ORIGINAL REPORT
IMPROVED FUNCTIONAL ORAL INTAKE AND EXERCISE TRAINING ATTENUATE DECLINE IN AEROBIC CAPACITY FOLLOWING CHEMORADIOTHERAPY IN PATIENTS WITH OESOPHAGEAL CANCER
Shu-Chun HUANG, MD PhD1-3, Lan-Yan YANG, PhD4,5, Yin-Kai CHAO, MD PhD6, Wei-Yang CHANG, MS4, Ya-Tzu TSAO, MS7, Chuan-Yi CHOU, MD2, Ching-Chung HSIAO8 and Chien-Hung CHIU, MD6
From the 1Department of Physical Medicine and Rehabilitation, New Taipei Municipal Tucheng Hospital, Chang Gung Memorial Hospital, New Taipei City, 2Department of Physical Medicine & Rehabilitation, Chang Gung Memorial Hospital, Linkou, Taoyuan, 3College of Medicine, Chang Gung University, Kwei-Shan, Tao-Yuan County, 4Clinical Trial Center, Chang Gung Memorial Hospital, Taoyuan, 5Division of Clinical Trial, Taichung Veterans General Hospital, Taichung, 6Division of Thoracic Surgery, Chang Gung Memorial Hospital, Linkou, Taoyuan, 7Department of Medical Nutrition Therapy, Chang Gung Memorial Hospital, Linkou, Taoyuan, and 8Department of Nephrology, New Taipei Municipal Tucheng Hospital, Chang Gung Memorial Hospital, New Taipei City, Taiwan
Purpose: To investigate the impact of chemoradiotherapy on the physical fitness of patients with oesophageal cancer, and the clinical factors influencing it.
Method: A total of 67 participants successfully completed the study, with 18 of them engaging in supervised, in-hospital aerobic training at moderate intensity for a minimum of 20 sessions. Cardiopulmonary exercise testing, hand grip strength, body composition assessed via bioelectrical impedance analysis, patient-generated subjective global assessment, albumin, and the Functional Oral Intake Scale (FOIS) were evaluated before chemoradiotherapy and 6–8 weeks after its completion.
Result: Among the participants, cardiopulmonary fitness, hand grip strength, and phase angle of BC-BIA declined during chemoradiotherapy. Before and after chemoradiotherapy, V̇O2peak was 19.6 ± 4.4 and 17.4 ± 3.9 mL/min/kg respectively. The improvement in FOIS during chemoradiotherapy showed a positive correlation with changes in aerobic capacity. Additionally, exercise training was associated with attenuating the decline in aerobic capacity.
Conclusion: Physical fitness deteriorated in patients with oesophageal cancer following chemoradiotherapy. Improvement in dysphagia helps maintain aerobic capacity. Additionally, exercise training has the potential to mitigate the decline. This discovery can serve as a reference for enhancing holistic care for patients with oesophageal cancer.
LAY ABSTRACT
After treatment with chemoradiotherapy, patients with oesophageal cancer often find that their aerobic fitness, hand grip strength, and certain body composition measurements like phase angle decrease. These effects can last for at least 6–8 weeks after treatment. Interestingly, the present study suggests that as swallowing function gets better, so does aerobic capacity, which is a new finding. Doing structured exercise during chemoradiotherapy, such as 20 sessions of moderate-intensity workouts lasting 30 min each, might also stop aerobic capacity from dropping too much.
Key words: chemoradiotherapy; fitness; prehabilitation; swallowing; nutrition.
Citation: J Rehabil Med 2024; 56: jrm25906. DOI: https://doi.org/10.2340/jrm.v56.25906.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Submitted: Nov 17, 2023; Accepted after revision: Aug 20, 2024; Published: Oct 18, 2024.
Correspondence address: Dr Chien-Hung Chiu, MD. Division of Thoracic Surgery, Chang Gung Memorial Hospital, Linkou, Taoyuan, No.5, Fuxing St., Guishan Dist., Taoyuan City 333, Taiwan (R.O.C.). E-mail address: b9102067@cgmh.org.tw
Competing interests and funding: The authors have no conflicts of interest to declare.
Oesophageal cancer constitutes a highly lethal ailment with a poor long-term survival rate. However, since the implementation of multimodality therapy, the prognosis for oesophageal cancer patients has shown significant improvement (1, 2). The integration of various therapeutic approaches, including chemoradiotherapy (CRT), has played a pivotal role in enhancing the outcomes of advanced oesophageal cancer. In the case of locally advanced oesophageal cancer, the standard therapeutic approach involves neoadjuvant CRT (nCRT) followed by oesophagectomy, with curative intent for patients deemed suitable for surgery (3, 4). On the other hand, definitive CRT (dCRT) stands as an alternative curative treatment strategy for patients diagnosed with cervical oesophageal cancer or those who are not suitable candidates for surgical interventions (3, 5).
Nonetheless, CRT could have an unfavourable effect on physical fitness, encompassing cardiopulmonary fitness, muscle strength, and body composition (6–9). Literature regarding the impact of nCRT on physical fitness is inconsistent. Most studies showed that exercise capacity declined during nCRT (8–13). The regression persists even immediately before oesophagectomy, which is about 4–6 weeks after completion of nCRT (8, 11, 12). On the other hand, 2 studies reported that exercise capacity was not changed after nCRT (14, 15). The discrepant result may result from relatively small sample size, which ranged from 21 to 56 participants in the aforementioned 8 studies. Among these, 2 studies further showed that prehabilitation attenuated the declining trend of exercise capacity during nCRT (8, 9). However, only 6-min-walk distance (6MWD), a submaximal testing, was used as the measure of cardiopulmonary fitness. Moreover, factors that influence the change in physical fitness during CRT have not been investigated.
Accordingly, in the present study, to address the contradictory findings, a larger sample size was implemented to investigate whether CRT has a negative impact on physical fitness. Cardiopulmonary exercise testing by gas analysis (CPET), the gold-standard measure of cardiopulmonary fitness, was used to determine the magnitude of the impact of CRT on aerobic capacity. In-hospital supervised exercise training was facilitated. Hand grip strength (HGS), body composition by bioelectrical impedance analysis (BC-BIA), functional oral intake scale (FOIS), and nutritional status were also evaluated. We hypothesized that physical fitness would deteriorate during CRT, and that improvements in nutritional status, swallowing function, and exercise training could attenuate this decline.
METHODOLOGY
Participants and design
The patients were evaluated for eligibility based on the following criteria: (i) age 20 years or older, (ii) a diagnosis of oesophageal cancer, and (iii) having a planned course of concurrent chemoradiotherapy (CRT) with curative intent, including oesophagectomy after neoadjuvant chemoradiotherapy (nCRT) and definitive chemoradiotherapy (dCRT). Exclusion criteria included comorbid medical, physical, and mental conditions that contraindicate exercise, acute or unstable cardiac conditions (such as unstable angina or symptomatic severe aortic stenosis), disabling orthopaedic or neuromuscular diseases, and dementia (16).
A total of 138 patients diagnosed with oesophageal cancer who underwent oesophagectomy after receiving neoadjuvant chemoradiotherapy (nCRT) or definitive chemoradiotherapy (dCRT) at Chang Gung Memorial Hospital in Linkou, Taiwan, between February 2020 and February 2023, were screened. After excluding individuals who had contraindications for exercise testing or those who could not ride on the stationary cycle ergometer (n = 19), and those who declined to participate in the study (n = 47), a total of 72 patients were eligible for inclusion in our analysis.
The assessment of physical fitness and nutrition occurred at 2 specific time points: initially at baseline and 6–8 weeks after the completion of chemoradiotherapy (CRT). Every patient received comprehensive explanations regarding the exercise training programme as an integral part of the protocol. The participants decided whether to join the exercise training programme based on their own will. The study protocol was approved by the Institutional Review Board of Chang Gung Memorial Hospital.
Exercise training programme
The exercise protocol was a hospital-based supervised programme comprising aerobic training by cycle ergometer. The participants attended the rehabilitation centre 5 times a week to undergo exercise therapy, typically scheduled on the day before or after their radiotherapy sessions. Exercise sessions might be temporarily halted on the day or for several days following chemotherapy if patients were unable to tolerate training. The intensity was set initially at ventilatory anaerobic threshold and gradually titrated up to respiratory compensatory point based on the breath-by-breath cardiopulmonary exercise testing. The duration was 30 min per session plus 5-min warm-up and 5-min cool-down. Those who decided to participate in the exercise training programme were required to complete a minimum of 20 sessions in total.
Cardiopulmonary exercise testing
A symptom-limited incremental exercise test was performed in the upright position on a calibrated bicycle ergometer (Ergoselect 150P; ergoline GmbH, Bitz, Germany) to assess aerobic fitness and haemodynamic function. CPET was performed 2–4 h after a light meal. It began with 2 min of rest and 1 min of warm-up at 10 W, followed by a ramp increase of 10 W every min, until exhaustion. Minute ventilation (V̇E), oxygen consumption (V̇O2), and carbonic dioxide production (V̇CO2) were measured breath-by-breath using a computer-based system (MasterScreen CPX, Cardinal Health, Halberstadt, Germany). The data were averaged every 15 s. Four parameters were employed to assess the ventilation efficiency: (i) EqCO2nadir refers to the smallest value of ventilatory equivalent for CO2 (V̇E /V̇CO2) during incremental exercise testing (17); (ii) oxygen uptake efficiency slope (OUES) was derived from the slope of V̇O2 vs natural logarithm of V̇E, OUES is an estimation of the efficiency of ventilation with respect to V̇O2, with a greater slope indicating higher oxygen uptake efficiency (18); (iii) the V̇E –V̇CO2 slope was calculated as Y mX+b, where Y is V̇E, X is V̇CO2, and m is the slope. V̇E and V̇CO2 were acquired from the initiation of exercise to the peak values. A more horizontal slope suggests better ventilation efficiency (19). Heart rate (HR) was determined from the R–R interval on a 12-lead electrocardiogram, arterial pressure was measured using an automatic blood pressure system (Tango, SunTech Medical, Eynsham, UK), and arterial O2 saturation was monitored using finger pulse-oximetry (model 9500, Nonin Onyx, Plymouth, MA, USA). The exercise test was terminated using the following criteria: (1) the subject could not keep up with the pedalling frequency to 50 rpm; (2) the participant reached volitional fatigue and was requested to end the test; (3) the participant’s peak V̇O2 plateaued or decreased despite the continuation of exercise, or (4) an adverse cardiovascular event was observed. Ventilatory anaerobic threshold (VAT) was determined primarily by the V-slope method and verified based on ventilatory criteria as follows: (i) departure from linearity for V̇CO2 against V̇O2, (ii) the V̇E-V̇O2 ratio increased without a corresponding increase in the V̇E–V̇CO2 ratio and (iii) end-tidal tensions of oxygen increases without a corresponding decrease in end-tidal tensions of carbon dioxide (20). VAT was identified by 2 independent reviewers.
Body composition
Whole-body composition was determined using InBody s10 (Seoul, Korea) and by measuring the electrical resistance to 4 different frequencies (5, 50, 250, and 500 kHz) (21, 22). Each participant remained seated upright on a non-conductive chair throughout the entire testing duration. The sensors measuring electrical resistance were placed at the level of each body segment following the manufacturer instructions. To undergo this 10-min procedure, participants were instructed to fast for 2 h prior to the test. Appendicular skeletal muscle index (ASMI), body cell mass (BCM), fat free mass (FFM), lean body mass (LBM), phase angle (PA), and body fat percentage (BF) were recorded.
Nutrition assessment
The nutrition assessments comprised bodyweight (BW), albumin blood levels, and the Patient-Generated Subjective Global Assessment (PGSGA). PGSGA is a nutritional evaluation tool designed for cancer patients, with a higher score indicating a greater risk of malnutrition (23). The PG-SGA assessments were conducted by a specialized dietitian.
Functional oral intake scale
The Functional Oral Intake Scale (FOIS) is a validated tool used to evaluate the functional oral intake status of individuals with dysphagia (24, 25). FOIS categorizes individuals into 7 levels, reflecting their capacity to safely and effectively consume food and liquids by mouth. 1 = No oral intake; 2 = Tube dependent with minimal/inconsistent oral intake; 3 = Tube supplements with consistent oral intake; 4 = Total oral intake of a single consistency; 5 = Total oral intake of multiple consistencies requiring special preparation; 6 = Total oral intake with no special preparation, but must avoid specific foods, 7 = Total oral intake with no restrictions.
Statistics
The data were expressed as the mean ± standard deviation and were analysed using IBM SPSS Statistics 22.0 (IBM Corp, Armonk, NY, USA). In the comparison between participants who underwent supervised exercise training with those who did not (received usual care), the χ2 test was used to analyse the correlation between categorical variables, while the independent t-test was used for continuous variables. A paired t-test was employed to compare the pre- and post-CRT statuses. Additionally, univariate and multivariate forward linear stepwise regression analyses were conducted to identify parameters correlating with the change in V̇O2peak (mL/min) (Δ V̇O2peak = V̇O2peak at post-CRT - V̇O2peak at pre-CRT). Independent variables with p-value < 0.1 in the univariate analysis were included in the multivariate linear stepwise regression. “Δ” represents the difference between the post-CRT value and the pre-CRT status value. The criterion for significance was p-value < 0.05.
RESULTS
Five dropped out due to their reluctance to return of their own volition. Ultimately, 67 participants successfully completed the study. Forty-eight patients received nCRT and 19 patients underwent dCRT. Eighteen participated in the supervised exercise training programme (Table I). Among them, no exercise-related adverse events were reported and the adherence rate was 100%. No significant difference was found in the basic data between participants who underwent supervised exercise training and those who did not (received usual care) (Table I).
All the cardiopulmonary fitness-related parameters, whether derived from peak or submaximal status, showed a decline in the post-CRT condition compared with the pre-CRT, persisting even 6–8 weeks after the completion of CRT (Table II). Specifically, VO2peak decreased from 19.6 ± 4.4 to 17.4 ± 3.9 mL/min/kg and HGS also declined at 41.7 ± 7.9 vs 39.6 ± 8.6 kg. Regarding BC-BIA, the PA exhibited deterioration in all 4 limbs and the trunk following CRT. However, ASMI, BCM, FFM, LBM, and BF remain unchanged. In terms of nutritional status, PGSGA showed improvement. Conversely, albumin levels exhibited a declining trend with marginal significance (Table II).
To identify the parameters correlated with Δ V̇O2peak (mL/min), those with a p-value less than 0.1 in the univariate linear analysis were included in the multivariate linear stepwise regression. These parameters encompass exercise training, preV̇O2peak (mL/min), preVO2peak (mL/min/kg), preAT (mL/min), preEqO2@AT, preOUES, Δ HGS (kg), Δ FOIS, and Δ ASMI (kg/m2). When they were entered into the multivariate forward linear stepwise regression model, 3 of them exhibited a significant regression coefficient: preV̇O2peak (mL/min), exercise training, and Δ FOIS (Table III).
| Parameter | Univariate model (n = 67) | Multivariate model (n = 67) | ||
| Model coefficient B (95% CI) | p-value | Model coefficient (95% CI) | p-value | |
| Sex | –151.557 (–460.863, 157.749) | 0.331 | ||
| Age (year) | –2.315 (–9.344, 5.073) | 0.556 | ||
| PreBMI (kg/m2) | –11.281 (–25.579, 3.017) | 0.120 | ||
| PreBW (kg) | –1.85 (–6.073, 2.374) | 0.385 | ||
| RTO dose | 15.019 (–106.774, 136.813) | 0.806 | ||
| CT regimen | –15.870 (–133.440, 101.700) | 0.788 | ||
| CRT goal | –1.474 (–121.093, 118.144) | 0.980 | ||
| CRT response | –31.01 (–226.573, 164.553) | 0.752 | ||
| Subsequent oesophagectomy | –45.181 (–153.411, 63.049) | 0.407 | ||
| Exercise training | –117.059 (–233.111, 1.008) | 0.048 | –148.552 (–244.736, –52.368) | 0.003 |
| PreV̇O2peak (mL/min) | –3.22 (–4.61, –0.183) | < 0.001 | –0.339 (–0.467, –0.211) | < 0.001 |
| PreVO2peak (mL/min/kg) | –18.885 (–28.626, –9.144) | < 0.001 | ||
| PreAT (mL/min) | –3.90 (–0.678, –0.102) | 0.009 | ||
| PreAT (mL/min/kg) | –14.715 (–33.368, 3.938) | 0.120 | ||
| PreEqO2@AT | 10.389 (–0.952, 21.731) | 0.072 | ||
| PreEqCO2nadir | 7.998 (–2.557, 18.553) | 0.135 | ||
| PreOUES | –0.623 (–0.974, –0.271) | 0.001 | ||
| PreV’E-V’CO2 slope | 4.399 (–5.869, 14.667) | 0.395 | ||
| PreHGS (kg) | –2.299 (–9.033, 4.434) | 0.498 | ||
| Δ HGS (kg) | 10.685 (0.018, 21.352) | 0.050 | ||
| PreBW (kg) | –1.85 (–6.073, 2.374) | 0.385 | ||
| PrePGSGA | –1.047 (–17.163, 15.069) | 0.897 | ||
| Δ PGSGA | –8.347 (–19.231, 2.538) | 0.130 | ||
| PreFOIS | –7.654 (–25.573, 10.264) | 0.397 | ||
| Δ FOIS | 63.997 (27.720, 100.274) | 0.001 | 41.060 (9.596, 72.524) | 0.011 |
| PreAlbumin (g/dL) | –15.347 (–71.281, 40.587) | 0.586 | ||
| Δ Albumin (g/dL) | 36.568 (–86.511, 159.648) | 0.555 | ||
| PreASMI (kg/m2) | –19.248 (–51.839, 13.344) | 0.243 | ||
| Δ ASMI (kg/m2) | 114.412 (–1.956, 230.781) | 0.054 | ||
| PreBCM (kg) | –3.270 (–10.050, 3.509) | 0.339 | ||
| Δ BCM (kg) | –9.522 (–23.688, 4.644) | 0.184 | ||
| PreBCM/BW | –57.814 (–590.022, 474.393) | 0.829 | ||
| Δ BCM/BW | –674.841 (–1707.248, 516.943) | 0.196 | ||
| PrePARA | –20.858 (–61.995, 20.279) | 0.315 | ||
| Δ PARA | –2.291 (–11.003, 6.420) | 0.601 | ||
| PrePALA | –26.249 (–68.351, 15.853) | 0.218 | ||
| Δ PALA | 49.789 (–41.816, 141.394) | 0.281 | ||
| PrePATR | –3.283 (–27.251, 20.686) | 0.785 | ||
| Δ PATR | 6.774 (–30.227, 43.775) | 0.716 | ||
| PrePARL | –20.858 (–61.995, 20.279) | 0.315 | ||
| Δ PARL | 25.891 (–52.187, 003.969) | 0.510 | ||
| PrePALL | –26.249 (–68.351, 15.853) | 0.218 | ||
| Δ PALL | 38.432 (–38.422, 115.286) | 0.321 | ||
| Prebody fat (%) | –4.007 (–10.871, 2.857) | 0.248 | ||
| Δ body fat (%) | 1.374 (–12.010, 14.757) | 0.838 | ||
| Dependent variable = Δ V̇O2peak = VO2peak at post-CRT –V̇O2peak at pre-CRT (mL/min). “Pre” indicates before CRT; “Δ” represents the difference between the post-CRT value and the pre-CRT status value. Other abbreviations are as described in Tables I and II. |
||||
Fig. 1A illustrates that an improvement in Δ FOIS correlates with a positive change in Δ V̇O2peak. After CRT, among the minority (19/67, 28%) who experienced an increase in V̇O2peak, nearly all demonstrated improvement in Δ FOIS (18/19, 95%, first quadrant), with only 1 exception (1/19, second quadrant). Fig. 1B demonstrates that exercise training is associated with a reduction in the declining trend following CRT. Additionally, a higher preV̇O2peak is correlated with a larger negative change in Δ is 2peak.
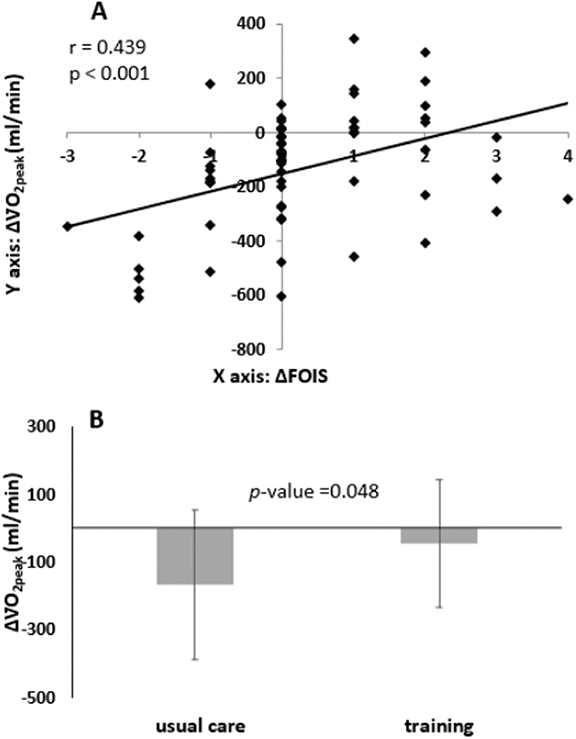
Fig. 1. (A) An improvement in Δ FOIS is associated with a positive change in ΔV̇O2peak. (B) Exercise training correlates with a decline in Δ V̇O2peak during CRT. Usual care vs training V̇O2peak = –168 ± 222 vs –47 ± 189 (mL/min); –2.4 ± 3.4 vs –1.0 ± 2.4 (mL/min/kg).
It is worth mentioning that, in this cohort, the following factors do not show an association with Δ V̇O2peak (mL/min): radiotherapy dose (> 4500 vs ≤ 4500 cGy), CT regimen (cisplatin+5-fluorouracil vs carboplatin+paclitaxel), CRT goal (neoadjuvant vs definitive), CRT response and whether subsequent oesophagectomy was performed.
DISCUSSION
The primary experimental findings can be summarized as follows. In patients with oesophageal cancer, cardiopulmonary fitness significantly declined following CRT, persisting for at least 6–8 weeks after the completion of CRT. The magnitude of VO2peak decrease (19.6 ± 4.4 vs 17.4 ± 3.9 mL/min/kg) in the present cohort is clinically significant. Interestingly, the improvement in FOIS during CRT is positively correlated with changes in cardiopulmonary fitness, a novel finding proposed by the present study. Following CRT, among the minority (28%) who experienced an increase in V̇O2peak, nearly all demonstrated improvement in Δ FOIS (95%). Meanwhile, the decline in aerobic capacity could potentially be attenuated by structured exercise training during CRT, which was well received by the participants. Additionally, CRT has an adverse impact on patients’ strength, as evidenced by HGS. BC-BIA indicated no significant changes in ASMI, BCM, FFM, or LBM after CRT. However, the phase angle for both the trunk and all 4 extremities showed an average decrease ranging from 0.4 to 0.6 degrees. Thus, PA is the most sensitive marker among the BC-BIA measurement to monitor the patient’s overall health and nutritional status in the oesophageal patients receiving CRT.
Influence of CRT
The literature on how cardiopulmonary fitness changes after CRT displays inconsistencies. While most studies suggested a decrease (8–13), a minority reported no significant change (14, 15). The current experimental findings align with the majority of previous research results. Furthermore, the current study demonstrates that recovery of aerobic capacity does not occur within 6–8 weeks after completing CRT. Consistent with these findings, prior studies also indicated that the observed decrease in AT, V̇O2peak or 6MWD following nCRT does not spontaneously improve after 4 weeks or 4–6 weeks following the completion of nCRT (8, 11, 12).
Elements from 3 domains (chemotherapy, radiotherapy, and cancer-related factors) can have a negative impact on physical fitness. In the present investigation, 2 combinations of chemotherapeutic agents were used: cisplatin+5-fluorouracil and carboplatin+paclitaxel. These can result in diminished cardiorespiratory fitness, primarily attributed to their impact on the cardiovascular and respiratory systems (10). Fatigue and anaemia are also common side effects in these 4 chemotherapy medications in the present study, ranging from 11~90% based on Micromedex®. Fluorouracil also has common side effect of anorexia. These treatments also influence cellular and mitochondrial metabolism. Cisplatin and paclitaxel were reported to alter the function of mitochondria, followed by disruption of respiratory chain function and increased production of reactive oxygen species (26). In addition, radiotherapy can result in radiation pneumonitis (27). Other than chemoradiotherapy effects, cancer-related factors such as poor nutrition and cancer cachexia may also contribute to deterioration of physical fitness.
Phase angle has been used as a marker of nutritional status, muscle mass and function, and cell integrity (28). Previous studies have shown a decrease in PA following chemotherapy in non-small-cell lung cancer (29) and breast cancer (30, 31). To the best of our knowledge, this study is the first to demonstrate that PA decreases following CRT in patients with oesophageal cancer, both in the trunk and in all 4 extremities. The average reduction magnitude ranges from 0.4 to 0.6 degrees. Conversely, no changes were noted in ASMI, BCM, FFM, or LBM, indicating that PA may serve as a more sensitive marker.
Functional Oral Intake Scale
The present finding indicates a significant association between Δ FOIS and Δ V̇O2peak. Improvement in swallowing function benefits physical fitness. It is important to note that other related indicators, such as CRT response, PGSGA, albumin, and BW, do not exhibit a similar correlation. Hence, FOIS is a convenient and valuable scale for evaluating swallowing function in oesophageal cancer patients. In a cross-sectional study by Matsuda et al., self-efficacy tended to increase as the FOIS improved in cancer patients (32). To the best of our knowledge from the literature search, this study is the first to utilize FOIS for quantifying clinical outcomes of dysphagia and demonstrating its value in oesophageal cancer patients (33–35).
Exercise training
Two published randomized clinical trials (RCT) have investigated exercise training during nCRT in patients with oesophageal cancer. In the first study (8), when compared with the control group (n = 25), prehabilitation (n = 26) effectively prevented a decline in the 6MWD. Prehabilitation encompassed aerobic moderate continuous training 3 times weekly, resistance training, and nutrition optimization. The median length of prehabilitation was 36 days (IQR 17–73 days). In the second RCT (9), a walk-and-eat intervention was employed, where participants in the intervention group completed an average of 8.4 ± 3.6 sessions of moderate-intensity walking before and after chemoradiation therapy over a span of 4–5 weeks of nCRT. Likewise, this intervention mitigated the decline in 6MWD and HGS when compared with the control group. In the 2 aforementioned studies, 6MWD, a submaximal test, was utilized to assess aerobic capacity. The result of the current study is similar to the 2 previous studies, but instead employed CPET, the gold standard for measuring cardiopulmonary fitness. BC-BIA and HGS were also incorporated to evaluate physical fitness comprehensively. Moreover, exercise training might also benefit postoperative morbidity (36). Future studies on multimodal prehabilitation are necessary to refine optimal programmes for patients with oesophagogastric cancer.
Nutrition
Malnutrition is common for oesophageal cancer patients due to a combination of mechanical obstruction and cancer cachexia. In the current cohort, PGSGA showed significant improvement following CRT, whereas there seemed to be a borderline decrease in albumin levels. This phenomenon is likely attributable to the nature of PGSGA, a patient-generated subjective score; a reduction in the score indicates a reduction in the risk of malnutrition. On the other hand, a decrease in albumin level does not necessarily indicate malnutrition. It has been reported that serum albumin concentration is not a useful marker for malnutrition (37). In our case, the oxidative and inflammatory stress generated by CRT can deplete serum albumin, leading to a decrease in albumin level (38). Therefore, PGSGA may improve more rapidly during CRT. In contrast, given albumin’s 22-day half-life and the impact of CRT, its blood levels may take some time to recover.
Limitation
The study has a limitation as it is a prospective observational study; the patients opted to participate in the exercise training programme, introducing potential selection bias when evaluating the impact of exercise training. However, the primary objective of the current study was to investigate diverse clinical factors associated with changes in aerobic capacity following CRT, going beyond the specific focus on exercise training alone.
Conclusion
Physical fitness of patients with oesophageal cancer, including cardiopulmonary fitness, HGS, and phase angle of body composition by bioelectrical impedance analysis, declined following CRT. The improvement in dysphagia during CRT is significantly positively correlated with changes in aerobic capacity. Additionally, the decline in aerobic capacity could potentially be attenuated by structured exercise training. This discovery can serve as a reference for enhancing holistic care for patients with oesophageal cancer focused on improving healthcare quality.
ACKNOWLEDGEMENTS
This research was funded by the National Science and Technology Council, Taiwan (grant no. MOST 109 - 2314 - B - 182A - 074 - MY3), and Chang Gung Memorial Hospital (grant no. CMRPVVL0121-3, CMRPVVK0111-3, CORPG5H0021 and Grant CLRPG3D0049).
The authors acknowledge the statistical assistance provided by the Clinical Trial Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan, which was funded by the Ministry of Health and Welfare of Taiwan (MOHW112-TDU-B-212-144005).
The data underlying the results presented in the study are available at https://cloudhd.cgmh.org.tw/navigate/a/#/s/A629F8CEDC73444091B6B0510B95A6696BL upon reasonable request.
REFERENCES
- Dubecz A, Gall I, Solymosi N, Schweigert M, Peters JH, Feith M, et al. Temporal trends in long-term survival and cure rates in esophageal cancer: a SEER database analysis. J Thorac Oncol 2012; 7: 443–447. https://doi.org/10.1097/JTO.0b013e3182397751
- Njei B, McCarty TR, Birk JW. Trends in esophageal cancer survival in United States adults from 1973 to 2009: A SEER database analysis. J Gastroenterol Hepatol 2016; 31: 1141–1146. https://doi.org/10.1111/jgh.13289
- Ajani JA, D’Amico TA, Bentrem DJ, Chao J, Corvera C, Das P, et al. Esophageal and esophagogastric junction cancers, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2019; 17: 855–883. https://doi.org/10.6004/jnccn.2019.0033
- van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med 2012; 366: 2074–2084. https://doi.org/10.1056/NEJMoa1112088
- Cooper JS, Guo MD, Herskovic A, Macdonald JS, Martenson JA Jr, Al-Sarraf M, et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA 1999; 281: 1623–1627. https://doi.org/10.1001/jama.281.17.1623
- Awad S, Tan BH, Cui H, Bhalla A, Fearon KC, Parsons SL, et al. Marked changes in body composition following neoadjuvant chemotherapy for oesophagogastric cancer. Clin Nutr 2012; 31: 74–77. https://doi.org/10.1016/j.clnu.2011.08.008
- Ida S, Watanabe M, Karashima R, Imamura Y, Ishimoto T, Baba Y, et al. Changes in body composition secondary to neoadjuvant chemotherapy for advanced esophageal cancer are related to the occurrence of postoperative complications after esophagectomy. Ann Surg Oncol 2014; 21: 3675–3679. https://doi.org/10.1245/s10434-014-3737-z
- Minnella EM, Awasthi R, Loiselle SE, Agnihotram RV, Ferri LE, Carli F. Effect of exercise and nutrition prehabilitation on functional capacity in esophagogastric cancer surgery: a randomized clinical trial. JAMA Surg 2018; 153: 1081–1089. https://doi.org/10.1001/jamasurg.2018.1645
- Xu YJ, Cheng JC, Lee JM, Huang PM, Huang GH, Chen CC. A walk-and-eat intervention improves outcomes for patients with esophageal cancer undergoing neoadjuvant chemoradiotherapy. Oncologist 2015; 20: 1216–1222. https://doi.org/10.1634/theoncologist.2015-0178
- Argudo N, Rodó-Pin A, Martínez-Llorens J, Marco E, Visa L, Messaggi-Sartor M, et al. Feasibility, tolerability, and effects of exercise-based prehabilitation after neoadjuvant therapy in esophagogastric cancer patients undergoing surgery: an interventional pilot study. Dis Esophagus 2021; 34: doaa086. https://doi.org/10.1093/dote/doaa086
- Jack S, West MA, Raw D, Marwood S, Ambler G, Cope TM, et al. The effect of neoadjuvant chemotherapy on physical fitness and survival in patients undergoing oesophagogastric cancer surgery. Eur J Surg Oncol 2014; 40: 1313–1320. https://doi.org/10.1016/j.ejso.2014.03.010
- Navidi M, Phillips AW, Griffin SM, Duffield KE, Greystoke A, Sumpter K, et al. Cardiopulmonary fitness before and after neoadjuvant chemotherapy in patients with oesophagogastric cancer. Br J Surg 2018; 105: 900–906. https://doi.org/10.1002/bjs.10802
- Sinclair R, Navidi M, Griffin SM, Sumpter K. The impact of neoadjuvant chemotherapy on cardiopulmonary physical fitness in gastro-oesophageal adenocarcinoma. Ann R Coll Surg Engl 2016; 98: 396–400. https://doi.org/10.1308/rcsann.2016.0135
- Drummond RJ, Vass D, Wadhawan H, Craig CF, MacKay CK, Fullarton GM, et al. Routine pre- and post-neoadjuvant chemotherapy fitness testing is not indicated for oesophagogastric cancer surgery. Ann R Coll Surg Engl 2018; 100: 515–519. https://doi.org/10.1308/rcsann.2018.0067
- Tatematsu N, Ezoe Y, Tanaka E, Muto M, Sakai Y, Tsuboyama T. Impact of neoadjuvant chemotherapy on physical fitness, physical activity, and health-related quality of life of patients with resectable esophageal cancer. Am J Clin Oncol 2013; 36: 53–56. https://doi.org/10.1097/COC.0b013e3182354bf4
- American College of Sports M, Riebe D, Ehrman JK, Liguori G, Magal M. ACSM’s guidelines for exercise testing and prescription. Tenth ed. Philadelphia: Wolters Kluwer Philadelphia; 2018.
- Wasserman K, Hansen J, Sue DY, Stringer W, Sietsema K, Sun X-G, et al. Principles of exercise testing and interpretation: including pathophysiology and clinical applications. Fifth ed. Philadelphia: Lippincott, Williams & Wilkins; 2011.
- Huang SC, Hsu CC, Fu TC, Chen CPC, Liao MF, Hsu CY, et al. Stepper-based training improves monocyte-platelet aggregation and thrombin generation in nonambulatory hemiplegic patients. Med Sci Sports Exerc 2022; 54: 821–829. https://doi.org/10.1249/MSS.0000000000002846
- Huang SC, Yeh CH, Hsu CC, Lin YC, Lee CH, Hsiao CC, et al. Trainability for cardiopulmonary fitness is low in patients with peripheral artery disease. Eur J Cardiovasc Nurs 2024; 23: 127–136. https://doi.org/10.1093/eurjcn/zvad044
- Whipp BJ, Ward SA, Wasserman K. Respiratory markers of the anaerobic threshold. Adv Cardiol 1986; 35: 47–64. https://doi.org/10.1159/000413438
- Morishita Y, Kubo K, Haga Y, Miki A, Ishibashi K, Kusano E, et al. Skeletal muscle loss is negatively associated with single-pool Kt/V and dialysis duration in hemodialysis patients. Ther Apher Dial 2014; 18: 612–617. https://doi.org/10.1111/1744-9987.12174
- Murakami K, Hirano H, Watanabe Y, Edahiro A, Ohara Y, Yoshida H, et al. Relationship between swallowing function and the skeletal muscle mass of older adults requiring long-term care. Geriatr Gerontol Int 2015; 15: 1185–1192. https://doi.org/10.1111/ggi.12572
- Bauer J, Capra S, Ferguson M. Use of the scored Patient-Generated Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with cancer. Eur J Clin Nutr 2002; 56: 779–785. https://doi.org/10.1038/sj.ejcn.1601412
- Crary MA, Mann GD, Groher ME. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch Phys Med Rehabil 2005; 86: 1516–1520. https://doi.org/10.1016/j.apmr.2004.11.049
- Kotz T, Federman AD, Kao J, Milman L, Packer S, Lopez-Prieto C, et al. Prophylactic swallowing exercises in patients with head and neck cancer undergoing chemoradiation: a randomized trial. Arch Otolaryngol Head Neck Surg 2012; 138: 376–382. https://doi.org/10.1001/archoto.2012.187
- Sorensen JC, Cheregi BD, Timpani CA, Nurgali K, Hayes A, Rybalka E. Mitochondria: inadvertent targets in chemotherapy-induced skeletal muscle toxicity and wasting? Cancer Chemother Pharmacol 2016; 78: 673–683. https://doi.org/10.1007/s00280-016-3045-3
- Tonison JJ, Fischer SG, Viehrig M, Welz S, Boeke S, Zwirner K, et al. Radiation pneumonitis after intensity-modulated radiotherapy for esophageal cancer: institutional data and a systematic review. Sci Rep 2019; 9: 2255. https://doi.org/10.1038/s41598-018-38414-5
- Conde Frio C, Härter J, Santos LP, Orlandi SP, Gonzalez MC. Phase angle, physical quality of life and functionality in cancer patients undergoing chemotherapy. Clin Nutr ESPEN 2023; 57: 331–336. https://doi.org/10.1016/j.clnesp.2023.07.017
- Detopoulou P, Tsiouda T, Pilikidou M, Palyvou F, Tsekitsidi E, Mantzorou M, et al. Changes in body weight, body composition, phase angle, and resting metabolic rate in male patients with stage IV non-small-cell lung cancer undergoing therapy. Medicina (Kaunas) 2022; 58: 1779. https://doi.org/10.3390/medicina58121779
- Ramos da Silva B, Mialich MS, Cruz LP, Rufato S, Gozzo T, Jordao AA. Performance of functionality measures and phase angle in women exposed to chemotherapy for early breast cancer. Clin Nutr ESPEN 2021; 42: 105–116. https://doi.org/10.1016/j.clnesp.2021.02.007
- Schmidt ME, Chong M, Klassen O, Wiskemann J, Steindorf K. Longitudinal associations of bioelectrical phase angle and fatigue in breast cancer patients. Int J Cancer 2023; 153: 1192–1200. https://doi.org/10.1002/ijc.34630
- Matsuda Y, Karino M, Kanno T. Relationship between the Functional Oral Intake Scale (FOIS) and the Self-Efficacy Scale among cancer patients: a cross-sectional study. Healthcare (Basel) 2020; 8: 269. https://doi.org/10.3390/healthcare8030269
- Liu D, Pickering T, Kokot N, Crookes P, Sinha UK, Swanson MS. Outcomes of combined antegrade-retrograde dilations for radiation-induced esophageal strictures in head and neck cancer patients. Dysphagia 2021; 36: 1040–1047. https://doi.org/10.1007/s00455-020-10236-6
- Sinha UK, Swanson MS, Villegas BC, Ouyoung LM, Kokot N. Outcomes of self-esophageal dilation for head and neck cancer patients. Am J Speech Lang Pathol 2019; 28: 1060–1066. https://doi.org/10.1044/2019_AJSLP-18-0190
- Vansant MB, Parker LA, McWhorter AJ, Bluoin D, Kunduk M. Predicting swallowing outcomes from objective videofluoroscopic timing and displacement measures in head and neck cancer patients. Dysphagia 2020; 35: 853–863. https://doi.org/10.1007/s00455-020-10091-5
- Bausys A, Mazeikaite M, Bickaite K, Bausys B, Bausys R, Strupas K. The role of prehabilitation in modern esophagogastric cancer surgery: a comprehensive review. Cancers (Basel) 2022; 14: 2096. https://doi.org/10.3390/cancers14092096
- Levitt DG, Levitt MD. Human serum albumin homeostasis: a new look at the roles of synthesis, catabolism, renal and gastrointestinal excretion, and the clinical value of serum albumin measurements. Int J Gen Med 2016; 9: 229–255. https://doi.org/10.2147/IJGM.S102819
- Wang CH, Ling HH, Liu MH, Pan YP, Chang PH, Lin YC, et al. Treatment-interval changes in serum levels of albumin and histidine correlated with treatment interruption in patients with locally advanced head and neck squamous cell carcinoma completing chemoradiotherapy under recommended calorie and protein provision. Cancers (Basel) 2022; 14: 3112. https://doi.org/10.3390/cancers14133112