ORIGINAL REPORT
IMMERSIVE VISUALIZATION OF MOVEMENT IN PATIENTS WITH HAEMOPHILIC ANKLE ARTHROPATHY: MULTICENTER, SINGLE-BLIND, RANDOMIZED CLINICAL TRIAL
Roberto UCERO-LOZANO, PhD1,2, Raúl PÉREZ-LLANES, PhD2,3, Rubén CUESTA-BARRIUSO, PhD2,4 and Elena DONOSO-ÚBEDA, PhD2,5
1Department of Physiotherapy, European University of Madrid, Madrid, 2InHeFis Research Group, Instituto Asturiano de Investigación Sanitaria (ISPA), Oviedo, 3Department of Physiotherapy, University of Murcia, Murcia, 4Department of Surgery and Medical-Surgical Specialties, University of Oviedo, Oviedo, and 5Department of Physiotherapy, Catholic University San Antonio-UCAM, Murcia, Spain
Objective: To evaluate the efficacy of immersive movement observation in adult patients with haemophilic ankle arthropathy.
Design: Multicentre, single-blind, randomized clinical trial.
Subjects: 48 patients with haemophilia.
Methods: Patients were randomly allocated to 2 groups (180º immersive video-based visualization of movement and a control group with no intervention). Twenty-eight consecutive 15-min home sessions, 1 per day, of immersive visualization of ankle flexion–extension movement were carried out. Three evaluations were performed: pretreatment (T0), post-intervention (T1), and at 16 weeks’ follow-up (T2). The primary variable was joint-pain intensity (visual analogue scale). The secondary variables were conditioned pain modulation (Conditioned Pain Modulation Index), pressure pain threshold (pressure algometer), range of motion (goniometry) and kinesiophobia (Tampa Scale of Kinesiophophia).
Results: There were intergroup differences in pain intensity (F = 37.14; p < 0.001), conditioned pain modulation (F = 5.40; p = 0.006), and dorsal (F = 19.17; p < 0.001) and plantar (F = 9.27; p<0.001) ankle flexion. More than 50% of experimental group patients exhibited changes exceeding the minimum detectable change in pain intensity (MDC = 0.43), and the pressure pain threshold in the extensor carpi radialis longus muscle (MDC = 1.34) and malleolus (MDC = 4.93).
Conclusions: 180º immersive video-based visualization of movement can improve the intensity of pain, conditioned pain modulation, and ankle range of motion in patients with haemophilic ankle arthropathy.
LAY ABSTRACT
Patients with haemophilia have a congenital coagulation problem. The most severe cases can have spontaneous bleeding that affects muscles and joints. Many of them suffer joint degeneration (haemophilic arthropathy) and chronic pain. Pain occurs in the brain like an alarm response and provokes cerebral changes. Indeed, this is the reason why we can use a virtual reality approach to treating pain. In this study we compare the effects of adding 15 min of seeing a movement wearing virtual reality googles in comparison with continuation of patients’ life for 28 days in patients with ankle haemophilic arthropathy. We evaluated before and after the 28 days, and 16 weeks after finishing the treatment. The results of this study show that this treatment can improve the intensity of pain perceived by patients and their ankle mobility in patients with haemophilic ankle arthropathy.
Key words: haemophilia; virtual reality exposure therapy; joint pain; conditioned pain modulation; pressure pain threshold; range of motion.
Citation: J Rehabil Med 2024; 56: jrm40775. DOI: https://doi.org/10.2340/jrm.v56.40775
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Submitted: May 13, 2024; Accepted after revision: Sept 8, 2024; Published: Sep 30, 2024
Correspondence address: Rubén Cuesta-Barriuso. Department of Surgery and Medical-Surgical Specialties, Faculty of Medicine, University of Oviedo, El Cristo Campus, ES-33006, Oviedo, Spain. E-mail: cuestaruben@uniovi.es.
Competing interests and funding: The authors have no conflicts of interest to declare.
Haemophilia is a chronic, congenital, and rare disease (1). Patients with haemophilia suffer from bleeding due to a deficiency of one of the clotting factors. The most common types of haemophilia are: haemophilia A (factor VIII deficiency) and haemophilia B (factor IX deficiency) (2). The severity of the disease is classified according to plasma levels of clotting factor: severe (<1%), moderate (1–5%), and mild (5–40%) (3).
Joint bleeding is characteristic of this disease (4). Such bleeding events can occur with minimal trauma (5). The joints most often affected are ankles, knees, and elbows (2). The recurrence of haemarthrosis causes changes in the synovial membrane that induce joint degeneration (haemophilic arthropathy) (5). The most disabling clinical features of this arthropathy include chronic pain and decreased joint range of motion (ROM), progressively leading patients to reduce their activity and social participation (4).
Pain is defined as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage” (6), beyond mere nociception. Acute pain is considered a failure of avoidance behaviour, transforming nociceptive activity into conscious pain. However, chronic pain lacks this physiological protective function (7).
Unhelpful beliefs concerning pain have developed, perceiving the body as something fragile and vulnerable, associating the experience of pain with structural damage. This evaluative bias perpetuates beliefs and fear of pain (8). This fear may seem useful to modify behaviours after an injury. However, it can be a source of long-term disability, if learning and exposure strategies are not offered to cope with fear. Learning can help the patient gain control over this process (8). Chronic pain of moderate intensity with peaks of severe pain is highly prevalent in patients with haemophilia. This pain is correlated with the degree of kinesiophobia and catastrophism (9).
Motion visualization consists of watching a video or live actions performed by an actor (10). The patient, through the activation of mirror neurons, transforms the visual input into activation of the same cortical areas that allow motor execution in real life (10, 11). The therapeutic use of virtual reality (VR) has shown its effectiveness in improving the range of motion and functionality in patients with total knee and hip arthroplasty (10).
The aim of this study was to evaluate the effectiveness of a movement visualization intervention using a 180-degree immersive video in first-person perspective in patients with haemophilic ankle arthropathy.
METHODS
Study design
A multicentre, single-blind, randomized clinical study was undertaken.
Patient recruitment and selection
The study was carried out between November 2021 and February 2022 in 6 regions of Spain (Andalusia, Aragon, Castilla y León, Galicia, Madrid, and Murcia).
The inclusion criteria in the study were: (i) over 18 years of age; (ii) medical diagnosis of haemophilia A or B; (iii) severe haemophilia phenotype (<1% of FVIII/FIX); (iv) bilateral ankle arthropathy; and (v) more than 5 points on the Haemophilia Joint Health Score (12) of joint damage.
Patients who: (i) did not present ankle pain; (ii) with cognitive impairments; (iii) diagnosed with epilepsy or with severe vision problems; (iv) receiving physiotherapy treatment during the study; and (v) who did not sign the informed consent were excluded from the study.
All patients received regular haemostatic monitoring at their referral hospital. The therapeutic regimen of the patients prescribed by their haematologist was not modified.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki. The subjects were informed of the risks and benefits of the study. All subjects signed the informed consent document. The project was approved by the CEIm of the Virgen de la Arrixaca University Hospital (ID: 2020-2-9-HCUVA). The research project was registered prior to the study (www.clinicaltrials.gov; ID: NCT04549402).
Measurement instruments
The primary variable was intensity of joint pain evaluated with the visual analogue scale (13). This scale has shown moderate reliability (14) in patients with chronic musculoskeletal pain. It assesses the intensity of the pain perceived by the patient on a 10-cm line. Within a range from 0 to 10, 10 indicates “the worst pain”.
The secondary variables were conditioned pain modulation, pressure pain threshold, ankle range of motion, and kinesio-phobia.
Conditioned pain modulation was measured using the Conditioned Pain Modulation Index (CPMI) (15). This procedure evaluates diffuse descending pain modulation by facilitating or inhibiting responses to a conditioned stimulus (15), with moderate reliability (16). For the evaluation, tonic pain was caused by pressing on a non-painful area (15). The threshold was first measured at the base of the dorsal part of the distal phalanx of the thumb and subsequently the conditioned stimulus was triggered using the ischaemia test (16) in the contralateral upper limb; the pain was rated on a numerical pain scale (17). The measurement was then repeated. The results were transformed according to the CPMI score. A positive result indicates pain inhibition and activation of the CPM phenomenon (18).
With a pressure gauge (model Wagner FDIX, Wagner Instruments, Riverside, CT, USA) (19) the pressure pain threshold was measured. Pressure was progressively applied until the feeling began to be painful (20). The pressure pain threshold was measured, bilaterally, in the ventral region to the lateral malleolus (21), in the same metamere (5th lumbar vertebra), and in an area with no direct neurological relationship (extensor carpi radialis longus) (19).
Using an analogue goniometer, the range of motion was measured. This instrument has shown excellent reliability (22). The joint range in plantar and dorsal flexion was measured (23). The unit of measurement is the degree (the higher the degree, the greater the mobility).
With the Spanish version of the Tampa Scale of Kinesiophophia questionnaire (TSK-11SV) (24) fear of movement was evaluated. This instrument offers moderate reliability (24). The scoring range is 11–44 points (a higher score indicates greater kinesiophobia).
Table I indicates the main characteristics of the measuring instruments used in the study.
| Measurement tool | Variable | How to use | Reliability | Units (range) |
| Visual analogue scale | Pain intensity |
|
0.60–0.77† | Score(0–10) |
| Conditioned Pain Modulation Index | Conditioned pain modulation |
|
0.60–0.75† | Score |
| Pressure algometer | Pressure pain threshold |
|
0.82–0.97† | n/cm2 |
| Analogic goniometer | Range of motion |
|
0.85–0.96† | Degrees(0–45) |
| Tampa Scale of Kinesiophobia | Kinesiophobia |
|
0.79α | Score(11–44) |
| †ICC: intraclass correlation coefficient; αCronbach’s alpha. PPT: pressure pain threshold; NRS: numeric rating scale. | ||||
In the pre-treatment evaluation, the anthropometric, sociodemographic, and clinical variables were evaluated. Joint condition was measured using the Haemophilia Joint Health Score (12). This scale, specific for patients with haemophilia, evaluates 8 items: inflammation and duration of inflammation, pain, atrophy and muscle strength, crepitus, and loss of flexion and extension. Each joint, knees, ankles, and elbows, is scored from 0 to 20 points (maximum joint damage).
Prior to recruitment, intra- and interobserver reliability was calculated based on 7 patients with ankle arthropathy. High intraobserver reliability was noted in pain intensity (ICC = 0.98), pressure pain threshold in the malleolus (ICC = 0.89) and extensor carpi radialis longus (ICC = 0.97), and plantar (ICC = 0.90) and dorsal ICC = 0.86) flexion. Intraobserver reliability was moderate in the variables for conditioned modulation (ICC = 0.76) and pressure pain threshold at L5 (ICC = 0.77).
Randomization
Randomization was performed with a computerized randomization procedure using permuted blocks of 8 subjects in each of the 6 recruitment centres. In each block, the 2 allocation possibilities (experimental or control) were randomly coded with 8 sequence alternatives. This process was carried out by an assistant blinded to group assignment and patient identification.
Intervention
An intervention of immersive visualization of ankle flexion–extension movement was carried out in patients included in the experimental group. A first-person-perspective 180-degree immersive video was used. This video was shown on the patient’s smartphone. The operating system was not an excluding factor. For immersive visualization, the smartphone was housed in virtual reality glasses (3D virtual reality glasses with remote control; model Qmax; https://www.qmax.bg/product-category/phones-and-tablets/gadgets-smart-technology/3d-glasses/) (25). The video was hosted on a YouTube channel® with access from the He-Mirror App®, designed ad hoc for the study. The subjects sat in a chair, with their feet relaxed and resting only on their heels. The intervention consisted of 28 consecutive home sessions, 1 per day. Each session lasted 15 min. During the session the patient needed only to watch the movement of both ankles in the video, without imagining the movement or performing it. Fig. 1 shows the performance of the intervention by 1 of the patients included in the study.

Fig. 1. Patient performing the intervention of 180-degree immersive VR motion visualization.
Patients included in the control group did not perform any visualization intervention, continuing with their usual routine of daily life activities and haemostatic control.
Procedure
The patients were evaluated at 3 time points: at baseline (T0), after the intervention (T1), and after 16 weeks’ follow-up (T2). All measurements were performed under the same conditions reproducing the same protocol. All the evaluations were carried out by the same rater, blinded to subject allocation to the study groups. The rater, with more than 20 years of clinical experience, was trained in the evaluation of patients with haemophilia. In the first measurement, the anthropometric and clinical variables were assessed.
Sample size
The sample size was calculated using the statistical package G*Power (version 3.1.9.2; Heinrich-Heine-Universität Düsseldorf, Germany). Assuming a high effect size (d = 0.81) (26), with an alpha level (type I error) of 0.01 and a statistical power of 90% (1-β = 0.90), a sample size of 20 patients in each group was estimated. Accounting for potential dropouts during the experimental phase and the follow-up period, an additional 20% were recruited. Thus, 48 patients with haemophilia and ankle arthropathy were included in the study.
Fifty-five patients with haemophilia were invited. Four failed to meet the selection criteria and 1 patient was excluded because of scheduled orthopaedic surgery. Two patients declined to participate.
Statistical analysis
Data were analysed using SPSS 19.0 software (IBM SPSS Statistics for Windows; IBM Corp, Armonk, NY, USA). According to a priori sample size calculation parameters, the statistical significance was set at p < 0.01 for a 99% confidence interval (CI). Full analysis set according to ICH guidelines was carried out.
The intra- and inter-rater reliability analysis was performed with the two-way random intraclass correlation coefficient. Although some data were not normally distributed, F-tests are robust in terms of type I error, and regardless of the manipulated conditions are considered a valid option for non-parametric distributions (27). The intergroup effect was calculated with repeated measures ANOVA. The Greenhouse–Geisser correction was considered when Mauchly’s test rejected sphericity (28). The effect size of the F-tests was analysed using the eta-squared coefficients (η2) and was interpreted as a small (η2 = 0.01), medium (η2 = 0.06), and large (η2 = 0.14) effect size (29).
The minimum detectable change (MDC) was obtained by estimating the standard error of measurement (SEM) with the formula: SEM = SDpre*√1-ICC (30). The formula (MDC = Z-score*√2*SEM) was used to obtain the MDC. The confidence level was set at 95% (Z-score = 1.96) (31). Finally, the proportion of patients whose change after the intervention exceeded the value indicated by the MDC was calculated.
RESULTS
Forty-eight patients were included in the study. During the experimental phase, 3 patients dropped out of the study. Another patient did not participate in the follow-up evaluation due to timetable incompatibility. Fig. 2 shows the flow diagram of the study.
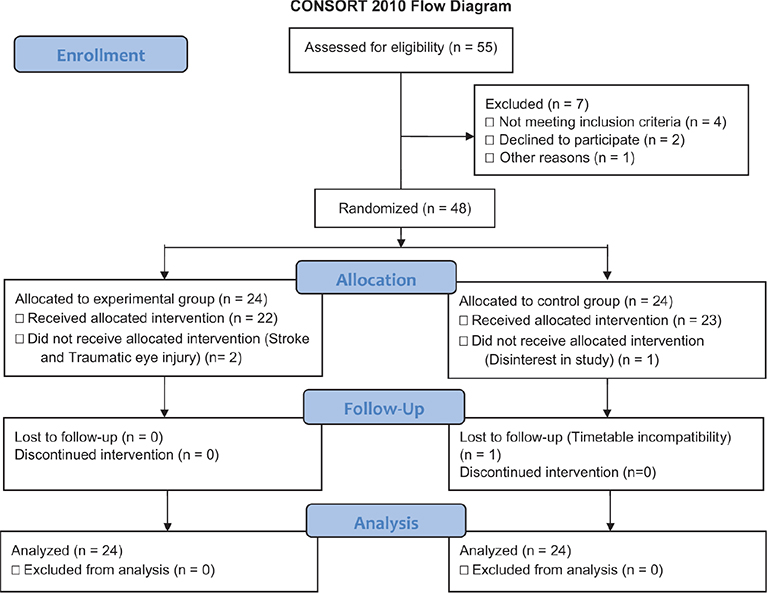
Fig. 2. Flowchart of randomization and follow-up.
The mean age of the patients was 39.85 (SD 6.89) years. The majority of patients had a diagnosis of haemophilia A (85.4%) and were receiving prophylactic treatment (64.5%). Four patients (20.8%) had developed inhibitors. None of the patients developed ankle hemarthrosis during the experimental phase. Table II lists the descriptive characteristics of the patients.
Pain intensity
When analysing the intergroup effect we observed statistically significant differences (F[1.74;162.67] = 37.14). In the pairwise comparison analysis there were significant changes in T1–T0 (99% CI (–0.75; –0.27) and T2–T0 (99% CI –0.81; –0.15). The value of the minimum detectable change was 0.43 points. Changes greater than the MDC after the intervention were reported in 75% of experimental group patients.
Repeated measures analysis
There were statistically significant intergroup differences (p < 0.001) in conditioned pain modulation (F[2;92] = 5.40). There were also statistically significant differences in dorsal (F[1.76;165.98] = 19.17) and plantar (F[2;188] = 9.27) flexion. However, there were no statistically significant differences (p > 0.01) in the pressure pain threshold in the extensor carpi radialis longus (F[2;92] = 3.25), malleolus (F[2;92] = 4.11), or fifth lumbar vertebra (F[1.54;71.17] = 4.62), or in kinesiophobia (F[2;92] = 2.92). Table III gives the results of the repeated measures analysis.
Minimum detectable change
When calculating the value of the minimum detectable change (MDC = 0.64), 37.5% of the patients in the experimental group showed equal or greater changes after the intervention in conditioned pain modulation. More than half of the patients who underwent the intervention showed values higher than the MDC in the pressure pain threshold of the extensor carpi radialis longus (MDC = 1.34) and malleolus (MDC = 4.93). More than 20% of the patients showed greater changes in dorsal (MDC = 3.51) and plantar (MDC = 2.91) flexion. When calculating the MDC of kinesiophobia, through the previously calculated SEM (32), we noted how 25% of the patients exhibited changes greater than the MDC (4.41). The results of the calculation of the minimum detectable change are respectively listed in Table IV.
DISCUSSION
The aim of this study was to evaluate the effectiveness of an intervention of immersive visualization of movement in patients with haemophilic ankle arthropathy. After the intervention there were intergroup changes in pain intensity, conditioned pain modulation, and range of motion. We noted a relevant clinical effect on the variables pain intensity and pressure pain threshold.
In patients with musculoskeletal pain, there is a relationship between motor deficits and pain, which may precede pain, being associated with cortical reorganization and changes in cortical processing (33). This cortical reorganization occurs in the primary somatosensory and motor cortex. This phenomenon has been proposed as the reason for the inconsistency between motor intention and sensory feedback that may persist, causing the affective experience of pain (33). Chronic perception of joint pain in patients with haemophilic arthropathy is common (4).
Exposure to virtual reality can improve the intensity of pain in patients with knee arthroplasty (34). While pain and disuse can cause neuroplastic changes that lead to cortical reorganization, visualization of movement promotes neuroplastic and motor control changes (10). The persistence of pain over time causes neuroplastic changes in patients with haemophilia. Maintained changes in pain after the follow-up period in the experimental group patients may be due to the influence on the previous painful experience.
Statistically significant changes do not necessarily reflect a clinically significant change. Calculation of the minimum detectable change (MDC) offers the minimum change in the score that, with 95% confidence, reflects a real clinical change and not one due to a measurement error (35). More than 50% of the patients included in the experimental group exhibited changes greater than the MDC in intensity of pain. These high percentages demonstrate how the results are able to detect the true clinical change from this intervention in patients with haemophilia. According to such values, the observed changes were homogeneous in a significant percentage of patients, thus suggesting the effectiveness of this intervention in patients with haemophilic ankle arthropathy.
Conditioned pain modulation is the joint effect of endogenous pathways that enhance or reduce the effects of afferent noxious stimuli (36), being an endogenous phenomenon of pain inhibition. Conditioned pain modulation is significantly impaired in a large number of patients with chronic pain (37). The reported changes may be due to the fact that, like other patients with chronic pain, haemophilia patients suffer from such a deterioration of this modulation system. Visualization of movement can have an impact on these patients through improving their modulation by inducing the activation of movement patterns without nociceptive inputs that would lead to central desensitization.
The pressure pain threshold of the sensitivity to the painful stimulus and its modification implies the mechanisms involved. More than half of the patients who underwent the intervention presented changes beyond the MDC in the local pressure pain threshold (malleolus) and remote pressure pain threshold (extensor carpi radialis longus). These results suggest changes in peripheral and central sensitization mechanisms. As much as 41% of patients who underwent the intervention exhibited changes in the pressure pain threshold at L5, above the minimum detectable change of that variable. This therapeutic approach in patients with arthropathy can promote a decrease in neurological sensitization, facilitating a change in the somatosensory profile affected in patients with haemophilia (38).
This study reports an improvement in ankle range of motion in patients who underwent the intervention compared with the control group. However, based on the minimal detectable change, these changes and their clinical relevance should be interpreted with caution. Improved ankle mobility affects lower limb functionality in these patients (39). Accordingly, the improvements observed in range of motion together with the motor reprogramming induced by the visualization of movement may make it advisable to use immersive virtual reality as a complementary intervention in the approach to these patients.
Pain catastrophizing can increase the painful experience, leading to avoidance behaviour and favouring kinesiophobia (8). The suitability of carrying out an approach on cortical reorganization and psychosocial factors in patients with kinesiophobia has been described.
Gradual exposure to the adverse stimulus through virtual reality has been used to address other phobias such as the fear of flying or social anxiety (40). No intergroup differences were found in this study, which may be due to the fact that kinesiophobia prior to the study was, on average, below 27 points.
Study limitations
This study presents some limitations that should be considered. The fact that patients were not blinded is an important limitation. Although the intake of analgesic drugs prior to the intervention was evaluated, the use of these drugs could not be monitored due to their self-administration without a doctor’s prescription in many cases. Their impact is a factor that must be taken into account for the interpretation of the results. The intervention was carried out on the patients’ mobile phone, with each of the various smartphone models, having respective operating systems and screen sizes. Use of a single stand-alone headset system, with greater video quality, realism, and immersion, would have been an ideal option to unify the intervention for all patients.
Conclusion
A 180-degree immersive VR video-based visualization of movement is an effective tool for addressing the intensity of pain in patients with haemophilic ankle arthropathy. This intervention can improve conditioned pain modulation and ankle range of motion in this population. Visualization of movement can produce a clinically relevant change in the pressure pain threshold locally, at the spinal segment, and at the unrelated neurological level (central sensitization).
ACKNOWLEDGEMENTS
The authors are especially grateful to the Spanish Federation of Haemophilia, Galician Association of Haemophilia, Malaga Association of Haemophilia, Andalusia Association of Haemophilia, Association of Haemophilia of Valladolid-Palencia, Murcia Regional Association of Haemophilia, and Association of Haemophilia of Burgos for their help in recruiting the sample.
Trial registration number: id NCT04549402.
Source of support: The authors state that this work has received financial support from Roche Farma, S.A. The funders played no role in the design, conduct, or reporting of this study.
REFERENCES
- Iorio A, Stonebraker JS, Chambost H, Makris M, Coffin D, Herr C, et al. Establishing the prevalence and prevalence at birth of hemophilia in males. Ann Intern Med 2019; 171: 540–546. https://doi.org/10.7326/M19-1208
- Pérez-Llanes R, Donoso-Úbeda E, Meroño-Gallut J, Ucero-Lozano R, Cuesta-Barriuso R. Safety and efficacy of a self-induced myofascial release protocol using a foam roller in patients with haemophilic knee arthropathy. Haemophilia 2022; 28: 326–333. https://doi.org/10.1111/hae.14498
- White G, Rosendaal F, Aledort L, Lusher J, Rothschild C, Ingerslev J. Definitions in hemophilia: recommendation of the Scientific Subcommittee on Factor VIII and Factor IX of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Thromb Haemost 2001; 85: 560–560. https://doi.org/10.1055/s-0037-1615621
- Gouw SC, Timmer MA, Srivastava A, de Kleijn P, Hilliard P, Peters M, et al. Measurement of joint health in persons with haemophilia: a systematic review of the measurement properties of haemophilia-specific instruments. Haemophilia 2019; 25: e1–e10. https://doi.org/10.1111/hae.13631
- Valentino LA, Hakobyan N, Enockson C. Blood-induced joint disease: the confluence of dysregulated oncogenes, inflammatory signals, and angiogenic cues. Semin Hematol 2008; 45: S50–57. https://doi.org/10.1053/j.seminhematol.2008.03.017
- Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain 2020; 161: 1976–1982. https://doi.org/10.1097/j.pain.0000000000001939
- Treede R-D, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019; 160: 19–27. https://doi.org/10.1097/j.pain.0000000000001384
- Caneiro JP, Smith A, Bunzli S, Linton S, Moseley GL, O’Sullivan P. From fear to safety: a roadmap to recovery from musculoskeletal pain. Phys Ther 2022; 102: pzab271. https://doi.org/10.1093/ptj/pzab271
- Ucero-Lozano R, López-Pina JA, Ortiz-Pérez A, Cuesta-Barriuso R. The relationship between chronic pain and psychosocial aspects in patients with haemophilic arthropathy: a cross-sectional study. Haemophilia 2021; 28: 176–182. https://doi.org/10.1111/hae.14469
- Paravlic AH. Motor imagery and action observation as appropriate strategies for home-based rehabilitation: a mini-review focusing on improving physical function in orthopedic patients. Front Psychol 2022; 13: 826476. https://doi.org/10.3389/fpsyg.2022.826476
- Hsieh Y-W, Lee M-T, Lin Y-H, Chuang L-L, Chen C-C, Cheng C-H. Motor cortical activity during observing a video of real hand movements versus computer graphic hand movements: an MEG study. Brain Sci 2020; 11: E6. https://doi.org/10.3390/brainsci11010006
- Fischer K, Kleijn P de. Using the Haemophilia Joint Health Score for assessment of teenagers and young adults: exploring reliability and validity. Haemophilia 2013; 19: 944–950. https://doi.org/10.1111/hae.12197
- Hawksley H. Pain assessment using a visual analogue scale. Prof Nurse Lond Engl 2000; 15: 593–597.
- Boonstra AM, Preuper HRS, Reneman M, Posthumus JB, Stewart RE. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int J Rehabil Res 2008; 31: 165–169. https://doi.org/10.1097/MRR.0b013e3282fc0f93
- Ferrer-Peña R, Muñoz-García D, Calvo-Lobo C, Fernández-Carnero J. Pain expansion and severity reflect central sensitization in primary care patients with greater trochanteric pain syndrome. Pain Med 2019; 20: 961–970. https://doi.org/10.1093/pm/pny199
- Kennedy DL, Kemp HI, Ridout D, Yarnitsky D, Rice ASC. Reliability of conditioned pain modulation: a systematic review. Pain 2016; 157: 2410–2419. https://doi.org/10.1097/j.pain.0000000000000689
- Alghadir AH, Anwer S, Iqbal A, Iqbal ZA. Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J Pain Res 2018; 11: 851–856. https://doi.org/10.2147/JPR.S158847
- Ibancos-Losada M del R, Osuna-Pérez MC, Castellote-Caballero MY, Díaz-Fernández Á. Conditioned pain modulation effectiveness: an experimental study comparing test paradigms and analyzing potential predictors in a healthy population. Brain Sci 2020; 10: 599. https://doi.org/10.3390/brainsci10090599
- Skou ST, Simonsen O, Rasmussen S. Examination of muscle strength and pressure pain thresholds in knee osteoarthritis: test-retest reliability and agreement. J Geriatr Phys Ther 2015; 38: 141–147. https://doi.org/10.1519/JPT.0000000000000028
- Leffler A-S, Kosek E, Lerndal T, Nordmark B, Hansson P. Somatosensory perception and function of diffuse noxious inhibitory controls (DNIC) in patients suffering from rheumatoid arthritis. Eur J Pain 2002; 6: 161–176. https://doi.org/10.1053/eujp.2001.0313
- Dhondt W, Willaeys T, Verbruggen LA, Oostendorp RAB, Duquet W. Pain threshold in patients with rheumatoid arthritis and effect of manual oscillations. Scand J Rheumatol 1999; 28: 88–93. https://doi.org/10.1080/030097499442540
- Konor MM, Morton S, Eckerson JM, Grindstaff TL. Reliability of three measures of ankle dorsiflexion range of motion. Int J Sports Phys Ther 2012; 7: 279–287.
- Gerhardt J, Cocchiarella L, Lea R. The practical guide to range of motion assessment. Chicago, IL: American Medical Association; 2002, p. 94–95.
- Gómez-Pérez L, López-Martínez AE, Ruiz-Párraga GT. Psychometric properties of the Spanish version of the Tampa Scale for Kinesiophobia (TSK). J Pain 2011; 12: 425–435. https://doi.org/10.1016/j.jpain.2010.08.004
- Choi JW, Kim BH, Huh S, Jo S. Observing actions through immersive virtual reality enhances motor imagery training. IEEE Trans Neural Syst Rehabil Eng 2020; 28: 1614–1622. https://doi.org/10.1109/TNSRE.2020.2998123
- Tat NM, Can F, Sasmaz HI, Tat AM, Antmen AB. The effects of manual therapy on musculo-skeletal system, functional level, joint health and kinesiophobia in young adults with severe haemophilia: a randomized pilot study. Haemophilia 2021; 27: e230–e238. https://doi.org/10.1111/hae.14031
- Blanca MJ, Alarcón R, Arnau J, Bono R, Bendayan R. Non-normal data: is ANOVA still a valid option? Psicothema 2017; 29: 552–557.
- Haverkamp N, Beauducel A. Violation of the sphericity assumption and its effect on type-I error rates in repeated measures ANOVA and multi-level linear models (MLM). Front Psychol 2017; 8: 1841. https://doi.org/10.3389/fpsyg.2017.01841
- Cohen J. Eta-squared and partial eta-squared in fixed factor Anova designs. Educ Psychol Meas 1973; 33: 107–112. https://doi.org/10.1177/001316447303300111
- Schmitt JS, Di Fabio RP. Reliable change and minimum important difference (MID) proportions facilitated group responsiveness comparisons using individual threshold criteria. J Clin Epidemiol 2004; 57: 1008–1018. https://doi.org/10.1016/j.jclinepi.2004.02.007
- de Vet HC, Terwee CB, Ostelo RW, Beckerman H, Knol DL, Bouter LM. Minimal changes in health status questionnaires: distinction between minimally detectable change and minimally important change. Health Qual Life Outcomes 2006; 4: 54. https://doi.org/10.1186/1477-7525-4-54
- Woby SR, Roach NK, Urmston M, Watson PJ. Psychometric properties of the TSK-11: a shortened version of the Tampa Scale for Kinesiophobia. Pain 2005; 117: 137–144. https://doi.org/10.1016/j.pain.2005.05.029
- Vittersø AD, Halicka M, Buckingham G, Proulx MJ, Bultitude JH. The sensorimotor theory of pathological pain revisited. Neurosci Biobehav Rev 2022; 139: 104735. https://doi.org/10.1016/j.neubiorev.2022.104735
- Peng L, Zeng Y, Wu Y, Si H, Shen B. Virtual reality-based rehabilitation in patients following total knee arthroplasty: a systematic review and meta-analysis of randomized controlled trials. Chin Med J (Engl) 2022; 135: 153–163. https://doi.org/10.1097/CM9.0000000000001847
- Stratford PW, Binkley JM, Riddle DL. Health status measures: strategies and analytic methods for assessing change scores. Phys Ther 1996; 76: 1109–1123. https://doi.org/10.1093/ptj/76.10.1109
- Ramaswamy S, Wodehouse T. Conditioned pain modulation – a comprehensive review. Neurophysiol Clin 2021; 51: 197–208. https://doi.org/10.1016/j.neucli.2020.11.002
- Lewis G, Rice D, McNair P. Conditioned pain modulation in populations with chronic pain: a systematic review and meta-analysis. J Pain 2012; 13: 936–944. https://doi.org/10.1016/j.jpain.2012.07.005
- Krüger S, Boettger MK, Hilberg T. Somatosensory profile of patients with haemophilia. Haemophilia 2018; 24: 97–103. https://doi.org/10.1111/hae.13370
- Cuesta-Barriuso R, Donoso-Úbeda E, Meroño-Gallut J, Pérez-Llanes R, López-Pina JA. Functionality and range of motion in patients with hemophilic ankle arthropathy treated with fascial therapy: a randomized clinical trial. Musculoskelet Sci Pract 2020; 49: 102194. https://doi.org/10.1016/j.msksp.2020.102194
- Botella C, Fernández-Álvarez J, Guillén V, García-Palacios A, Baños R. Recent progress in virtual reality exposure therapy for phobias: a systematic review. Curr Psychiatry Rep 2017; 19: 42. https://doi.org/10.1007/s11920-017-0788-4