ORIGINAL REPORT
EXERCISE- AND EDUCATION-BASED PREHABILITATION BEFORE TOTAL KNEE ARTHROPLASTY: A PILOT STUDY
Pascale GRÄNICHER, MSc1,2, Loes MULDER, MSc1,3, Ton LENSSEN, PhD1,3, Sandro F. FUCENTESE, MD4, Jaap SWANENBURG, PhD5–7, Rob DE BIE, PhD1 and Johannes SCHERR, MD2
From the 1Department of Epidemiology, CAPHRI School for Public Health and Primary Care, Maastricht University, Maastricht, The Netherlands, 2University Center for Prevention and Sports Medicine, Balgrist University Hospital, University of Zurich, Zurich, Switzerland, 3Maastricht University MUMC+ Maastricht, The Netherlands, 4Department of Orthopedic Surgery, Balgrist University Hospital, University of Zurich, Zurich, Switzerland, 5Integrative Spinal Research ISR, Department of Chiropractic Medicine, Balgrist University Hospital, Zurich, 6UZH Space Hub, Air Force Center, Dübendorf, Switzerland and 7Institute of Anatomy, Faculty of Medicine, University of Zurich, Zurich, Switzerland
Objective: To determine the feasibility and estimates of effects of a supervised exercise- and education-based prehabilitation programme aiming to improve knee functioning compared with usual care in patients awaiting total knee arthroplasty.
Design: A randomized controlled pilot study.
Subjects: Patients receiving primary, unilateral total knee arthroplasty.
Methods: Patients randomized to the intervention group participated in a personalized 4–8-week prehabilitation programme before surgery. Feasibility of the intervention and self-reported knee functioning, pain, physical performance and hospital stay were assessed at baseline, immediately preoperatively, 6 and 12 weeks after surgery.
Results: Twenty patients (mean age 72.7±5.95 years) were enrolled in this study. The personalized prehabilitation programme was found to be feasible and safe, with an exercise adherence of 90%. Significant medium interaction effects between groups and over time favouring prehabilitation were reported for the sport subscale of the Knee Osteoarthritis Outcome Score (F(3/54) = 2.895, p = 0.043, η² = 0.139) and Tegner Activity Scale (F(2.2/39.1) = 3.20, p = 0.048, η² = 0.151).
Conclusion: The absence of adverse events and high adherence to the programme, coupled with beneficial changes shown in the intervention group, support the conduct of a full-scale trial investigating the effectiveness of prehabilitation.
LAY ABSTRACT
Physical and mental preparation before major surgery, known as prehabilitation, can reduce the risk factors for prolonged recovery time and allow a faster return to daily activities. This pilot study investigated whether a personalized programme based on exercise and education over a period of 4–8 weeks is acceptable and tolerable for patients with severe knee osteoarthritis who are scheduled for total knee replacement surgery. This study also investigated how this additional stage of the patient journey fits into existing clinical routines and how it affects pain and physical activities. The results show that this programme is safe and well accepted by patients, and that it can enable a return to more demanding physical activities after total knee arthroplasty compared with usual care. It is important to inform and educate patients early about the potential benefits of preoperative preparation to ensure high participation rates and sustainable implementation into clinical practice.
Key words: arthroplasty; replacement; knee; exercise therapy; preoperative exercise; recovery of function.
Citation: J Rehabil Med 2024; 56: jrm18326. DOI: https://dx.doi.org/10.2340/jrm.v56.18326.
Copyright: © Published by Medical Journals Sweden, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Submitted: Jul 28, 2023; Accepted: Nov 6, 2023; Published: Jan 8, 2024
Correspondence address: Pascale Gränicher, University Center for Prevention and Sports Medicine, Balgrist University Hospital, Forchstrasse 319, CH-8008, Zurich, Switzerland. E-mail: pascale.graenicher@balgrist.ch
Competing interests and funding: The authors have no conflicts of interest to disclose.
Total knee arthroplasty (TKA) represents a major life event for patients with end-stage knee osteoarthritis where conservative treatments have been exhausted (1). With 16,555 surgeries in 2021 and an increase of 7.3% since 2020, primary TKA is one of the most common procedures in Switzerland (1). A similar increase can be seen in the UK, where, in 2019, the number of primary TKAs more than doubled compared with 2004 (2). Despite low complication rate, perioperative procedures and postoperative rehabilitation remain a multidisciplinary challenge with dissatisfaction rates as high as 30% (3). These patients report persistent pain or fail to achieve meaningful functional improvements. Preoperative risk factors for poor outcome, dissatisfaction and delayed recovery after TKA include low physical capacity (e.g. loss of muscle function and strength), limited participation in activities of daily living (ADL), increased symptoms (e.g. pain) and psychological aspects (e.g. inappropriately high expectations) (4, 5). Moreover, long waiting periods between indication for and actual surgery promote a sedentary lifestyle with further physical deconditioning and increasing functional limitations (6).
In the search for methods to improve outcomes after TKA, physical and mental preparation of patients within the framework of a prehabilitation (prehab) programme could be a possible strategy to optimize the basis for rehabilitation (7). However, evidence is still limited and contradictory regarding potential mid- to long-term benefits, content of prehabilitation and selection of target groups. In a meta-analyses, we concluded that the evidence for the effectiveness of preoperative exercise on knee functioning is low to very low and the effects disappeared after 3 months postoperatively (8). Beaupre et al. (9) were unable to demonstrate benefits in knee functioning at any time-point after a 6-week exercise programme, while Gränicher et al. (10) found positive differences up to 12 weeks postoperatively after a 4-week resistance and sensorimotor programme compared with no prehabilitation. Moreover, the effectiveness of the exercise programme may have been reduced in several prehabilitation studies, because the same intervention was administered to all patients, meaning that the intervention was not tailored to individual exercise capacity, performance level or physical impairments and symptoms or comorbidities (8). Thus, significant treatment effects after non-personalized, ineffective training interventions cannot be expected (11). Furthermore, the content or intensity of prehabilitation programmes is hardly described in detail, which limits the interpretation of results and transferability (12). For complex intervention studies, preceding feasibility and pilot studies are recommended to identify barriers (e.g. clinical routines, adherence to the intervention) before conducting a definitive large-scale trial (13).
Therefore, the main objective of this study was to assess the feasibility of a clinic- and home-based, supervised exercise- and education-based prehabilitation programme prior to TKA. Secondary objectives were: (i) to report preliminary effects of this piloting intervention immediately after prehabilitation, 6 and 12 weeks after surgery compared with baseline and compared with patients receiving usual care (no prehabilitation); (ii) to investigate readiness for discharge (length of stay; LOS) from the hospital; and (iii) to guide sample size calculation for future trial planning.
METHODS
Trial design
This pilot study was designed as a parallel-group randomized controlled trial conducted at Balgrist University Hospital, Zurich, Switzerland. The study protocol was registered and previously published on ClinicalTrials.gov (ID: NCT05314985) and approved by the local ethics committee of Zurich, Switzerland, prior to recruitment (BASEC-Nr 2020-03060). This study was conducted in accordance with Good Clinical Practice guidelines, the guiding principles of the Declaration of Helsinki, and was reported according to the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement extension to randomized pilot and feasibility trials (13).
Participants
Recruitment and eligibility criteria. Patients were consecutively recruited from the orthopaedic department of the Balgrist University Hospital, Switzerland. Eligibility for study participation was assessed by an independent study nurse. Inclusion criteria were: (i) adult persons (age ≥ 18 years); (ii) awaiting primary unilateral TKA. Exclusion criteria were: (i) body mass index (BMI) > 35 kg/m2; (ii) patella alta (Caton Deschamps Index > 1.2); (iii) muscle weakness due to neurological diagnosis; (iv) known or suspected non-compliance (e.g. dementia; rejective behaviour towards physiotherapy or active physical treatments); (v) known depression or other psychiatric disorders; (vi) acute pain exacerbations or inflammation; (vii) patellar instability; (viii) non-German speaking. All patients had to provide formal written informed consent before baseline assessment.
Randomization and blinding. Twenty patients were randomized to the intervention group (IG), participating in the prehabilitation programme, or the control group (CG), receiving usual care (no prehab). Assignment to the groups was performed by an independent study nurse by a random selection procedure: drawing a sealed envelope containing the group allocation. Due to the nature of the exercise intervention, neither the patient him/herself nor the physical therapists (PTs) or the investigators could be blinded to the group allocation. The postoperative PTs and the hospital staff were unaware of the group allocation. To prevent cross-contamination between groups, the content of the prehabilitation programme was known only to the IG. The sample size of 20 (10 in each group) was considered as sufficient to assess feasibility and plan for a larger trial.
Interventions
Patients randomized into IG passed through a supervised 4–8-week exercise and education programme at Balgrist University Hospital with a minimum of 2 training sessions per week (clinic- and/or home-based). The first session always took place at the clinic and a specially trained team of experienced PTs performed the prehabilitation intervention. The PT selected the exercises from a standardized catalogue with the highest possible intensity (following the recommendations of the American College of Sports Medicine (ACSM) (11)) and difficulty based on the patients’ needs, individual impairments and goals regarding knee functioning. For each exercise, the number of repetitions and sets was recorded and, if necessary, the intensity was adjusted to ensure appropriate intensity. Topics for patient education were based on a general checklist available to every PT (e.g. pain education and management, information on perioperative procedures, wound-healing process, mobility in ADLs, walking with aids and transfers) (14). A typical prehabilitation session consisted of a warm-up, exercise training and/or education and a cool-down component. A session lasted 30 min and patients were allowed to continue using the clinics’ training facility afterwards for further exercising. More details on the intervention are given in Table SI.
Patients in the CG received no additional pre-surgical treatment, which corresponded to the up-to-date procedure before TKA among surgeons. The hospital’s usual brochures for patients receiving a TKA, consisting of information regarding surgical and rehabilitation procedures, were provided. The CG was asked to keep the activity level the same during the preoperative stage and not to start a new type of therapy or training. All patients received a primary, unilateral TKA performed by the same surgical team. After TKA, all patients, regardless of their group allocation, received individual, non-monitored medical treatment independent of this pilot study.
Outcome measures
Feasibility data, such as recruiting rate, adherence to and safety of the prehabilitation programme, and health economic data (LOS), were retrieved from the clinic’s information system (KISIM, version 5.4.1.5, Cistec AG, Zurich, Switzerland). Adverse events (AE) and serious adverse events (SAE) were defined according to the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) guideline for good clinical practice (15) and systematically recorded by the research team. Physical performance-based outcome measures were assessed at baseline (T1), immediately before surgery (T2) and 12 weeks after surgery (T4). Self-reported outcomes were assessed at 4 assessment points, including 6 weeks after surgery (T3) in addition to those previously mentioned. Data on subjective assessment of health-related quality of life (HRQoL), feasibility of the use of a personal diary (e.g. compliance, applicability) to continuously assess self-reported daily pain levels will be reported elsewhere.
Feasibility of the prehabilitation programme. Feasibility of the prehabilitation programme was assessed by participation rate, adherence to and safety of the intervention. Participation rate was analysed by successful recruitment to target sample size, consent rate (% of eligible patients participating in the study) and retention rate (% of randomized participants assessed at baseline and included in the analysis). The participation rate was considered feasible, if the consent rate was ≥ 72% and retention rate was ≥ 88%, according to Jacques (16). The intervention was declared feasible when ≥ 80% of the planned preoperative therapy sessions were completed and no AE or SAE in relation with the study procedure occurred.
Self-reported outcomes. Self-reported knee functioning was assessed by the Knee Osteoarthritis Outcome Score (KOOS) (17). The KOOS is a questionnaire covering 5 dimensions: pain (9 items), knee-specific symptoms (symptoms) (7 items), ADL (17 items), sport and recreation function (sports) (5 items), and knee-related quality of life (KRQoL) (4 items) and is a valid, reliable, and responsive outcome measure in patients undergoing TKA (17). Current pain symptoms were assessed at all 4 time-points by the valid and reliable numerical rating scale (NRS) to assess pain intensity in patients with knee osteoarthritis (18). The Tegner Activity Scale (TAS) is commonly used to assess knee functioning and physical activity level after knee ligament injuries, with the German versions of the TAS (Tegner-G) validated with acceptable psychometric performances for patients after TKA (19). The Patient Global Impression of Change (PGIC) score reflects a patient’s belief about the efficacy of therapeutic and surgical treatment and was assessed at 12 weeks postoperative measurement only (20, 21).
Physical performance-based outcomes. Strength was measured by the 5 Times Sit-To-Stand (5STS) test (22) and maximum grip strength (MGS) using the JAMAR© Smart Hand Dynamometer (JAMAR© Smart, Cedarburg, Wisconsin, USA), a validated measurement for assessing the strength of knee extensors and flexors (23). Walking performance was assessed by the Timed Up and Go (TUG) (24) and 2-min Walking Test (2MWT) (25). Knee pain intensity (NRS) was documented after completion of the test. Stair negotiation was assessed by the Stair-climbing Test (SCT) using steps with a height of 16 cm (26). Joint mobility of the involved knee was assessed by active knee range of motion (ROM) in degrees (°) with a long-legged goniometer with extendable legs (76.5 cm) in the supine position (27). LOS was defined by the number of days from surgery until readiness for discharge according to the hospital criteria: (i) independent mobility with walking aids (transfers, walking, stair-climbing); and (ii) dry wound conditions.
Statistical methods
Qualitative data were presented as mean and standard deviation (SD) and categorical data were described as absolute and relative frequencies. Feasibility outcomes (adherence to the programme, participation rate, safety) and LOS were analysed using descriptive statistics or qualitative data wherever appropriate. Sample size was calculated based on the results of the KOOS ADL immediately before surgery (T2) for use in future larger studies. This outcome parameter best represents the construct of knee functioning and, at this point, immediately after the intervention phase, the exploratory effect of the prehabilitation programme could be analysed without the confounding influence of surgery. Normality of data was evaluated and parametric methods were used for exploration of group × time interaction. To present the difference between IG and CG over time, a 2-way analysis of variance (ANOVA) (2 groups: IG and CG; 4 time-points: baseline, preoperative, 6- and 12-weeks postoperative) with repeated measures on self-reported outcomes (KOOS, pain, TAS) and 2×3 ANOVA for physical performance outcomes (5STS, TUG, 2MWT, pain 2MWT, MGS, SCT, ROM) was performed. Furthermore, the effect size eta-squared (η2) was calculated (< 0.02 = trivial; 0.02–0.13 = small; 0.13–0.26 = medium; > 0.26 = large). An intention-to-treat analysis (ITT) was performed where missing value imputation was applied using the last observation carried forward method for single missing values and the mean value of the respective group for those patients who were lost to follow-up. A prior sensitivity analysis was performed with the highest, lowest and mean value of each group, which did not lead to different results in terms of significance. PGIC was compared between the groups using an independent t-test. Analyses were conducted with SPSS software version 29.0 (SPSS, Chicago, IL, USA), and significance was tested 2-sided and set at p < 0.05.
RESULTS
Participants
Between August 2021 and May 2022, a total of 135 patients scheduled for TKA were assessed for eligibility. Seventy-six met the eligibility criteria, whereof 20 patients were included (10 per group) (Fig. 1). The demographics and baseline characteristics of the participants are shown in Table I. There were no between-group differences at baseline, except for a higher BMI (p = 0.013), higher knee pain under load (p = 0.023) and after 2MWT (p = 0.007) in the CG.
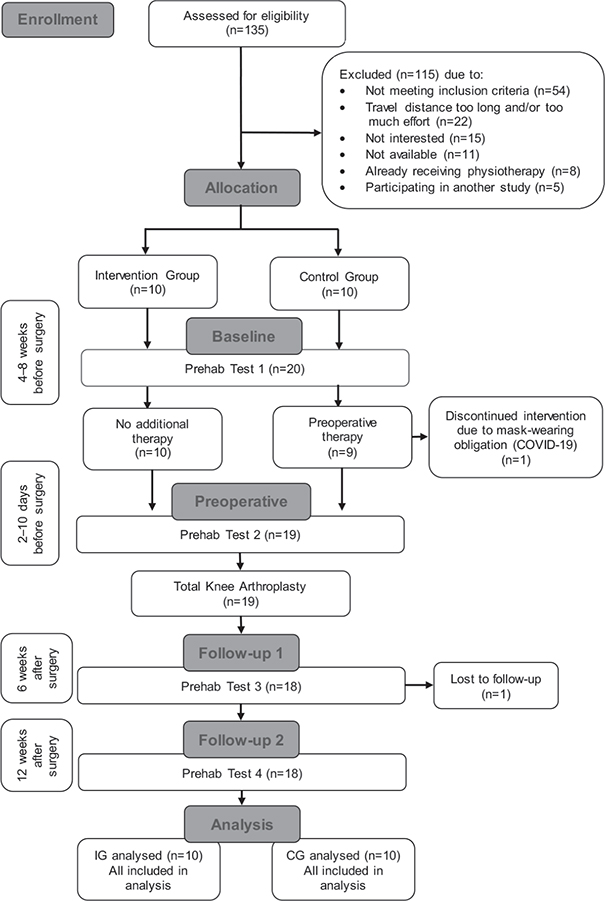
Fig. 1. Consolidated Standards of Reporting Trials (CONSORT) flow chart of randomized controlled trials. CG: control group; IG: intervention group; prehab: prehabilitation.
| Demographics | Total (n = 20) Mean (SD) |
IG (n = 10) Mean (SD) |
CG (n = 10) Mean (SD) |
p-value |
| Sex, F/M | 15/5 | 8/2 | 7/3 | 0.628 |
| Age, years | 72.70 (5.95) | 73.40 (4.60) | 72.00 (7.24) | 0.612 |
| Height, cm | 165.95 (9.15) | 167.50 (10.42) | 164.40 (7.92) | 0.463 |
| Weight, kg | 77.90 (15.50) | 73.20 (16.01) | 82.60 (14.11) | 0.181 |
| BMI, kg/m2 | 28.15 (4.43) | 25.80 (3.20) | 30.49 (4.35) | 0.013* |
| Self-reported outcomes | ||||
| KOOS pain, score 0-100 | 46.39 (15.39) | 51.11 (16.68) | 41.67 (12.8) | 0.173 |
| KOOS symptoms, score 0-100 | 45.71 (12.78) | 48.93 (12.26) | 42.5 (13.09) | 0.272 |
| KOOS ADL, score 0-100 | 60.04 (16.68) | 66.41 (18.83) | 53.68 (11.93) | 0.088 |
| KOOS sports, score 0-100 | 20.25 (16.34) | 21.00 (16.47) | 19.50 (17.07) | 0.844 |
| KOOS KRQoL, score 0-100 | 26.15 (13.61) | 27.29 (16.59) | 25.00 (10.62) | 0.717 |
| Pain at rest, NRS 0-10 | 2.20 (2.38) | 1.90 (2.38) | 2.50 (2.44) | 0.586 |
| Pain under load, NRS 0-10 | 6.35 (1.73) | 5.50 (1.84) | 7.20 (1.14) | 0.023* |
| TAS, level 0-10 | 2.75 (1.12) | 2.90 (0.99) | 2.60 (1.27) | 0.563 |
| Physical performance outcomes | ||||
| 5STS, s | 13.03 (4.50) | 12.72 (5.28) | 11.37 (5.22) | 0.767 |
| MGS, kg | 27.00 (9.44) | 26.53 (10.18 | 27.46 (9.16) | 0.832 |
| TUG, s | 8.96 (3.03) | 8.17 (2.52) | 9.75 (3.41) | 0.540 |
| 2MWT, m | 154.15 (46.18) | 167.50 (43.45) | 140.80 (47.11) | 0.204 |
| Pain 2MWT, NRS | 3.50 (2.48) | 2.10 (1.97) | 4.90 (2.18) | 0.007* |
| SCT, s | 17.27 (8.75) | 17.47 (10.50) | 17.07 (7.16) | 0.920 |
| ROM knee flexion, ° | 118.30 (16.86) | 122.20 (9.58) | 114.40 (21.79) | 0.314 |
| ROM knee extension, ° | 3.95 (8.15) | 4.90 (6.98) | 3.00 (9.45) | 0.615 |
| *Significant p < 0.05; 2MWT: 2-minute walking-test; 5STS: 5-Times Sit-To-Stand test; ADL: activities of daily living; BMI: body mass index; KOOS: Knee Osteoarthritis Outcome Score; KRQoL: knee-related quality of life; MGS: maximum grip strength; NRS: numerical rating scale; p-value: independent t-test; SCT: stair-climbing test; SD: standard deviation; TAS: Tegner Activity Scale; TUG: Timed-Up and Go test. | ||||
Feasibility and readiness for discharge
Recruitment to target sample size was successful with 20 enrolled patients. The consent rate of eligible patients was insufficient at 26% (20 out of 76), with a further 5 patients unable able to participate due to participation in other trials. Most patients declined participation due to long travel distance between their home and the clinic (35.6 ± 15.7 km) and/or because the additional therapy was too much effort in this phase before surgery (n = 22). Most frequent reasons for not fulfilling inclusion criteria were: BMI> 35 (n = 17), subsidiary diagnosis (n = 12), not German-speaking (n = 12); were not reachable by phone and/or mail or e-mail several times (n = 8). There were no AE or SAE, and the programme proved to be safe and tolerable for this patient group. Between August 2021 and September 2022, patient recruitment, baseline assessments, intervention implementation and follow-up proceeded as planned, with no major obstacles experienced. The retention rate was 90% and a total of 9 (90%) patients in the IG completed all individually scheduled therapy sessions (7 sessions (2-11)) as planned during the 4-8-week period, whereas 1 patient declined to attend the prehabilitation programme due to face mask obligations (due to SARS-CoV-2 (COVID-19)) at the clinic. No complications occurred during the surgery, but 1 patient in the IG developed an accidental strain of the gluteal muscle shortly before the 12-week follow-up and was therefore not able to complete the physical assessments at T4. LOS was similar in both groups, with no significant differences between the number of days to reach discharge criteria (CG 5 days (4-9); IG 4 days (3-8)). For the IG a total number of 46 days at the hospital was recorded, whereas the CG stayed for a total of 54 days.
In addition, the sample size for future studies investigating the efficacy of prehabilitation on knee functioning using the current KOOS ADL results at T2 as the primary outcome was calculated. Accordingly, a group size of 35 patients is recommended to ensure a power of 80% (α = 0.05).
Self-reported outcomes
Statistics of self-reported outcomes at baseline and changes preoperatively and 6 and 12 weeks after surgery are summarized in Table II. Among self-reported outcomes, significant interaction effects were observed in the ITT analyses for KOOS sports (F(3/54) = 2.895, p = 0.043, η² = 0.139) and TAS (F(2.2/39.1) = 3.20, p = 0.048, η² = 0.151) between groups and over time (Fig. 2). The improvement over time reached minimum important change (MIC) in KOOS sports (17), but not in TAS (28). Within-group analysis between the time-points separately revealed that, in IG, the KOOS sports improved significantly from 6 (T3) to 12 (T4) weeks postoperatively (p < 0.001) (Fig. 3) and TAS scores increased significantly from T1 to T2 (p = 0.021) and decreased from T2 to T3 (p = 0.023) (Fig. 4). CG shows no significant changes between any time-points in KOOS sports or TAS. The PGIC was assessed only at T3 and showed no significant between-group differences (IG 2.11 (1.45) vs CG 2.44 (1.65), p = 0.280).

Fig. 2. Frequency distribution of Tegner Activity Scale (TAS) levels T1-T4 per group. CG: control group; IG: intervention group; preop: preoperative; postop: postoperative; wk: weeks.

Fig. 3. Change of mean values in Knee Osteoarthritis Outcome Score (KOOS) sports. Preop: preoperative; postop: postoperative; CG: control group; IG: intervention group; wk: weeks.
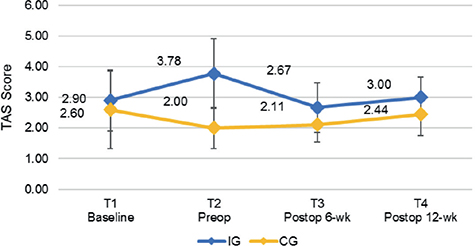
Fig. 4. Change of mean values on Tegner Activity Scale (TAS). Preop: preoperative; postop: postoperative; wk: weeks; CG: control group; IG: intervention group.
| Variable [Scale] | Time-point | IG (n = 10) Mean (SD) | CG (n = 10) Mean (SD) | Main effect of time p-value | Main effect of group p-value | Group × time p-value interaction | η2 interaction | F interaction |
| KOOS pain [score 0-100] | Baseline T1 | 51.11 (16.68) | 41.67 (12.83) | < 0.001** | 0.032* | 0.742 | 0.023 | (3/54) = 0.416 |
| ΔT1-T2 | 8.46 (23.61) | 2.22 (6.52) | ||||||
| ΔT2-T3 | 7.41 (25.26) | 11.67 (15.87) | ||||||
| ΔT3-T4 | 10.19 (12.00) | 14.20 (20.05) | ||||||
| KOOS symptoms [score 0-100] | Baseline T1 | 48.93 (12.26) | 42.50 (13.09) | < 0.001** | 0.110 | 0.930 | 0.008 | (3/54) = 0.149 |
| ΔT1-T2 | 9.40 (15.71) | 8.21 (17.82) | ||||||
| ΔT2-T3 | 2.78 (14.16) | 3.65 (21.61) | ||||||
| ΔT3-T4 | 13.49 (15.68) | 9.13 (9.24) | ||||||
| KOOS ADL [score 0-100] | Baseline T1 | 66.41 (18.83) | 53.68 (11.93) | < 0.001** | 0.068 | 0.665 | 0.028 | (3/54) = 0.528 |
| ΔT1-T2 | 2.06 (18.03) | 2.65 (11.80) | ||||||
| ΔT2-T3 | 8.17 (17.25) | 14.43 (16.92) | ||||||
| ΔT3-T4 | 6.05 (10.66) | 5.80 (21.20) | ||||||
| KOOS sports [score 0-100] | Baseline T1 | 21.00 (16.47) | 19.50 (17.07) | < 0.001** | 0.119 | 0.043* | 0.139 | (3/54) = 2.895 |
| ΔT1-T2 | 5.67 (18.38) | –2.50 (16.03) | ||||||
| ΔT2-T3 | –2.78 (21.87) | 2.44 (9.49) | ||||||
| ΔT3-T4 | 31.11 (20.11) | 9.44 (21.40) | ||||||
| KOOS KRQoL [score 0-100] | Baseline T1 | 27.29 (16.59) | 25.00 (10.62) | < 0.001** | 0.154 | 0.594 | 0.034 | (3/54.10) = 0.637 |
| ΔT1-T2 | 9.51 (18.68) | 1.25 (7.68) | ||||||
| ΔT2-T3 | 9.72 (20.65) | 6.39 (12.92) | ||||||
| ΔT3-T4 | 15.28 (15.62) | 19.44 (24.90) | ||||||
| Pain at rest [NRS 0-10] | Baseline T1 | 1.90 (2.38) | 2.50 (2.46) | 0.015* | 0.101 | 0.673 | 0.022 | (2/36.6) = 0.405 |
| ΔT1-T2 | –1.34 (1.53) | –0.40 (1.71) | ||||||
| ΔT2-T3 | 1.11 (1.10) | 0.34 (2.58) | ||||||
| ΔT3-T4 | –1.56 (1.42) | –1.22 (2.86) | ||||||
| Pain under load [NRS 0-10] | Baseline T1 | 5.50 (1.84) | 7.20 (1.14) | < 0.001** | 0.002* | 0.925 | 0.009 | (3/54) = 0.157 |
| ΔT1-T2 | –1.28 (2.97) | –0.80 (2.15) | ||||||
| ΔT2-T3 | –1.56 (2.54) | –2.29 (2.00) | ||||||
| ΔT3-T4 | –0.89 (1.79) | –0.56 (2.22) | ||||||
| TAS [Score 0-10] | Baseline T1 | 2.90 (0.99) | 2.60 (1.27) | 0.283 | 0.003* | 0.048* | 0.151 | (2.2/39.1) = 3.20 |
| ΔT1-T2 | 0.88 (0.99) | –0.60 (1.26) | ||||||
| ΔT2-T3 | –1.11 (1.29) | 0.11 (1.10) | ||||||
| ΔT3-T4 | –1.60 (1.71) | –2.96 (1.78) | ||||||
| *Significant p < 0.05; **significant p < 0.01; Δ: change; ADL: activities of daily living; F: Fisher test; KOOS: Knee Osteoarthritis Outcome Score; KRQoL: knee-related quality of life; η2: eta-square; NRS: numerical rating scale; p-value: 2-way analysis of variance (ANOVA) with repeated measures; SD: standard deviation; T1: baseline; T2: preoperative; T3: 6-weeks postoperative; T4: 12-weeks postoperative; TAS: Tegner Activity Scale. | ||||||||
Physical performance outcomes
There were no significant interactions detected in any physical performance outcome regarding strength, walking performance, stair negotiation or knee joint mobility between groups over time (Table III). However, the IG reached the MIC in SCT at 12 weeks postoperatively compared with baseline (–2.95 s) (29).
| Variable [Scale] | Time-point | IG (n = 10) Mean (SD) | CG (n = 10) Mean (SD) | Main effect of time p-value | Main effect of group p-value | Group × time p-value.interaction | η2interaction | Finteraction |
| 5STS [s] | Baseline T1 | 12.71 (5.28) | 13.35 (4.06) | 0.430 | 0.536 | 0.888 | 0.007 | (3/36) = 0.119 |
| ΔT1–T2 | –1.40 (3.89) | –0.97 (1.67) | ||||||
| ΔT2–T4 | 0.73 (5.69) | 1.24 (4.27) | ||||||
| MGS [kg] | Baseline T1 | 26.53 (10.18) | 27.46 (9.16) | 0.493 | 0.723 | 0.173 | 0.093 | (2/36) = 1.850 |
| ΔT1–T2 | 0.71 (2.86) | 0.17 (2.37) | ||||||
| ΔT2–T4 | –2.19 (1.70) | 0.45 (4.50) | ||||||
| TUG [s] | Baseline T1 | 8.17 (2.52) | 9.75 (3.41) | 0.941 | 0.225 | 0.556 | 0.032 | (2/36) = 0.597 |
| ΔT1–T2 | –0.21 (2.17) | 0.01 (1.09) | ||||||
| ΔT2–T4 | 0.45 (1.62) | –0.602.98) | ||||||
| 2MWT [m] | Baseline T1 | 167.50 (43.53) | 140.80 (47.11) | 0.860 | 0.098 | 0.910 | 0.003 | (1.5/27.0) = 0.049 |
| ΔT1–T2 | –1.06 (20.98) | –3.80 (13.54) | ||||||
| ΔT2–T4 | 1.92 (18.38) | 1.22 (33.16) | ||||||
| Pain 2MWT NRS [0–10] | Baseline T1 | 2.10 (1.97) | 4.90 (2.18) | <0.001** | 0.005* | 0.547 | 0.031 | (1.8/31.5) = 0.573 |
| ΔT1–T2 | 0.01 (2.53) | –0.60 (2.80) | ||||||
| ΔT2–T4 | –1.89 (1.59) | –2.30 (2.26) | ||||||
| SCT [s] | Baseline T1 | 17.47 (10.50) | 17.07 (7.16) | 0.407 | 0.782 | 0.735 | 0.017 | (2/36) = 0.310 |
| ΔT1–T2 | –1.28 (8.05) | 0.52 (2.14) | ||||||
| ΔT2–T4 | –1.67 (6.65) | –1.33 (5.36) | ||||||
| Knee flexion [°] | Baseline T1 | 122.20 (9.58) | 114.40 (21.79) | 0.005* | 0.419 | 0.255 | 0.073 | (1.8/17) = 1.425 |
| ΔT1–T2 | 1.24 (5.39) | 9.70 (12.41) | ||||||
| ΔT2–T4 | –6.33 (6.46) | –12.50 (12.89) | ||||||
| Knee extension [°] | Baseline T1 | 4.90 (6.98) | 3.00 (9.45) | 0.119 | 0.544 | 0.222 | 0.082 | (1.4/36) = 1.600 |
| ΔT1–T2 | –5.79 (3.47) | –3.00 (16.69) | ||||||
| ΔT2–T4 | 1.22 (4.05) | 5.83 (11.15) | ||||||
| *Significant p < 0.05; **significant p < 0.01; Δ: change; 2MWT: 2-minute walking-test; 5STS: 5-Times Sit-To-Stand test; F: Fisher test; MGS: maximum grip strength; η2: eta-square; NRS: numerical rating scale; p-value: 2-way analysis of variance (ANOVA) with repeated measures; SD: standard deviation; SCT: stair-climbing test; T1: baseline; T2: preoperative; T3: 6-weeks postoperative; T4: 12-weeks postoperative; TUG: Timed-Up and Go test. | ||||||||
DISCUSSION
This study investigated the feasibility and estimates of effects of a personalized education- and exercise-based prehabilitation programme in patients awaiting TKA. Participation in the programme proved to be safe and feasible and barriers to patient recruitment in the clinical pathway were identified. Compared with usual care, patients participating in prehabilitation benefited from higher levels of pre- and post-operative activity and were able to participate in more demanding physical tasks.
Feasibility
Alternative settings to clinic-based prehabilitation may be considered, as consent rate showed that almost 30% (22 of 76) of eligible patients declined participation due to travel distance and/or too much effort. Offering (partly) remote therapy or a more flexible combination of home- and clinic-based programmes may motivate more patients to participate in prehabilitation sessions, as, for example, preoperative tele-therapy already proved to be feasible (30). In addition, offering only clinic-based prehabilitation is likely to be a barrier to the working population, as patients who did not want to participate were, a mean of 6 years younger than those who did. To remove further barriers to participant engagement, patients already receiving physiotherapy for their osteoarthritis should be adequately educated on the different therapeutic strategy of prehabilitation and the purpose of the concept compared with classical conservative therapy should be explained in more detail. Furthermore, we assume that the consent rate might be higher in an open clinical programme outside a trial, as participation in the prehabilitation programme no longer depends on chance and compliance of IG was high.
Overall, clinical implementation of the prehabilitation patient journey, from indication for and up to the actual surgery, was safe and feasible and well tolerated by patients, with all but 1 patient participating in their scheduled therapy sessions. This patient decided not to participate in the programme after the baseline assessment due to protective measures during the SARS-CoV-2 (COVID-19) pandemic, which, it is hoped, will not be a barrier in future studies or in a future routine clinical implementation. Nevertheless, there were several confounding factors observed during this pilot trial. First, the randomized-controlled design ensured low selection bias, but since patients were not blinded to group allocation, performance bias may have occurred and CG may has changed its behaviour towards being more active (31). Secondly, rehabilitation care could not be standardized due to local standard policies; therefore, it was not possible to estimate the influence of individual procedures (e.g. inpatient vs home-based rehabilitation) on postoperative outcome parameters. Thirdly, several patients reported pain during MGS assessment by JAMAR© Smart due to trapeziometacarpal arthritis; thus, the limiting factor was not necessarily pure strength but rather a pain-induced strength limitation. A more appropriate assessment tool for this population might be the Martin Vigorimeter (32). Fourthly, no direct effect on health economic outcomes related to LOS was found, as days to discharge did not differ significantly between IG and CG, although, for the CG a total of 9 days more than IG was recorded. Therefore, this could be a result of interest in a cost-effectiveness analysis in larger future studies. However, analysis of the hospital’s internal planning processes revealed that established hospital routines influenced LOS more than patient’s condition or achievements of recovery milestones, which agrees with experiences by Janssen et al. (33) and therefore, the shorter stay may not be attributed to prehabilitation alone.
Effectiveness of prehabilitation programme
In this pilot trial, a preoperative exercise- and education-based intervention of 4–8 weeks with 10 patients in IG awaiting TKA showed significant benefits in levels of physical activity and self-reported knee functioning up to 12 weeks after surgery compared with patients receiving usual care. Despite the small sample size these results resemble the findings of Ohno et al. (34), where a 3-week training intervention was associated with improved knee functioning assessed by the Western Ontario and McMaster Universities Osteoarthritis Index up to 1 month after surgery, and the study of Hashizaki et al. (35), who applied a 3-week preoperative strength- and endurance training (IG) and reported significant improvement in physical function up to 3 months after TKA compared with exercise instruction only (CG), as measured by 6-min walk distance. Similarly, in this study, patients in IG were able to significantly improve their activity during the prehabilitation programme and may have therefore been more confident to engage in more demanding activities as assessed by the KOOS sports domain 3 months postoperatively. The decreasing TAS-score in IG at the short-term follow-up may be associated with higher expectations of respective patients regarding the continuation of their ability to be active at high levels immediately after surgery (36). Nevertheless, compared with CG, IG managed to exceed their baseline TAS level 12 weeks postoperatively.
A key element in the current exercise programme was the individually determined level of difficulty and the regular adjustments regarding intensity according to international guidelines of ACSM to ensure maximum training benefit (11). Nevertheless, no significant difference between the groups has been shown in any objectively assessed physical performance test at any time-point. Possible reasons are: (i) that 50% of the patients in the IG were exercising ≤6 weeks, and therefore, strength-related outcomes, such as 5STS, TUG, MGS or SCT and aerobic capacity (e.g. 2MWT), could not be expected to improve to a notable extent (37). Moreover, (ii) the spectrum of preoperative physical capacity was wide in both groups with TAS levels 2-5 (IG) and 1-5 (CG), including both high- and low-risk patients in the same programme. Therefore, exercise selection and intensity varied largely in IG, and priorities and goal setting for individual programmes differed. As a result, not all patients showed meaningful changes after prehabilitation, as effect estimates in low-risk patients may be weaker, explaining non-significant improvements in performance-based outcomes across the group or compared with CG. The personalized approach and its feasibility (safety and compliance) were weighted higher in this pilot trial than large treatment effects in IG, as our sample size was too small to present meaningful differences. However, these findings provide valuable insights for future trials, where subgroups and stratification according to individual goal setting, risk factors, level of physical activity and exercise priority are recommended (38). In addition, it is recommended that the personal activities of IG and CG are objectively monitored (e.g. by accelerometers), as it was not possible to estimate the contrast between physical activity levels of the groups or to ensure that the CG did not change their behaviour during the study period. Furthermore, (iii) another reason for the lack of differences between groups after TKA may be that the major beneficial effects of surgery outweigh those of the prehabilitation programme. As the influence of surgical stress decreases and confounding factors, such as non-standardized rehabilitation and other medical problems, increase after surgery, the initial advantage of prehabilitation seems to diminish compared with usual care, as several clinical trials have shown (8). Moreover, the original goal of prehabilitation is to target perioperative risk factors to avoid complications, enhance early recovery and faster regain independent mobility. It is therefore not realistic to expect long-term improvements based on interventions with short-term effectiveness (39). However, the preoperative period possibly designates an ideal time window, not only to decrease risk factors for prolonged early recovery, but also to induce sustainable changes in habits to achieve long-term improvements in movement behaviour by, for example, enhancing health literacy and self-efficacy (40). Last, but not least, (iv) 10 patients in each group was too few to detect meaningful changes or estimations of effects before and after prehabilitation.
Strengths and limitations
The lack of blinding of patients, PTs and investigators to the group assignment is a limitation of this study and may have led to measurement bias. PTs and patients may have been blinded by implementing an additional placebo group or subliminal sham intervention instead of a group without preoperative intervention and investigators by increasing personnel resources. The smaller improvement in physical activity level in the TAS and lower knee functioning in the KOOS sport in the CG may be biased by the significantly higher BMI and preoperative pain levels under load at baseline. Higher body weight promotes more pain under load; therefore, these patients were more prone to sedentary behaviour (41). A larger sample size would have prevented heterogeneity between groups, but our primary aim was to assess the feasibility of the pilot intervention and provide the effect estimates needed to design a large-scale study. Missing data were imputed with the advantage that all patients remained in the analysis, but the robustness of the results may be compromised (42). As the sensitivity analysis supported the use of mean values for imputation, this risk was minimized.
The strengths of this pilot study were (i) its randomized controlled design; (ii) the low risk of ineffectiveness due to the standardized, but customizable, prehabilitation programme delivered by a specially trained group of PTs; (iii) the same surgical team performing all TKAs and; (iv) safety and high compliance rate with and feasibility of the programme.
Conclusion
The feasibility and preliminary effectiveness of the prehabilitation programme before TKA were supported, but further research with larger sample sizes and improved study design and recruiting procedures is recommended to confirm and expand upon these findings.
ACKNOWLEDGEMENTS
The authors acknowledge David Schmidt, Rebekka Stotz, Yves Knecht and Anja Meier who conducted the prehabilitation intervention. The authors further acknowledge Michel Kocher who supported data collection.
The local ethics committee of Zurich, Switzerland approved the study protocol prior to recruitment (BASEC-Nr. 2020-03060).
The study protocol was registered and previously published on ClinicalTrials.gov (ID: NCT05314985).
REFERENCES
- Beck M, Christen B, Zdravkovic V, Brand C. Implantatregister SIRIS Hüfte und Knie: Kurzfassung – SIRIS Report 2022. Bern: SIRIS; 2022.
- Ben-Shlomo Y, Blom A, Boulton C, et al. The National Joint Registry 19th Annual Report 2022 [Accessed November 30, 2023]. London: National Joint Registry. Available from: https://www.ncbi.nlm.nih.gov/books/NBK587525/.
- Klem NR, Kent P, Smith A, Dowsey M, Fary R, Schutze R, et al. Satisfaction after total knee replacement for osteoarthritis is usually high, but what are we measuring? A systematic review. Osteoarthr Cartil Open 2020; 2: 100032. DOI: 10.1016/j.ocarto.2020.100032
- Mohammad HR, Gooberman-Hill R, Delmestri A, Broomfield J, Patel R, Huber J, et al. Risk factors associated with poor pain outcomes following primary knee replacement surgery: analysis of data from the clinical practice research datalink, hospital episode statistics and patient reported outcomes as part of the STAR research programme. PLoS One 2021; 16: e0261850. DOI: 10.1371/journal.pone.0261850
- Olsen U, Lindberg MF, Rose C, Denison E, Gay C, Aamodt A, et al. Factors correlated with physical function 1 year after total knee arthroplasty in patients with knee osteoarthritis: a systematic review and meta-analysis. JAMA Netw Open 2022; 5: e2219636. DOI: 10.1001/jamanetworkopen.2022.19636
- Desmeules F, Dionne CE, Belzile EL, Bourbonnais R, Fremont P. The impacts of pre-surgery wait for total knee replacement on pain, function and health-related quality of life six months after surgery. J Eval Clin Pract 2012; 18: 111–120. DOI: 10.1111/j.1365-2753.2010.01541.x
- Zheng Y, Huang Z, Dai L, Liu Y, Chen Y, Zhang W, et al. The effect of preoperative rehabilitation training on the early recovery of joint function after artificial total knee arthroplasty and its effect evaluation. J Healthc Eng 2022; 2022: 3860991. DOI: 10.1155/2022/3860991
- Gränicher P, Mulder L, Lenssen T, Scherr J, Swanenburg J, de Bie R. Prehabilitation improves knee functioning before and within the first year after total knee arthroplasty: a systematic review with meta-analysis. J Orthop Sports Phys Ther 2022; 52: 709–725. DOI: 10.2519/jospt.2022.11160
- Beaupre L, Lier, D, Davies, DM, Johnston, DB. The effect of a preoperative exercise and education program on functional recovery, health related quality of life, and health service utilization following primary total knee arthroplasty. J Rheumatol 2004; 31: 1166–1173.
- Gränicher P, Stöggl T, Fucentese SF, Adelsberger R, Swanenburg J. Preoperative exercise in patients undergoing total knee arthroplasty: a pilot randomized controlled trial. Arch Physiother 2020; 10: 13. DOI: 10.1186/s40945-020-00085-9
- American College of Sports Medicine. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc 2009; 41: 687–708. DOI: 10.1249/MSS.0b013e3181915670
- Holden S, Barton CJ. ‘What should I prescribe?’: time to improve reporting of resistance training programmes to ensure accurate translation and implementation. Br J Sports Med 2019; 53: 264–265. DOI: 10.1136/bjsports-2017-098664
- Eldridge SM, Lancaster GA, Campbell MJ, Thabane L, Hopewell S, Coleman CL, et al. Defining feasibility and pilot studies in preparation for randomised controlled trials: development of a conceptual framework. PLoS One 2016; 11: e0150205. DOI: 10.1371/journal.pone.0150205
- Clode NJ, Perry MA, Wulff L. Does physiotherapy prehabilitation improve pre-surgical outcomes and influence patient expectations prior to knee and hip joint arthroplasty? Int J Orthop Trauma Nurs 2018; 30: 14–19. DOI: 10.1016/j.ijotn.2018.05.004
- European Medicines Agency. Guideline for good clinical practice E6(R2) 2018; London: European Medicines Agency; 2018.
- Jacques RM, Ahmed R, Harper J, Ranjan A, Saeed I, Simpson RM, Walters SJ. Recruitment, consent and retention of participants in randomised controlled trials: a review of trials published in the National Institute for Health Research (NIHR) Journals Library (1997–2020). BMJ Open 2022; 12: e059230. DOI: 10.1136/bmjopen-2021-059230
- Roos E, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes 2003; 3: 64. DOI: 10.1186/1477-7525-1-64.
- Alghadir AH, Anwer S, Iqbal A, Iqbal ZA. Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J Pain Res 2018; 11: 851–856. DOI: 10.2147/JPR.S158847
- Swanenburg J, Koch PP, Meier N, Wirth B. Function and activity in patients with knee arthroplasty: validity and reliability of a German version of the Lysholm Score and the Tegner Activity Scale. Swiss Med Wkly 2014; 144: w13976. DOI: 10.4414/smw.2014.13976
- Geisser ME, Clauw DJ, Strand V, Gendreau RM, Palmer R, Williams DA. Contributions of change in clinical status parameters to Patient Global Impression of Change (PGIC) scores among persons with fibromyalgia treated with milnacipran. Pain 2010; 149: 373–378. DOI: 10.1016/j.pain.2010.02.043
- Swanenburg J, Gruber C, Brunner F, Wirth B. Patients’ and therapists’ perception of change following physiotherapy in an orthopedic hospital’s outpatient clinic. Physiother Theory Pract 2015; 31: 293–298. DOI: 10.3109/09593985.2014.994152
- Medina-Mirapeix F, Vivo-Fernandez I, Lopez-Canizares J, Garcia-Vidal JA, Benitez-Martinez JC, Del Bano-Aledo ME. Five times sit-to-stand test in subjects with total knee replacement: Reliability and relationship with functional mobility tests. Gait Posture 2018; 59: 258–260. DOI: 10.1016/j.gaitpost.2017.10.028
- Hashimoto S, Hatayama K, Terauchi M, Saito K, Higuchi H, Chikuda H. Preoperative hand-grip strength can be a predictor of stair ascent and descent ability after total knee arthroplasty in female patients. J Orthop Sci 2020; 25: 167–172. DOI: 10.1016/j.jos.2019.03.003
- Yuksel E, Kalkan S, Cekmece S, Unver B, Karatosun V. Assessing minimal detectable changes and test-retest reliability of the timed up and go test and the 2-minute walk test in patients with total knee arthroplasty. J Arthroplasty 2017; 32: 426–430. DOI: 10.1016/j.arth.2016.07.031
- Butland RJ PJ, Gross ER, Woodcock AA, Geddes DM. Two-, six-, and 12-minute walking tests in respiratory disease. Br Med J (Clin Res Ed) 1982; 284: 1607–1608. DOI: 10.1136/bmj.284.6329.1607
- Mizner RL, Petterson SC, Clements KE, Zeni JA, Jr, Irrgang JJ, Snyder-Mackler L. Measuring functional improvement after total knee arthroplasty requires both performance-based and patient-report assessments: a longitudinal analysis of outcomes. J Arthroplasty 2011; 26: 728–737. DOI: 10.1016/j.arth.2010.06.004
- Cibere J, Bellamy N, Thorne A, Esdaile JM, McGorm KJ, Chalmers A, et al. Reliability of the knee examination in osteoarthritis: effect of standardization. Arthritis Rheum 2004; 50: 458–468. DOI: 10.1002/art.20025
- Wirth B, Meier N, Koch PP, Swanenburg J. Development and evaluation of a German version of the Tegner activity scale for measuring outcome after anterior cruciate ligament injury. Sportverletz Sportschaden 2013; 27: 21–27. DOI: 10.1055/s-0032-1330752
- Almeida GJ, Schroeder CA, Gil AB, Fitzgerald GK, Piva SR. Interrater reliability and validity of the stair ascend/descend test in subjects with total knee arthroplasty. Arch Phys Med Rehabil 2010; 91: 932–938. DOI: 10.1016/j.apmr.2010.02.003
- Doiron-Cadrin P, Kairy D, Vendittoli PA, Lowry V, Poitras S, Desmeules F. Feasibility and preliminary effects of a tele-prehabilitation program and an in-person prehablitation program compared to usual care for total hip or knee arthroplasty candidates: a pilot randomized controlled trial. Disabil Rehabil 2020; 42: 989–998. DOI: 10.1080/09638288.2018.1515992
- Banerjee A, Pluddemann A, O’Sullivan J, Nunan D. Performance Bias Catalogue of Bias: Nuffield Department of Primary Care Health Sciences; 2019 [acessed 2023 Nov 30]. Available from: https://catalogofbias.org/biases/performance-bias/.
- Sipers WM, Verdijk LB, Sipers SJ, Schols JM, van Loon LJ. The Martin Vigorimeter represents a reliable and more practical tool than the Jamar dynamometer to assess handgrip strength in the geriatric patient. J Am Med Dir Assoc 2016; 17: 466.e461–466.e467. DOI: 10.1016/j.jamda.2016.02.026
- Janssen ER, Osong B, van Soest J, Dekker A, van Meeteren NL, Willems PC, et al. Exploring associations of preoperative physical performance with postoperative outcomes after lumbar spinal fusion: a machine learning approach. Arch Phys Med Rehabil 2021; 102: 1324–1330. DOI: 10.1016/j.apmr.2021.02.013
- Ohno C, Ogawa T, Taniguchi T, Kinoshita T, Fujita Y, Nishimura Y, et al. Effect of 3-week preoperative rehabilitation on pain and daily physical activities in patients with severe osteoarthritis undergoing total knee arthroplasty. Br J Pain 2022; 16: 472–480. DOI: 10.1177/20494637221084190
- Hashizaki T, Nishimura Y, Ogawa T, Ohno C, Kouda K, Umemoto Y, et al. Effectiveness of a 3-week rehabilitation program combining muscle strengthening and endurance exercises prior to total knee arthroplasty: a non-randomized controlled trial. J Clin Med 2023; 12: 1523. DOI: 10.3390/jcm12041523
- Ponzio DY, Chiu YF, Salvatore A, Lee YY, Lyman S, Windsor RE. An analysis of the influence of physical activity level on total knee arthroplasty expectations, satisfaction, and outcomes: increased revision in active patients at five to ten years. J Bone Joint Surg Am 2018; 100: 1539–1548. DOI: 10.2106/jbjs.17.00920
- Carli F, Zavorsky, G.S. Optimizing functional exercise capacity in the elderly surgical population. Curr Opin Clin Nutr Metab Care 2005; 8: 23–32. DOI: 10.1097/00075197-200501000-00005.
- Durrand J, Singh, SJ, Danjoux, G. Prehabilitation. Clin Med (Lond) 2019; 19: 458–464. DOI: 10.7861/clinmed.2019-0257.
- Berghmans DDP, Lenssen AF, Emans PJ, de Bie RA. Functions, disabilities and perceived health in the first year after total knee arthroplasty; a prospective cohort study. BMC Musculoskelet Disord 2018; 19: 250. DOI: 10.1186/s12891-018-2159-7
- Warner D. Surgery as a teachable moment: lost opportunities to improve public health. Arch Surg 2009; 144: 1106–1107. DOI: 10.1001/archsurg.2009.205
- Akhavan NS, Ormsbee L, Johnson SA, George KS, Foley EM, Elam ML, et al. Functionality in middle-aged and older overweight and obese individuals with knee osteoarthritis. Healthcare (Basel) 2018; 6: 74. DOI: 10.3390/healthcare6030074
- Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ 2009; 338: b2393. DOI: 10.1136/bmj.b2393