in multiple sclerosis: a systematic review. Mult Scler 2015; 21: 305–317.
- Jacobson DN, Löwing K, Tedroff K. Health-related quality of life, pain, and fatigue in young adults with cerebral palsy. Dev Med Child Neurol 2020; 62: 372–378.
- Lai B, Young H, Bickel CS, Motl RW, Rimmer JH. Current trends in exercise intervention research, technology, and behavioral change strategies for people with disabilities: a scoping review. Am J Phys Med Rehabil 2017; 96: 748–761.
- George CL, Oriel KN, Blatt PJ, Marchese V. Impact of a community-based exercise program on children and adolescents with disabilities. J Allied Health 2011; 40: e55-e60.
- Bloemen MA, Backx FJ, Takken T, Wittink H, Benner J, Mollema J, et al. Factors associated with physical activity in children and adolescents with a physical disability: a systematic review. Dev Med Child Neurol 2015; 57: 137–148.
- Slaman J, van den Berg-Emons HJG, van Meeteren J, Twisk J, van Markus F, Stam HJ, et al. A lifestyle intervention improves fatigue, mental health and social support among adolescents and young adults with cerebral palsy: focus on mediating effects. Clin Rehabil 2015; 29: 717–727.
- Ryan JM, Cassidy EE, Noorduyn SG, O’Connell NE. Exercise interventions for cerebral palsy. Cochrane Database Syst Rev 2017; 6: CD011660.
- Verschuren O, Peterson MD, Balemans AC, Hurvitz EA. Exercise and physical activity recommendations for people with cerebral palsy. Dev Med Child Neurol 2016; 58: 798–808.
- van der Linden ML, Jahed S, Tennant N, Verheul MHG. The influence of lower limb impairments on Frame Running performance in athletes with hypertonia, ataxia or athetosis. Gait Posture 2018; 61: 362–367.
- Bolster EA, Dallmeijer AJ, de Wolf GS, Versteegt M, Schie PE. Reliability and construct validity of the 6-Minute Racerunner Test in children and youth with cerebral palsy, GMFCS Levels III and IV. Phys Occup Ther Pediatr 2017; 37: 210–221.
- Hjalmarsson E, Fernandez-Gonzalo R, Lidbeck C, Palmcrantz A, Jia A, Kvist O, et al. Frame Running training improves stamina and promotes skeletal muscle hypertrophy in young individuals with cerebral palsy. BMC Musculoskelet Disord 2020; 21: 193.
- Reedman SE, Boyd RN, Trost SG, Elliott C, Sakzewski L. Efficacy of participation-focused therapy on performance of physical activity participation goals and habitual physical activity in children with cerebral palsy: a randomized controlled trial. Arch Phys Med Rehabil 2019; 100: 676–686.
- Lauruschkus K, Nordmark E, Hallström I. “It’s fun, but …” Children with cerebral palsy and their experiences of participation in physical activities. Disabil Rehabil 2015; 37: 283–289.
- Al-Sharman A, Khalil H, El-Salem K, Aldughmi M, Aburub A. The effects of aerobic exercise on sleep quality measures and sleep-related biomarkers in individuals with Multiple Sclerosis: a pilot randomised controlled trial. NeuroRehabilitation 2019; 45: 107–115.
- Edwards T, Pilutti LA. The effect of exercise training in adults with multiple sclerosis with severe mobility disability: a systematic review and future research directions. Mult Scler Relat Disord 2017; 16: 31–39.
- World Health Organization. (2001). International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization. [accessed January 18, 2022] Available from: https://apps.who.int/iris/handle/10665/42407.
- Graham HK, Harvey A, Rodda J, Nattrass GR, Pirpiris M. The Functional Mobility Scale (FMS). J Pediatr Orthop 2004; 24: 514–520.
- Nilsagård Y, Lundholm C, Denison E, Gunnarsson LG. Predicting accidental falls in people with multiple sclerosis – a longitudinal study. Clin Rehabil 2009; 23: 259–269.
- Yates JS, Lai SM, Duncan PW, Studenski S. Falls in community-dwelling stroke survivors: an accumulated impairments model. J Rehabil Res Dev 2002; 39: 385–394.
- Plante TG, Lantis A, Checa G. The Influence of perceived versus aerobic fitness on psychological health and physiological stress responsivity. Int J Stress Manag 1998; 5: 141–156.
- Shimmell LJ, Gorter JW, Jackson D, Wright M, Galuppi B. “It’s the participation that motivates him”: physical activity experiences of youth with cerebral palsy and their parents. Phys Occup Ther Pediatr 2013; 33: 405–420.
- Dodd KJ, Taylor NF, Damiano DL. A systematic review of the effectiveness of strength-training programs for people with cerebral palsy. Arch Phys Med Rehabil 2002; 83: 1157–1164.
- Steele KM, Damiano DL, Eek MN, Unger M, Delp SL. Characteristics associated with improved knee extension after strength training for individuals with cerebral palsy and crouch gait. J Pediatr Rehabil Med 2012; 5: 99–106.
- Tuakli-Wosornu YA, Mashkovskiy E, Ottesen T, Gentry M, Jensen D, Webborn N. Acute and chronic musculoskeletal injury in para sport: a critical review. Phys Med Rehabil Clin N Am 2018; 29: 205–243.
- Frame Running coaches manual, 2017. [accessed January 18, 2022] Available from: https://framerunning.org/media/1133/Frame Running-coaches-manual.pdf.