ORIGINAL REPORT
TEST-RETEST AND INTER-RATER RELIABILITY OF THE 20-METER AMBULATION TEST IN PATIENTS WITH PARKINSON‘S DISEASE
Emilie HUTIN, PhD1,2, Mouna GHÉDIRA, PT, PhD1,2, Valentina MARDALE, MD1, Mina BOUTOU, MSc1, Tharaga SANTIAGO, PT, MSc1, Sandrine JOUDOUX, PT, MSc1, Caroline GAULT-COLAS, MD1, Jean-Michel GRACIES, MD, PhD1,2 and Nicolas BAYLE, MD, MSc1,2
From the 1Laboratoire Analyse et Restauration du Mouvement, Service de Rééducation Neurolocomotrice, Hôpitaux Universitaires Henri Mondor, Assistance Publique-Hôpitaux de Paris, and 2UR 7377 Bioingénierie, Tissus et Neuroplasticité, Université Paris-Est Créteil Val de Marne
Objective: In patients with Parkinson’s disease, limited sit-to-stand, walk and turn contribute to decreased independence and quality of life. The 20-meter Ambulation Test (AT20) evaluates walking a total of 20 m, over a 10-m distance, back and forth between 2 chairs, starting and ending in a seated position. The aim of this study was to evaluate test-retest and inter-rater reliability of the AT20 in patients with Parkinson’s disease.
Methods: Patients with idiopathic Parkinson’s disease performed the AT20 in 3 conditions: free speed, fast speed, and with large steps, twice 1 week apart. The total number of steps and the time to complete the task were recorded manually by 4 independent raters. The main outcome criteria were the test-retest and inter-rater intraclass correlation coefficients and coefficients of variation for speed, step length and cadence in the 3 conditions.
Results: Twenty participants completed the 2 visits. Across all conditions, test-retest and inter-rater intraclass correlation coefficients for step length and speed were > 95%. Test-retest and inter-rater coefficients of variation were < 0.08.
Conclusion: The AT20 is a reliable ambulation test in Parkinson’s disease, with excellent test-retest and inter-rater reliability for step length and speed in all 3 conditions: at free speed, fast speed, and with large steps. The AT20 might be useful to assess ambulation in parkinsonism in clinical practice.
LAY ABSTRACT
In patients with Parkinson’s disease, limited sit-to-stand, walk and turn contribute to decreased autonomy and quality of life. The 20-meter Ambulation Test (AT20) evaluates walking for a total of 20 m, over a 10 m distance, back and forth between 2 chairs, starting and ending in a seated position. The aim of the current study was to evaluate test-retest and inter-rater reliability for speed, step length and cadence measurement using the AT20 in subjects with Parkinson’s disease. Twenty patients with idiopathic Parkinson’s disease performed the AT20 in 3 conditions: free speed, fast speed, and with large steps, twice 1 week apart. The total number of steps and the time to complete the task were recorded manually by 4 independent raters. The AT20 is a reliable ambulation test in Parkinson’s disease, with excellent reliability between tests and between raters in all 3 conditions: free speed, fast speed, and with large steps. The AT20 might be useful in clinical practice to assess ambulation disorders in patients with parkinsonism.
Key words: gait; movement; hypokinesia; rehabilitation.
Citation: J Rehabil Med 2023; 55: jrm00378. DOI: https://doi.org/10.2340/jrm.v55.4381
Copyright: © Published by Medical Journals Sweden, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Jan 19, 2023; Published: Mar 21, 2023
Correspondence address: Emilie Hutin, Laboratoire Analyse et Restauration du Mouvement, Service de Rééducation Neurolocomotrice, Hôpital Henri Mondor, 51, avenue du Maréchal de Lattre de Tassigny, FR-94000 Créteil, France. E-mail: emilie.hutin@aphp.fr
Competing interests and funding: The authors have no conflicts of interest to declare.
Slow gait, short steps, festination and balance impairment are classic clinical features of linear ambulation in persons with Parkinson’s disease (1). However, there are additional features that are equally important in altering functional capacities and perceived quality of life. Weakness, predominating in extensor muscles, challenges the patient’s sit-to-stand capacity, i.e. their access to walking (2, 3). Impaired axial rotation of the spine, with reduced dissociation between head, trunk and pelvis rotation increases the risk of falling (4, 5) and perceived disability (6). Finally, repeated movements (such as walking steps) may deteriorate in amplitude and regularity if the number of required repetitions is sufficient (7, 8) and walking velocity may deteriorate over longer distances (9). Overall, real-life ambulation combines standing up from a chair, linear walking for several metres and turning to sit down, which are also affected in subjects with Parkinson’s disease. It therefore seems appropriate to assess all of these components, in order to better evaluate real-life ambulation capacities in patients with Parkinson’s disease. Therefore, a functional ecological test (i.e. assessment of the patient own abilities in daily life), which includes a sufficient walking distance and numbers of turns, stand-to-sit and sit-to-stand, may be a sensitive test to assess ambulatory function in parkinsonism.
A number of laboratory-based gait measures have been reported to be valid and reliable in assessing gait parameters in patients with parkinsonian syndromes, but these are time-consuming, expensive and have little applicability in clinical routine (10–13). On the other hand, simple, reliable and quantified clinical walking tests (i.e. non-instrumental measurement) have been suggested to assess gait in patients with Parkinson’s disease, such as the timed up-and-go test (14–16), 5- to 10-m walk tests (15–18), the L-test (19) and the 6-min walk test (16, 17). However, these tests usually involve short walking distance, potentially hampering the observation of mild festination, in particular in mild to moderate stages of the disease (9), or do not incorporate sit-to-stand and u-turn tasks, which are systematically associated with walking in daily life. The L-test meets these criteria, but requires large spaces, which are often not available in clinical centres (19). Finally, the reliability of these walking tests may vary, depending on testing conditions, such as walking at comfortable speed or with an imposed gait condition (e.g. fast velocity or large step length), the use of walking aids or dopaminergic medication state.
In an attempt to better reflect real-life functional mobility in patients with Parkinson’s disease, we have developed the 20-meter ambulation test (AT20, Fig. 1), to evaluate the 3 main parameters of gait (speed, step length and cadence) without sensors placed on the patient. The AT20 is thus a modified timed up-and-go test, which evaluates walking over a total of 20 m, walked over a 10-m distance, back and forth between 2 chairs, starting and ending in a seated position, with 2 u-turns, 2 sit-to-stands and 2 stand-to-sit transfers. The 2 main changes that distinguish the AT20 from the timed up-and-go test are the increase in walking distance and the formalization of 3 conditions of test (formalization is allowed by the longer distance used) to perform quantitative comparisons and ratios to estimate: the natural walking of the patient (free speed), the ability to accelerate and the step length regulation during speed increase (fast speed) (20), and the ability to lengthen steps (with large steps). The relatively long distance used in the AT20 (20 m) thus enables an overview of the real-life ambulation capacities in patients, including the difficulties occurring across step repetitions (step length decrement, festination, and freezing). The patient is always tested in the clinically defined levodopa-off state, without the use of walking aids.
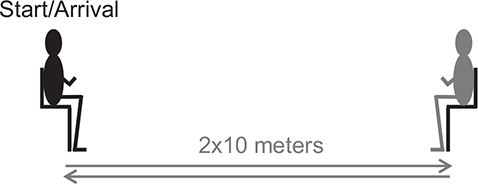
Fig. 1. The 20-m ambulation test (AT20). The AT20 evaluates walking over a 20 m total distance back and forth between 2 chairs, 10 m apart, starting and ending in a seated position.
The aim of the current study is to evaluate test-retest and inter-rater reliability for speed, step length, and cadence measurements, using AT20 at free speed, at fast speed and with large steps, in patients with Parkinson’s disease.
METHODS
Ethics
This prospective, non-interventional protocol to evaluate the reliability of assessments routinely performed at our centre was conducted in the Analysis and Restoration of Movement laboratories at Henri Mondor Hospital, Créteil, France, and registered at Agence Nationale de Sécurité du Médicament et des produits de santé (ANSM registration number, ID-RCB: 2017-A00367-46). The study was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki 1975), and Good Clinical Practice guidelines. All participants were informed about the study and attested in writing to their non-opposition to the use of their anonymous data for this research. The study complied with all mandatory laboratory health and safety procedures. The manuscript meets the Strengthening the Reporting of Observational Studies in Epidemiology guidelines (21).
Inclusion criteria
Subjects were invited to participate in the study if they were diagnosed with idiopathic Parkinson’s disease, based on the United Kingdom-Parkinson’s Disease Society Brain Bank (UK-PDSBB) criteria (7), were ambulatory, able to walk over a distance of 20 m without aids or anti-Parkinson’s medications, and did not have any intercurrent medical condition preventing them from participating in 2 consecutive ambulation tests twice 1 week apart.
Procedures
Following classical guidelines, assessments were performed in the clinically defined off status after withdrawal of levodopa for 12 h (“off” phase of the medication cycle), or of dopaminergic agonists or slow-release forms of levodopa for 24 h. The AT20 started with the subject seated on the first chair. They were asked to stand up, walk a distance of 10 m, make a 180° turn then sit in the second chair, stand up again, walk 10 m back to the starting point, turn 180° and sit back down on the first chair. The total number of steps was counted manually, including the small steps necessary for each u-turn. The time of completion was measured using a stopwatch, from the onset of the sit-to-stand task (“backside lifted off “) to the end of the stand-to-sit task (“backside back on”).
In the current study, participants performed the AT20, with shoes and without assistive devices or human assistance, in 3 conditions in the following, systematic order: at “natural” speed (free speed), at maximal safe speed (fast speed), and while using steps that were as long as possible (with large steps). Those 3 tests were run twice 1 week apart (test and retest) by 4 independent raters with a mean (95% CI) of 7 (1) years of experience in evaluating gait with parkinsonism: 1 physician, 2 physiotherapists and 1 engineer in biomechanics. The 4 raters participated together in a single specific training session, in which the AT20 methods were agreed upon before the start of the study.
Outcome measures
This study determined the mean ambulation characteristics, speed, step length and cadence (step frequency) from the time recorded, and the number of steps was counted manually over the whole ambulation test, at free speed, maximal speed, and with large steps. Ambulation speed was calculated by dividing the length of the walkway (i.e. 20 m) by the elapsed time, measured using the stopwatch, and the cadence was calculated by dividing the total number of steps by the elapsed time. The parameter step length was defined as the total number of metres covered in the test (i.e. 20 m) divided by the total number of steps, counted as described above; thus the “angular” displacement of each u-turn was not accounted for with this definition of step length.
Statistical analysis
For all dependent variables, data normality was tested using Kolmogorov-Smirnov tests. Descriptive statistics were used to present the mean, minimal and maximal values and 95% confidence intervals (95% CI) for the variables considered (age, time since diagnosis, ambulation speed, step length, and cadence), or median and interquartile differences depending on the conditions of normality. For this reliability study, the number of subjects was arbitrarily set at 30. Inter-rater reliability was assessed using intraclass correlation coefficients (ICC (2, 1), absolute agreement) (22, 23), coefficients of variation (standard deviation over mean) and mean absolute differences between ambulation parameters at the first (test) and the second (retest) session for each rater. The assumption was that raters were randomly selected among rehabilitation professionals and that the results could be generalized to any similar raters in the field. The level of agreement was defined as excellent above 90%, good between 75% and 90%, moderate between 50% and 70%, and poor below 50% (24). To assess test-retest reliability, intraclass correlation coefficients, coefficients of variation and mean absolute differences were calculated for the ambulation parameters measured in the 2 sessions 1 week apart for each condition. Coefficients of variation and mean absolute differences were compared between the 3 conditions (free speed vs fast speed vs large steps) and the 3 parameters measured (speed vs step length vs cadence) using repeated measures analysis of variance (ANOVA) and Bonferroni corrections.
RESULTS
Participants
Among the 30 patients with idiopathic Parkinson’s disease enrolled in the study to participate in the test and retest visits, 3 missed the first appointment (visit “test”) and another missed the second appointment (visit “retest)”. Among the 26 participants who made the 2 visits, 6 patients were in the clinically defined “on” status within less than 12 h of taking levodopa at the first visit (test) or at the second visit (retest). Overall, the data from 20 patients could be analysed for the study (mean (95% CI) [minimum value–maximum value], age 65 years (4) [50–80], time since diagnosis 6 (2) [2–17] years). Mean walking ambulation parameters at test and retest are shown in Table I.
Test-retest reliability
The test-retest and inter-rater reliability results are presented by condition (free speed, fast speed, and with large steps) in Fig. 2. Across all conditions, mean test-retest intraclass correlation coefficients were all greater than 76% (speed, 0.96 (0.01); step length, 0.96 (0.02); cadence, 0.84 (0.03), Fig. 2A). Mean test-retest coefficients of variation were 0.06 (0.07) for speed, 0.04 (0.04) for step length, and 0.05 (0.04) for cadence (Fig. 2B). Mean test-retest absolute differences were 0.08 (0.08) m/s in speed, 0.04 (0.04) m in step length, and 0.11 (0.10) step/s in cadence (Fig. 2C).
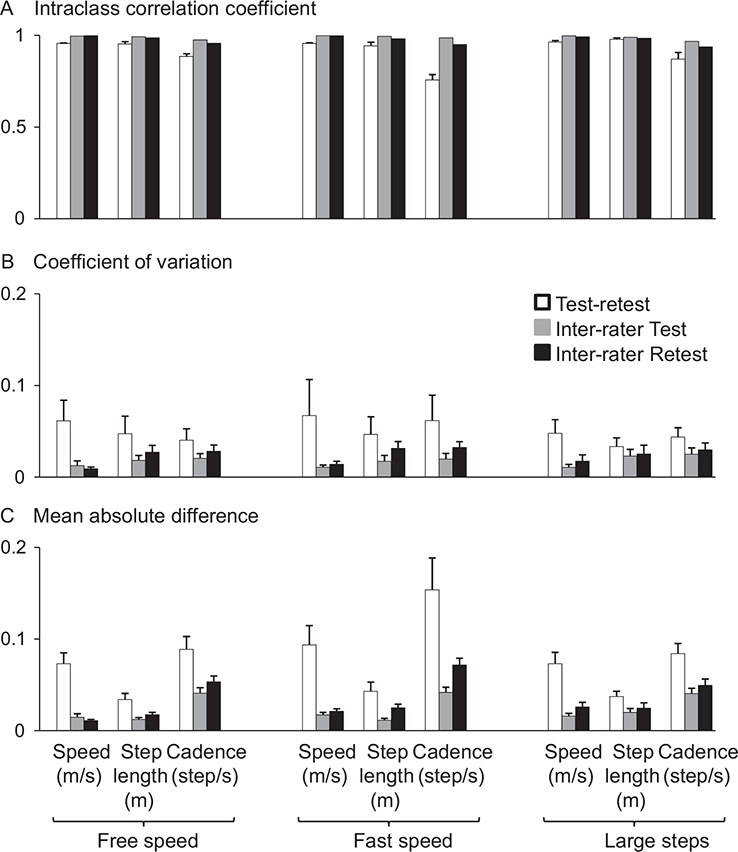
Fig. 2. Intraclass correlation coefficients, coefficients of variation and mean absolute differences. The results are expressed in mean (SD) of the 4 raters and the 20 patients for (A) the intraclass correlation coefficients, (B) coefficients of variation, and (C) mean absolute differences. Mean absolute differences are expressed in m/s for speed, m for step length and step/s for cadence.
Inter-rater reliability
Mean inter-rater intraclass correlation coefficients were all greater than 95% (speed 0.997 (0.003); step length 0.99 (0.01); cadence 0.96 (0.02), Fig. 2A). Mean inter-rater coefficients of variation were 0.01 (0.01) for speed, 0.02 (0.02) for step length, and 0.03 (0.02) for cadence (Fig. 2B). Mean inter-rater absolute differences were 0.02 (0.02) m/s for speed, 0.02 (0.02) m for step length, and 0.05 (0.03) step/s for cadence (Fig. 2C).
Effects of conditions and measurements on test-retest reliability
The test-retest coefficients of variation were similar in all conditions and for all walking parameters (non significant). However, the test-retest mean absolute differences proved lower for the step length parameter (ANOVA, measurement effect, p = 8.10–6; Bonferroni, step length vs speed, p = 0.006; step length vs cadence, p = 5×10–6; Fig. 1C) and higher for cadence at fast speed compared with the other conditions and the other measurements (ANOVA, condition*measurements, p = 0.04; Bonferroni, cadence at fast speed walking vs each other measurements, p < 0.01).
DISCUSSION
Test-retest and inter-rater reliability of manually calculated speed, step length and cadence measurements in the AT20 were found to be excellent in patients with Parkinson’s disease in each of the 3 tested walking conditions: free speed, fast speed, and with large steps, step length being the most reliable parameter.
AT20: a reliable manual evaluation of ambulation
The current overall reliability results are at least as good as those collected from previous studies using electronic equipment for 2- or 3-dimensional spatial-temporal measurements (12, 13) or clinical routine tests (14–18). The multiple tasks of ambulation used in AT20 (2 full turns, 2 sit-to-stand and 2 stand-to-sit transfers) and its relatively long distance thus do not seem to impact, and may even improve, the previously reported reliability of ambulation assessments in patients with Parkinson’s disease. This study found that gait performances of subjects remained quite stable 1 week apart: the differences in speed were mostly below the known minimal detectable change (16, 17). In addition, the 2 additional “imposed” gait patterns (fast speed and large steps conditions), which therefore involved internal cueing (25), did not seem to affect reliability. Therefore, the more comprehensive evaluation of ambulation of AT20 vs the timed up-and-go test, due to the longer distance and 3 conditions tested, might be of considerable interest for the follow-up of patients with Parkinson’s disease. Lastly, having such moderately advanced patients walk in the practically-defined “off”-medication state and without the use of walking aids, imposed maximal strain on the neuromuscular system, which proved to be feasible and safe, and probably helped to optimize the reliability of the assessments (26). Further investigations could test the reliability of the AT20 in the “on”-medication state and/or with the use of walking aids, and evaluate the modifications of ambulation with these chemical and physical assistances.
Step length: a valuable measurement in Parkinson’s disease
In contrast to most of the walking tests in the literature, the methodology of the current study did not require to separate straight-line walking from turning, since all steps were counted, from the first sit-to-stand to the last stand-to-sit, u-turns included. The AT20 thus takes into account the number of steps used to cover the distance of 20 m and the 2 u-turns, which makes measurements of step length and cadence easy, in the same way, speed calculation is quite easy using a stopwatch. The current study shows that cadence measurement at fast speed might have slightly lower reliability, while step length is the most reliable test-retest and inter-rater measurement for all walking conditions (test-retest mean absolute differences, p < 0.01). The cadence measurement is impacted by the potential cumulated lack of accuracy of 2 manual measures, of the number of steps and the number of seconds using a stopwatch, in potentially difficult conditions, such as with festination or freezing of gait episodes, or faster walking; this may explain the lesser reliability. Yet, the reliability of the cadence measurement remains good in all conditions tested (ICC > 75%).
Specifically, the measurement of step length is a functional assessment of parkinsonian hypometria and is highly test-retest and inter-rater reliable, making it highly relevant in the assessment of parkinsonian ambulation. In addition, step length regulation is impaired in Parkinson’s disease, while the ability to modulate ambulation cadence is relatively preserved (20, 26). Of note, freezing episodes were not specifically inventoried; the clinician counted each step used for the whole ambulation task, i.e. when each foot was completely “off the ground”, whether or not it occurred during freezing episodes. A systematic video analysis classically complements the AT20 to discriminate the performances of each ambulation tasks (27), with an expected increase in step consumption during u-turns (28), and the possibility of detecting episodes of freezing of gait.
Three test conditions for better understanding of ambulation impairments in Parkinson’s disease
In patients with Parkinson’s disease, the ability to walk is classically tested at comfortable speed; investigators do not assess walking abilities at fast speed as often (20). The AT20 tests 3 walking conditions that challenge the patient, the latter 2 providing 2 different types of cueing: 1: free speed; 2: fast speed; and 3: with large steps. Ambulation uses considerable attention, becoming less automatic from the early stages of the disease (29). Thus, walking ability at free speed is an essential marker of the disease at any stage, which reflects everyday walking well. Walking at faster speed leads the patient to achieve faster, and if possible larger, coordinated movements. In patients with Parkinson’s disease, besides the presence of bradykinesia and hypometria on each movement, fast walking is limited by the failed temporal and spatial scaling of movements according to the targeted walking speed (20), which is almost automatic in healthy subjects. This condition of test might exacerbate the difficulties already present in comfortable walking, or reveal those that are not yet perceptible, and thus may contribute to better characterization of the ambulation difficulties in the early stages. In addition, the relative contribution of step lengthening to ambulation speed increase (observed comparing free and fast walking speed) is a marker of advancement of Parkinson’s disease (20). The final condition of the test, walking with large steps, requires the patient to focus attention on step amplitude; the degree of functional hypometria in the lower limbs is then measurable alone, by calculating the difference between natural step length and maximal step length, therefore showing a form of “step length reserve”. Overall, this step-wise evaluation may end up guiding rehabilitation care: for example, towards re-learning to walk with increased attention (in case of step length impairment associated with normal cadence at free speed, or of lack of step length modulation between free and fast speed) using a cueing method (30), or towards motor strengthening for improving range of motion of hip, knee and ankle flexion-extension (in case of poor step length reserve when walking with large steps) (31).
Study limitations
The study was not designed to evaluate potential variations in the reliability of the AT20 with the stage of Parkinson’s disease or time since diagnosis, as the small sample size does not allow stratification to explore the effects of the severity of motor disorders on the reliability of the test. The only inclusion criterion related to motor ability was the ability to walk for a distance of 20 m without assistance or any anti-Parkinson drugs. In fact, the relatively good mean speed of free ambulation (0.92 m/s) suggests that the participants were in the early to moderate stages of the disease. The use of the AT20 could be challenged in more advanced stages of the disease, when the walking perimeter becomes small. Given the number of missing data, results may need to be confirmed using a larger sample (at least 30 subjects) (24). In addition, ecological validation of the AT20 may be important in the future. This would involve validating the results of the AT20 against the number of steps performed in daily life (pedometer) and ambulation classifications related to disease stage.
CONCLUSION
In the clinic, the performance of the AT20 in the 3 tested conditions reveals the state of spontaneous walking (free speed), the management modalities of the need to accelerate (fast speed walking), and spontaneous hypometria by measuring the step length reserve (walking with large steps). The results of this study may be used as the basis of choice of outcome criteria in future clinical trials in patients with Parkinson’s disease.
REFERENCES
- Snijders AH, van de Warrenburg BP, Giladi N, Bloem BR. Neurological gait disorders in elderly people: clinical approach and classification. Lancet Neurol 2007; 6: 63–74. DOI: 10.1016/S1474-4422(06)70678-0
- Nogaki H, Kakinuma S, Morimatsu M. Muscle weakness in Parkinson’s disease: a follow-up study. Parkinsonism Relat Disord 2001; 8: 57–62. DOI: 10.1016/s1353-8020(01)00002-5
- Robichaud JA, Pfann KD, Comella CL, Brandabur M, Corcos DM. Greater impairment of extension movements as compared to flexion movements in Parkinson’s disease. Exp Brain Res 2004; 156: 240–254. DOI: 10.1007/s00221-003-1782-0.
- Crenna P, Carpinella I, Rabuffetti M, Calabrese E, Mazzoleni P, Nemni R, et al. The association between impaired turning and normal straight walking in Parkinson’s disease. Gait Posture 2007; 26: 172–178. DOI: 10.1016/j.gaitpost.2007.04.010
- Spildooren J, Vercruysse S, Heremans E, Galna B, Vandenbossche J, Desloovere K, et al. Head-pelvis coupling is increased during turning in patients with Parkinson’s disease and freezing of gait. Mov Disord 2013; 28: 619-625. DOI: 10.1002/mds.25285
- Stack E, Ashburn A. Dysfunctional turning in Parkinson’s disease. Disabil Rehabil 2008; 30: 1222–1229. DOI: 10.1080/09638280701829938
- Gibb WR, Lees AJ. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson’s disease. J Neurol Neurosurg Psychiatry 1988; 51: 745–752. DOI: 10.1136/jnnp.51.6.745
- Ling H, Massey LA, Lees AJ, Brown P, Day BL. Hypokinesia without decrement distinguishes progressive supranuclear palsy from Parkinson’s disease. Brain 2012; 135: 1141–1153. DOI: 10.1093/brain/aws038
- Canning CG, Ada L, Johnson JJ, McWhirter S. Walking capacity in mild to moderate Parkinson’s disease. Arch Phys Med Rehabil 2006; 87: 371–375. DOI: 10.1016/j.apmr.2005.11.021
- Cuzzolin F, Sapienza M, Esser P, Saha S, Franssen MM, Collett J, et al. Metric learning for Parkinsonian identification from IMU gait measurements. Gait Posture 2017; 54: 127–132. DOI: 10.1016/j.gaitpost.2017.02.012
- Rennie L, Löfgren N, Moe-Nilssen R, Opheim A, Dietrichs E, Franzén E. The reliability of gait variability measures for individuals with Parkinson’s disease and healthy older adults – the effect of gait speed. Gait Posture 2018; 62: 505–509. DOI: 10.1016/j.gaitpost.2018.04.011
- Geerse DJ, Coolen B, Roerdink M. Quantifying spatiotemporal gait parameters with hololens in healthy adults and people with Parkinson’s disease: test-retest reliability, concurrent validity, and face validity. Sensors (Basel) 2020; 20: 3216. DOI: 10.3390/s20113216
- Lee YY, Li MH, Luh JJ, Tai CH. Reliability of using foot-worn devices to measure gait parameters in people with Parkinson’s disease. NeuroRehabilitation 2021; 49: 57–64. DOI: 10.3233/NRE-210101
- Morris S, Morris ME, Iansek R. Reliability of measurements obtained with the Timed “Up & Go” test in people with Parkinson disease. Phys Ther 2001; 81: 810–818. DOI: 10.1093/ptj/81.2.810
- Lim LI, van Wegen EE, de Goede CJ, Jones D, Rochester L, Hetherington V, et al. Measuring gait and gait-related activities in Parkinson’s patients own home environment: a reliability, responsiveness and feasibility study. Parkinsonism Relat Disord 2005; 11: 19–24. DOI: 10.1016/j.parkreldis.2004.06.003
- Steffen T, Seney M. Test-retest reliability and minimal detectable change on balance and ambulation tests, the 36-item short-form health survey, and the unified Parkinson disease rating scale in people with parkinsonism. Phys Ther 2008; 88: 733–746. DOI: 10.2522/ptj.20070214
- Combs SA, Diehl MD, Filip J, Long E. Short-distance walking speed tests in people with Parkinson disease: reliability, responsiveness, and validity. Gait Posture 2014; 39: 784–788. DOI: 10.1016/j.gaitpost.2013.10.019
- Lang JT, Kassan TO, Devaney LL, Colon-Semenza C, Joseph MF. Test-retest reliability and minimal detectable change for the 10-meter walk test in older adults with Parkinson’s disease. J Geriatr Phys Ther 2016; 39: 165–170. DOI: 10.1519/JPT.0000000000000068
- Haas B, Clarke E, Elver L, Gowman E, Mortimer E, Byrd E. The reliability and validity of the L-test in people with Parkinson’s disease. Physiotherapy 2019; 105: 84–89. DOI: 10.1016/j.physio.2017.11.218
- Bayle N, Patel AS, Crisan D, Guo LJ, Hutin E, Weisz DJ, et al. Contribution of step length to increase walking and turning speed as a marker of Parkinson’s disease progression. PLoS One 2016; 11: e0152469. DOI: 10.1371/journal.pone.0152469
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 2007; 370: 1453–1457. DOI: 10.1016/S0140-6736(07)61602-X
- Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull 1979; 86: 420–428. DOI: 10.1037//0033-2909.86.2.420
- Park MS, Kang KJ, Jang SJ, Lee JY, Chang SJ. Evaluating test-retest reliability in patient-reported outcome measures for older people: a systematic review. Int J Nurs Stud 2018; 79: 58–69. DOI: 10.1016/j.ijnurstu.2017.11.003
- Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 2016; 15: 155–163. DOI: 10.1016/j.jcm.2016.02.012.
- Morris ME, Iansek R, Matyas TA, Summers JJ. Stride length regulation in Parkinson’s disease. Normalization strategies and underlying mechanisms. Brain 1996; 119: 551–568. DOI: 10.1093/brain/119.2.551
- Anderson ED, Horak FB, Lasarev MR, Nutt JG. Performance of a motor task learned on levodopa deteriorates when subsequently practiced off. Mov Disord 2014; 29: 54–60. DOI: 10.1002/mds.25702
- Li T, Chen J, Hu C, Ma Y, Wu Z, Wan W, et al. Automatic timed up-and-go sub-task segmentation for Parkinson’s disease patients using video-based activity classification. IEEE Trans Neural Syst Rehabil Eng 2018; 26: 2189–2199. DOI: 10.1109/TNSRE.2018.2875738
- Huxham F, Baker R, Morris ME, Iansek R. Footstep adjustments used to turn during walking in Parkinson’s disease. Mov Disord 2008; 23: 817–823. DOI: 10.1002/mds.21932
- Parkinson J. Essay on the shaking palsy. London: Whittingham and Rowland; 1817.
- Nieuwboer A, De Weerdt W, Dom R, Truyen M, Janssens L, Kamsma Y. The effect of a home physiotherapy program for persons with Parkinson’s disease. J Rehabil Med 2001; 33: 266–272. DOI: 10.1080/165019701753236455
- Gracies JM. Neurorééducation des syndromes parkinsoniens [Neurorehabilitation in parkinsonian syndromes]. Rev Neurol (Paris) 2010; 166: 196–212 (in French). DOI: 10.1016/j.neurol.2009.10.026