REVIEW ARTICLE
BETTER SLEEP IS ASSOCIATED WITH IMPROVED MOBILITY IN ADULTS: A SCOPING REVIEW
Catherine SIENGSUKON, PT, PhD1, Mahya BEHESHTI, MD2, Sarah J. DONKERS, PT, PhD3, Silvana L. COSTA, PhD4,5, Prasanna VADUVATHIRIYAN, MLS6, Allison GLASER, MPH1, Garrett BABER, MA1,7 Joy WILLIAMS, PT, DPT8
From the 1Department of Physical Therapy, Rehabilitation Science, and Athletic Training, University of Kansas Medical Center, Kansas City, KS, 2Department of Physical Medicine and Rehabilitation, NYU Grossman School of Medicine, New York, NY, USA, 3School of Rehabilitation Science, University of Saskatchewan, Saskatoon, Canada, 4Center for Neuropsychology and Neuroscience Research, Kessler Foundation, East Hanover, NJ, 5Department of Physical Medicine and Rehabilitation, Rutgers – New Jersey Medical School, Newark, NJ, 6A.R. Dykes Library, University of Kansas Medical Center, Kansas City, KS, 7Department of Psychology, University of Kansas, Lawrence, KS, and 8Department of Physical Therapy, University of the Pacific, Stockton, CA, USA
Objective: To review the literature on whether sleep impacts mobility in adults.
Methods: Ovid Medline, Web of Science, Embase, and CINAHL databases were searched. Citations were randomly divided so that each was screened separately by 2 authors. Data were extracted from included articles independently by 2 reviewers.
Results: The search strategy generated 8,772 references, 697 articles underwent full-text screening, and 108 eligible articles were included in the scoping review. Most studies (n = 69; 64%) included only self-reported sleep, and “walking” was the most common mobility category (n = 99). Most studies (n = 60; 56%) reported a positive association between sleep and mobility, indicating better sleep was associated with better mobility or worse sleep was associated with worse mobility. Most studies, including people with cardiovascular, kidney, metabolic, mental health, neurological, and pulmonary conditions, reported a positive association between sleep and mobility.
Conclusions: Most studies reported a positive association between sleep and mobility. However, due to the variety of sleep and mobility outcomes used, it was challenging to compare studies and synthesize results. Further, due to a relatively small sample size and variety of health conditions, conclusions cannot be drawn, and further research is needed.
LAY ABSTRACT
Inadequate sleep can negatively impact health and function. The purpose of this scoping review was to evaluate the literature on whether sleep impacts mobility in adults. Multiple databases were searched, and the authors reviewed the search results for relevant articles to include. Information was extracted from the 108 included articles. Most studies (56%) reported a positive association between sleep and mobility, indicating better sleep was associated with better mobility or worse sleep was associated with worse mobility. Most studies including people with cardiovascular, kidney, metabolic, mental health, neurological, and pulmonary conditions reported a positive association between sleep and mobility. Due to the variety of ways the studies assessed sleep and mobility, it was challenging to compare studies and synthesize results. Clinicians should assess and address patients’ sleep issues. Further research is needed to confirm the association between sleep and mobility and to determine whether addressing sleep issues impacts mobility.
Key words: sleep; mobility; adults; scoping review.
Citation: J Rehabil Med 2026; 58: jrm44109. DOI: https://doi.org/10.2340/jrm.v58.44109.
Copyright: © 2026 The Author(s). Published by MJS Publishing, on behalf of the Foundation for Rehabilitation Information. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/).
Submitted: Jun 9, 2025; Accepted after revision: Sep 19, 2025; Published: Jan 7, 2026.
Correspondence address: Catherine F. Siengsukon, PT, PhD, Department of Physical Therapy, Rehabilitation Science, and Athletic Training, University of Kansas Medical Center, 3901 Rainbow Blvd, Mail Stop 2002, Kansas City, KS 66160, USA. E-mail: csiengsukon@kumc.edu
Sleep disturbances and insufficient sleep are common issues. More than 30% of adults get less than the recommended 7 h of sleep each night, and 50% report not feeling well rested (1, 2), suggesting inadequate sleep quality. Insufficient sleep is particularly pronounced in older adults, with approximately 75% of older adults reporting symptoms of insomnia (1).
Inadequate sleep and sleep disturbances have negative consequences on health and well-being, including reducing physical and cognitive function, negatively impacting participation in physical activity, and increasing the risk of falls (3–5). Poor sleep disrupts the body’s natural restorative processes, which are crucial for muscle repair, memory consolidation, and overall recovery (4, 6). Particularly regarding functional ability, older adults who have insomnia walk more slowly, demonstrate poorer cognitive performance, and report difficulty walking or negotiating stairs without resting (7, 8). Additionally, poor sleep quality has been associated with difficulties with community ambulation, navigating stairs, and performing activities of daily living (9–12). While there is evidence that poor sleep negatively impacts physical activity (13, 14) and physical performance (15–17), the nature of the relationship between sleep and mobility is still not fully understood.
Mobility is often impaired after injury or disease onset, and thus is a frequent target for rehabilitation. Understanding how sleep impacts mobility would provide insight into whether improving sleep should also be a goal during rehabilitation to enhance outcomes and recovery. Therefore, the purpose of this scoping review is to review the literature on whether sleep impacts mobility in adults. Optimal mobility has been defined as “being able to safely and reliably go where you want to go, when you want to go, and how you want to get there” (18). This refers to all forms of movement, including basic ambulation, exercising, completion of daily responsibilities, driving, and/or using any form of public transport. The International Classification of Functioning, Disability, and Health (ICF) model includes “mobility” as a subcategory within the domain of Activities and Participation (19). Because the ICF uses a broad description of mobility, and to keep focus for this scoping review, we focused on specific activities within the ICF mobility subcategories of “Changing basic body position” (d410), “Walking” (d450), and “Running” (d4552). We hypothesize that sleep would be positively associated with mobility, meaning better sleep would be associated with better mobility or worse sleep would be associated with worse mobility.
METHODS
For this scoping review, mobility is defined as: changing body position (d410), including getting into and out of a lying position (d4100), sitting position (d4103), or standing position (d4104), and rolling over (d4107); walking (d450) or running (d4552), regardless of distance or surface or obstacles; and going up and down stairs (d451) (19). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA – ScR) (20) guidelines and the Joanna Briggs Institute’s (JBI) updated methodology for scoping reviews (21) were followed for this scoping review. The research question was formulated based on the Population (Adult), Concept (Sleep), and Context (Mobility) framework recommended by the JBI Manual of Evidence Synthesis. A protocol was developed and registered in the Open Science Forum for conducting this scoping review (22).
We searched in the following bibliographic databases: Ovid Medline, Web of Science, Embase, and CINAHL. Additionally, Google Scholar and hand searching were conducted to find grey literature. The pilot search strategy of this review protocol was updated and rerun in Ovid Medline on 3 January 2024; the remaining searches were completed on the same date. Controlled vocabularies such as sleep, sleep deprivation, sleep disorder, mobility, mobility limitation, actigraphy etc. along with text words on the same concepts were used for searching without applying date filters. The searches have been conducted by author PV, a biomedical librarian. A complete search history from all 4 databases is available in Appendix S1.
Criteria for study inclusion were: (i) included human adult (> 18 years old) participants, (ii) study design that answered the scoping review question (i.e., cross-sectional, longitudinal, cohort, or retrospective study design; intervention if sleep was the intervention target), (iii) assessed sleep as part of the study (via self-report or objective measures; assessment of “daytime sleepiness” included), (iv) assessed mobility (via self-report or objective measures) per scoping review’s operational definition, (v) included statistical analyses to relate sleep assessment(s) to mobility assessment(s), and (vi) included original data. Studies were excluded if: (i) they included animals, (ii) they were written in a language other than English, (iii) the study design did not answer the research question (i.e., reviews, opinions, editorials, protocols; studies that quantified or categorized physical activity or physical fitness without assessment of mobility per scoping review definition of mobility; studies that assessed physical activity via questionnaire such as the IPAQ; studies that assessed falls or balance; tangential measures of sleep such as heart rate variability during sleep, use of sleep medications, and risk of a sleep disorder), (iv) data were reported in another study (duplicate dataset), (v) they were abstracts or non-peer reviewed sources (i.e., conference proceedings, preprint), (vi) they were irrelevant to the study question.
Citations were uploaded to EndNote version 21, and duplicates were removed. Citations were then uploaded into Covidence (Veritas Health Innovation, Melbourne, Australia; www.covidence.org), a web-based collaboration software platform, to perform the review process and data extraction. Each title/abstract was independently reviewed by 2 of 5 reviewers (CS, MB, SD, JW, AG) and the full-text articles were reviewed by 2 of 6 reviewers (CS, MB, SD, JW, AG, GB) to determine eligibility. Discrepancies were resolved by another reviewer (SC).
A standard data extraction form was built in Covidence by CS and reviewed and approved by all study personnel before data extraction started. For each article, data were extracted by 2 of 6 reviewers (CS, MB, SD, JW, AG, GB) and were then reviewed for accuracy, completeness, and to reach consensus by another reviewer (SC). Data extracted included the first author’s last name, year the article was published, the country in which the study was completed, the study design, the study aim, participant information (i.e., number of participants enrolled, age, sex, race, ethnicity, comorbid conditions), information on the intervention (if applicable), the mobility outcome and classification, the sleep outcome, and main results of how sleep impacts mobility. Bias risk and quality were not assessed in accordance with updated methodological recommendations (21).
Descriptive statistics (i.e.n number and percentage) were calculated. Sleep outcomes were coded by AG as “self-report” (i.e., questionnaire, answer to verbal or written question, etc.) or “objective” (i.e., wearable, actigraphy, polysomnography). Mobility outcomes were coded by AG into 7 mobility categories as per our operation definition of mobility (i.e., getting into and out of a lying position, getting into and out of a sitting position, getting into and out of a standing position, rolling over, walking, running, and going up and down stairs). The association between sleep and mobility was coded as “positive” (i.e., better sleep was associated with better mobility or poor sleep was associated with worse mobility), “negative” (i.e., better sleep was associated with worse mobility or poor sleep was associated with better mobility), “not associated” (sleep was not associated with mobility), or “mixed” (some results within the study were positive or negative and some results within the study were not associated). One author (MB) coded the association between sleep and mobility and the decision was reviewed by 2 other authors (AG, SC) and consensus was reached by CS.
RESULTS
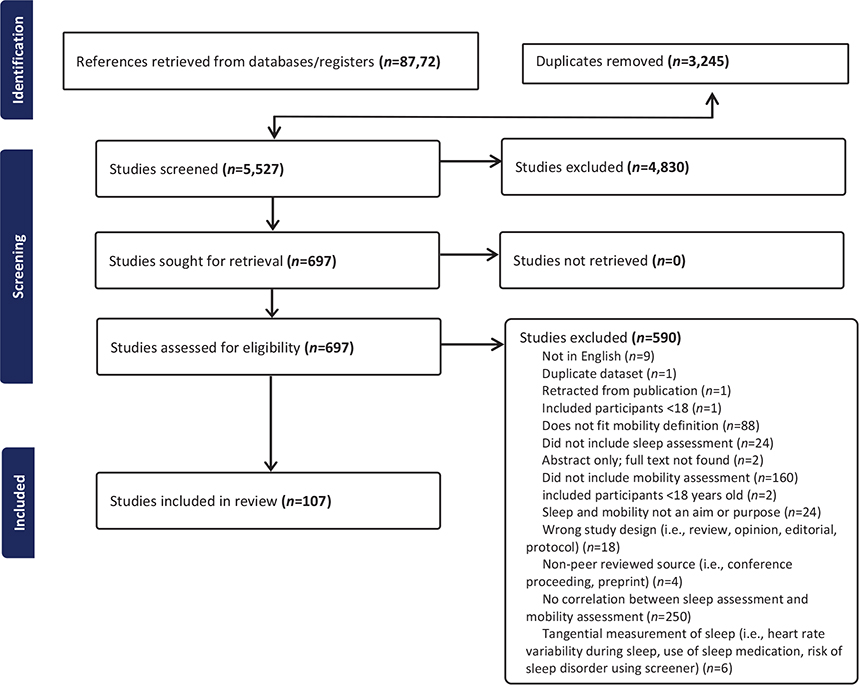
The search strategy generated 8,772 references. Duplicates (n = 3,245) were removed, leaving 5,527 titles/abstracts for review. Of the titles/abstracts reviewed, 4,830 were excluded due to not meeting eligibility criteria, leaving 697 full-text articles for review. Of the full-text articles, 590 were excluded for not meeting eligibility criteria, leaving 107 eligible articles for inclusion in the scoping review (Fig. 1; Appendix S2, Full Reference List of Included Articles).
The United States was the country where the highest number of studies were conducted (n = 34, 32%) followed by China (n = 11, 10%) and Japan (n = 10, 9%; Table I). Fifty-nine (55%) studies included people with health conditions, with neurological conditions (n = 22) being the most common category included and stroke being the most common specific neurologic condition (n = 9; Table II). Most studies included only self-reported sleep (n = 68, 64%; Table III) using measures ranging from 1-item questions to validated questionnaires (Table SI). The most common mobility category included in studies was walking (n = 101) followed by getting into and out of a sitting position (n = 26) and standing position (n = 24; Table III). It should be noted that some studies included more than 1 measure to assess a mobility category (e.g., used accelerometer and a self-report question to assess walking), included more than 1 mobility category so included multiple mobility measures (e.g., included accelerometer to assess walking mobility and included stairs to assess stair mobility), or some measures were used to examine more than 1 mobility category (e.g., the 5 times sit-to-stand test was counted for both getting into and out of sitting and getting into and out of standing position).
| Continent | n |
| Africa | 1 |
| Nigeria | 1 |
| Asia | 36 |
| China | 11 |
| India | 1 |
| Japan | 10 |
| Korea | 5 |
| South Korea | 2 |
| Taiwan | 5 |
| Turkey | 2 |
| Europe | 23 |
| Croatia | 1 |
| Denmark | 1 |
| Finland | 1 |
| Germany | 1 |
| Greece | 2 |
| Iceland* | 1 |
| Ireland | 2 |
| Italy | 1 |
| Netherlands | 1 |
| Norway | 1 |
| Portugal | 1 |
| Spain | 4 |
| Sweden | 1 |
| United Kingdom | 5 |
| North America | 39 |
| Canada | 5 |
| United States* | 34 |
| South America | 7 |
| Brazil | 7 |
| Australia/New Zealand | 2 |
| Australia | 1 |
| New Zealand | 1 |
| *One study included participants from 2 countries so n = 108. | |
| Item | n |
| Sleep measure category | |
| Objective only | 21 |
| Self-report only | 68 |
| Self-report and objective | 18 |
| Mobility category* | |
| Getting into and out of lying position | 6 |
| Getting into and out of sitting position | 26 |
| Getting into and out of standing position | 24 |
| Rolling over | 7 |
| Walking | 101 |
| Running | 1 |
| Going up and down stairs | 10 |
| Association between sleep and mobility | |
| Positive | 60 |
| Mixed | 33 |
| Not associated | 14 |
| Negative | 0 |
| *Some studies included more than 1 mobility outcome, or a mobility outcome could fall within more than 1 mobility category, so n does not equal 107. | |
The majority of studies (n = 60; 56%; Table III) reported a positive association between sleep and mobility, indicating better sleep was associated with better mobility or worse sleep was associated with worse mobility, 33 studies (31%) reported a mixed association meaning some results within the study showed a positive association while other results within the study did not show an association, and 14 studies (13%) reported no association between sleep and mobility (see Table SII). Of the 14 studies that reported no association between sleep and mobility, n = 6 did not enrol people with specific concurrent health conditions, and n = 8 were spread across different health conditions (n = 2 for musculoskeletal condition, neurological condition, and “Other; n = 1 for cardiovascular and pulmonary disease; Table IV). Of the 60 studies that reported a positive association and 33 studies that reported mixed association, n = 26 and n = 16 (respectively) did not enrol people with specific concurrent health conditions, and n = 34 and n = 17 (respectively) were spread across different health conditions (Table IV). No studies reported a negative association, indicating better sleep was associated with worse mobility or worse sleep was associated with better mobility.
When considering the association between sleep and mobility by health condition (see Table IV), most studies, including people with cardiovascular, kidney, metabolic, mental health, neurological, and pulmonary conditions reported a positive association between sleep and mobility. When the number of mixed association results is combined with positive association results, between 50% (musculoskeletal conditions on the low end) and 100% (kidney, metabolic, mental health, and sleep conditions on the high end) of studies reported some positive association between sleep and mobility.
When considering the association between sleep and mobility by type of sleep assessment (self-report only, objective only, both self-report and objective; Table V), there was a higher percentage of studies that reported a positive association between sleep outcomes and mobility outcomes in studies that used only self-report sleep assessments (59%) and those that used both self-report and objective sleep assessment (56%) than studies that used objective sleep assessments only (43%). When the number of mixed association results is combined with positive association results, 81% of objective only studies, 86% of self-report only, and 100% that used both sleep assessment reported some positive association between sleep and mobility.
When considering the association between sleep and mobility by mobility category (Table VI), half or more of the articles, including the mobility categories of getting into and out of a lying position, rolling over, walking, and going up and down stairs, reported a positive association between sleep and mobility. The mobility category with the highest percentage of articles that reported no association between sleep and mobility was walking (n = 14; 19%) followed by getting into and out of a standing position (n = 4; 17%).
DISCUSSION
Overall, the hypothesis that sleep would be positively associated with mobility was supported. When examining the association between sleep and mobility by comorbid condition, the lowest percentage of studies that included at least some positive association between sleep and mobility (mixed + positive in Table IV) was in studies including people with musculoskeletal comorbid conditions (50% of studies) and the highest percentage (100%) was in studies including people with kidney disease, metabolic conditions, mental health conditions, and sleep disorders.
It is perhaps not a surprise that all studies including people with kidney disease, metabolic conditions, mental health conditions, and sleep disorders had at least some positive association between sleep and mobility, as sleep disorders and disturbances increase the risk of metabolic conditions, kidney disease, and mental health conditions. Sleep and circadian rhythms play a critical role in regulating daily physiological patterns essential for maintaining normal metabolic function (23). Disruption of circadian rhythms has increasingly been identified as a significant factor contributing to impaired physiological processes and the development of various diseases, particularly metabolic dysregulation (24–26). Factors such as irregular sleep patterns, insomnia, sleep apnoea, narcolepsy, and shift work disorder are well recognized as contributors to sleep deficiencies, which may, in turn, promote the onset of metabolic disorders (27–30). A growing body of evidence indicates that sleep disturbances may also contribute to the development of kidney disease. A meta-analysis identified an association between short sleep duration and proteinuria, a surrogate marker for kidney disease progression (35). Additionally, renal hyperfiltration, an early indicator of renal damage, has been linked to both short sleep duration (less than 6 h) and long sleep duration (more than 10 h) (36, 37). Renal hyperfiltration can cause an increase in urination due to the larger volume of urine being produced by the kidneys (38); this may impact sleep quality and an individual’s ability to get comfortable in bed and fall back asleep after getting up to use the bathroom during the night. Further, sleep disorders often coexist with mental health conditions, and sleep disruption may be involved in the development and maintenance of mental health conditions (39). The mechanisms underpinning how sleep disturbances may contribute to the development of mental health disorders are likely to be a combination of circadian disruption or misalignment, genetic associations, sleep’s impact on neuroplasticity, and sleep’s impact on cognition and emotional regulation (39). Indeed, interventions that address sleep and circadian disruption have a positive impact on mental health conditions (39).
It is also not a surprise that studies including people with musculoskeletal comorbid conditions had the lowest percentage of results with positive or mixed association. People with musculoskeletal comorbid conditions may have limited mobility due to the musculoskeletal condition itself (i.e., impaired joint mobility, muscle weakness, impaired mechanics, or pain). Also, only 3 studies included people with musculoskeletal conditions, so more research is needed in this area before conclusions can be made.
It is interesting that the majority of studies examined walking mobility (n = 101), and relatively few examined rolling over (n = 7). Humans change position, including rolling over, periodically throughout the night while sleeping, often without waking. If someone has impaired ability to roll in bed, it is conceivable that additional effort or exertion to roll or inability to roll into a more comfortable position would increase the likelihood of awakening and sleep disturbances. Indeed, impaired rolling ability was associated with poorer sleep outcomes in people with Parkinson’s disease, spinal cord injury, and amyotrophic lateral sclerosis in studies included in this scoping review (40–43). Similarly, getting into and out of a lying position and standing position is needed to rise from bed to go to the bathroom. More effort or exertion, or frustration with impaired mobility of getting into and out of a lying or standing position, could conceivably increase arousal and impair the ability to return to sleep and, thus, increase sleep disturbances. Additional research is needed to examine how impaired mobility, particularly bed mobility, may impact sleep and whether focused interventions to improve bed mobility also improve sleep outcomes.
A challenge with examining how sleep impacts mobility for this scoping review is the variety of measures used to assess both sleep and mobility, which made the synthesis of results and comparison across studies difficult. The majority of studies included (64%) used only self-reported measures to assess sleep, and some used invalid and unreliable measures to assess sleep or used only a single question to assess sleep. Self-report and objective sleep measures assess different sleep constructs, so it is ideal to include both types of valid and reliable measures (only 17% of included studies included both) as well as intentionally select sleep measures for the intended sleep construct (i.e., use the PSQI to assess self-reported sleep quality). Also, attempts to build consensus for mobility measures have focused on addressing the variability and lack of standardization in definitions, constructs, and assessments. Researchers emphasize the need for a unified approach to define mobility comprehensively, encompassing constructs like physical capacity, performance, and functional independence. Efforts to standardize include the development of core sets of outcome measurement instruments and detailed protocols to ensure consistency in assessment across studies. These initiatives aim to improve comparability of data, enhance the precision of findings, and facilitate large-scale data sharing, enabling a deeper understanding of complex relationships (such as those between sleep and mobility). Standardization is essential to advancing personalized and effective interventions in clinical and research contexts (44, 45).
A strength of this scoping review is that included studies were conducted in 27 different countries, spanning 6 continents (Antarctica not included), indicating the generalizability of the results. However, a high number of studies (n = 40, 37%) were conducted in North America, with the United States being the most represented country (n = 35, 32%). Another strength is the variety of comorbid conditions included, which allowed for the exploration of how sleep impacts mobility by major health category or system. Due to the relatively small number of studies of each health category or system and the variety of specific conditions within each category/system, conclusions cannot be drawn at this point. However, this scoping review does provide insight into health categories/systems where further research is warranted. Given that most sleep disorders are treatable, addressing sleep disturbances may play a crucial role in alleviating mobility impairments in individuals with these comorbidities. Targeted interventions for sleep disorders could offer a promising pathway to improving overall mobility and quality of life in affected populations. We also acknowledge that our definition of mobility, which was based on specific “mobility” subcategories (“Lying down” d4100, “Sitting” d4103, “Standing” d4104, “Rolling over” d4107, “Walking” d450, and “Running” d4552) within the domain of Activities and Participation of the ICF model (19) excludes other types of mobility such as wheelchair mobility, driving, jumping, climbing, swimming, and use of transportation. Future reviews should consider examining how sleep impacts other subcategories of mobility, such as maintaining body position, carrying, moving and handling objects, and moving around using transportation. In addition, a future meta-analysis should consider the strength of the association between sleep and mobility. A limitation of this scoping review is that the search was completed in January 2024, which limits its scope.
Overall, this scoping review provides a description of the literature on the association between sleep and mobility in adults. The results indicate that there is a positive association between sleep and mobility; better sleep is associated with better mobility and worse sleep is associated with worse mobility, particularly for getting into and out of a lying position, rolling over, walking, and going up and down stairs. Due to the variety of sleep and mobility outcomes used, it was challenging to compare studies and synthesize results. Most studies, including people with cardiovascular disease, kidney disease, metabolic conditions, mental health conditions, neurological conditions, and pulmonary disease, reported a positive association between sleep and mobility. However, due to a relatively small sample size within a given health condition, conclusions cannot be drawn, and further research is needed.
ACKNOWLEDGEMENT
Conflict of interest: Catherine Siengsukon is owner and CEO of Sleep Health Education, LLC. The other authors do not have any conflicts of interest to declare
REFERENCES
- Sleep Foundation. 100+ Sleep Statistics. 2025 [cited 2025 Aug 20]. Available from: https://www.sleepfoundation.org/how-sleep-works/sleep-facts-statistics.
- National Sleep Foundation. Sleep in America Poll: Sleep health & scheduling. 2019 [cited 2025 Aug 20]. Available from: https://www.sleepfoundation.org/wp-content/uploads/2019/02/SIA_2019_Sleep_Health_and_Scheduling.pdf.
- Colten HR, Altevogt BM, Committee on Sleep Medicine and Research. Sleep disorders and sleep deprivation: an unmet public health problem. Washington, DC: National Academies Press; 2006.
- Medic G, Wille M, Hemels ME. Short- and long-term health consequences of sleep disruption. Nat Sci Sleep 2017; 9: 151–161. https://doi.org/10.2147/NSS.S134864
- Buysse DJ. Sleep health: can we define it? Does it matter? Sleep 2014; 37: 9–17. https://doi.org/10.5665/sleep.3298
- Walker MP. The role of slow wave sleep in memory processing. JCSM 2009; 5: S20–26. https://doi.org/10.5664/jcsm.5.2S.S20
- Stenholm S, Kronholm E, Sainio P, Borodulin K, Era P, Fogelholm M, et al. Sleep-related factors and mobility in older men and women. J Gerontol A Biol Sci Med Sci 2010; 65: 649–657. https://doi.org/10.1093/gerona/glq017
- Kirshner D, Kizony R, Gil E, Asraf K, Krasovsky T, Haimov I, et al. Why do they fall? The impact of insomnia on gait of older adults: a case-control study. Nat Sci Sleep 2021; 13: 329–338. https://doi.org/10.2147/NSS.S299833
- Goldman SE, Stone KL, Ancoli-Israel S, Blackwell T, Ewing SK, Boudreau R, et al. Poor sleep is associated with poorer physical performance and greater functional limitations in older women. Sleep 2007; 30: 1317–1324. https://doi.org/10.1093/sleep/30.10.1317
- Campanini MZ, Mesas AE, Carnicero-Carreño JA, Rodríguez-Artalejo F, Lopez-Garcia E. Duration and quality of sleep and risk of physical function impairment and disability in older adults: results from the ENRICA and ELSA Cohorts. Aging Dis 2019; 10: 557–569. https://doi.org/10.14336/AD.2018.0611
- Vincent BM, Johnson N, Tomkinson GR, McGrath R, Clark BC, Choi BJ. Sleeping time is associated with functional limitations in a national sample of older Americans. Aging Clin Exp Res 2021; 33: 175–182. https://doi.org/10.1007/s40520-020-01524-0
- Spira AP, Covinsky K, Rebok GW, Punjabi NM, Stone KL, Hillier TA, et al. Poor sleep quality and functional decline in older women. J Am Geriatr Soc 2012; 60: 1092–1098. https://doi.org/10.1111/j.1532-5415.2012.03968.x
- McCoy T, Sochan AJ, Spaeth AM. The relationship between sleep and physical activity by age, race, and gender. Rev Cardiovasc Med 2024; 25: 378–392. https://doi.org/10.31083/j.rcm2510378
- Bisson ANS, Lachman ME. The relationship of daily physical activity and sleep in adults: variations by age, sex, and race. J Behav Med 2023; 46: 642–654. https://doi.org/10.1007/s10865-022-00387-2
- Craven J, McCartney D, Desbrow B, Sabapathy S, Bellinger P, Roberts L, et al. Effects of acute sleep loss on physical performance: a systematic and meta-analytical review. Sports Med 2022; 52: 2669–2690. https://doi.org/10.1007/s40279-022-01706-y
- Grandou C, Wallace L, Fullagar HHK, Duffield R, Burley S. The effects of sleep loss on military physical performance. Sports Med 2019; 49: 1159–1172. https://doi.org/10.1007/s40279-019-01123-8
- Gong M, Sun M, Sun Y, Jin L, Li S. Effects of acute sleep deprivation on sporting performance in athletes: a comprehensive systematic review and meta-Analysis. Nat Sci Sleep 2024; 16: 935–948. https://doi.org/10.2147/NSS.S467531
- Satariano WA, Guralnik JM, Jackson RJ, Marottoli RA, Phelan EA, Prohaska TR. Mobility and aging: new directions for public health action. Am J Public Health. 2012; 102: 1508–1515. https://doi.org/10.2105/AJPH.2011.300631
- World Health Organization. International classification of functioning, disability and health (ICF). n.d. [cited 2025 Aug 25]. Available from: https://icd.who.int/dev11/l-icf/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f2048203604.
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018; 169: 467–473. https://doi.org/10.7326/M18-0850
- Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Implement 2021; 19: 3–10. https://doi.org/10.1097/XEB.0000000000000277
- Siengsukon C, Vaduvathiriyan P, Donkers S, Costa SL, Williams J, Beheshti M. How does sleep impact mobility? A scoping review protocol. 2024 [cited 2025 Aug 25]. Available from: https://osf.io/d9e5k. https://doi.org/10.1101/2025.05.05.25326996
- Serin Y, Acar Tek N. Effect of circadian rhythm on metabolic processes and the regulation of energy balance. Ann Nutr Metab 2019; 74: 322–330. https://doi.org/10.1159/000500071
- Markwald RR, Melanson EL, Smith MR, Higgins J, Perreault L, Eckel RH, et al. Impact of insufficient sleep on total daily energy expenditure, food intake, and weight gain. Proc Natl Acad Sci U S A 2013; 110: 5695–5700. https://doi.org/10.1073/pnas.1216951110
- Spiegel K, Tasali E, Leproult R, Scherberg N, Van Cauter E. Twenty-four-hour profiles of acylated and total ghrelin: relationship with glucose levels and impact of time of day and sleep. J Clin Endocrinol Metab 2011; 96: 486–493. https://doi.org/10.1210/jc.2010-1978
- Nguyen J, Wright KP, Jr. Influence of weeks of circadian misalignment on leptin levels. Nat Sci Sleep 2010; 2: 9–18. https://doi.org/10.2147/NSS.S7624
- Marcheva B, Ramsey KM, Buhr ED, Kobayashi Y, Su H, Ko CH, et al. Disruption of the clock components CLOCK and BMAL1 leads to hypoinsulinaemia and diabetes. Nature 2010; 466: 627–631. https://doi.org/10.1038/nature09253
- Spiegel K, Knutson K, Leproult R, Tasali E, Van Cauter E. Sleep loss: a novel risk factor for insulin resistance and Type 2 diabetes. J Appl Physiol 2005; 99: 2008–2019. https://doi.org/10.1152/japplphysiol.00660.2005
- Turek FW, Joshu C, Kohsaka A, Lin E, Ivanova G, McDearmon E, et al. Obesity and metabolic syndrome in circadian clock mutant mice. Science 2005; 308: 1043–1045. https://doi.org/10.1126/science.1108750
- Depner CM, Stothard ER, Wright KP, Jr. Metabolic consequences of sleep and circadian disorders. Curr Diab Rep 2014; 14: 507–522. https://doi.org/10.1007/s11892-014-0507-z
- D’Elia JA, Roshan B, Maski M, Weinrauch LA. Manifestation of renal disease in obesity: pathophysiology of obesity-related dysfunction of the kidney. Int J Nephrol Renovasc Dis 2009; 2: 39–49. https://doi.org/10.2147/IJNRD.S7999
- Bastard JP, Maachi M, Lagathu C, Kim MJ, Caron M, Vidal H, et al. Recent advances in the relationship between obesity, inflammation, and insulin resistance. Eur Cytokine Netw 2006; 17: 4–12.
- Davydov GG, Nashat H, Ghali S, Afifi S, Suryadevara V, Habab Y, et al. Common sleep disorders in `patients with chronic kidney disease: a systematic review on what they are and how we should treat them. Cureus 2023; 15: e44009. https://doi.org/10.7759/cureus.44009
- Lyons OD. Sleep disorders in chronic kidney disease. Nat Rev Nephrol 2024; 20: 690–700. https://doi.org/10.1038/s41581-024-00848-8
- Cheungpasitporn W, Thongprayoon C, Gonzalez-Suarez ML, Srivali N, Ungprasert P, Kittanamongkolchai W, et al. The effects of short sleep duration on proteinuria and chronic kidney disease: a systematic review and meta-analysis. Nephrol Dial Transplant 2017; 32: 991–996. https://doi.org/10.1093/ndt/gfw072
- Lin M, Su Q, Wen J, Wei S, Yao J, Huang H, et al. Self-reported sleep duration and daytime napping are associated with renal hyperfiltration in general population. Sleep Breath 2018; 22: 223–232. https://doi.org/10.1007/s11325-017-1470-0
- Koh JH, Yeo BSY, Tan TWE, See MYS, Ng ACW, Loh SRH, et al. The association of sleep duration with the risk of chronic kidney disease: a systematic review and meta-analysis. Clin Kidney J 2024; 17: sfae177. https://doi.org/10.1093/ckj/sfae177
- Moriconi D, Sacchetta L, Chiriacò M, Nesti L, Forotti G, Natali A, et al. Glomerular hyperfiltration predicts kidney function decline and mortality in type 1 and type 2 diabetes: a 21-year longitudinal study. Diabetes Care 2023; 46: 845–853. https://doi.org/10.2337/dc22-2003
- Meyer N, Lok R, Schmidt C, Kyle SD, McClung CA, Cajochen C, et al. The sleep–circadian interface: a window into mental disorders. Proc Natl Acad Sci U S A 2024; 121: e2214756121. https://doi.org/10.1073/pnas.2214756121
- Diaz-Abad M, Buczyner JR, Venza BR, Scharf SM, Kwan JY, Lubinski B, et al. Poor sleep quality in patients with amyotrophic lateral sclerosis at the time of diagnosis. J Clin Neuromuscul Dis 2018; 20: 60–68. https://doi.org/10.1097/CND.0000000000000234
- Lee W, Jeong S, Lee B-S, Lim J-c, Kim O. Association between functional outcomes and psychological variables in persons with spinal cord injury. Sci Rep 2023; 13: 23092. https://doi.org/10.1038/s41598-023-50252-8
- Stack EL, Ashburn AM. Impaired bed mobility and disordered sleep in Parkinson’s disease. Mov Disord 2006; 21: 1340–1342. https://doi.org/10.1002/mds.20944
- Xue F, Wang FY, Mao CJ, Guo SP, Chen J, Li J, et al. Analysis of nocturnal hypokinesia and sleep quality in Parkinson’s disease. J Clin Neurosci 2018; 54: 96–101. https://doi.org/10.1016/j.jocn.2018.06.016
- Reijnierse EM, Geelen SJG, van der Schaaf M, Visser B, Wust RCI, Pijnappels M, et al. Towards a core-set of mobility measures in ageing research: the need to define mobility and its constructs. BMC Geriatr 2023; 23: 220–235. https://doi.org/10.1186/s12877-023-03859-5
- Van Criekinge T, Saeys W, Truijen S, Vereeck L, Sloot LH, Hallemans A. A full-body motion capture gait dataset of 138 able-bodied adults across the life span and 50 stroke survivors. Sci Data 2023; 10: 852–860. https://doi.org/10.1038/s41597-023-02767-y