EFFECTS OF VIRTUAL REALITY-BASED NECK-SPECIFIC SENSORIMOTORTRAINING IN PATIENTS WITH CHRONIC NECK PAIN: A RANDOMIZED CONTROLLED PILOT TRIAL
Marina Nusser, MSc1, Michael Kramer, MD2, Sebastian Knapp, PhD1 and Gert Krischak, MD, MBA1
From the 1Institute for Research in Rehabilitation Medicine at Ulm University, 2Alb Donau Clinic Ehingen, Bad Buchau, Germany
Objective: To evaluate the effects of neck-specific sensorimotor training using a virtual reality device compared with 2 standard rehabilitation programmes: with, and without general sensorimotor training, in patients with non-traumatic chronic neck pain.
Design: Pilot randomized control study.
Patients and methods: A total of 51 participants were randomly assigned to 1 of 3 groups: 1: control group; 2: sensorimotor group; 3: virtual reality group. All 3 groups received the clinic’s standard rehabilitation programme. Group 2 also received “general sensorimotor training” in the form of group therapy, for a total of 120 min. Group 3 received additional virtual reality-based “neck-specific sensorimotor training” for a total of 120 min. Participants’ neck pain, headaches, active cervical range of motion, and Neck Disability Index were determined before and after 3 weeks of intervention.
Results: Compared with the control group, the virtual reality group showed significant (p < 0.05) advantages in relief of headaches, and active cervical range of motion in flexion and extension. Compared with the sensorimotor group, the virtual reality group showed significant improvements in cervical extension.
Conclusion: Virtual reality-based sensorimotor training may increase the effects of a standard rehabilitation programme for patients with non-traumatic chronic neck pain, especially active cervical range of motion in extension.
Key words: neck pain; rehabilitation; virtual reality; kinematics.
Accepted Dec 14, 2020; Epub ahead of print Dec 28, 2020
J Rehabil Med 2021; 53: jrm00151
Correspondence address: Gert Krischak, Institute for Research in Rehabilitation Medicine at Ulm University, Am Kurpark 1, 88422 Bad Buchau, Germany. E-mail: gert.krischak@uni-ulm.de
Doi: 10.2340/16501977-2786
The aim of this study was to evaluate the effectiveness of neck-specific coordination training using a virtual reality device, in comparison with general coordination training and a standard exercise programme as part of inpatient rehabilitation for patients with chronic neck pain. Pain, disability and mobility of the neck were determined before and after 3 weeks of training intervention in 51 patients. The virtual reality training group exhibited greater effects in relief of headaches, and bending the neck forwards and backwards compared with the standard exercise group, and an increased ability to bend the neck backwards compared with the coordination training group. The results suggest that neck-specific coordination training using a virtual reality device increases the benefits of standard inpatient rehabilitation in patients with chronic neck pain, particularly in bending the neck backwards.
Neck pain is a widespread problem; 60–80% of individuals develop neck pain during their lifetime, with 30–50% of the general population reporting neck pain annually (1–3). Many patients experience neck pain as a complex biopsychosocial disorder, with problematic physical and psychological symptoms (3), such as reduced cervical range of motion, headaches, lack of concentration, emotional and cognitive disorders (4, 5). Aside from the decreased quality of life, these complaints are a major cause of inability to work (6, 7) and lead to considerable economic damage (8). Hence, the demand for an effective treatment is indisputable.
According to a recently published review (9), the strongest treatment effects for neck pain are those associated with exercise. However, the evidence for this claim is only of moderate quality. Since there is no data available at present to show that any one form of exercise is evidentially more effective than another, multimodal care is concordantly recommended by leading experts (3, 9).
Sensorimotor training methods are a current trend in exercise therapy, and for the first time they take into account the special function of the neck, by including connections between the perceptions of sensory organs located in the head and neck muscles (10–14). Alterations of sensorimotor control have been identified in many patients with neck pain, and are thought to play an important role in the aetiology and maintenance of associated disorders (14, 15).
To date, there are only a few sensorimotor training concepts that have been specially developed for the neck region. Initial studies found that patients undergoing these training methods experienced reduced neck pain, as well as improvements in cervical range of motion, self-reported disability, and general health (11, 13, 14, 16). However, a systematic review from 2014 (17) revealed very little evidence for eye-neck coordination and proprioceptive exercises. Furthermore, a randomized controlled trial (RCT) found that neck coordination exercises did not produce a larger effect than strength training and massages (18).
Application of a virtual reality (VR) device is a novel and promising option for training cervical kinematics (10, 12, 19). In theory, this technique provides several advantages: distracting attention and therefore reducing pain and kinesiophobia (20, 21), engaging and motivating physical activities, and improving the effectiveness of exercise (22, 23).
To date, only one RCT has compared the effects of VR-based training with conventional kinematic training using laser beams in patients with chronic neck pain (12). The VR group exhibited significant improvements in motion velocity, pain intensity, health status, and accuracy of neck motion.
Due to the conflicting evidence and lack of research, there is a need for more studies that consider the effectiveness of VR-based sensorimotor training concepts, especially in combination with other effective therapeutic exercises or as part of individually tailored programmes (12).
The aim of this study was therefore to evaluate the effects of neck-specific sensorimotor training using a VR device, in comparison with standard rehabilitation programmes, both with and without general sensorimotor training, in patients with non-traumatic chronic neck pain.
Participants
A total of 55 patients who underwent inpatient rehabilitation at the Federseeklinik Bad Buchau (Germany) due to experiencing non-traumatic chronic neck pain (more than 3 months) were recruited between February 2014 and March 2017. Diagnoses were primarily made by patients’ general practitioners, and confirmed by the physician in charge at the rehabilitation hospital. Further inclusion criteria were such that the patients must be adults aged 18 years or more, and have taken no pain medication or muscle relaxants for 24 h before the tests. Exclusion criteria were: traumatic neck pain, neck pain originating from whiplash, cervical fracture/dislocation, operations in the cervical spine area, damage to the inner ear, vertebrobasilar insufficiency, basic neurological diseases, range of motion of the cervical spine < 10° in flexion, extension, and/or rotation.
The subjects were divided randomly into 3 groups: a control group (CG), a sensorimotor group (SMG), and a VR group (VRG). Randomization of subjects was carried out in blocks (block-size 15), and stratified by sex. The randomization scheme was generated using the software “Randomization.com” (http://www.randomization.com).
The study was approved by the ethics committee of the University of Ulm (registration number 317/13), and was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent prior to study entry.
Sample size estimation and blinding
As there is no dependable data to date, the choice of sample size based on clinical experience and feasibility. A sample size of 15–20 patients per group was considered, at very least, to show tendencies concerning therapeutic effects.
Due to the nature of the intervention, blinding was not possible for the patient or the therapist.
Intervention
Between the start (pre-intervention) and end of rehabilitation (post-intervention), there was a period of approximately 3 weeks, during which the inpatient interventions described below took place.
The CG underwent a “standard rehabilitation programme”, including a combination of individual and group therapies instructed by physiotherapists and certified sports scientists. In detail, the programme comprised different forms of general and neck-specific exercise therapy, such as strengthening, mobilization, relaxation, medical training therapy, functional gymnastics, aqua therapy, physical therapy, and traditional “back school”. The adaptation of exercises was up to the individual therapist and their clinical expertise. Patients also received special lectures from orthopaedists and psychologists, who provided information about chronic pain, along with therapeutic goals, and an emphasis on the importance of being proactive.
The SMG received the “standard rehabilitation programme” plus a total of 120 min of “general sensorimotor training”. This training took place over 4 30-min group therapy sessions, and was instructed by a physiotherapist or a certified sports scientist. The objective was training and improvement in patients’ coordination through skill exercises (e.g. passing an obstacle course, dribbling, rope skipping, tossing balls through rings), balance exercises (e.g. standing with eyes closed, single-leg stance, slacklining), small game forms (e.g. juggling, curling, throwing and catching), and partner games, such as badminton or table tennis.
In addition to the “standard rehabilitation programme”, patients in the VRG completed a total of 120 min of “neck-specific sensorimotor training” (NSST) using a VR device in individual therapy. Due to the required concentration, the training was divided into 6 20-min sessions. The training was instructed by a scientific assistant with a basic education in physiotherapy.
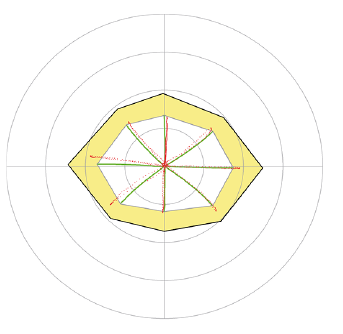
The NSST was executed using a modified VR system (Fraunhofer- Institut für Graphische Datenverarbeitung, Darmstadt, Germany) based on that described by Kramer et al. (19), as follows. In the upright sitting position, the patient wore a helmet (Schutzhelm uvex pheos alpine. Fürth, Germany) with an integrated monitor (virtual reality head-mounted display 5DT HMD 800-26 2D, League City, Texas, USA). A globe was shown, moving in a virtual space on predetermined trajectories, on the monitor (Figs 1–3). The patient was asked to follow by moving the head the orbital pathways of the globe. The patient had to try to track the virtual globe as closely as possible with a white circle, whose position in the virtual scene corresponded to their head position. A fixed eye position was maintained due to the short distance between the patient’s eyes and the monitor in the helmet, so this task could only be accomplished with head movements.
A 3Space Fastrak System (Polhemus Inc., Colchester, VT, USA) was used for head-movement tracking. The sensors of the tracking system were attached to the test helmet.
Before each training session, the current maximum active cervical range of motion (ACROM) of the patient was determined in a total of 8 directions: flexion, extension, right and left rotation, and the diagonals in between. The current maximum ACROM was registered using 3Space Fastrak in order to calibrate the system (external black octagon in Figs 1–3).
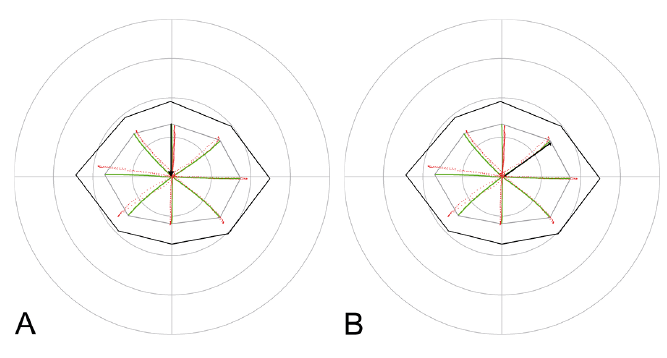
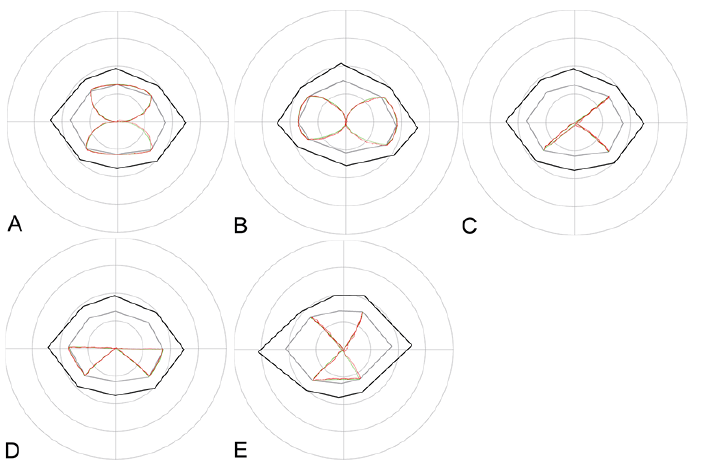
In every NSST session, the VRG patients underwent each of the following tasks twice: the Head Repositioning Test (HRT) (Fig. 2A) on the basis of Revel et al. (24), the Head to Target Test (HTT) (Fig. 2B) on the basis of Loudon et al. (25) and Kramer et al. (19), and a dynamic exercise including 5 different trajectories (Fig. 3A–E) on the basis of Kramer et al. (19).
Rest breaks of approximately 3 min were given between tasks, and extended if any side-effect (e.g. motion sickness, nausea, or headaches) was reported. Patients only continued if side-effects subsided, otherwise they would stop the training session.
Head Repositioning Test and Head to Target Test. The subject started in an upright seated position, with their head in a neutral position, which the subject was asked to memorize (required position HRT) (Fig. 2A). The globe then led the subject’s head to a specific position in 1 of the 8 directions (required position HTT) (Fig. 2B), and disappeared. After that, the subject was asked to first find the neutral position again without visual guidance (actual position HRT), and then the specific end position (actual position HTT).
Dynamic exercise. In this exercise, globes travelled along trajectory A–E, one after another, and the subject had to follow them in the virtual scene by moving their head precisely (Fig. 3A–E).
In order to achieve the best possible effects, the NSST was adapted to the participants, and successively increased in level of difficulty. Therefore, every training unit was different in terms of the underlying ranges of motion and speeds: the boundaries for the globe’s trajectories varied from 30% to 90% (inner grey octagon in Figs 1–3) of the current individual maximum ACROM (external black octagon in Figs 1–3).The speed of travel of the globe increased from 5 s (very slow) to 3 s (very fast) per trajectory.
Outcome measures
A 0–10 numerical rating scale (NRS) was used to investigate the mean pain intensity during the last week. Higher scores indicate greater intensity. The NRS is a well-evaluated, reliable and valid tool to measure pain (26). The following pain categories were evaluated: neck pain at rest, neck pain during motion, headache at rest, headache during motion.
For patients with neck pain, the NRS exhibits a minimal detectable change (MDC) value of 2.1, and a minimum clinically important difference (MCID) value of 1.3 (27).
ACROM was determined using the VR device twice at both measuring points, and represented as angles (in degrees). Mean values were calculated for further data analysis. The following movement directions were evaluated: flexion, extension, left rotation, and right rotation. Thus far, there are no data on MCID (5).
The Neck Disability Index (NDI) (28), a questionnaire with 10 items, was used to examine self-reported disability associated with neck pain. Each section was scored on a 0–5 rating scale. Higher scores (maximum 50) indicate greater disability. The NDI was shown to demonstrate good validity and reliability (29). Changes should exceed the MDC of 8.4 points, or at a minimum the MCID of 3.5 points’ cut-off to be considered relevant (30).
All outcome measures were collected pre- and post- intervention for each patient in each group. A non-blinded scientific assistant (the same as instructed the NSST) handed out the assessments (NRS and NDI) to the patients, and asked them to complete them autonomously. In order to avoid assessor-caused bias, explanations regarding how to deal with the assessments were provided in writing on the corresponding questionnaires.
Statistical analysis
All statistical analyses were performed using the statistical programme “R” (31). The Shapiro–Wilk test was used to check the normality of the outcome variables. Parametric statistics were used as the majority of variables were found to be normally distributed. Descriptive statistics are presented as means with standard deviations (SD). Within-group differences between pre- and post-intervention were evaluated using a paired 2-tailed t-test. The significance level was set at p < 0.05.
Due to the exploratory nature of this pilot, no adjustments (concerning the significance level of the p-value) were made for multiple tests, in order to maintain sensitivity to potentially interesting effects, even at the risk of increased Type I error.
Basic treatment effects between the 3 groups were examined using a 1-way analysis of variance (ANOVA) for each parameter, based on the score differences post-intervention minus pre-intervention. For post hoc tests, the Tukey-Kramer test was used.
To demonstrate the estimated effect sizes of observed between-group changes and its precision, Cohen’s d and its 95% confidence interval (95% CI) was calculated (32). It was interpreted as suggested by Cohen, with d ≥ 0.2 indicating small effect size, 0.5 medium, and d ≥ 0.8 large effect size (33).
General characteristics of the subjects
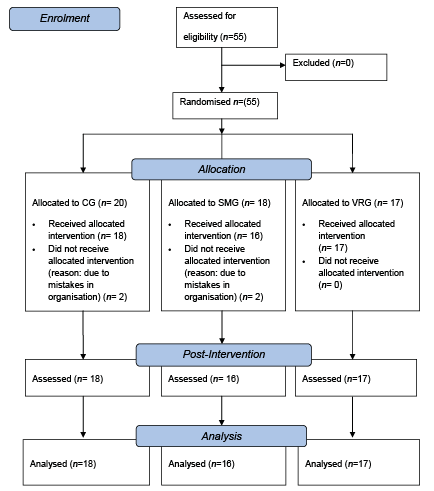
A total of 55 patients with non-traumatic chronic neck pain were enrolled in the study. 20 were assigned to the CG, 18 to the SMG, and 17 to the VRG. Four patients had to be excluded from the analysis due to organizational deviations from the treatment planning set out in the study plan. Therefore, only the data for the final 51 patients were analysed. The flow diagram for participants in the study is shown in Fig. 4.
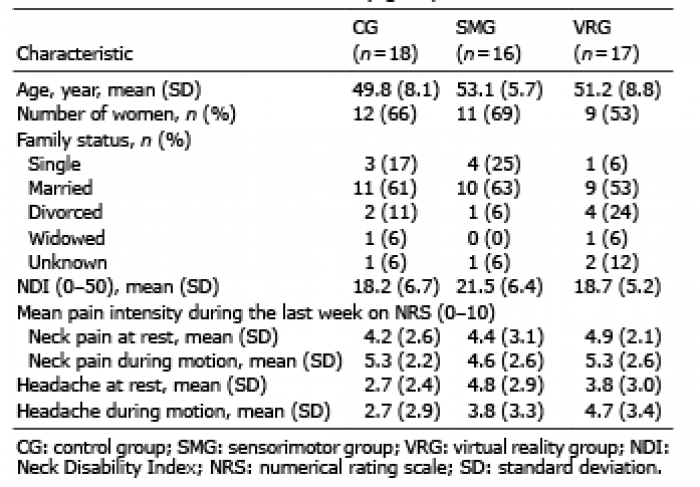
The patients’ baseline characteristics are shown in Table I. The distribution of age, sex, and family status was similar in all 3 groups.
In addition to neck pain, most patients experienced headaches. The pre-intervention prevalence of headache at rest (at least 1 on NRS) was 67% in the CG, 88% in the SMG, and 82% in the VRG. The pre-intervention prevalence of headache during motion was 56% in the CG, 69% in the SMG, and 88% in the VRG.
The mean intensity of headache was slightly higher in the SMG and VRG than in the CG, and the mean NDI was comparatively high in the SMG (Table I). There were no major differences in any other parameters between the groups.
Side-effects
Besides the weight of the helmet, which some patients found unpleasant, no other negative side-effects were reported regarding the VR device or in general. Therefore, all patients (not including the 4 who discontinued participation) could complete the measurements required for the training, as planned.
Pain
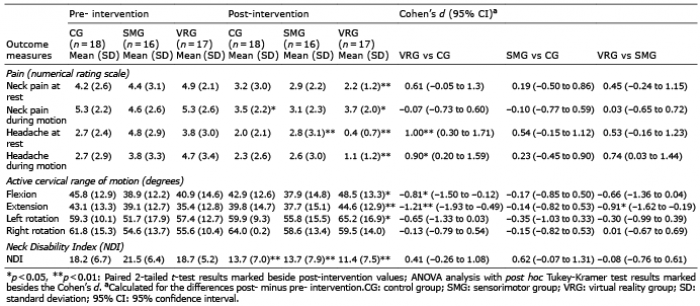
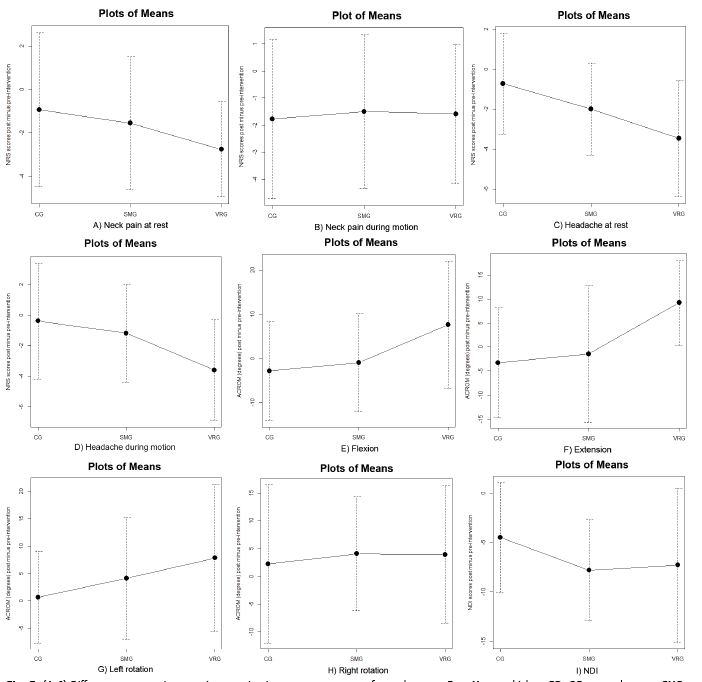
The rehabilitation led to a clinically relevant relief of neck pain and headaches for most patients (Table II, Fig. 5A–D). Within-group analysis showed a statistically significant improvement in the VRG across all pain categories. For the SMG, significant improvements were seen in reducing headaches while at rest. The CG saw significantly reduced neck pain during motion. Between-group analysis showed that the VRG improved significantly more than the CG in reducing headaches at rest (VRG vs CG p = 0.008) and headaches during motion (VRG vs CG p = 0.023), each with large effect sizes.
Active cervical range of motion
The VRG improved in each movement direction (Table II, Fig. 5E–H). For flexion, extension, and left rotation, the improvements were statistically significant. For increase in flexion and extension, the differences between groups were statistically significant (flexion: VRG vs CG p = 0.041, extension: VRG vs CG p = 0.007; VRG vs SMG p = 0.031), with medium-to-large size effects in favour of the VRG.
Neck Disability Index
The improvements in self-reported disability were both statistically significant and clinically relevant in all 3 groups. The mean changes in NDI scores achieved were all above the MCID of 3.5 points, with the SMG and VRG showing clearer improvements than the CG (Table II, Fig. 5I).
This pilot study is the first to evaluate the effects of neck-specific sensorimotor training using a VR device in combination with a standard rehabilitation programme, in direct comparison with the same standard rehabilitation programme both with and without general sensorimotor training in patients with non-traumatic chronic neck pain.
Overall, the results show that patients in the VRG underwent significant improvements in their neck pain, headaches, ACROM in flexion, extension, and left rotation, as well as in self-reported disability. Compared with the CG, the between-group analysis revealed that the additional VR training had greater effects in improving headaches, and ACROM in flexion and extension. The only statistically significant difference relevant to the SMG was a between-group comparison showing a marked improvement in cervical extension in the VRG.
Considered in detail, the relief of neck pain during motion was almost equal in all 3 groups. Regarding neck pain at rest, the VRG was the only group that showed a statistically significant improvement, even though between-group analyses found no statistically significant advantage compared with the other groups.
More conspicuous were the different reductions in headaches. In the VRG these reductions were statistically significant, and the differences in the mean values clearly constitute a clinically significant change, as they exceeded both MCID (1.3) and MDC (2.1). Moreover, between-group analysis revealed that these improvements were significantly higher than those in the CG, and the corresponding size effects were large.
Aside from the fact that the prevalence and the baseline values for pain variables were partly higher in the VRG, which might be a determining factor in explaining the greater improvements, the present results appear to suggest that additional sensorimotor training using a VR device might reduce pain more effectively than a pure standard rehabilitation programme in patients with non-traumatic chronic neck pain.
These findings are in accordance with previous research. Several studies have shown that exercises based both on eye-head coordination (13, 16) and neck coordination that aimed to improve patients’ sense of their cervical position lead to a reduction in neck pain in cervicalgic patients (11, 13, 14). Training using VR techniques decreased pain more effectively than the same training using a laser pointer attached to the participant’s head (10, 12).
Sarig Bahat et al. (10, 12) consider that, due to cervical kinematic training directing impairments such as reduced movement range, accuracy, velocity, and smoothness, fine motor control and coordination are improved.
According to Panjabi (34) and Jull et al. (14), improved coordination between the deep and superficial cervical muscles may lead to better support of the cervical segments, and could decrease the stress on cervical structures, which, in turn, could reduce neck pain. Furthermore, Sarig Bahat et al. (10) consider that (VR-based) kinematic training might enhance neural connections between the eyes, neck, and vestibular systems. Assuming that cervicogenic headache might be related to a disturbed cervicocephalic reflex system (15), an appropriate reorganization, potentially caused by VR-based training, might explain the significant reduction in headaches within the VRG in the current study.
In addition to pain, the current study investigated changes in the ACROM, and found that the best improvements were achieved in the VRG. Flexion and extension increased by approximately 20–25%, which is a clinically significant change that would probably make a difference in everyday activities for patients. Improvements in rotation were smaller, possibly due to the near-normative baseline values (5) and ceiling effects.
Sarig Bahat et al. (10) also found that kinematic training both with and without an interactive VR device increased ACROM, with some advantages in the VRG, especially in flexion and extension.
Besides the VR technique, which is known to enhance baseline ACROM (35), another explanation might be the procedure used for VR-based training in the current study. The explicit request for subjects to reach the maximum end of motion and their active involvement encouraged patients to push themselves to their limits in each training session. Each subsequent training session was undertaken within the regained motion range, and thus represents an optimum stimulus for the increased motion. Such, probably crucial, individual and regular adjustment of the training parameters is rarely seen in other applications of standard rehabilitation methods.
The combination of improved pain and ACROM might have contributed to the reduction in self-reported disability in the present study’s population. This hypothesis is supported by the detected changes of the NDI scores, which indicate that sensorimotor training in the SMG and VRG increased the effects of the pure standard rehabilitation concerning activities of daily living.
This is also in agreement with previous findings. Studies including patients with chronic neck pain, of both idiopathic and traumatic origin, demonstrate the effectiveness of neck-specific sensorimotor exercises on neck disability (11, 14). Again, VR-based regimes seem to be more effective than training using laser pointers (10, 12).
As the findings of this pilot study largely agree with previous findings, the results may be translated to patients with non-traumatic chronic neck pain in general, although further research is necessary to confirm these effects. The training could also be a good option for patients with whiplash-associated disorders (WAD). These patients are often more challenging to treat than patients with non-traumatic neck pain. The assumption that this is due to differences in physical impairment (6) is arguable. Jull et al. (6) found impairment in the neck flexor synergy in patients with neck pain of both whiplash and insidious origin. While this impairment between the 2 groups appears to be similar (6), deficits in head repositioning accuracy and cervical movement control are known to be greater in patients with traumatic neck pain (16, 36–38). As the VR-based training used in the present study addresses both head repositioning accuracy (using HRT and HTT) and movement control (using the dynamic exercise), patients with WAD might benefit from such a training method even more than patients with non-traumatic neck pain.
The study design made it possible to investigate the supposed benefit of a new and promising exercise methodology, namely the VR device, within a common standard rehabilitation setting in patients with non-traumatic chronic neck pain.
The application of VR in rehabilitation therapy offers new possibilities. In addition to the neck-specific sensorimotor training, which appears to improve fine motor control as well as the ACROM, it distracts patients’ attention, and therefore also has potential to positively influence psychological aspects, such as kinesiophobia (39), which play an important role for chronic pain patients (40). Follow-up studies should consider this aspect by incorporating appropriate outcome measures.
This study demonstrated that the VR technique can be integrated into the rehabilitation daily routine with little effort. The main challenge was in treatment planning, as can be seen from the reasons for participants withdrawing from this study. Negative side-effects, such as VR-associated sickness, which have been reported in other trials (10, 12) did not occur in the present study population. However, some patients complained about the weight of the helmet, and so, in future, lightweight glasses should be used instead.
Study limitations
This study has a number of limitations. Firstly, there was a potential risk of bias. Despite the fact that patients were asked to complete the questionnaires (NRS and NDI) autonomously, and the ACROM was (objectively) measured via the 3Space Fastrak System, an assessor-caused risk of bias cannot be ruled out, as the assessor was not blinded.
Secondly, the small sample size could be problematic. Although the within-group changes indicate that patients in the VRG benefited most from the treatment, a statistically significant superiority of method could only partly be confirmed by between-group analysis, which might be due to the small sample size.
Thirdly, due to lack of long-term follow-up there is a possibility that the results may have only been short-lived. Originally, it was planned to perform a follow-up after 6 months, but due to a low response rate (<30%) it was not possible to carry out a useful data analysis.
Despite these constraints, the results of this pilot study provide important data on how to calculate the number of cases to include in follow-up studies.
Conclusion
This study shows that, for patients with non-traumatic chronic neck pain, the application of a VR-based neck-specific sensorimotor training within a common standard rehabilitation programme is both feasible and reasonable. The results suggest that patients in the VRG improved in terms of their neck pain, headaches, ACROM in flexion, extension, and left rotation, as well as in self-reported disability. Specific between-group differences implied potential advantages of the VR training concerning headaches and ACROM in flexion and extension, compared with the CG, and concerning enhanced cervical extension compared with the SMG.
Although the results of this pilot study largely agree with those of previous research, follow-up studies are needed to validate the effects in a larger cohort of patients with neck pain of both non-traumatic and traumatic origins. Moreover, future studies should use lightweight glasses for the application of VR, and should explore the potential effects of VR concerning kinesiophobia.
The authors would like to thank the Fraunhofer-Institut für Graphische Datenverarbeitung, Darmstadt for software development and support.
We thank the research assistants Lena Tepohl and Angelina Knoll for their help with data collection for outcome measures.
The authors have no conflicts of interest to declare.
1. Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world population: a systematic critical review of the literature. Eur Spine J 2006; 15: 834-848.
DOI:
https://doi.org/10.1007/s00586-004-0864-4
2. Hogg-Johnson S, van der Velde G, Carroll LJ, Holm LW, Cassidy JD, Guzman J, et al. The burden and determinants of neck pain in the general population: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine 2008; 33 Suppl 4: S39-S51.
DOI:
https://doi.org/10.1097/BRS.0b013e31816454c8
3. Côté P, Wong JJ, Sutton D, Shearer HM, Mior S, Randhawa K, et al. Management of neck pain and associated disorders: a clinical practice guideline from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur Spine J 2016; 25: 2000-2022.
DOI:
https://doi.org/10.1007/s00586-016-4467-7
4. Röijezon U, Björklund M, Djupsjöbacka M. The slow and fast components of postural sway in chronic neck pain. Man Ther 2011; 16: 273-278.
DOI:
https://doi.org/10.1016/j.math.2010.11.008
5. Stenneberg MS, Rood M, de Bie R, Schmitt MA, Cattrysse E, Scholten-Peeters GG. To what degree does active cervical range of motion differ between patients with neck pain, patients with whiplash, and those without neck pain? a systematic review and meta-analysis. Arch Phys Med Rehabil 2017; 98: 1407-1434.
DOI:
https://doi.org/10.1016/j.apmr.2016.10.003
6. Jull G, Kristjansson E, Dall'Alba P. Impairment in the cervical flexors: a comparison of whiplash and insidious onset neck pain patients. Man Ther 2004; 9: 89-94.
DOI:
https://doi.org/10.1016/S1356-689X(03)00086-9
7. Côté P, van der Velde G, David Cassidy J, Carroll LJ, Hogg-Johnson S, Holm LW, et al. The burden and determinants of neck pain in workers. Eur Spine J 2008; 17 Suppl 1: S60-S74.
DOI:
https://doi.org/10.1007/s00586-008-0626-9
8. Allen D, Hines EW, Pazdernik V, Konecny LT, Breitenbach E. Four-year review of presenteeism data among employees of a large United States health care system: a retrospective prevalence study. Hum Resour Health 2018; 16: 59.
DOI:
https://doi.org/10.1186/s12960-018-0321-9
9. Sterling M, de Zoete RMJ, Coppieters I, Farrell SF. Best evidence rehabilitation for chronic pain part 4: neck pain. J Clin Med 2019; 8: 1219.
DOI:
https://doi.org/10.3390/jcm8081219
10. Sarig Bahat H, Takasaki H, Chen X, Bet-Or Y, Treleaven J. Cervical kinematic training with and without interactive VR training for chronic neck pain - a randomized clinical trial. Man Ther 2015; 20: 68-78.
DOI:
https://doi.org/10.1016/j.math.2014.06.008
11. Röijezon U, Björklund M, Bergenheim M, Djupsjöbacka M. A novel method for neck coordination exercise--a pilot study on persons with chronic non-specific neck pain. J Neuroeng Rehabil 2008; 5: 36.
DOI:
https://doi.org/10.1186/1743-0003-5-36
12. Sarig Bahat H, Croft K, Carter C, Hoddinott A, Sprecher E, Treleaven J. Remote kinematic training for patients with chronic neck pain: a randomised controlled trial. Eur Spine J 2018; 27: 1309-1323.
DOI:
https://doi.org/10.1007/s00586-017-5323-0
13. Revel M, Minguet M, Gregoy P, Vaillant J, Manuel JL. Changes in cervicocephalic kinesthesia after a proprioceptive rehabilitation program in patients with neck pain: a randomized controlled study. Arch Phys Med Rehabil 1994; 75: 895-899.
DOI:
https://doi.org/10.1016/0003-9993(94)90115-5
14. Jull G, Falla D, Treleaven J, Hodges P, Vicenzino B. Retraining cervical joint position sense: the effect of two exercise regimes. J Orthop Res 2007; 25: 404-412.
DOI:
https://doi.org/10.1002/jor.20220
15. Treleaven J. Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control. Man Ther 2008; 13: 2-11.
DOI:
https://doi.org/10.1016/j.math.2007.06.003
16. Humphreys BK, Irgens PM. The effect of a rehabilitation exercise program on head repositioning accuracy and reported levels of pain in chronic neck pain subjects. J Whiplash Relat Dis 2002; 1: 99-112.
DOI:
https://doi.org/10.3109/J180v01n01_09
17. McCaskey MA, Schuster-Amft C, Wirth B, Suica Z, de Bruin ED. Effects of proprioceptive exercises on pain and function in chronic neck- and low back pain rehabilitation: a systematic literature review. BMC Musculoskelet Disord 2014; 15: 382.
DOI:
https://doi.org/10.1186/1471-2474-15-382
18. Rudolfsson T, Djupsjöbacka M, Häger C, Björklund M. Effects of neck coordination exercise on sensorimotor function in chronic neck pain: a randomized controlled trial. J Rehabil Med 2014; 46: 908-914.
DOI:
https://doi.org/10.2340/16501977-1869
19. Kramer M, Honold M, Hohl K, Bockholt U, Rettig A, Elbel M, et al. Reliability of a new virtual reality test to measure cervicocephalic kinaesthesia. J Electromyogr Kinesiol 2009; 19: e353-e361.
DOI:
https://doi.org/10.1016/j.jelekin.2008.05.005
20. Hoffman HG, Richards TL, Van Oostrom T, Coda BA, Jensen MP, Blough DK, et al. The analgesic effects of opioids and immersive virtual reality distraction: evidence from subjective and functional brain imaging assessments. Anesth Analg 2007; 105: 1776-1783.
DOI:
https://doi.org/10.1213/01.ane.0000270205.45146.db
21. Yilmaz Yelvar GD, Çırak Y, Dalkılınç M, Parlak Demir Y, Guner Z, Boydak A. Is physiotherapy integrated virtual walking effective on pain, function, and kinesiophobia in patients with non-specific low-back pain? Randomised controlled trial. Eur Spine J 2017; 26: 538-545.
DOI:
https://doi.org/10.1007/s00586-016-4892-7
22. Bryanton C, Bossé J, Brien M, McLean J, McCormick A, Sveistrup H. Feasibility, motivation, and selective motor control: virtual reality compared to conventional home exercise in children with cerebral palsy. Cyberpsychol Behav 2006; 9: 123-128.
DOI:
https://doi.org/10.1089/cpb.2006.9.123
23. Costa MTS, Vieira LP, Barbosa E de O, Mendes Oliveira L, Maillot P, Ottero Vaghetti CA, et al. Virtual reality-based exercise with exergames as medicine in different contexts: a short review. Clin Pract Epidemiol Ment Health 2019; 15: 15-20.
DOI:
https://doi.org/10.2174/1745017901915010015
24. Revel M, Andre-Deshays C, Minguet M. Cervicocephalic kinesthetic sensibility in patients with cervical pain. Arch Phys Med Rehabil 1991; 72: 288-291.
25. Loudon JK, Ruhl M, Field E. Ability to reproduce head position after whiplash injury. Spine 1997; 22: 865-868.
DOI:
https://doi.org/10.1097/00007632-199704150-00008
26. Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs 2005; 14: 798-804.
DOI:
https://doi.org/10.1111/j.1365-2702.2005.01121.x
27. Cleland JA, Childs JD, Whitman JM. Psychometric properties of the Neck Disability Index and Numeric Pain Rating Scale in patients with mechanical neck pain. Arch Phys Med Rehabil 2008; 89: 69-74.
DOI:
https://doi.org/10.1016/j.apmr.2007.08.126
28. Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther 1991; 14: 409-415.
DOI:
https://doi.org/10.1037/t35122-000
29. Vernon H. The Neck Disability Index: state-of-the-art, 1991-2008. J Manipulative Physiol Ther 2008; 31:491-502.
DOI:
https://doi.org/10.1016/j.jmpt.2008.08.006
30. Jorritsma W, Dijkstra PU, de Vries GE, Geertzen JHB, Reneman MF. Detecting relevant changes and responsiveness of Neck Pain and Disability Scale and Neck Disability Index. Eur Spine J 2012; 21: 2550-2557.
DOI:
https://doi.org/10.1007/s00586-012-2407-8
31. R Foundation for Statistical Computing, Vienna, Austria. R Core Team: a language and environment for statistical computing. 2012 [cited 2020 Nov 18]. Available from:
http://www.R-project.org/.
32. Hedges L, Olkin I. Statistical methods for meta-analysis. New York: Academic Press; 1985.
33. Cohen J. Statistical power analysis for the behavioral sciences. 2nd edn. New York: Lawrence Erlbaum Associates; 1988.
34. Panjabi MM. A hypothesis of chronic back pain: ligament subfailure injuries lead to muscle control dysfunction. Eur Spine J 2006; 15: 668-676.
DOI:
https://doi.org/10.1007/s00586-005-0925-3
35. Sarig Bahat H, Weiss PL, Laufer Y. Cervical motion assessment using virtual reality. Spine 2009; 34: 1018-1024.
DOI:
https://doi.org/10.1097/BRS.0b013e31819b3254
36. Heikkilä HV, Wenngren BI. Cervicocephalic kinesthetic sensibility, active range of cervical motion, and oculomotor function in patients with whiplash injury. Arch Phys Med Rehabil 1998; 79: 1089-1094.
DOI:
https://doi.org/10.1016/S0003-9993(98)90176-9
37. Kristjansson E, Dall'Alba P, Jull G. A study of five cervicocephalic relocation tests in three different subject groups. Clin Rehabil 2003; 17: 768-774.
DOI:
https://doi.org/10.1191/0269215503cr676oa
38. Kristjansson E, Oddsdottir GL. "The Fly": a new clinical assessment and treatment method for deficits of movement control in the cervical spine: reliability and validity. Spine 2010; 35: E1298-1305.
DOI:
https://doi.org/10.1097/BRS.0b013e3181e7fc0a
39. Chen KB, Sesto ME, Ponto K, Leonard J, Mason A, Vanderheiden G, et al. Use of virtual reality feedback for patients with chronic neck pain and kinesiophobia. IEEE Trans Neural Syst Rehabil Eng 2017; 25: 1240-1248.
DOI:
https://doi.org/10.1109/TNSRE.2016.2621886
40. Luque-Suarez A, Martinez-Calderon J, Falla D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: a systematic review. Br J Sports Med 2019; 53: 554-559.
DOI:
https://doi.org/10.1136/bjsports-2017-098673