ORIGINAL ARTICLE
THE CZECH FUGL–MEYER ASSESSMENT FOR POST-STROKE SENSORIMOTOR FUNCTION: TRANSLATION AND CROSS-CULTURAL ADAPTATION AND VALIDATION
Barbora KOLÁŘOVÁ, PT, PhD1,2 , Petra GAUL-ALÁČOVÁ, PT, PhD1, Nicole MUSILOVÁ, MD2,3, Anna MAJEROVÁ, PT, MSc1,2 and Margit ALT MURPHY, PT, PhD4,5*
, Petra GAUL-ALÁČOVÁ, PT, PhD1, Nicole MUSILOVÁ, MD2,3, Anna MAJEROVÁ, PT, MSc1,2 and Margit ALT MURPHY, PT, PhD4,5*
From the 1Department of Clinical Rehabilitation, Faculty of Health Sciences, Palacký University, Olomouc, Czech Republic, 2Department of Rehabilitation, University Hospital, Olomouc, Czech Republic, 3Department of Neurology, Faculty of Medicine and Dentistry, Palacký University Olomouc, Czech Republic, 4Department of Clinical Neuroscience, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden, and 5Department of Rehabilitation and Health, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Objective: To ensure wider use of the internationally recommended Fugl–Meyer Assessment (FMA) of sensorimotor function for people with stroke, official translations of the scale are needed. This study aimed to perform a translation and cross-cultural adaptation/validation of the FMA into the Czech language.
Design: Translation and cross-cultural adaptation/validation.
Subjects/Patients: Five clinical experts and 1 external expert participated as reviewers; 11 individuals with stroke in the early subacute phase were included in the pilot testing.
Methods: A standardized process using forward–backward translations, expert panel reviews, and pilot testing between and within the raters (inter- and intra-rater reliability) were employed to ensure conceptual, semantic, and operational validity of the new Czech FMA. Agreement between raters was assessed in 11 individuals with stroke on 2 consecutive days at University Hospital Olomouc by using Svensson’s rank-based statistics.
Results: Percentage of agreement between and within raters ranged between 70–100% and 55–100%, respectively. Systematic disagreements, found in 7 out of 96 FMA items, were discussed and revised in the final version.
Conclusion: The Czech FMA offers a more unified and standardized assessment of sensorimotor impairment in clinical and research settings. This will improve stroke rehabilitation care and allow for wider international collaboration.
LAY ABSTRACT
The Fugl–Meyer Assessment is the number one scale recommended for assessment of motor and sensory function in people with stroke. For correct clinical use official validated translations are needed. This study performed a translation and cross-cultural adaptation of the Fugl–Meyer Assessment into Czech. A standardized protocol with forward–backward translation, expert consensus, and pilot testing in 11 individuals with stroke were used to ensure conceptual, semantic, and operational consistency. The results of pilot testing showed good agreement and allowed final adjustments in 7 problematic test items. The cross-culturally adapted Czech Fugl–Meyer Assessment is now available and provides a more unified and standardized assessment of sensorimotor impairment after stroke in both clinical and research settings.
Key words: cross-cultural comparison; lower extremity; stroke; sensorimotor assessment; translation; upper extremity; validation.
Citation: J Rehabil Med 2025; 57: jrm43010. DOI: https://doi.org/10.2340/jrm.v57.43010.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Submitted: Jan 22, 2025; Accepted after revision: Mar 20, 2025; Published: May 7, 2025.
Correspondence address: Margit Alt Murphy, Department of Clinical Neuroscience, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Vita stråket 12, plan 4, Sahlgrenska University Hospital, 413 46 Gothenburg Sweden. E-mail: margit.alt-murphy@neuro.gu.se
Competing interests and funding: The authors have no conflicts of interest to declare.
This work was supported by Palacký University grant IGA_FZV_2024_002 and by MH CZ– DRO (FNOl, 00098892).
Stroke ranks as 1 of the top 3 causes of non-traumatic death and long-term disability worldwide (1, 2). The Czech Republic is among the countries with the highest incidence of stroke in the world (3). In 2021, approximately 291 patients per 100,000 population were hospitalized for stroke (4). Despite the reduction in the overall incidence and mortality in the Czech Republic, which follows the global trend of this disease (3, 5), the ageing population results in an increasing number of stroke survivors living with some kind of residual deficit.
One of the most common clinical manifestations of stroke is hemiparesis, which particularly limits voluntary control of upper and lower limb movement contralateral to the lesion (6). This leads to impaired postural control, gait, or upper extremity function, limiting the patient’s independence in daily activities (2, 6). The central goal of rehabilitation is to maximize independence in activities of daily living and to improve the quality of life. To evaluate these goals, it is necessary to use reliable and validated tools for assessment of stroke severity and impairment.
Worldwide, one of the most widely used clinical tools for the assessment of sensorimotor function after stroke is the Fugl–Meyer Assessment (FMA) (7–9). The FMA, recognized as the gold standard in clinical and research settings, demonstrates high validity and reliability in the subacute (10, 11) and chronic stages of stroke (6, 12, 13).
The FMA assesses motor functions at the impairment level in respect of the International Classification of Functioning, Disability and Health (ICF) (14). The international consensus recommends including the FMA in all clinical trials in people with stroke (15) and as a key assessment to evaluate the effectiveness of rehabilitation (12). The FMA has been shown to be sensitive in capturing changes after therapeutic interventions, such as robotic rehabilitation (16), virtual reality (17), mental training (18), constrained induced movement therapy (19), and pharmacological treatment (20).
The FMA is an observational ordinal rating scale for evaluating upper (FMA-UE) and lower extremity (FMA-LE) sensorimotor functions (21). The scoring of each test item is clear and standardized, no specific tools are needed, and the administration time is relatively short, which makes the scale easily accessible and clinically feasible (22). This scale is commonly used by physiotherapists and other professionals with appropriate training (medical doctors, occupational therapists). An official version of the FMA in the Czech language is needed to ensure access to nationwide standardized assessment procedures, evaluate outcomes of stroke care within the Czech Republic, and promote international collaboration. It is important to follow standardized translation and cross-cultural adaptation procedures to ensure that the translated version of the scale agrees with the established construct validity and reliability of the original scale and will allow comparisons over time, across countries, and across organizations (23). The official translations of the FMA are available for non-profit clinical or research use in several languages (https://www.gu.se/en/neuroscience-physiology/fugl-meyer-assessment) (10, 11, 24–29).
The aim of this study was to translate and create an official cross-culturally adapted Czech FMA for the assessment of upper and lower extremity sensorimotor function in people with stroke.
METHODS
Translation and cross-cultural adaptation encompass a process of both language and cultural adaptation to maintain the content validity of the assessment at a conceptual level across different cultures, languages, and countries (30, 31). The translation and cross-cultural adaptation process used within this study was based on the guidelines recommended by Beaton et al. (30) and more recently by Sousa and Rojjanasrirat (31). A standardised forward and backward translation combined with expert reviews was performed in accordance with Barbosa et al. (28) or Busk et al. (24), who further specified slight nuances that are more suitable for the FMA, as this assessment is not administered by the patients themselves, but by trained professionals. The whole process for cross-cultural adaptation was initiated after approval from the curator of the original FMA at the University of Gothenburg. An interdisciplinary team from the Stroke Research Group of Palacký University and University Hospital Olomouc conducted the translation, revision, and cross-cultural validation of pre-final version by pilot testing in post-stroke patients to identify possible disagreements in the pre-final version. The University of Gothenburg provided regular consultations during the entire process.
Translation process
The original version of the FMA (available at https://www.gu.se/en/neuroscience-physiology/fugl-meyer-assessment) was used for the translation (21). A standardized forward and backward translation combined with expert reviews was performed to ensure conceptual, semantic, and operational equivalence (28, 30, 31). The entire process is shown in Fig. 1. Two professional translators (native speakers of the target language), fluent in both English and Czech, performed the forward translation independently. These translations were compared, to draft the first Czech version, by the expert group consisting of another professional translator, 3 physiotherapists, and 1 medical doctor, all specialized in neurorehabilitation. The first version was translated back to English by another professional bilingual translator (native in English and fluent in Czech) and reviewed by the University of Gothenburg expert (MAM) and 2 Czech clinical researchers (BK and PGA), fluent in English and with knowledge of FMA, to ensure semantic, idiomatic, and conceptual equivalence with the original version. The 2 versions were re-evaluated and the second Czech version of FMA was drafted.
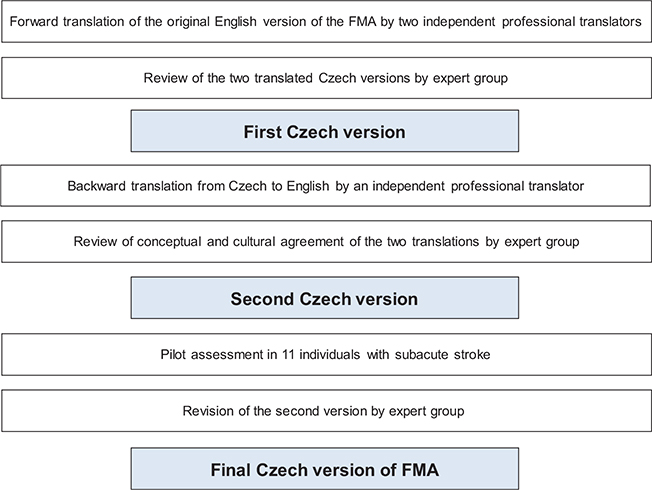
Fig. 1. Flowchart of translation and cross-cultural adaptation process.
Pilot testing of the pre-final version
Pilot testing of the pre-final 2nd version was conducted to identify potential disagreements within and between raters when the FMA was used in the Czech context. In this step, 11 participants with stroke were requited from the Rehabilitation Department of University Hospital Olomouc, which is part of the Comprehensive Stroke Centre at University Hospital Olomouc. The inclusion criteria were: first ever stroke verified by CT/MRI scan, lower or/and upper limb paresis due to stroke (as evaluated and documented by a medical doctor specialized in Rehabilitation and Physical Medicine), age 18–80 years, sufficient cognitive function to understand the physiotherapist’s instructions during the FMA assessment, able to provide informed consent and to understand the purpose of the study. Exclusion criteria were: recurrent stroke, other neurological diseases, cognitive, visual, or/and hearing deficit, or aphasia preventing cooperation during the assessment of the FMA. The screening for eligibility was performed by the medical doctor within the first 2 weeks after stroke onset in the Rehabilitation Department. All patients admitted during this period were screened for potentially meeting the inclusion criteria. The research was performed in accordance with the principles stated in the Declaration of Helsinki and was approved by the Ethics Committee of the Faculty of Health Sciences, Palacký University in Olomouc (UPOL-1703/1040-2020). All participants who expressed their agreement to participate in the study signed an informed consent.
The full FMA for the upper and lower extremities, including the non-motor domains of sensation, range of motion, and pain, was carried out by 2 experienced physiotherapists, on 2 consecutive days. Both assessors read properly the Czech version of the FMA and watched the instructional videos with English subtitles (https://www.gu.se/en/neuroscience-physiology/fugl-meyer-assessment). Any unclarities were discussed with a certified English interpreter and a native speaker to avoid any potential impact of misunderstanding or misinterpretation on the study results. In addition, both assessors underwent mutual training sessions on themselves and assessed 3 patients (not included in this study) prior to the study. On the first day, 1 physiotherapist was the lead assessor, who instructed the patient, while the other physiotherapist observed the patient’s performance. Both therapists scored the patient’s performance on each tested item independently. The next day, the assessors’ roles were switched. The assessors did not communicate with each other regarding the assessment during or after the evaluation; however, the observing assessor could ask the patient to repeat a movement whenever necessary for scoring (if they had not had enough time to complete it or could not see the performance properly). Scoring in each FMA domain was based on direct observation of performance. The entire assessment lasted approximately 30 min. The assessment protocols were stored in sealed envelopes immediately after the assessment and were only opened after all participants had been assessed (24, 28).
Elisabeth Svensson’s rank-based statistical method was used. This statistical method is particularly designed for ordinal data to evaluate the inter-rater and intra-rater reliability (32, 33). This method quantifies the type and the extent of observed systematic and non-systematic inter- and intra-rater disagreements (33).
The percentage of agreement (PA%) was calculated. An agreement of ≥ 70% was considered satisfactory and ≥ 90% excellent (24). Systematic disagreement between assessors was evaluated by relative position (RP), which determines whether scores are distributed systematically towards lower or higher values, and by relative concentration (RC), which determines whether scoring is concentrated towards the central category compared with the other categories. RP and RC take values from –1 to 1, where 0 means that there was no difference between the assessors. A value equal or greater than 0.1 is considered as a potential disagreement. Relative rank variation (RRV) demonstrates non-systematic random disagreement caused by individual variability and values < 0.1 indicate that the random error is negligible. The results of the analyses were used to identify which items and in which direction were scored differently by the 2 assessors. These items were discussed and agreed on in the expert group and with the external expert to improve coherence and interpretability.
RESULTS
Forward and backward translation
Minor linguistic differences were found between the two forward translations, mostly regarding nomenclature of anatomical terms or positions, similar to the results in Cecchi et al. (25) and Barbosa et al. (28). After a few contextual modifications considering the clinical terminology used in the Czech Republic by physical and occupational therapists as well as medical doctors, consensus was reached for the 1st Czech version of FMA. In the next stage, the 1st version was compared with the back-translated version. Only minor semantic discrepancies, which did not have any effect on the meaning, were found and revised for the finalization of the 2nd Czech version of the FMA.
Pilot clinical testing
Of 27 patients who were screened for participation in the cross-cultural adaptation of the Czech FMA, 13 were eligible for participation in this study. However, 1 was subsequently excluded due to early discharge from hospital before the second day of assessment, and 1 was excluded due to clinical complications during hospitalization. Pilot testing and final analysis was then based on data collected from 11 participants in an early subacute stage (Table I).
The percentage of agreement between assessor A and assessor B (inter-rater agreement) ranged from 73% to 100% for each item of the FMA-UE and FMA-LE, which is classified as a sufficient level of agreement (Tables SI and SII). No systematic or random disagreements were found between assessors (inter-rater agreement).
A minor disagreement was found within assessors between day 1 and day 2 (intra-rater agreement). For FMA-UE, the intra-rater agreement varied between 55% and 100% and was observed to be < 70% in 9 motor items and 1 non-motor item (Table SI). Statistically significant systematic disagreement (CI did not include a zero value and the RP or RC was ≥ 0.1) was present in 3 items: A.III: Movement mixing synergies (shoulder flexion and pronation–supination), and for I: Passive joint motion (shoulder external rotation). For FMA-LE, the intra-rater agreement was in the range of 45–100%, where agreement < 70% was present in 3 motor items and 2 non-motor items (Table SII). Statistically significant systematic disagreement was found for A.II: Voluntary movement in synergies (ankle dorsal flexion) and in A.III: Movement in mixed synergies (ankle dorsiflexion), H: Sensation (position toe), and I: Passive joint motion (foot pronation). No random disagreements were detected.
Final Czech version
The identified disagreements from the pilot testing were reviewed and discussed with the assessors in the expert group. The main final adjustments agreed in the expert groups are described below.
For the item III: Movement mixing synergies (pronation–supination), the translation of expression “no pronation/supination, starting position impossible” was revised and changed from “bez pronace/supinace, výchozí pozice nemožná” (meaning without pronation/supination) to “žádná pronace/supinace, výchozí pozice nemožná” (with a more exact meaning of any or no pronation/supination). The translation of the expression “elbow flexion” was revised and changed from “flexe lokte” to “flexe v lokti” for better understanding.
Furthermore, according to the assessors’ suggestions, the expression “Volitional movement mixing synergies” was changed from “Volní pohyby smíšené synergie” to “Volní pohyby kombinující synergie” (volitional movement combining synergies) in both FMA-UE and FMA-LE. On the FME-UE, the expression ‘Volitional movement within synergies, without gravitational help” was also changed from “…bez pomoci gravitace” (without the help of gravity) to “…bez pomoci proti gravitaci” (without help against gravity) to align with the terms commonly used in Czech, for example, in manual muscle strength testing. The expression “no support to wrist” was changed from “žádná opora o zápěstí” to “opora zápěstí není poskytnuta” (support at wrist is not provided), to align with the expression used in the lower extremity section. The expression for Coordination/speed subscale in FMA-UE “after one trial with both arms” was changed from “nejdříve jeden zkušební test oběma rukama” to “zkušební test jednou a následně druhou rukou”, as in Czech “oběma rukama” means precisely simultaneously performed with both arms, but the test trial before scoring needed to be performed first with the non-paretic and then with the paretic upper limb.
These final modifications were sent to the researchers at the University of Gothenburg in May 2022, who reviewed and approved these proposed adjustments. The last revision of the FMA protocol and application manual resulted in the final Czech version of the FMA, which is now available on the website (https://www.gu.se/en/neuroscience-physiology/fugl-meyer-assessment).
DISCUSSION
This study provides an official translation and cross-cultural adaptation of the original FMA assessment protocol from English into Czech. The preliminary inter- and intra-rater reliability evaluation showed sufficient inter-rater reliability for both FMA-UE and FMA-LE. The official protocol of the Czech FMA will ensure standardized assessment of sensorimotor impairment in patients at all stages after stroke.
The FMA is the most frequently used measure in stroke rehabilitation trials (7–9, 34) and the motor domains of the FMA have shown high validity, reliability, and responsiveness for stroke populations (35). It has been used in both subacute (10, 11) and chronic patients after stroke (6, 12, 13, 36). Ceiling effect has been observed in patients with mild motor deficits (37, 38), while patients with severe motor deficits may demonstrate a floor effect (36, 39). The FMA is considered a valid tool for assessment of motor impairment severity poststroke in clinical practice and rehabilitation research (40). Given the strong evidence of measurement properties, the FMA is included in the core set of European evidence-based recommendations for Clinical Assessment of the Upper Limb in Neurorehabilitation (52) and in the international consensus-based core recommendations of the Stroke Recovery and Rehabilitation Roundtable (53).
In the current study, both motor and non-motor subscales of FMA were translated and further analysed for item-level reliability to identify any problematic items where disagreements were found between the assessors. The translation of both motor and non-motor subscales will provide access to the complete protocol of Czech FMA in clinical and research settings.
The FMA assesses impairment according to ICF, and together with other assessments of activity level will provide deeper insight into the course of motor recovery after stroke, which can facilitate a more precise rehabilitation strategy (41). From both a clinical and scientific perspective, the Czech FMA will provide an opportunity to compare the results between clinical sites nationally to improve the quality of care and in the long term also internationally when included in European or global databases compiling larger datasets from multiple sites and countries to better describe stroke severity and recovery patterns in all post-stroke stages (28, 42). Additionally, the use of the FMA allows clinicians and researchers to determine whether the change in the FMA scores, due to intervention, represents clinically significant improvement, as minimal clinically significant differences are well established for both FMA-UE and FMA-LE (43–45). The FMA also has potential to predict motor recovery early post-stroke (46). The FMA-UE has been used to predict upper limb motor recovery within 72 h after stroke onset (47–49).
The pilot testing showed excellent to sufficient inter-rater reliability, as the level of agreement was for both FMA-UE and FMA-LE on all items in the range of 70–100%. These results agreed with previously reported intra- and inter-rater agreements of the Spanish, Danish, and Italian translated FMA versions (70–100%) (10, 11, 24, 50). Excellent inter-rater reliability with high ICC values was demonstrated for the German version of the FMA, although the percentage of inter-rater agreement at item level was reported to be lower (median 77%, range 44–100%) (51). Even the Korean (26), Romanian (27), or Urdu (29) versions of the FMA have been validated for clinical use on the basis of good to excellent reliability and validity.
No statistically significant systematic disagreements were found in any items for the inter-rater reliability in our study. However, the intra-rater reliability (agreement between the assessments done by the same assessor 1 day apart) showed disagreements below 70% on some items. A similar trend with disagreements detected between the first and second assessment for 2 items (ankle dorsiflexion during flexor synergy and the normal reflex activity) was reported in the study of Hernandéz et al. (11). The shifts towards higher scores on the second day may indicate possible spontaneous recovery at an early stage of stroke (11). For future studies conducted on participants in the early subacute stage, the reassessment should preferably be conducted in a shorter time interval, e.g. within the same day, to avoid mixing potential spontaneous improvements with differences in assessment scores.
Both assessors underwent prior training on the FMA by watching the instructional videos and conducting trial assessments. We agree with the statement of Busk et al. (24) that proper practice with testing and scoring prior to assessment itself is essential. We also acknowledge that performing all parts of the FMA might be tiring for the patient in the early subacute phase and here the upper and lower extremity assessments could preferably be performed separately in clinical settings. However, none of the participants in the current study reported complaints of exhaustion.
The cross-cultural adaptation of the Czech FMA conducted in this study was sufficient to identify problematic items to improve the final Czech FMA, although further studies with a larger sample size are necessary to confirm its validity and reliability in the Czech context.
The use of the FMA worldwide has great significance for clinicians, researchers, and educators in the field of stroke rehabilitation. The current study adds a new official Czech translation, which will allow for wider standardized use of the scale. The FMA is easy to use and does not need any special equipment (28), which makes it easy to use in research and clinical practice.
Strength and limitations
The strength of this current study is in a comprehensive standardized translation and cross-cultural validation procedure carried out in 8 steps. It included 2 forward translations, their comparison, and finalization of the first draft, which was then subjected to backward translation, compared with the original, with step-wise reviewing by a proof-reader as well as a bilingual physiotherapist. The final translation was subsequently tested in a pilot study on 11 post-stroke patients to reveal any possible discrepancies in all the evaluation steps. An important limitation of the current study is that this preliminary reliability evaluation of the Czech FMA provides only limited information on reliability, as only a minor range of possible scores of the FMA were covered in this small sample.
Conclusions
The official translation of the Czech FMA for both the upper and lower extremities was developed in this study. The official Czech FMA is now available for clinical, educational, and scientific use. Systematic post-stroke assessment of sensorimotor function is essential to gain a better understanding of post-stroke motor recovery and to select an appropriate rehabilitation strategy more precisely. The FMA can be successfully used to classify the stroke severity level and to predict recovery outcome. The Czech FMA will allow for appropriate and unified assessment of motor impairment post-stroke and a comparison of the outcomes across countries worldwide. From this perspective, internationally comparable outcomes from the FMA have the potential to add pieces of evidence to improve the quality of rehabilitation in all stages after stroke.
ACKNOWLEDGEMENTS
The authors would like to thank the participants for their contribution and Dagmar Tečová for statistical analysis.
Ethical approval: This study was approved by the Faculty of Health Sciences Ethical committee at Palacký University in Olomouc (UPOL-1703/1040-2020).
Data availability: The data supporting the findings of this study are available via the corresponding author on reasonable request.
REFERENCES
- Feigin VL, Brainin M, Norrving B, et al. World Stroke Organization: Global Stroke Fact Sheet 2025. Int J Stroke 2025; 20: 132–144. https://doi.org/10.1177/17474930241308142
- Gialanella B, Santoro R, Ferlucci C. Predicting outcome after stroke: the role of basic activities of daily living predicting outcome after stroke. Eur J Phys Rehabil Med 2013; 49: 629–637.
- Bryndziar T, Šedová P, Mikulík R. Stroke incidence in Europe: a systematic review. Cesk Slov Neurol N 2017; 80: 180–189. https://doi.org/10.14735/amcsnn2017180
- Institute of Health Information and Statistics of the Czech Republic (ÚZIS). Zdravotnická ročenka 2021 [retrieved 2023 June 23]. Available from: https://www.uzis.cz/index.php?pg=aktuality&aid=8619
- Thayabaranathan T, Kim J, Cadilhac DA, Thrift AG, Donnan GA, Howard G, et al. Global stroke statistics 2022. Int J Stroke 2022; 17: 946–956. https://doi.org/10.1177/17474930221123175
- Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: a systematic review. Lancet Neurol 2009; 8: 741–754. https://doi.org/10.1016/S1474-4422(09)70150-4
- Alt Murphy M, Danielsson A, Sunnerhagen KS. Letter by Murphy et al. regarding article, “Fugl–Meyer assessment of sensorimotor function after stroke: standardized training procedure for clinical practice and clinical trials”. Stroke 2011; 42: e402. https://doi.org/10.1161/STROKEAHA.111.619304
- Burridge J, Alt Murphy M, Buurke J, Feys P, Keller T, Klamroth-Marganska V, et al. A systematic review of international clinical guidelines for rehabilitation of people with neurological conditions: what recommendations are made for upper limb assessment? Front Neurol 2019; 10: 567. https://doi.org/10.3389/fneur.2019.00567
- Santisteban L, Térémetz M, Bleton JP, Baron JC, Maier MA, Lindberg PG. Upper limb outcome measures used in stroke rehabilitation studies: a systematic literature review. PLoS One 2016; 11: e0154792. https://doi.org/10.1371/journal.pone.0154792
- Hernández ED, Galeano CP, Barbosa NE, Forero SM, Nordin Å, Sunnerhagen KS, et al. Intra- and inter-rater reliability of Fugl–Meyer Assessment of Upper Extremity in stroke. J Rehabil Med 2019; 51: 652–659. https://doi.org/10.2340/16501977-2590
- Hernández ED, Forero SM, Galeano CP, Barbosa NE, Sunnerhagen KS, Alt Murphy M. Intra- and inter-rater reliability of Fugl–Meyer Assessment of Lower Extremity early after stroke. Braz J Phys Ther 2020; 25: 709–718. https://doi.org/10.1016/j.bjpt.2020.12.002
- See J, Dodakian L, Chou C, Chan V, McKenzie A, Reinkensmeyer DJ, et al. A standardized approach to the Fugl–Meyer assessment and its implications for clinical trials. Neurorehabil Neural Repair 2013; 27: 732–741. https://doi.org/10.1177/1545968313491000
- Amano S, Umeji A, Uchita A, Hashimoto Y, Takebayashi T, Kanata Y, et al. Reliability of remote evaluation for the Fugl–Meyer assessment and the action research arm test in hemiparetic patients after stroke. Top Stroke Rehabil 2018; 25: 43–47. https://doi.org/10.1080/10749357.2018.1484987
- International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health Organization; 2001.
- Kwakkel G, Lannin NA, Borschmann K, English C, Ali M, Churilov L, et al. Standardized measurement of sensorimotor recovery in stroke trials: consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Neurorehabil Neural Repair 2017; 31: 784–792. https://doi.org/10.1177/1545968317732662
- Lee HC, Kuo FL, Lin YN, Liou TH, Lin JC, Huang SW. Effects of robot-assisted rehabilitation on hand function of people with stroke: a randomized, crossover-controlled, assessor-blinded study. Am J Occup Ther 2021; 75: 7501205020p1–7501205020p11. https://doi.org/10.5014/ajot.2021.038232
- Hernandez A, Bubyr L, Archambault PS, Higgins J, Levin MF, Kairy D. Virtual reality-based rehabilitation as a feasible and engaging tool for the management of chronic poststroke upper-extremity function recovery: randomized controlled trial. JMIR Serious Games 2022; 10: e37506. https://doi.org/10.2196/37506
- Park J, Lee N, Cho M, Kim D, Yang Y. Effects of mental practice on stroke patients’ upper extremity function and daily activity performance. J Phys Ther Sci 2015; 27: 1075–1077. https://doi.org/10.1589/jpts.27.1075
- Rocha LSO, Gama GCB, Rocha RSB, Rocha LB, Dias CP, Santos LLS, et al. Constraint induced movement therapy increases functionality and quality of life after stroke. J Stroke Cerebrovasc Dis 2021; 30: 105774. https://doi.org/10.1016/j.jstrokecerebrovasdis.2021.105774
- Hara T, Niimi M, Yamada N, Shimamoto Y, Masuda G, Hara H, et al. Prognosis prediction of the effect of botulinum toxin therapy and intensive rehabilitation on the upper arm function in post-stroke patients using hierarchical cluster analysis. Disabil Rehabil 2022; 44: 6815–6823. https://doi.org/10.1080/09638288.2021.1977394
- Fugl–Meyer AR, Jääskö L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient. 1. A method for evaluation of physical performance. Scand J Rehabil Med 1975; 7: 13–31. https://doi.org/10.2340/1650197771331
- Sullivan JE, Crowner BE, Kluding PM, Nichols D, Rose DK, Yoshida R, et al. Outcome measures for individuals with stroke: process and recommendations from the American Physical Therapy Association neurology section task force. Phys Ther 2013; 93: 1383–1396. https://doi.org/10.2522/ptj.20120492
- Cruchinho P, López-Franco MD, Capelas ML, Almeida S, Bennett PM, Miranda da Silva M, et al. Cross-cultural adaptation, and validation of measurement instruments: a practical guideline for novice researchers. J Multidiscip Healthc 2024; 17: 2701–2728. https://doi.org/10.2147/JMDH.S419714
- Busk H, Alt Murphy M, Korsman R, Skou ST, Wienecke T. Cross-cultural translation and adaptation of the Danish version of the Fugl–Meyer assessment for post stroke sensorimotor function. Disabil Rehabil 2022; 44: 4888–4895. https://doi.org/10.1080/09638288.2021.1919215
- Cecchi F, Carrabba C, Bertolucci F, Castagnoli C, Falsini C, Gnetti B, et al. Transcultural translation and validation of Fugl–Meyer assessment to Italian. Disabil Rehabil 2021; 43: 3717–3722. https://doi.org/10.1080/09638288.2020.1746844
- Kim TL, Hwang SH, Lee WJ, Hwang JW, Cho I, Kim EH, et al. The Korean version of the Fugl–Meyer Assessment: reliability and validity evaluation. Ann Rehabil Med 2021; 45: 83–98. https://doi.org/10.5535/arm.20225
- Onose G, Anghelescu A, Ionescu A, Tataranu LG, Spînu A, Bumbea AM, et al. Translation of the Fugl–Meyer assessment into Romanian: transcultural and semantic-linguistic adaptations and clinical validation. Front Neurol 2023; 13: 1022546. https://doi.org/10.3389/fneur.2022.1022546
- Barbosa NE, Forero SM, Galeano CP, Hernández ED, Landinez NS, Sunnerhagen KS, et al. Translation and cultural validation of clinical observational scales: the Fugl–Meyer assessment for post stroke sensorimotor function in Colombian Spanish. Disabil Rehabil 2019; 41: 2317–2323. https://doi.org/10.1080/09638288.2018.1464604
- Ikram M, Rehman S, Sunnerhagen K, Alt Murphy M. Urdu translation and cross-cultural validation of the Fugl–Meyer assessment in people with stroke. Disabil Rehabil 2022; 44: 8048–8053. https://doi.org/10.1080/09638288.2021.2003449
- Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000; 25: 3186–3191. https://doi.org/10.1097/00007632-200012150-00014
- Sousa VD, Rojjanasrirat W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J Eval Clin Pract 2011; 17: 268–274. https://doi.org/10.1111/j.1365-2753.2010.01434.x
- Svensson E. Different ranking approaches defining association and agreement measures of paired ordinal data. Stat Med 2012; 31: 3104–3117. https://doi.org/10.1002/sim.5382
- Svensson E, Holm S. Separation of systematic and random differences in ordinal rating scales. Stat Med 1994; 13: 2437–2453. https://doi.org/10.1002/sim.4780132308
- Duncan Millar J, van Wijck F, Pollock A, Ali M. Outcome measures in post-stroke arm rehabilitation trials: do existing measures capture outcomes that are important to stroke survivors, carers, and clinicians? Clin Rehabil 2019; 33: 737–749. https://doi.org/10.1177/0269215518823248
- Kim H, Her J, Ko J, Park DS, Woo JH, You Y, et al. Reliability, concurrent validity, and responsiveness of the Fugl–Meyer Assessment (FMA) for hemiplegic patients. J Phys Ther Sci 2012; 24: 893–899. https://doi.org/10.1589/jpts.24.893
- Gladstone DJ, Danells CJ, Black SE. The Fugl–Meyer assessment of motor recovery after stroke: a critical review of its measurement properties. Neurorehabil Neural Repair 2002; 16: 232–240. https://doi.org/10.1177/154596802401105171
- Lee HH, Kim DY, Sohn MK, Shin YI, Oh GJ, Lee YS, et al. Revisiting the proportional recovery model in view of the ceiling effect of Fugl–Meyer Assessment. Stroke 2021; 52: 3167–3175. https://doi.org/10.1161/STROKEAHA.120.032409
- Hawe RL, Scott SH, Dukelow SP. Taking proportional out of stroke recovery. Stroke 2019; 50: 204–211. https://doi.org/10.1161/STROKEAHA.118.023006
- Kristersson T, Persson HC, Alt Murphy M. Evaluation of a short assessment for upper extremity activity capacity early after stroke. J Rehabil Med 2019; 51: 257–263. https://doi.org/10.2340/16501977-2534
- Sullivan KJ, Tilson JK, Cen SY, Rose DK, Hershberg J, Correa A, et al. Fugl–Meyer assessment of sensorimotor function after stroke: standardized training procedure for clinical practice and clinical trials. Stroke 2011; 42: 427–432. https://doi.org/10.1161/STROKEAHA.110.592766
- Boyd LA, Hayward KS, Ward NS, Stinear CM, Rosso C, Fisher RJ, et al. Biomarkers of stroke recovery: consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int J Stroke 2017; 12: 480–493. https://doi.org/10.1177/1747493017714176
- Woytowicz EJ, Rietschel JC, Goodman RN, Conroy SS, Sorkin JD, Whitall J, et al. Determining levels of upper extremity movement impairment by applying a cluster analysis to the Fugl–Meyer Assessment of the upper extremity in chronic stroke. Arch Phys Med Rehabil 2017; 98: 456–462. https://doi.org/10.1016/j.apmr.2016.06.023
- Huynh BP, DiCarlo JA, Vora I, Ranford J, Gochyyev P, Lin DJ, et al. Sensitivity to change and responsiveness of the upper extremity Fugl–Meyer assessment in individuals with moderate to severe acute stroke. Neurorehabil Neural Repair 2023; 37: 545–553. https://doi.org/10.1177/15459683231186985
- Hiragami S, Inoue Y, Harada K. Minimal clinically important difference for the Fugl–Meyer assessment of the upper extremity in convalescent stroke patients with moderate to severe hemiparesis. J Phys Ther Sci 2019; 31: 917–921. https://doi.org/10.1589/jpts.31.917
- Pandian S, Arya KN, Kumar D. Minimal clinically important difference of the lower-extremity Fugl–Meyer assessment in chronic-stroke. Top Stroke Rehabil 2016; 23: 233–239. https://doi.org/10.1179/1945511915Y.0000000003
- Prabhakaran S, Zarahn E, Riley C, Speizer A, Chong JY, Lazar RM, et al. Inter-individual variability in the capacity for motor recovery after ischemic stroke. Neurorehabil Neural Repair 2008; 22: 64–71. https://doi.org/10.1177/1545968307305302
- Winters C, van Wegen EE, Daffertshofer A, Kwakkel G. Generalizability of the proportional recovery model for the upper extremity after an ischemic stroke. Neurorehabil Neural Repair 2015; 29: 614–622. https://doi.org/10.1177/1545968314562115
- Smith MC, Byblow WD, Barber PA, Stinear CM. Proportional recovery from lower limb motor impairment after stroke. Stroke 2017; 48: 1400–1403. https://doi.org/10.1161/STROKEAHA.116.016478
- Ghaziani E, Couppé C, Siersma V, Christensen H, Magnusson SP, Sunnerhagen KS, et al. Easily conducted tests during the first week post-stroke can aid the prediction of arm functioning at 6 months. Front Neurol 2019; 10: 1371. https://doi.org/10.3389/fneur.2019.01371
- Hochleitner I, Pellicciari L, Castagnoli C, Paperini A, Politi AM, Campagnini S, et al. Intra- and inter-rater reliability of the Italian Fugl–Meyer assessment of upper and lower extremity. Disabil Rehabil 2023; 45: 2989–2999. https://doi.org/10.1080/09638288.2022.2114553
- Wiesner K, Schwarz A, Meya L, Kaufmann JE, Traenka C, Luft AR, et al. Interrater reliability of the Fugl–Meyer Motor assessment in stroke patients: a quality management project within the ESTREL study. Front Neurol 2024; 15: 1335375. https://doi.org/10.3389/fneur.2024.1335375
- Prange-Lasonder GB, Alt Murphy M, Lamers I, Hughes AM, Buurke JH, Feys P, et al. European evidence-based recommendations for clinical assessment of upper limb in neurorehabilitation (CAULIN): data synthesis from systematic reviews, clinical practice guidelines and expert consensus. J NeuroEngineering Rehabil 2021; 18: 162. https://doi.org/10.1186/s12984-021-00951-y
- Van Criekinge T, Heremans C, Burridge J, et al. Standardized measurement of balance and mobility post-stroke: consensus-based core recommendations from the third Stroke Recovery and Rehabilitation Roundtable. Neurorehabil Neural Repair 2023; 38: 41–51. https://doi.org/10.1177/15459683231209154